
Validity and Reliability of the Helkimo Clinical Dysfunction Index for the Diagnosis of Temporomandibular Disorders


 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Statistical Analysis
3. Results
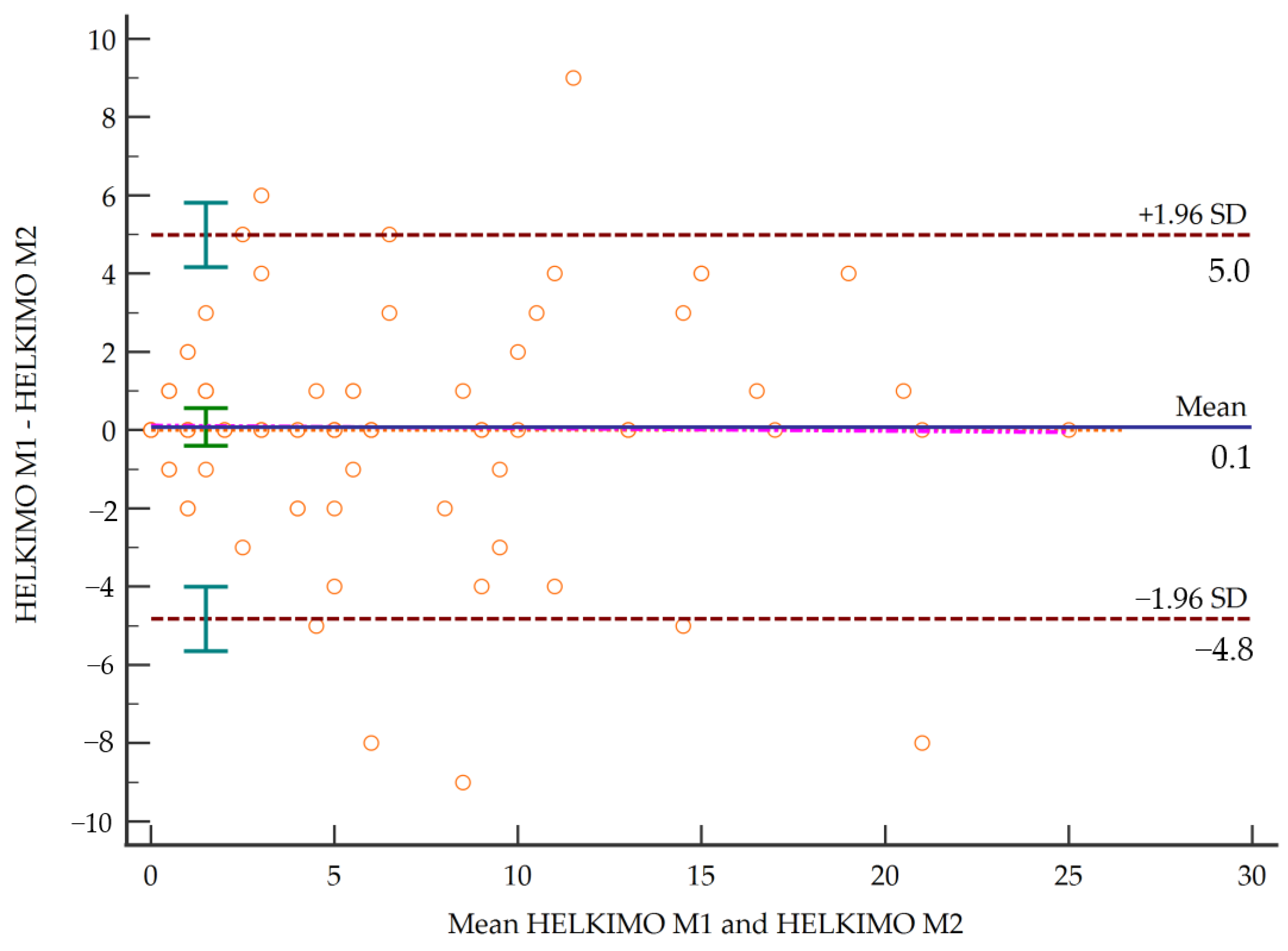
3.1. Inter-Rater Reliability
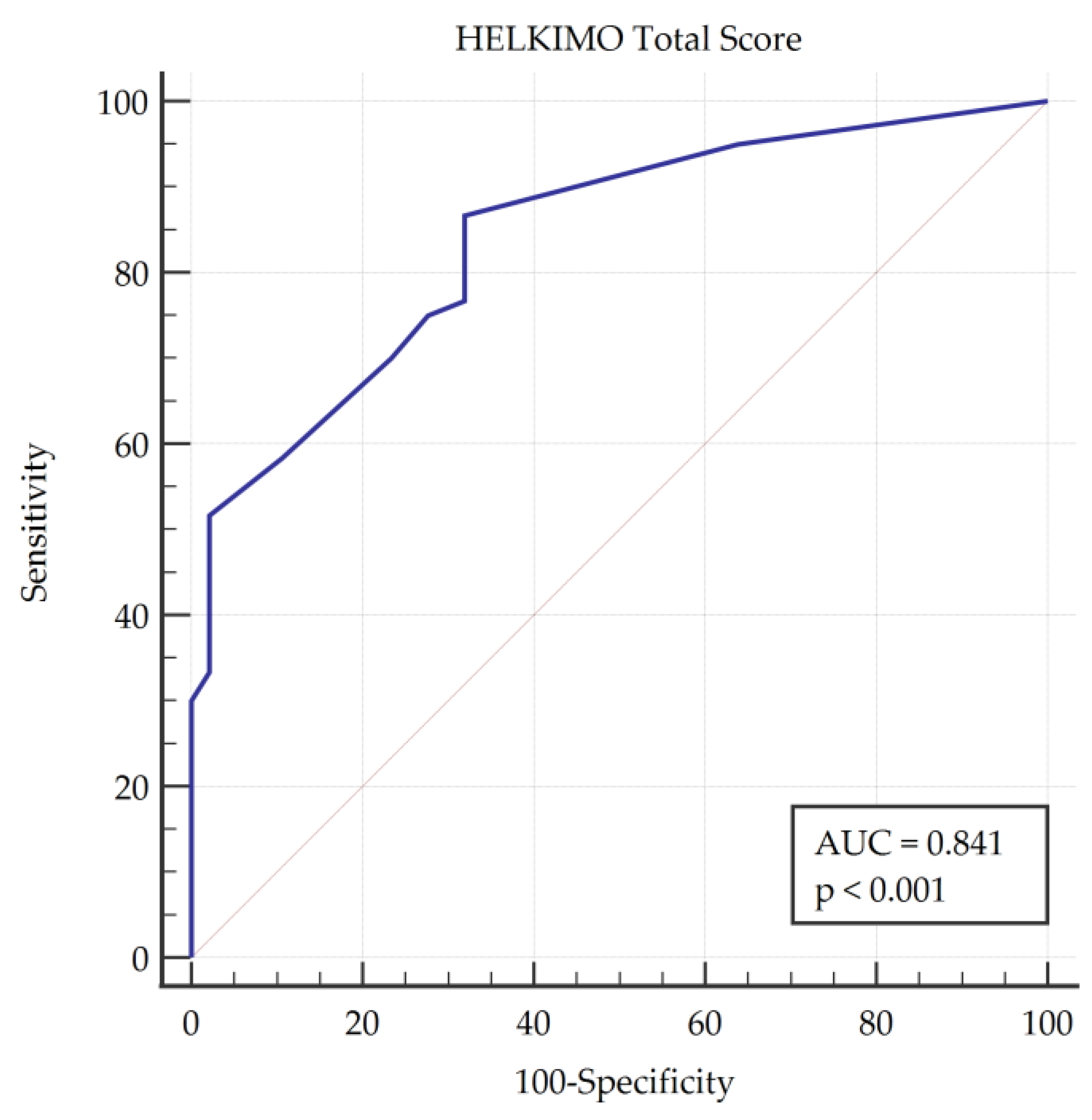
3.2. Validity and Accuracy of the TMD Diagnostic Ability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paduano, S.; Bucci, R.; Rongo, R.; Silva, R.; Michelotti, A. Prevalence of temporomandibular disorders and oral parafunctions in adolescents from public schools in Southern Italy. Cranio J. Craniomandib. Pract. 2020, 38, 370–375. [Google Scholar] [CrossRef]
- Perez, C.V.; De Leeuw, R.; Okeson, J.P.; Carlson, C.R.; Li, H.F.; Bush, H.M.; Falace, D.A. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath 2013, 17, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Nieto Fernández-Pacheco, M.J. Análisis de los Costes Producidos por una Incorrecta Derivación de Pacientes con Síndrome de Disfunción Temporomandibular; Universidad Autónoma de Madrid: Madrid, Spain, 2017. [Google Scholar]
- Ibi, M. Inflammation and temporomandibular joint derangement. Biol. Pharm. Bull. 2019, 42, 538–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral superior condylar neck fracture with dislocation in a child treated with an acrylic splint in the upper arch for functional repositioning of the mandible. Cranio J. Craniomandib. Pract. 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Oh, N.; Kim, I.K. A follow-up study of condyle fracture in children. Int. J. Oral Maxillofac. Surg. 2005, 34, 851–858. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Reade, P.C.; Kemppainen, P.; Könönen, M.; Dworkin, S.F. Review of aetiological concepts of temporomandibular pain disorders: Towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur. J. Pain 2005, 9, 613. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Von Piekartz, H. Clinical reasoning for the examination and physical therapy treatment of temporomandibular disorders (TMD): A narrative literature review. J. Clin. Med. 2020, 9, 3686. [Google Scholar] [CrossRef]
- Eberhard, D. The efficacy of anterior repositioning splint therapy studied by magnetic resonance imaging. Eur. J. Orthod. 2002, 24, 343–352. [Google Scholar] [CrossRef]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular disc displacement with reduction treated with anterior repositioning splint: A 2-year clinical and magnetic resonance imaging (MRI) follow-up. J. Biol. Regul. Homeost. Agents 2020, 34, 151–160. [Google Scholar] [PubMed]
- Canter, H.I.; Kayikcioglu, A.; Aksu, M.; Mavili, M.E. Botulinum toxin in closed treatment of mandibular condylar fracture. Ann. Plast. Surg. 2007, 58, 474–478. [Google Scholar] [CrossRef]
- Fayed, M.; El-Mangoury, N.; El-Bpkle, D.; Belal, A. Occlusal splint therapy and magnetic resonance imaging. Worlf J. Orthod. 2004, 5, 133–140. [Google Scholar]
- Moccia, S.; Nucci, L.; Spagnuolo, C.; d’Apuzzo, F.; Piancino, M.G.; Minervini, G. Polyphenols as potential agents in the management of temporomandibular disorders. Appl. Sci. 2020, 10, 5305. [Google Scholar] [CrossRef]
- Ting, J.; Li, J.; Zhen Kang, S. A primary research on the concomitant syntoms of temporomandibular joint pain. Zhonghua Kou Qiang Yi Xue Za Zhi 2005, 40, 219–222. [Google Scholar]
- Katsoulis, K.; Bassetti, R.; Windecker Getaz, I.; Mericske Stern, R.; Katsoulis, J. Temporomandibular disorders/myoarthropathy of the masticatory system. Res. Sci. 2012, 122, 510–518. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Rani, S.; Pawah, S.; Gola, S.; Bakshi, M. Analysis of Helkimo index for temporomandibular disorder diagnosis in the dental students of Faridabad city: A cross-sectional study. J. Indian Prosthodont. Soc. 2017, 17, 48–52. [Google Scholar] [CrossRef]
- Suhas, S.; Ramdas, S.; Lingam, P.; Naveen Kumar, H.; Sasidharan, A.; Aadithya, R. Assessment of temporomandibular joint dysfunction in condylar fracture of the mandible using the Helkimo index. Indian J. Plast. Surg. 2017, 50, 207–212. [Google Scholar] [CrossRef]
- Nokar, S.; Sadighpour, L.; Shirzad, H.; Shahrokhi Rad, A.; Keshvad, A. Evaluation of signs, symptoms, and occlusal factors among patients with temporomandibular disorders according to Helkimo index. Cranio J. Craniomandib. Pract. 2019, 37, 383–388. [Google Scholar] [CrossRef]
- Fu, K.; Ma, X.; Zhang, Z.; Tian, Y.; Zhou, Y.; Zhao, Y. Study on the use of temporomandibular joint dysfunction index in temporomandibular disorders-PubMed. Zhonghua Kou Qiang Yi Xue Za Zhi 2002, 37, 320–322. [Google Scholar]
- John, M.; Zwijnenburg, A. Interobserver variability in assessment of signs of TMD-PubMed. Int. J. Prosthodont. 2001, 14, 265–270. [Google Scholar]
- Abud, M.C.; Figueiredo, M.D.; dos Santos, M.B.F.; Consani, R.L.X.; Marchini, L. Correlation of prosthetic status with the GOHAI and TMD indices-PubMed. Eur. J. Prosthodont. Rest. Dent. 2011, 19, 38–42. [Google Scholar]
- Pocock, P.R.; Mamandras, A.H.; Bellamy, N. Evaluation of an anamnestic questionnaire as an instrument for investigating potential relationships between orthodontic therapy and temporomandibular disorders. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 239–243. [Google Scholar] [CrossRef]
- Hobart, J.C.; Cano, S.J.; Warner, T.T.; Thompson, A.J. What sample sizes for reliability and validity studies in neurology? J. Neurol. 2012, 259, 2681–2694. [Google Scholar] [CrossRef]
- World Health Organization. 2013–2020 Global Action Plan for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Duinkerke, A.S.H.; Luteijn, F.; Bouman, T.K.; Jong, H.P. Reproducibility of a palpation test for the stomatognathic system. Community Dent. Oral Epidemiol. 1986, 14, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, S.C.; Nogueira, R.V.B.; Duarte, Â.P.; Vasconcelos, B.C.D.E.; Almeida, R.D.A.C. Análise dos índices de Helkimo e craniomandibular para diagnóstico de desordens temporomandibulares em pacientes com artrite reumatóide. Braz. J. Otorhinolaryngol. 2007, 73, 19–26. [Google Scholar] [CrossRef] [Green Version]
- van der Weele, L.T.; Dibbets, J.M.H. Helkimo’s index: A scale or just a set of symptoms? J. Oral Rehabil. 1987, 14, 229–237. [Google Scholar] [CrossRef]
- Rodrigues-Bigaton, D.; de Castro, E.M.; Pires, P.F. Factor and Rasch analysis of the Fonseca anamnestic index for the diagnosis of myogenous temporomandibular disorder. Braz. J. Phys. Ther. 2017, 21, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Torrelo, C.; Zagalaz-Anula, N.; Alonso-Royo, R.; Ibáñez-Vera, A.; López-Collantes, J.; Rodríguez-Almagro, D.; Obrero-Gaitán, E.; Lomas-Vega, R. Transcultural adaptation and validation of the Fonseca Anamnestic Index in a Spanish population with temporomandibular disorders. J. Clin. Med. 2020, 9, 3230. [Google Scholar] [CrossRef] [PubMed]
- Pires, P.F.; de Castro, E.M.; Pelai, E.B.; de Arruda, A.B.C.; Rodrigues-Bigaton, D. Analysis of the accuracy and reliability of the Short-Form Fonseca Anamnestic Index in the diagnosis of myogenous temporomandibular disorder in women. Braz. J. Phys. Ther. 2018, 22, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Castarlenas, E.; Roy, R.; Tomé Pires, C.; Racine, M.; Pathak, A.; Miró, J. The utility and construct validity of four measures of pain intensity: Results from a University-Based Study in Spain. Pain Med. 2019, 20, 2411–2420. [Google Scholar] [CrossRef]
- Andrade Ortega, J.A.; Delgado Martínez, A.D.; Almécija Ruiz, R. Validation of a Spanish version of the Neck Disability Index. Spine 2010, 35, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, G.P.; Newman, C.W. The Development of the Dizziness Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 425–427. [Google Scholar] [CrossRef]
- Perez, N.; Garmendia, I.; García-Granero, M.; Martin, E.; García-Tapia, R. Factor analysis and correlation between Dizziness Handicap Inventory and Dizziness Characteristics and Impact on Quality of Life Scales. Acta Oto-Laryngol. Suppl. 2001, 545, 145–154. [Google Scholar]
- Pérez, N.; Garmendia, I.; Martín, E.; García-Tapia, R. Cultural adaptation of 2 questionnaires for health measurements in patients with vertigo. Acta Otorrinolaringol. Esp. 2000, 51, 572–580. [Google Scholar]
- Martin, M.; Blaisdell, B.; Kwong, J.W.; Bjorner, J.B. The Short-Form Headache Impact Test (HIT-6) was psychometrically equivalent in nine languages. J. Clin. Epidemiol. 2004, 57, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Kliebsch, U. Dependence of weighted kappa coefficients on the number of categories. Epidemiology 1996, 7, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.; Koch, G.G. The measurement of the observer agreement for categorial data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciencies, 2nd ed.; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1998; ISBN 0805802835. [Google Scholar]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef] [PubMed]
- Swets, J. Measuring the accuracy of diagnostic information. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Ciencia e Innovación de España Estadística de Estudiantes. Available online: https://www.ciencia.gob.es/portal/site/MICINN/menuitem.7eeac5cd345b4f34f09dfd1001432ea0/?vgnextoid=0930dd449de8b610VgnVCM1000001d04140aRCRD (accessed on 3 October 2020).
- de Santis, T.O.; Motta, L.J.; Biasotto-Gonzalez, D.A.; Mesquita-Ferrari, R.A.; Fernandes, K.P.S.; de Godoy, C.H.L.; Alfaya, T.A.; Bussadori, S.K. Accuracy study of the main screening tools for temporomandibular disorder in children and adolescents. J. Bodyw. Mov. Ther. 2014, 18, 87–91. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All | n = 107 | Healthy | n = 47 | Temporomandibular Disorders (TMDs) | n = 60 | ||
|---|---|---|---|---|---|---|---|
| Weight (kilograms) | 72.83 | 17.05 | 77.86 | 19.22 | 68.90 | 14.07 | |
| Height (meters) | 1.63 | 0.09 | 1.65 | 0.09 | 1.61 | 0.07 | |
| Body mass index | 27.48 | 6.91 | 28.48 | 7.10 | 26.69 | 6.72 | |
| Age (years) | 46.25 | 13.88 | 49.66 | 14.56 | 43.53 | 12.79 | |
| Sex | Female | 83 | 77.6 | 27 | 57.45 | 56 | 93.3 |
| Male | 24 | 22.4 | 20 | 42.55 | 4 | 6.7 | |
| Study level | Primary | 19 | 17.8 | 12 | 25.53 | 7 | 11.7 |
| Secondary | 52 | 48.6 | 25 | 53.19 | 27 | 45.0 | |
| University | 36 | 33.6 | 10 | 21.28 | 26 | 43.3 | |
| Physical activity | No | 45 | 42.1 | 19 | 40.43 | 26 | 43.3 |
| Yes | 62 | 57.9 | 28 | 59.57 | 34 | 56.7 | |
| Economic level | <€20.000 | 62 | 57.9 | 29 | 61.70 | 33 | 55.0 |
| >€20.000 | 45 | 42.1 | 18 | 38.30 | 27 | 45.0 | |
| Smoker | No | 69 | 64.5 | 28 | 59.57 | 41 | 68.3 |
| Yes | 13 | 12.1 | 6 | 12.77 | 7 | 11.7 | |
| Occasional | 12 | 11.2 | 6 | 12.77 | 6 | 10.0 | |
| Ex-smoker | 13 | 12.1 | 7 | 14.89 | 6 | 10.0 | |
| Drinker | No | 38 | 35.5 | 19 | 40.43 | 19 | 31.7 |
| Regular drinker | 6 | 5.6 | 3 | 6.38 | 3 | 5.0 | |
| Occasional | 63 | 58.9 | 25 | 53.19 | 38 | 63.3 |
| Measure | Value | 95% Confidence Interval | Degree of Concordance |
|---|---|---|---|
| Item A1 | 0.62548 | 0.48243 to 0.76853 | Substantial |
| Item A2 | 0.42641 | 0.20367 to 0.64916 | Moderate |
| Item A3 | 0.51430 | 0.31876 to 0.70983 | Moderate |
| Item A4 | 0.64430 | 0.52330 to 0.76529 | Substantial |
| Item A | 0.61987 | 0.49568 to 0.74407 | Substantial |
| Item B | 0.51661 | 0.37930 to 0.65391 | Moderate |
| Item C | 0.77395 | 0.66415 to 0.88375 | Substantial |
| Item D | 0.75750 | 0.65350 to 0.86149 | Substantial |
| Item E | 0.72116 | 0.60305 to 0.83926 | Substantial |
| Total score | 0.9053 | 0.8642 to 0.9345 | Excellent |
| Variable | Pearson’s r | p-Value | Correlation |
|---|---|---|---|
| Fonseca Anamnestic Index | 0.692 | <0.001 | Strong |
| Short Form of the Fonseca Anamnestic Index | 0.626 | <0.001 | Strong |
| Numerical Pain-Rating Scale Orofacial | 0.777 | <0.001 | Strong |
| Numerical Pain-Rating Scale Neck Pain | 0.302 | 0.002 | Moderate |
| Neck Disability Index | 0.265 | 0.006 | Poor |
| Dizziness Handicap Inventory Functional | 0.276 | 0.004 | Poor |
| Dizziness Handicap Inventory Emotional | 0.301 | 0.002 | Moderate |
| Dizziness Handicap Inventory Physical | 0.339 | <0.001 | Moderate |
| Dizziness Handicap Inventory Total | 0.339 | <0.001 | Moderate |
| Headache Impact Test 6 items | 0.187 | 0.054 | Poor |
| Physical Component Summary SF-12 | 0.003 | 0.975 | Poor |
| Mental Component Summary SF-12 | −0.171 | 0.078 | Poor |
| Sensitivity | 95% CI | Specificity | 95% CI | +LR | 95% CI | -LR | 95% CI | +PV | 95% CI | -PV | 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 86.67% | 75.4–94.1 | 68.09% | 52.9–80.9 | 2.72 | 1.8–4.2 | 0.20 | 0.10–0.4 | 77.6 | 69.3–84.2 | 80.0 | 67.1–88.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Royo, R.; Sánchez-Torrelo, C.M.; Ibáñez-Vera, A.J.; Zagalaz-Anula, N.; Castellote-Caballero, Y.; Obrero-Gaitán, E.; Rodríguez-Almagro, D.; Lomas-Vega, R. Validity and Reliability of the Helkimo Clinical Dysfunction Index for the Diagnosis of Temporomandibular Disorders. Diagnostics 2021, 11, 472. https://doi.org/10.3390/diagnostics11030472
Alonso-Royo R, Sánchez-Torrelo CM, Ibáñez-Vera AJ, Zagalaz-Anula N, Castellote-Caballero Y, Obrero-Gaitán E, Rodríguez-Almagro D, Lomas-Vega R. Validity and Reliability of the Helkimo Clinical Dysfunction Index for the Diagnosis of Temporomandibular Disorders. Diagnostics. 2021; 11(3):472. https://doi.org/10.3390/diagnostics11030472
Chicago/Turabian StyleAlonso-Royo, Roger, Carmen María Sánchez-Torrelo, Alfonso Javier Ibáñez-Vera, Noelia Zagalaz-Anula, Yolanda Castellote-Caballero, Esteban Obrero-Gaitán, Daniel Rodríguez-Almagro, and Rafael Lomas-Vega. 2021. "Validity and Reliability of the Helkimo Clinical Dysfunction Index for the Diagnosis of Temporomandibular Disorders" Diagnostics 11, no. 3: 472. https://doi.org/10.3390/diagnostics11030472
APA StyleAlonso-Royo, R., Sánchez-Torrelo, C. M., Ibáñez-Vera, A. J., Zagalaz-Anula, N., Castellote-Caballero, Y., Obrero-Gaitán, E., Rodríguez-Almagro, D., & Lomas-Vega, R. (2021). Validity and Reliability of the Helkimo Clinical Dysfunction Index for the Diagnosis of Temporomandibular Disorders. Diagnostics, 11(3), 472. https://doi.org/10.3390/diagnostics11030472