
Effect of Aging, Gender and Sensory Stimulation of TRPV1 Receptors with Capsaicin on Spontaneous Swallowing Frequency in Patients with Oropharyngeal Dysphagia: A Proof-of-Concept Study

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.1.1. Healthy Volunteers
2.1.2. Stroke Patients
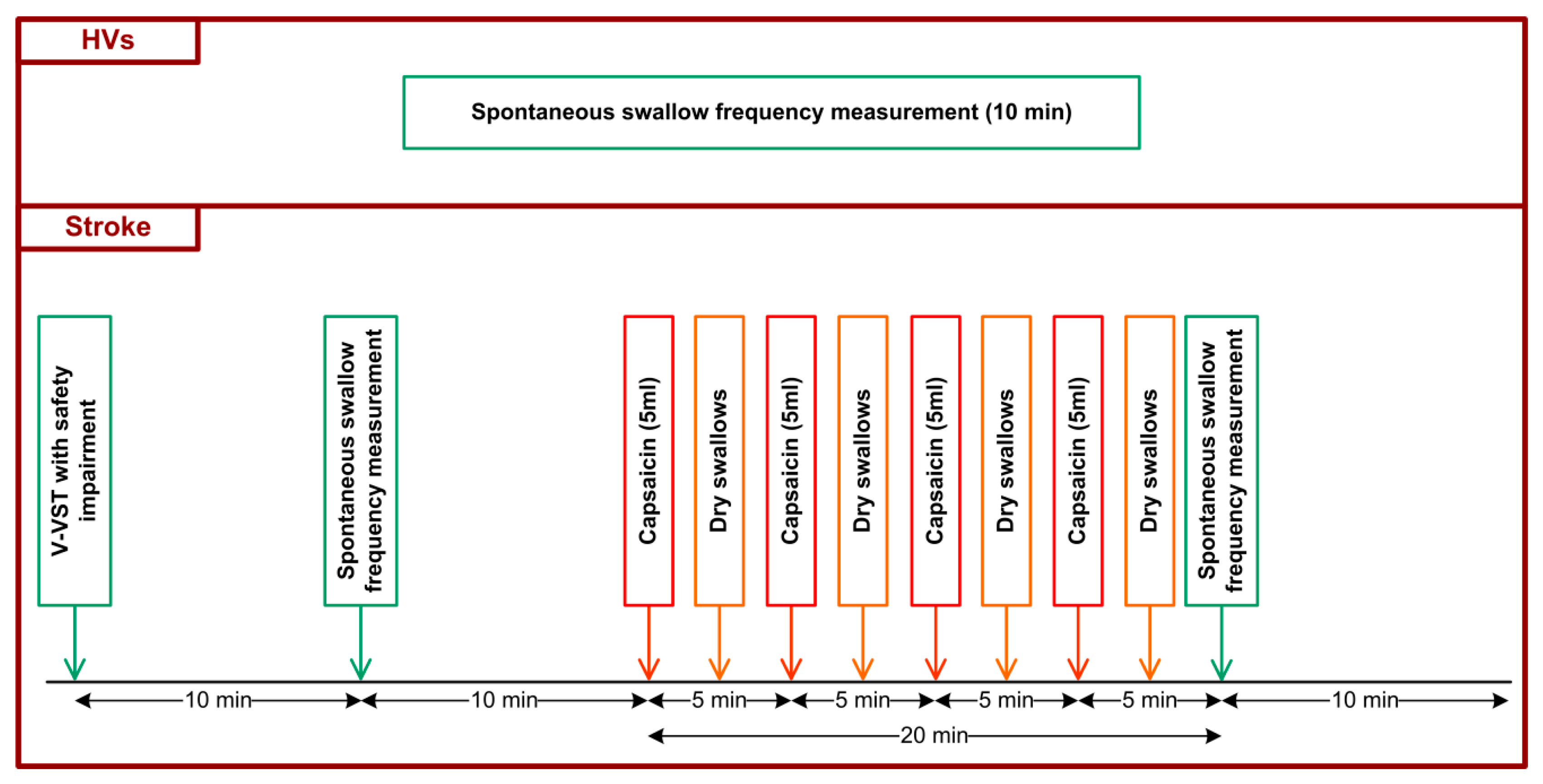
2.2. Experimental Design
2.3. Volume–Viscosity Swallowing Test (V-VST)
2.4. Spontaneous Swallow Frequency Recordings (SSF)
2.5. Intervention: Effect of Oropharyngeal Sensory Stimulation with TRPV1 Agonists
2.6. Data Analysis and Statistical Methods
3. Results
3.1. Study Population
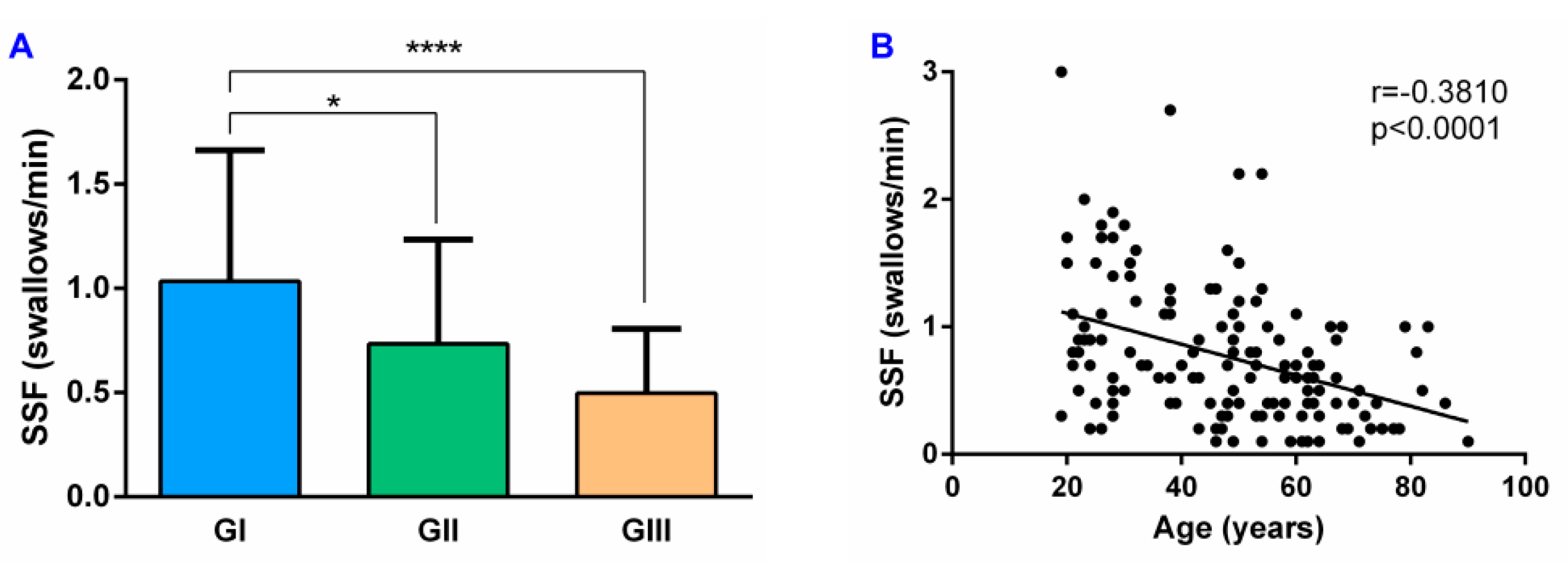
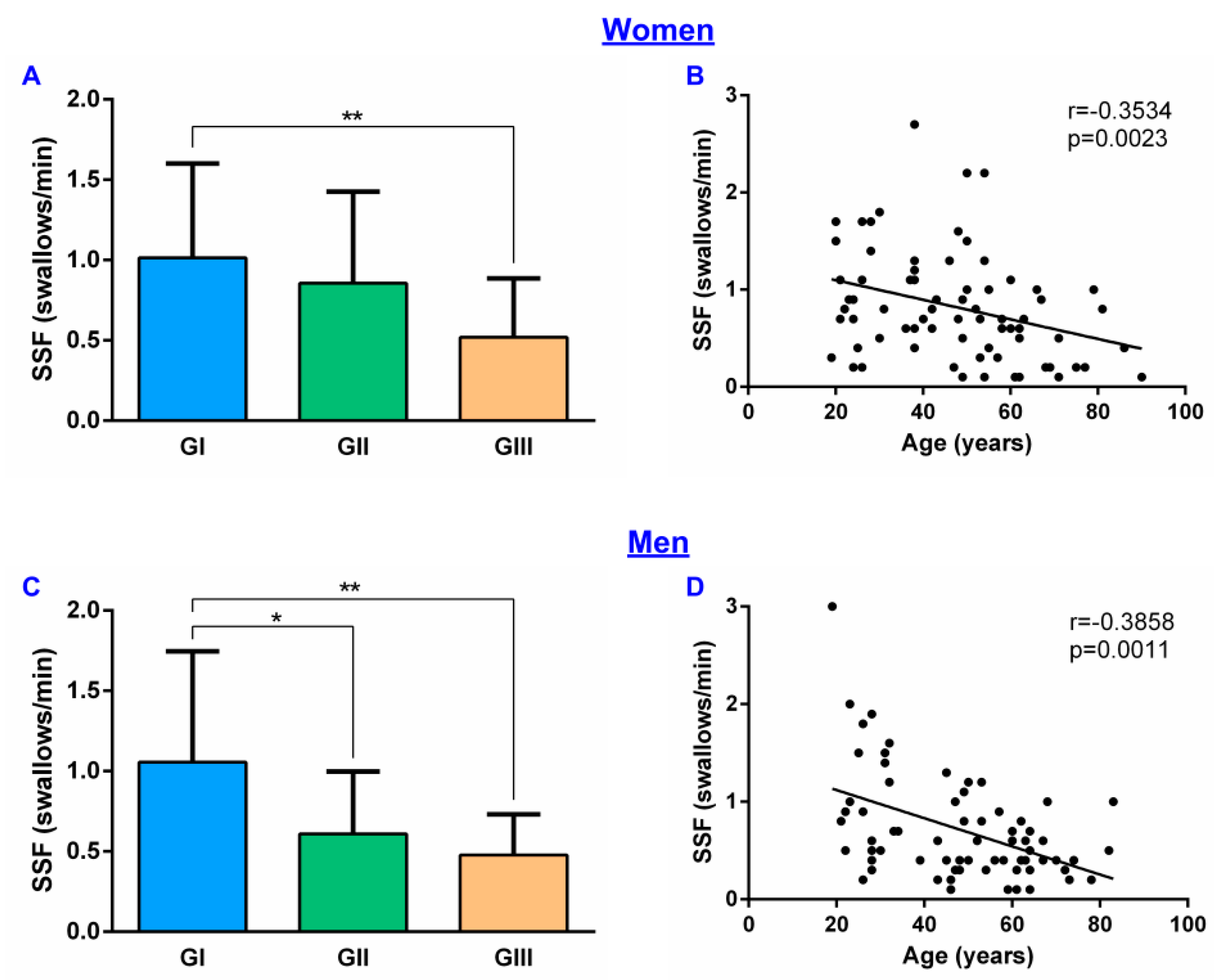
3.2. Basal SSF in HV and PSD Patients
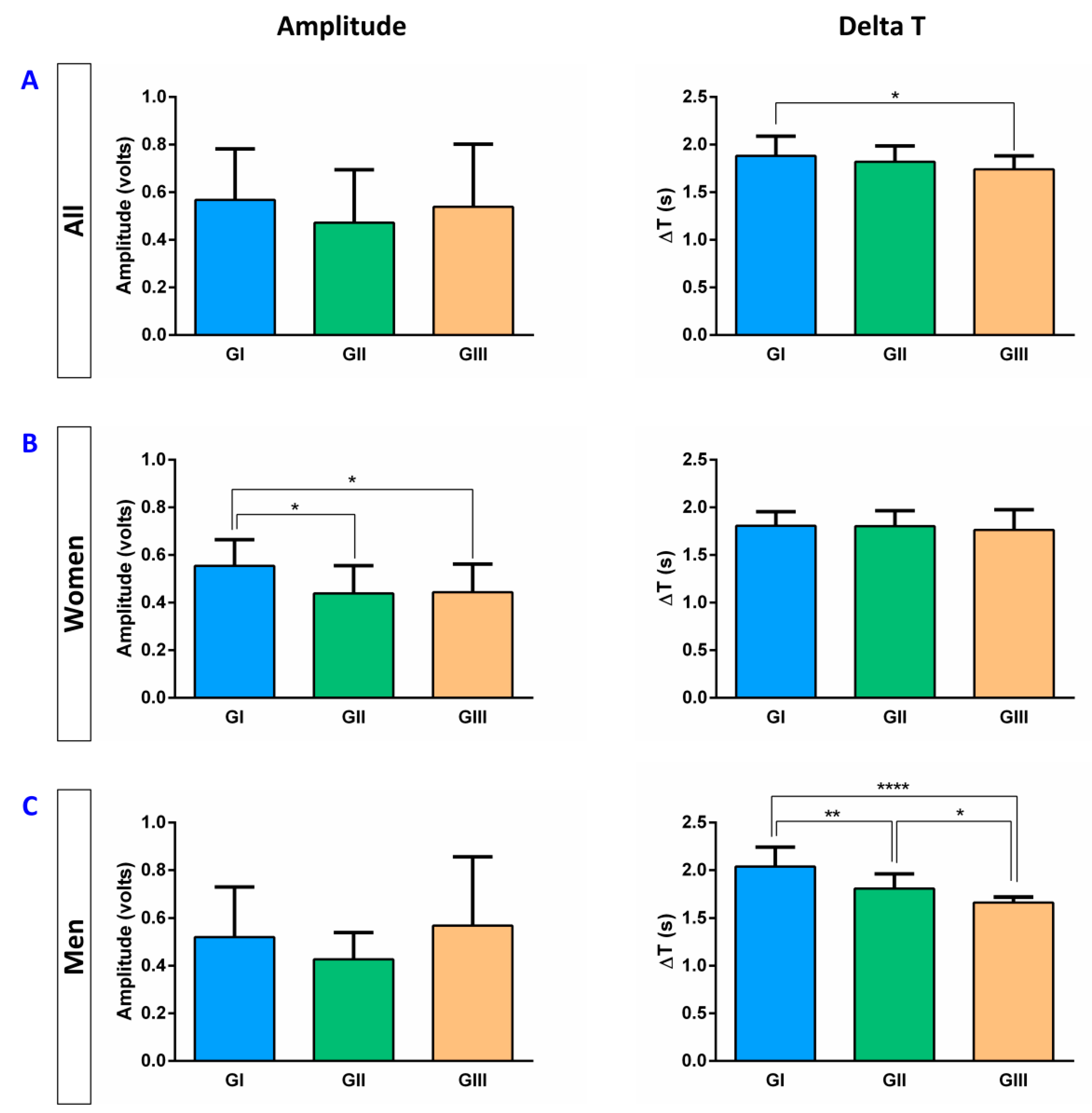
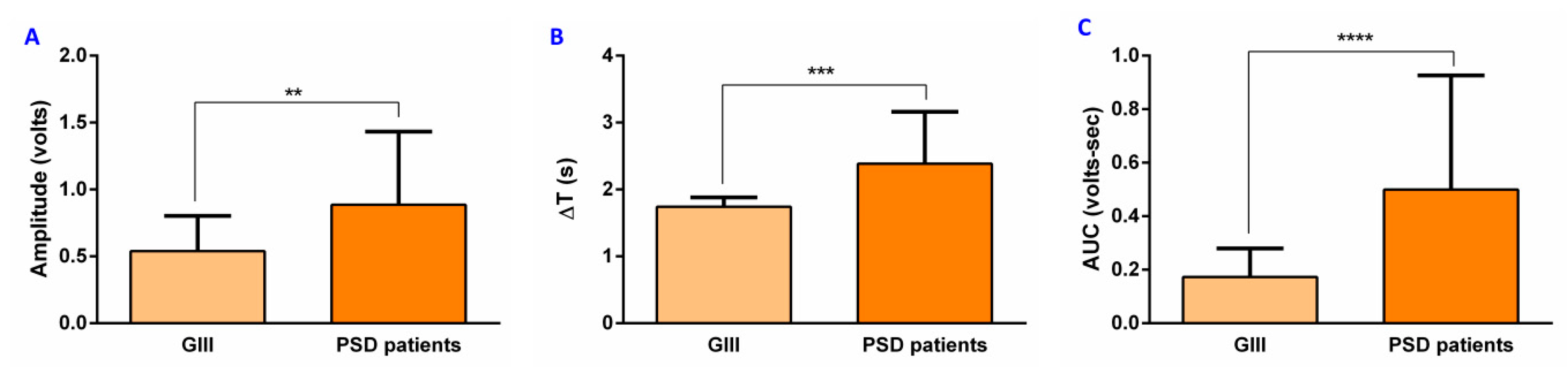
3.3. Basal EMG Metrics
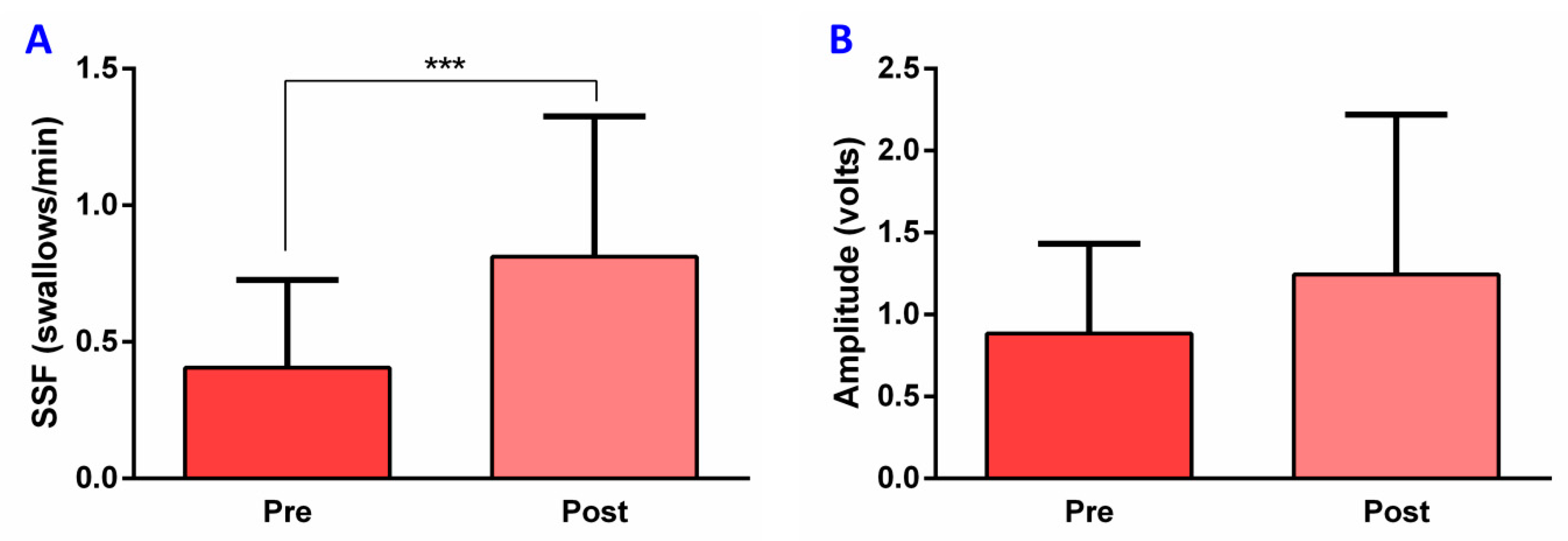
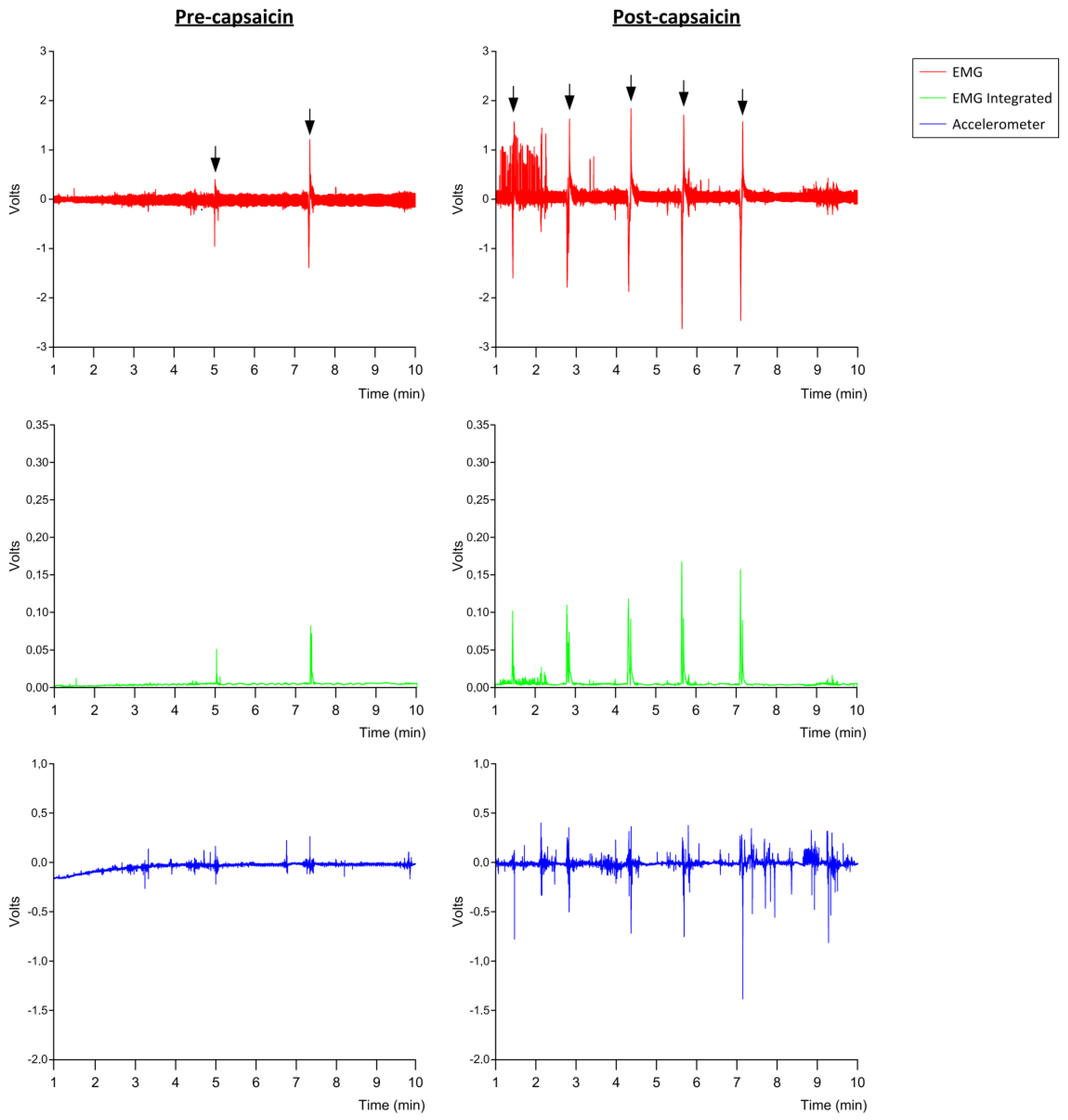
3.4. Effect of TRPV1 Stimulation on SSF and EMG Metrics in PSD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, J.; Langmore, S.E.; Ginsberg, S.; Dostie, A. The significance of accumulated oropharyngeal secretions and swallowing frequency in predicting aspiration. Dysphagia 1996, 11, 99–103. [Google Scholar] [CrossRef]
- Hamdy, S.; Mikulis, D.J.; Crawley, A.; Xue, S.; Lau, H.; Henry, S.; Diamant, N.E. Cortical activation during human volitional swallowing: An event- related fMRI study. Am. J. Physiol. 1999, 277. [Google Scholar] [CrossRef] [PubMed]
- Jean, A. Brain stem control of swallowing: Neuronal network and cellular mechanisms. Physiol. Rev. 2001, 81, 929–969. [Google Scholar] [CrossRef] [Green Version]
- Mosier, K.M.; Liu, W.C.; Maldjian, J.A.; Shah, R.; Modi, B. Lateralization of cortical function in swallowing: A functional MR imaging study. Am. J. Neuroradiol. 1999, 20, 1520–1526. [Google Scholar] [PubMed]
- Martin, R.E.; Goodyear, B.G.; Gati, J.S.; Menon, R.S. Cerebral cortical representation of automatic and volitional swallowing in humans. J. Neurophysiol. 2001, 85, 938–950. [Google Scholar] [CrossRef] [PubMed]
- Kamarunas, E.; Mulheren, R.; Palmore, K.; Ludlow, C. Timing of cortical activation during spontaneous swallowing. Exp. Brain Res. 2018, 236, 475–484. [Google Scholar] [CrossRef]
- Berardelli, A.; Accornero, N.; Cruccu, G.; Fabiano, F.; Guerrisi, V.; Manfredi, M. The orbicularis oculi response after hemispheral damage. J. Neurol. Neurosurg. Psychiatry 1983, 46, 837–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabib, C.; Llufriu, S.; Martinez-Heras, E.; Saiz, A.; Valls-Sole, J. Abnormal control of orbicularis oculi reflex excitability in multiple sclerosis. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Afkari, S. Measuring frequency of spontaneous swallowing. Australas. Phys. Eng. Sci. Med. 2007, 30, 313–317. [Google Scholar]
- Theurer, J.A.; Czachorowski, K.A.; Martin, L.P.; Martin, R.E. Effects of oropharyngeal air-pulse stimulation on swallowing in healthy older adults. Dysphagia 2009, 24, 302–313. [Google Scholar] [CrossRef]
- Crary, M.A.; Carnaby, G.D.; Sia, I.; Khanna, A.; Waters, M.F. Spontaneous swallowing frequency has potential to identify dysphagia in acute stroke. Stroke 2013, 44, 3452–3457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crary, M.A.; Carnaby, G.D.; Sia, I. Spontaneous swallow frequency compared with clinical screening in the identification of dysphagia in acute stroke. J. Stroke Cerebrovasc. Dis. 2014, 23, 2047–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niimi, M.; Hashimoto, G.; Hara, T.; Yamada, N.; Abo, M.; Fujigasaki, H.; Ide, T. Relationship Between Frequency of Spontaneous Swallowing and Salivary Substance P Level in Patients with Acute Stroke. Dysphagia 2018, 33, 414–418. [Google Scholar] [CrossRef]
- Alvarez-berdugo, D.; Rofes, L.; Casamitjana, J.F. Oropharyngeal and laryngeal sensory innervation in the pathophysiology of swallowing disorders and sensory stimulation treatments. Ann. N. Y. Acad. Sci. 2016, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Berdugo, D.; Rofes, L.; Farré, R.; Casamitjana, J.F.; Enrique, A.; Chamizo, J.; Padrón, A.; Navarro, X.; Clave, P. Localization and expression of TRPV1 and TRPA1 in the human oropharynx and larynx. Neurogastroenterol. Motil. 2016, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Canning, B.J.; Chang, A.B.; Bolser, D.C.; Smith, J.A.; Mazzone, S.B.; McGarvey, L. Anatomy and Neurophysiology of Cough: CHEST Guideline and Expert Panel Report. Chest 2014, 146, 1633–1648. [Google Scholar] [CrossRef] [Green Version]
- Rofes, L.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P. Spatiotemporal characteristics of the pharyngeal event-related potential in healthy subjects and older patients with oropharyngeal dysfunction. Neurogastroenterol. Motil. 2017, 29, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cabib, C.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P.; Rofes, L. Chronic post-stroke oropharyngeal dysphagia is associated with impaired cortical activation to pharyngeal sensory inputs. Eur. J. Neurol. 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Arreola, V.; Martin, A.; Clave, P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut 2014, 62, 1280–1287. [Google Scholar] [CrossRef]
- Wang, Z.; Wu, L.; Fang, Q.; Shen, M.; Zhang, L.; Liu, X. Effects of capsaicin on swallowing function in stroke patients with dysphagia: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Tomsen, N.; Ortega, O.; Rofes, L.; Arreola, V.; Martin, A.; Mundet, L.; Clavé, P. Acute and subacute effects of oropharyngeal sensory stimulation with TRPV1 agonists in older patients with oropharyngeal dysphagia: a biomechanical and neurophysiological randomized pilot study. Therap. Adv. Gastroenterol. 2019, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Oosterhout, W.P.J.; Schoonman, G.G.; Garrelds, I.M.; Danser, A.H.J.; Chan, K.Y.; Terwindt, G.M.; Ferrari, M.D.; Maassenvandenbrink, A. A human capsaicin model to quantitatively assess salivary CGRP secretion. Cephalalgia 2015, 35, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Nakato, R.; Manabe, N.; Shimizu, S.; Hanayama, K.; Shiotani, A.; Hata, J.; Haruma, K. Effects of Capsaicin on Older Patients with Oropharyngeal Dysphagia: A Double-Blind, Placebo-Controlled, Crossover Study. Digestion 2017, 95, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Clavé, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Samson, N.; Praud, J.P.; Quenet, B.; Similowski, T.; Straus, C. New insights into sucking, swallowing and breathing central generators: A complexity analysis of rhythmic motor behaviors. Neurosci. Lett. 2017, 638, 90–95. [Google Scholar] [CrossRef]
- Mortelliti, A.J.; Malmgren, L.T.; Gacek, R.R. Ultrastructural Changes With Age in the Human Superior Laryngeal Nerve. Arch. Otolaryngol. Neck Surg. 1990, 116, 1062–1069. [Google Scholar] [CrossRef]
- Moayedi, Y.; Duenas-Bianchi, L.F.; Lumpkin, E.A. Somatosensory innervation of the oral mucosa of adult and aging mice. Sci. Rep. 2018, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabré, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 1–9. [Google Scholar] [CrossRef]
- Vaiman, M.; Eviatar, E.; Segal, S. Surface electromyographic studies of swallowing in normal subjects: A review of 440 adults. Report 1. Quantitative data: Timing measures. Otolaryngol. Head Neck Surg. 2004, 131, 548–555. [Google Scholar] [CrossRef]
- Vaiman, M.; Eviatar, E.; Segal, S. Surface electromyographic studies of swallowing in normal subjects: A review of 440 adults. Report 2. Quantitative data: Amplitude measures. Otolaryngol. Head Neck Surg. 2004, 131, 773–780. [Google Scholar] [CrossRef]
- Sakai, K.; Nakayama, E.; Rogus-Pulia, N.; Takehisa, T.; Takehisa, Y.; Urayama, K.Y.; Takahashi, O. Submental muscle activity and its role in diagnosing sarcopenic dysphagia. Clin. Interv. Aging 2020, 15, 1991–1999. [Google Scholar] [CrossRef] [PubMed]
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Vilardell, N.; Arreola, L.R.V.; Muriana, A.M.D.; Clavé, P. Videofluoroscopic assessment of the pathophysiology of chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2017, 1–8. [Google Scholar] [CrossRef]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Muriana, D.; Palomeras, E.; Michou, E.; Clavé, P.; et al. Neurophysiological and Biomechanical Evaluation of the Mechanisms Which Impair Safety of Swallow in Chronic Post-stroke Patients. Transl. Stroke Res. 2019, 11, 16–28. [Google Scholar] [CrossRef]
- Nordander, C.; Willner, J.; Hansson, G.Å.; Larsson, B.; Unge, J.; Granquist, L.; Skerfving, S. Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers and BMI, on the EMG amplitude. Eur. J. Appl. Physiol. 2003, 89, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Suntrup-Krueger, S.; Muhle, P.; Kampe, I.; Egidi, P.; Ruck, T.; Lenze, F.; Jungheim, M.; Gminski, R.; Labeit, B.; Claus, I.; et al. Effect of Capsaicinoids on Neurophysiological, Biochemical, and Mechanical Parameters of Swallowing Function. Neurotherapeutics 2021. [Google Scholar] [CrossRef]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Palomeras, E.; Michou, E.; Clavé, P.; Ortega, O. Short-term neurophysiological effects of sensory pathway neurorehabilitation strategies on chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32, 1–14. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, W.; Tomsen, N.; Acedo, S.; Campos-Alcantara, C.; Cabib, C.; Alvarez-Larruy, M.; Clavé, P. Effect of Aging, Gender and Sensory Stimulation of TRPV1 Receptors with Capsaicin on Spontaneous Swallowing Frequency in Patients with Oropharyngeal Dysphagia: A Proof-of-Concept Study. Diagnostics 2021, 11, 461. https://doi.org/10.3390/diagnostics11030461
Nascimento W, Tomsen N, Acedo S, Campos-Alcantara C, Cabib C, Alvarez-Larruy M, Clavé P. Effect of Aging, Gender and Sensory Stimulation of TRPV1 Receptors with Capsaicin on Spontaneous Swallowing Frequency in Patients with Oropharyngeal Dysphagia: A Proof-of-Concept Study. Diagnostics. 2021; 11(3):461. https://doi.org/10.3390/diagnostics11030461
Chicago/Turabian StyleNascimento, Weslania, Noemí Tomsen, Saray Acedo, Cristina Campos-Alcantara, Christopher Cabib, Marta Alvarez-Larruy, and Pere Clavé. 2021. "Effect of Aging, Gender and Sensory Stimulation of TRPV1 Receptors with Capsaicin on Spontaneous Swallowing Frequency in Patients with Oropharyngeal Dysphagia: A Proof-of-Concept Study" Diagnostics 11, no. 3: 461. https://doi.org/10.3390/diagnostics11030461
APA StyleNascimento, W., Tomsen, N., Acedo, S., Campos-Alcantara, C., Cabib, C., Alvarez-Larruy, M., & Clavé, P. (2021). Effect of Aging, Gender and Sensory Stimulation of TRPV1 Receptors with Capsaicin on Spontaneous Swallowing Frequency in Patients with Oropharyngeal Dysphagia: A Proof-of-Concept Study. Diagnostics, 11(3), 461. https://doi.org/10.3390/diagnostics11030461