
Remote Gait Type Classification System Using Markerless 2D Video

 , and
, and
Abstract
:1. Introduction
1.1. Related Work
- floor-based sensors;
- wearable sensors;
- vision-based sensors.
1.1.1. Gait Classification Systems
1.1.2. Gait Datasets
2. Materials and Methods
- proposal of a new, larger, gait type dataset: GAIT-IT;
- a gait type classification system;
- a remote diagnosing web application.
2.1. GAIT-IT Dataset
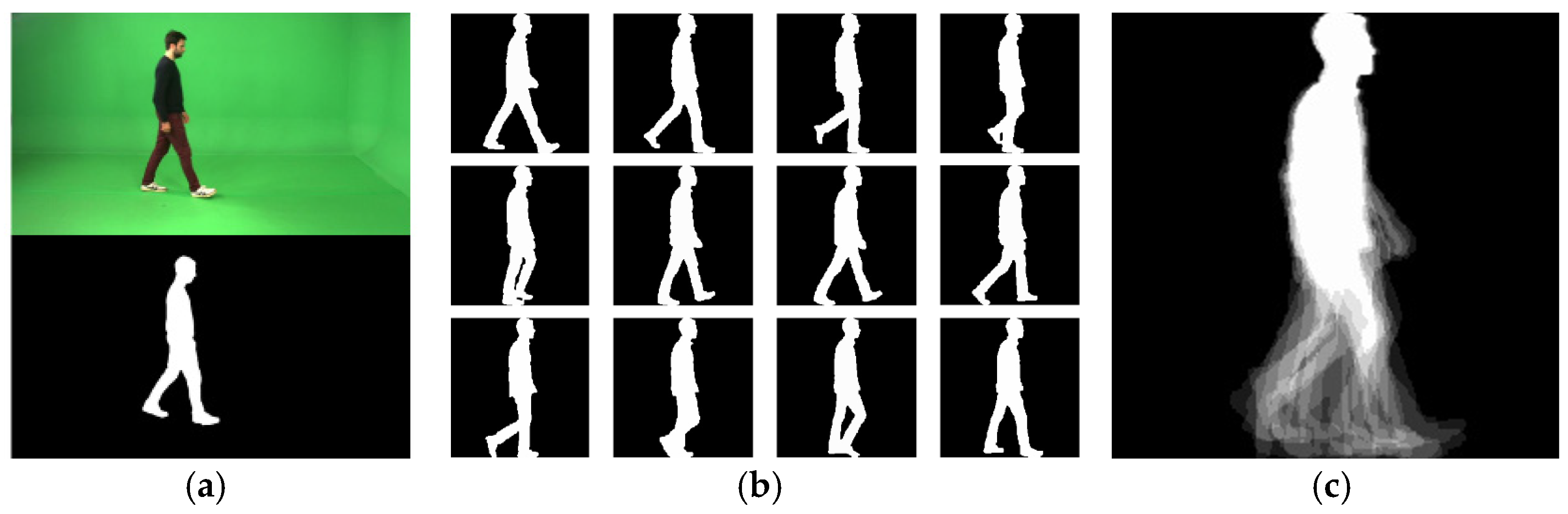
- sequence of binary silhouettes;
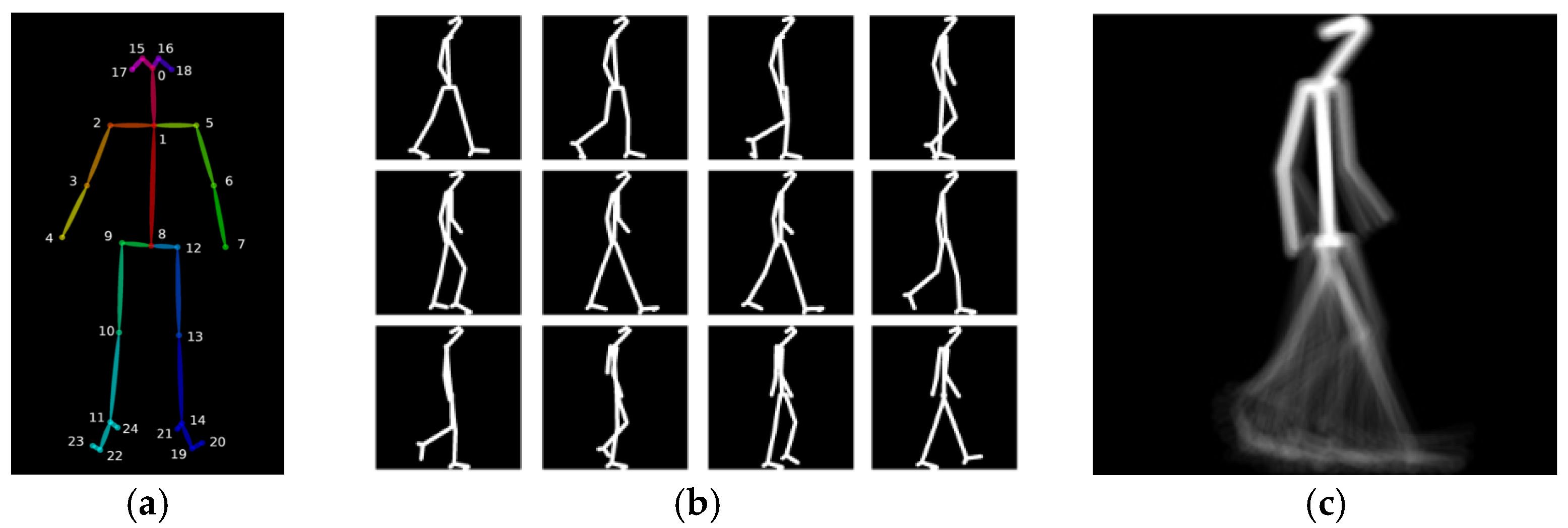
- sequence of skeletal images;
- GEIs;
- SEIs.
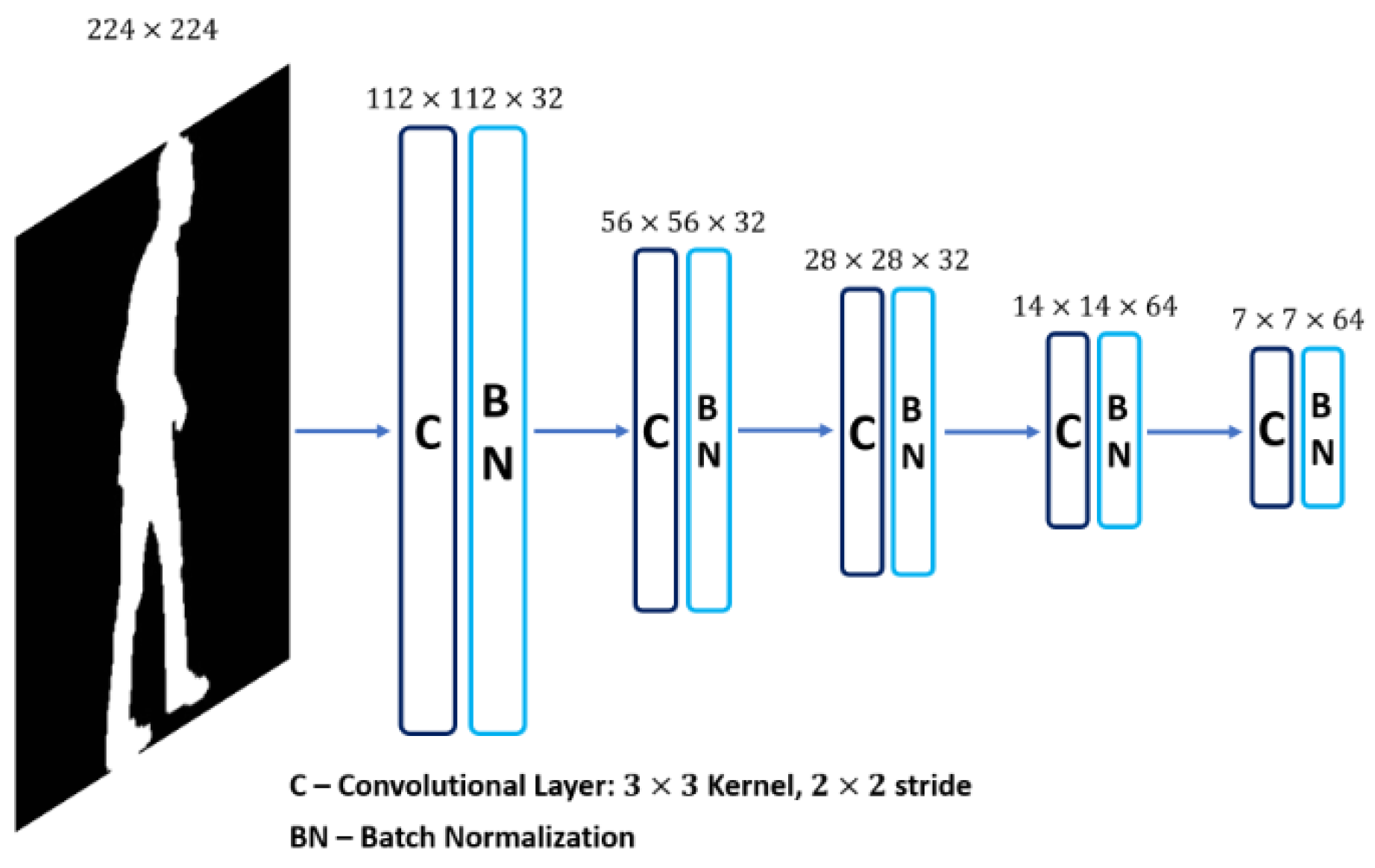
2.2. Gait Type Classification System
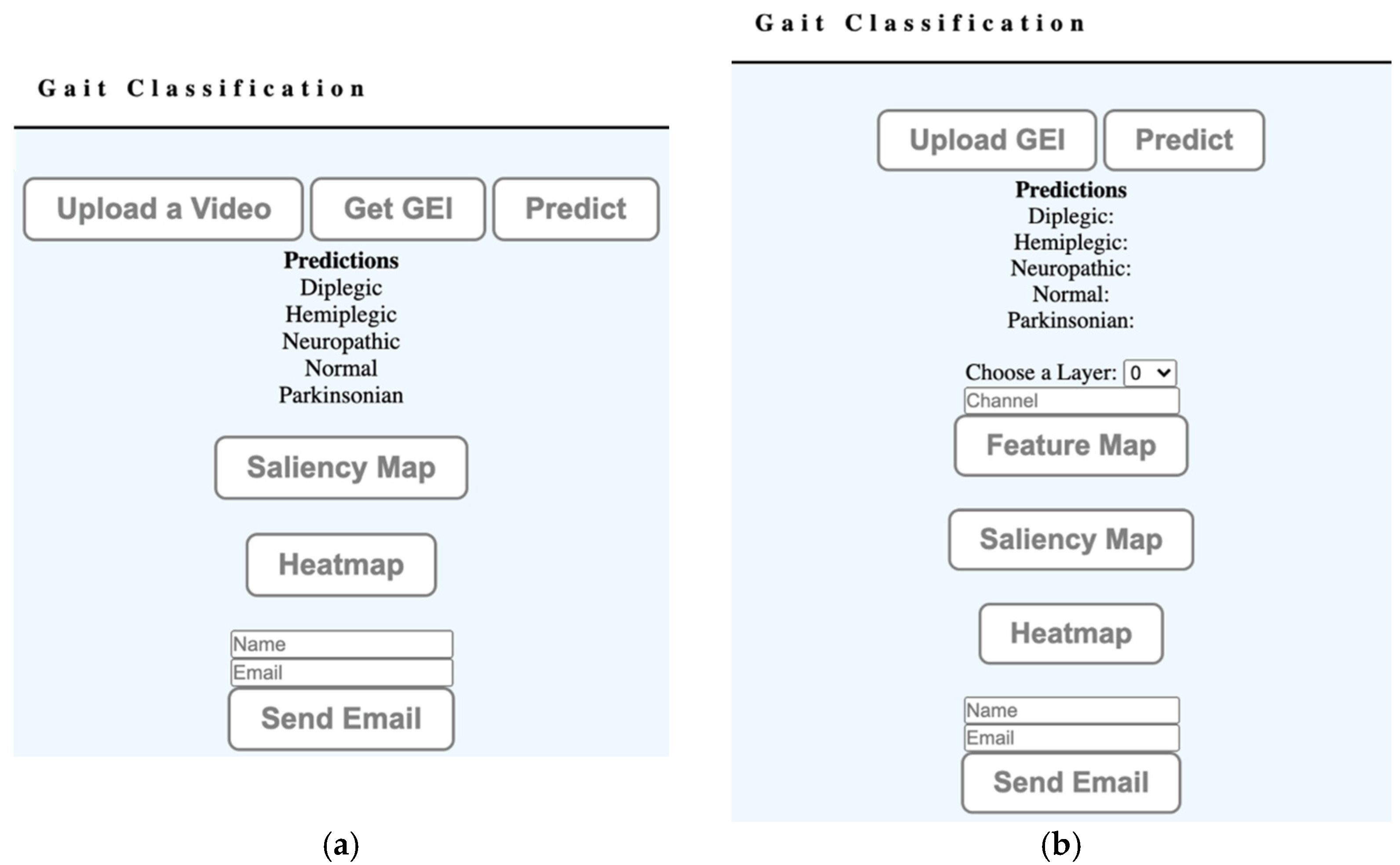
2.3. A Remote Diagnostic Web Application Prototype
- basic mode;
- advanced mode.
3. Results
4. Discussion
5. Conclusions
- The shallower network model achieves a better fit using the GAIT-IT dataset, which contains data from only 21 subjects, as confirmed by the cross-database test results. This is significant as the proposed web application accepts video sequences captured under different conditions and environments.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kirtley, C. Clinical Gait Analysis: Theory and Practice; Elsevier Health Sciences: New York, NY, USA, 2006. [Google Scholar]
- Boyd, J.E.; Little, J.J. Biometric gait recognition. In Advanced Studies in Biometrics; Springer: Berlin/Heidelberg, Germany, 2005; pp. 19–42. [Google Scholar]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ailisto, H.J.; Lindholm, M.; Mantyjarvi, J.; Vildjiounaite, E.; Makela, S.-M. Identifying people from gait pattern with accelerometers. Biom. Technol. Hum. Identif. Int. Soc. Opt. Photonics 2005, 5779, 7–14. [Google Scholar]
- Verlekar, T.T.; Soares, L.D.; Correia, P.L. Automatic classification of gait impairments using a marker-less 2D video-based system. Sensors 2018, 18, 2743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loureiro, J.; Correia, P.L. Using a skeleton gait energy image for pathological gait classification. In Proceedings of the 15th IEEE International Conference on Automatic Face and Gesture Recognition, Buenos Aires, Argentina, 16–20 May 2020; pp. 410–414. [Google Scholar]
- Khokhlova, M.; Migniot, C.; Morozov, A.; Sushkova, O.; Dipanda, A. Normal and pathological gait classification LSTM model. Artif. Intell. Med. 2019, 94, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Verlekar, T.T.; Soares, L.D.; Correia, P.L. Using transfer learning for classification of gait pathologies. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 3–6 December 2018; pp. 2376–2381. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556, preprint. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Li, F.-F. Imagenet: A large-scale hierarchical image database. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Slijepcevic, D.; Zeppelzauer, M.; Gorgas, A.M.; Schwab, C.; Schüller, M.; Baca, A.; Breiteneder, C.; Horsak, B. Automatic classification of functional gait disorders. IEEE J. Biomed. Health Inform. 2018, 22, 1653–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannini, A.; Trojaniello, D.; Cereatti, A.; Sabatini, A. A Machine Learning Framework for Gait Classification Using Inertial Sensors: Application to Elderly, Post-Stroke and Huntington’s Disease Patients. Sensors 2016, 16, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanrenterghem, J.; Gormley, D.; Robinson, M.; Lees, A. Solutions for representing the whole-body centre of mass inside cutting manoeuvres based on data that is typically available for lower limb kinematics. Gait Posture 2010, 31, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Verlekar, T.; Vroey, H.; Claeys, K.; Hallez, H.; Soares, L.; Correia, P. Estimation and validation of temporal gait features using a markerless 2D video system. Comput. Methods Programs Biomed. 2019, 175, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; She, M.; Nahavandi, S.; Kouzani, A. A review of vision-based gait recognition methods for human identification. In Proceedings of the International Conference on Digital Image Computing: Techniques and Applications, Sydney, Australia, 1–3 December 2010; pp. 320–327. [Google Scholar]
- Verlekar, T.; Correia, P.; Soares, L. Gait recognition using normalized shadows. In Proceedings of the 25th European Signal Processing Conference (EUSIPCO), Kos Island, Greece, 28 August–2 September 2017; pp. 936–940. [Google Scholar]
- Wang, Y.; Sun, J.; Li, J.; Zhao, D. Gait recognition based on 3D skeleton joints captured by kinect. In Proceedings of the IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, 25–28 September 2016; pp. 3151–3155. [Google Scholar]
- Han, J.; Bhanu, B. Individual recognition using gait energy image. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 28, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.; Sheikh, Y. Open pose: Realtime multi-person 2D pose estimation using part affinity fields. arXiv 2018, arXiv:1812.08008. [Google Scholar]
- Nieto-Hidalgo, M.; García-Chamizo, J. Classification of pathologies using a vision based feature extraction. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Philadelphia, PA, USA, 7–10 November 2017; pp. 265–274. [Google Scholar]
- Ortells, J.; Herrero-Ezquerro, M.; Mollineda, R. Vision-based gait impairment analysis for aided diagnosis. Med Biol. Eng. Comput. 2018, 56, 1553–1564. [Google Scholar] [CrossRef] [PubMed]
- Nieto-Hidalgo, M.; Ferrández-Pastor, F.; Valdivieso-Sarabia, R.; Mora-Pascual, J.; García-Chamizo, J. Vision based extraction of dynamic gait features focused on feet movement using RGB camera. In Ambient Intelligence for Health; Springer: Cham, Switzerland, 2015; pp. 155–166. [Google Scholar]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Stanford School of Medicine. Gait Abnormalities. Available online: https://stanfordmedicine25.stanford.edu/the25/gait.html (accessed on 3 September 2021).
- Digit Recognizer. Available online: https://www.kaggle.com/c/digit-recognizer/overview (accessed on 3 September 2021).
- Deotte, C. How to Choose CNN Architecture MNIST. Available online: https://www.kaggle.com/cdeotte/how-to-choose-cnn-architecture-mnist (accessed on 3 September 2021).
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdi-nov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Kingma, D.; Ba, J. Adam: A method for stochastic optimization. In Proceedings of the 3rd International Conference on Learning Representations, ICLR, San Diego, CA, USA, 7–9 May 2015; pp. 1–15. [Google Scholar]
- Nesterov, Y. A method for solving the convex programming problem with convergence rate O(1/k2). Dokl. Akad. Nauk Sssr. 1983, 269, 543–547. [Google Scholar]
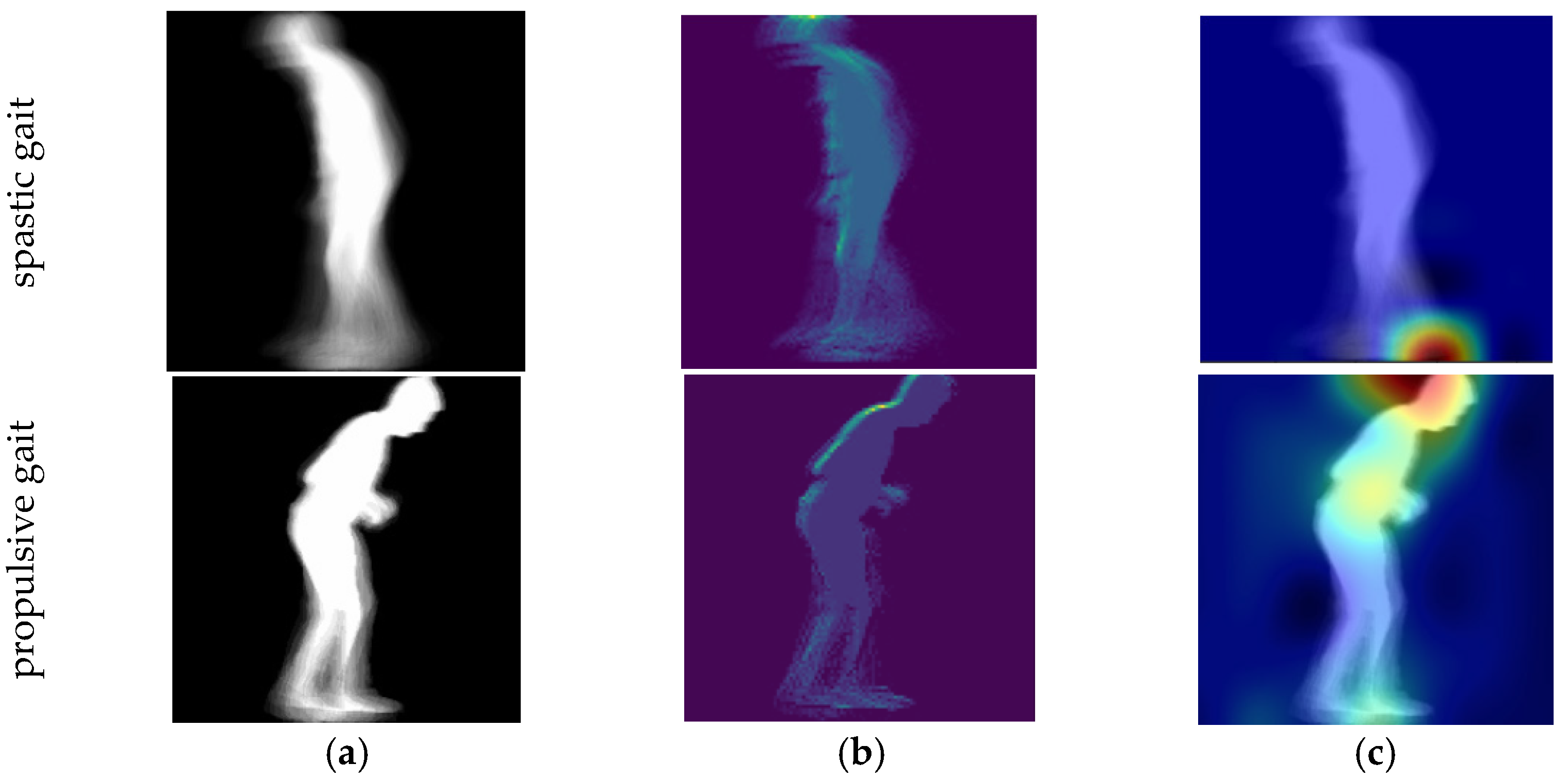
- Simonyan, K.; Vedaldi, A.; Zisserman, A. Deep inside convolutional networks: Visualizing image classification models and saliency maps. arXiv 2013, arXiv:1312.6034. [Google Scholar]
- Selvaraju, R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE international conference on computer vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Folk, M.; Heber, G.; Koziol, Q.; Pourmal, E.; Robinson, D. An overview of the HDF5 technology suite and its applications. In Proceedings of the EDBT/ICDT 2011 Workshop on Array Databases, Uppsala, Sweden, 25 March 2011; pp. 36–47. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gait Classification System | Input | Accuracy (%) |
|---|---|---|
| Fine-Tuned VGG-19 [8] | GEI | 94.0 |
| Fine-Tuned VGG-19 [6] | SEI | 93.6 |
| Proposed system | GEI | 93.4 |
| Proposed system | SEI | 92.6 |
| Gait Classification System | Parameters | Size (Mb) | Execution Time (ms) | |
|---|---|---|---|---|
| Train | Test | |||
| Fine-Tuned VGG-19 [6,8] | 139,330,565 | 558.4 | 15 | 6 |
| Proposed system | 1,684,421 | 6.8 | 1 | 1 |
| Gait Classification System | Input | Accuracy (%) |
|---|---|---|
| Fine-Tuned VGG-19 [8] | GEI | 86.4 |
| Fine-Tuned VGG-19 [6] | SEI | 85.1 |
| Proposed system | GEI | 89.8 |
| Proposed system | SEI | 86.4 |
| Predicted Class | ||||||
|---|---|---|---|---|---|---|
| True Class | Gait Type | Scissor (Diplegic) | Spastic (Hemiplegic) | Steppage (Neuropathic) | Normal (Healthy) | Propulsive (Parkinsonian) |
| Scissor | 87 | 7 | 0 | 0 | 5 | |
| Spastic | 9 | 89 | 2 | 0 | 0 | |
| Steppage | 0 | 2 | 97 | 1 | 0 | |
| Normal | 0 | 0 | 0 | 99 | 0 | |
| Propulsive | 5 | 0 | 0 | 0 | 95 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albuquerque, P.; Machado, J.P.; Verlekar, T.T.; Correia, P.L.; Soares, L.D. Remote Gait Type Classification System Using Markerless 2D Video. Diagnostics 2021, 11, 1824. https://doi.org/10.3390/diagnostics11101824
Albuquerque P, Machado JP, Verlekar TT, Correia PL, Soares LD. Remote Gait Type Classification System Using Markerless 2D Video. Diagnostics. 2021; 11(10):1824. https://doi.org/10.3390/diagnostics11101824
Chicago/Turabian StyleAlbuquerque, Pedro, João Pedro Machado, Tanmay Tulsidas Verlekar, Paulo Lobato Correia, and Luís Ducla Soares. 2021. "Remote Gait Type Classification System Using Markerless 2D Video" Diagnostics 11, no. 10: 1824. https://doi.org/10.3390/diagnostics11101824
APA StyleAlbuquerque, P., Machado, J. P., Verlekar, T. T., Correia, P. L., & Soares, L. D. (2021). Remote Gait Type Classification System Using Markerless 2D Video. Diagnostics, 11(10), 1824. https://doi.org/10.3390/diagnostics11101824