
Diagnostic Role of Four-Dimensional Computed Tomography for Preoperative Parathyroid Localization in Patients with Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
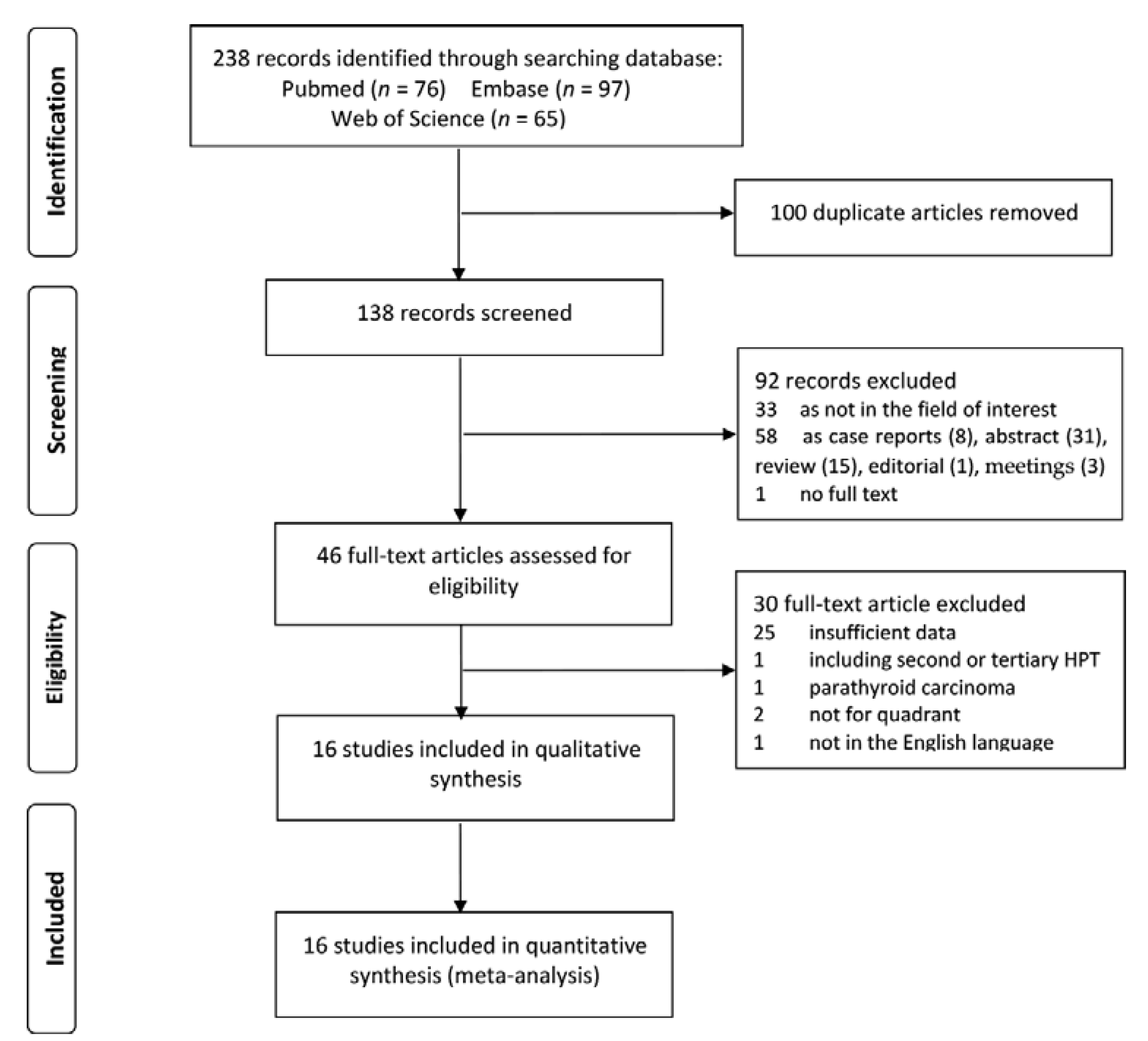
3.1. Literature Search
3.2. Characteristics of the Included Studies
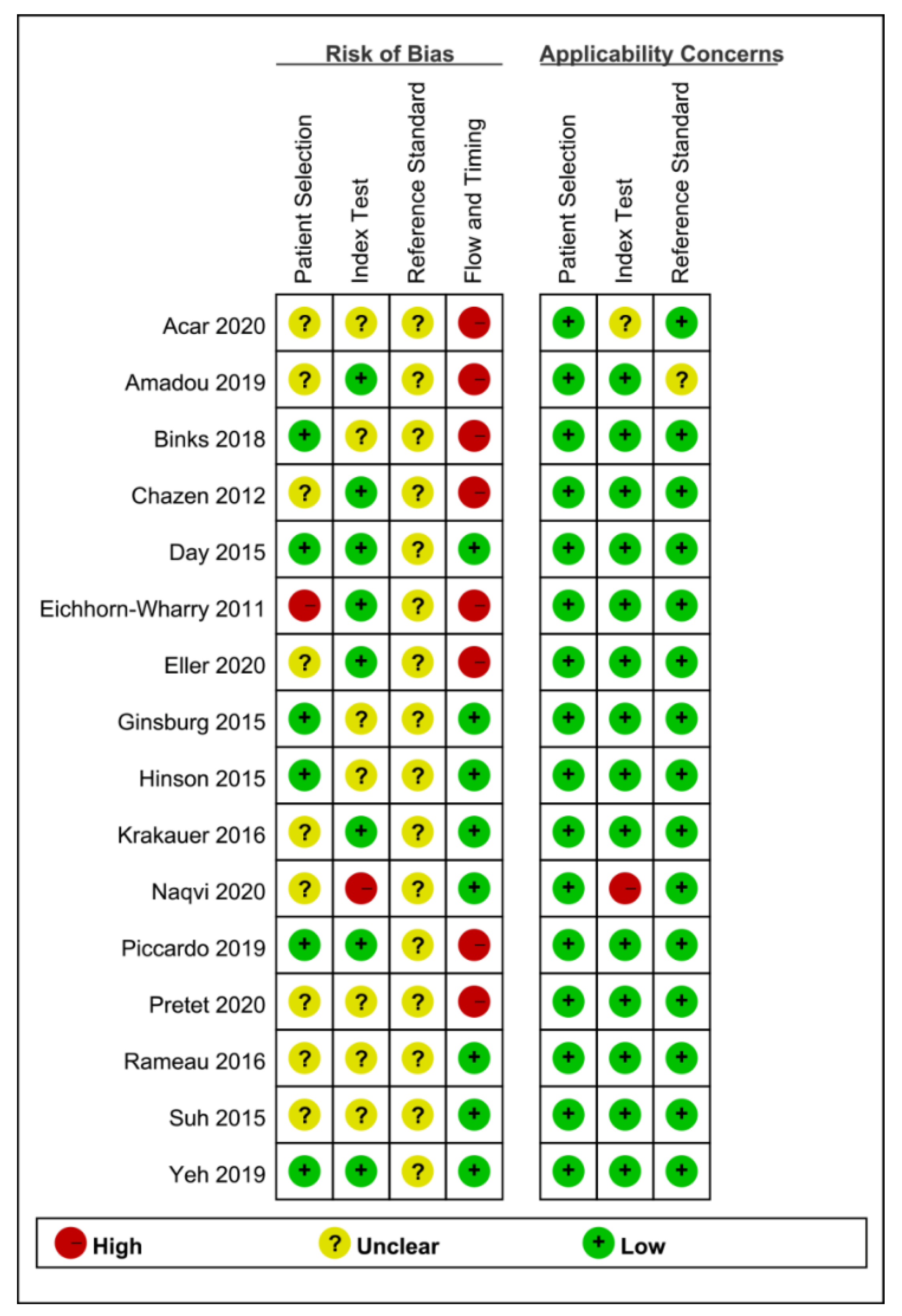
3.3. Quality Assessment
3.4. Summary of 4D-CT’s Diagnostic Performance
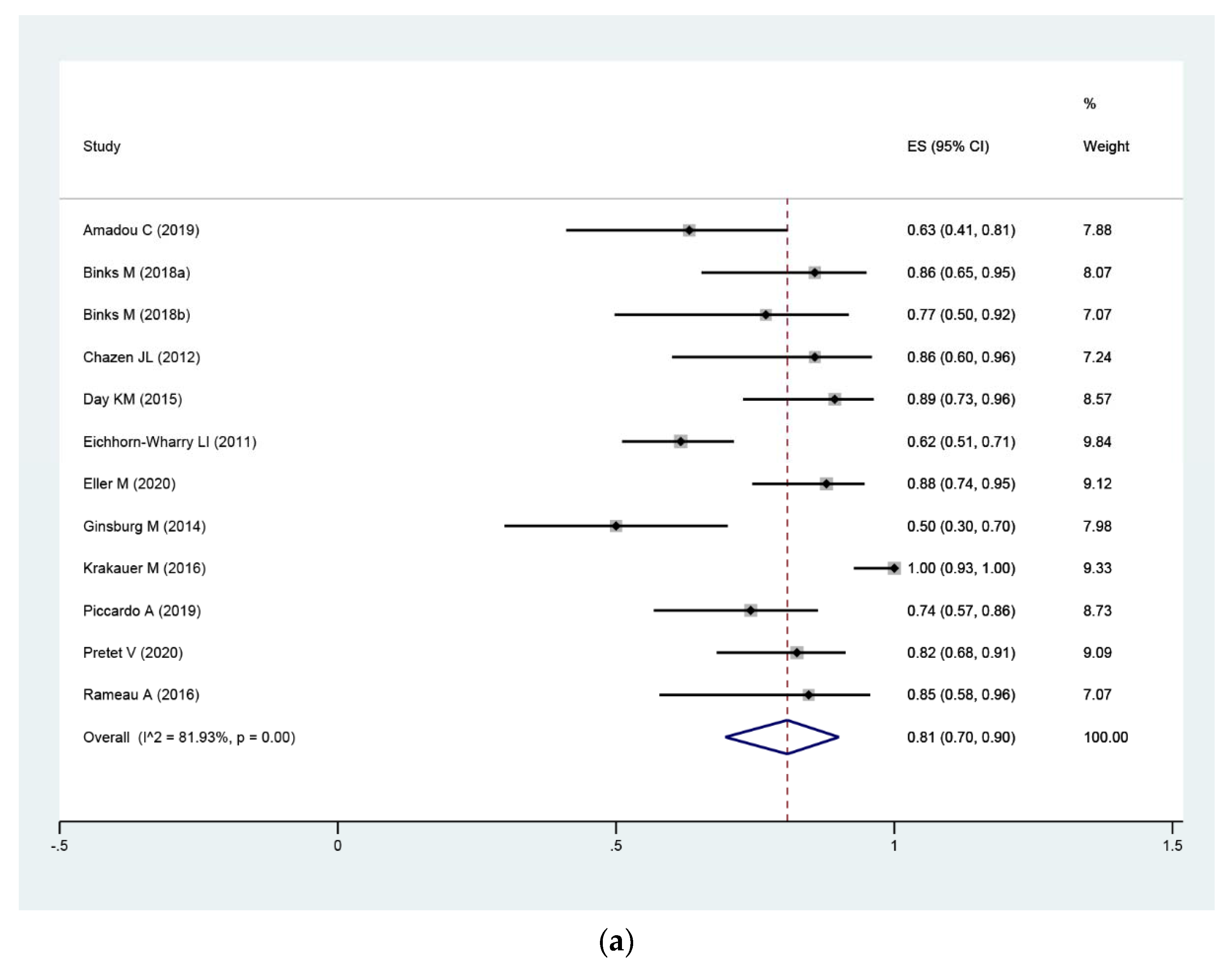
3.4.1. Per-Lesion Level Analysis
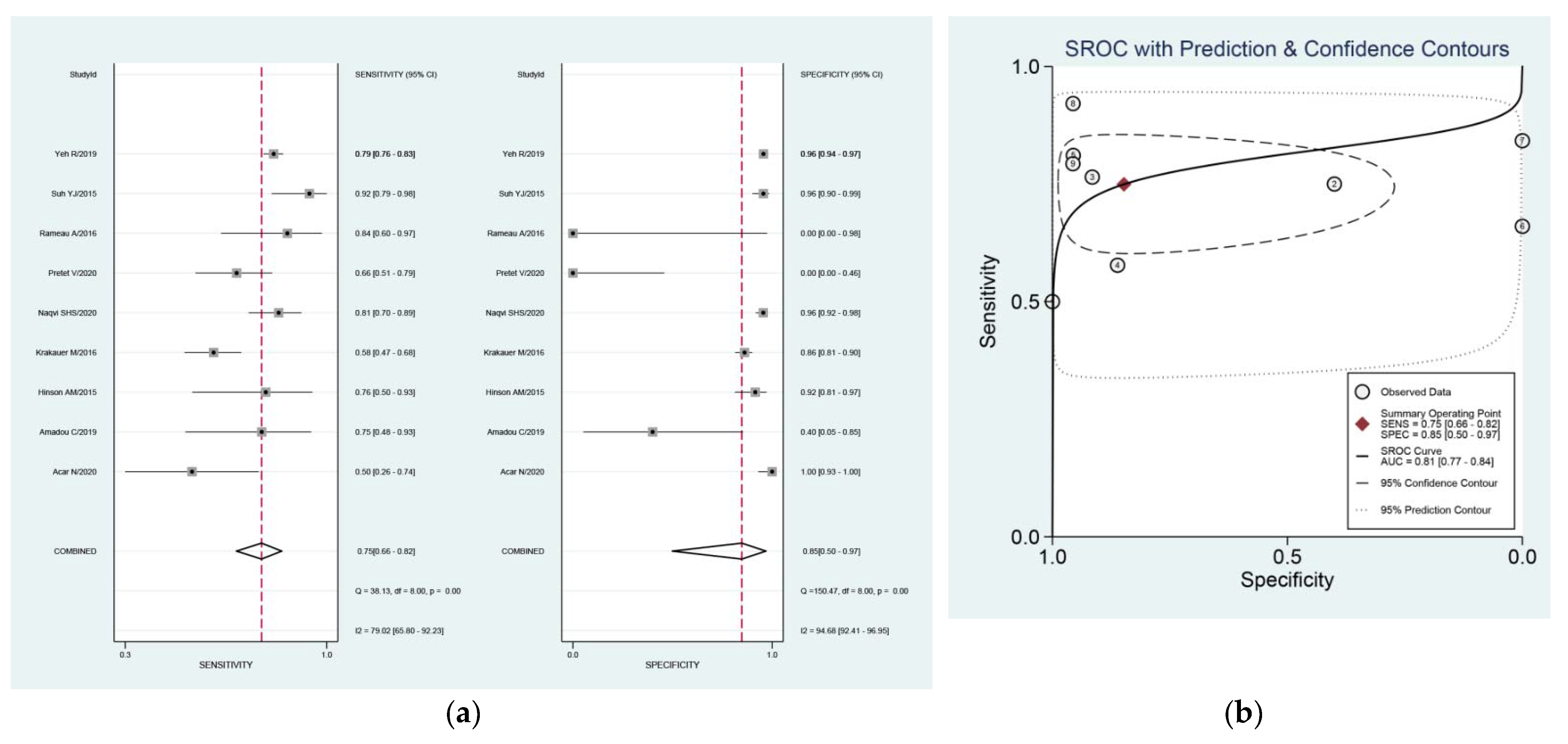
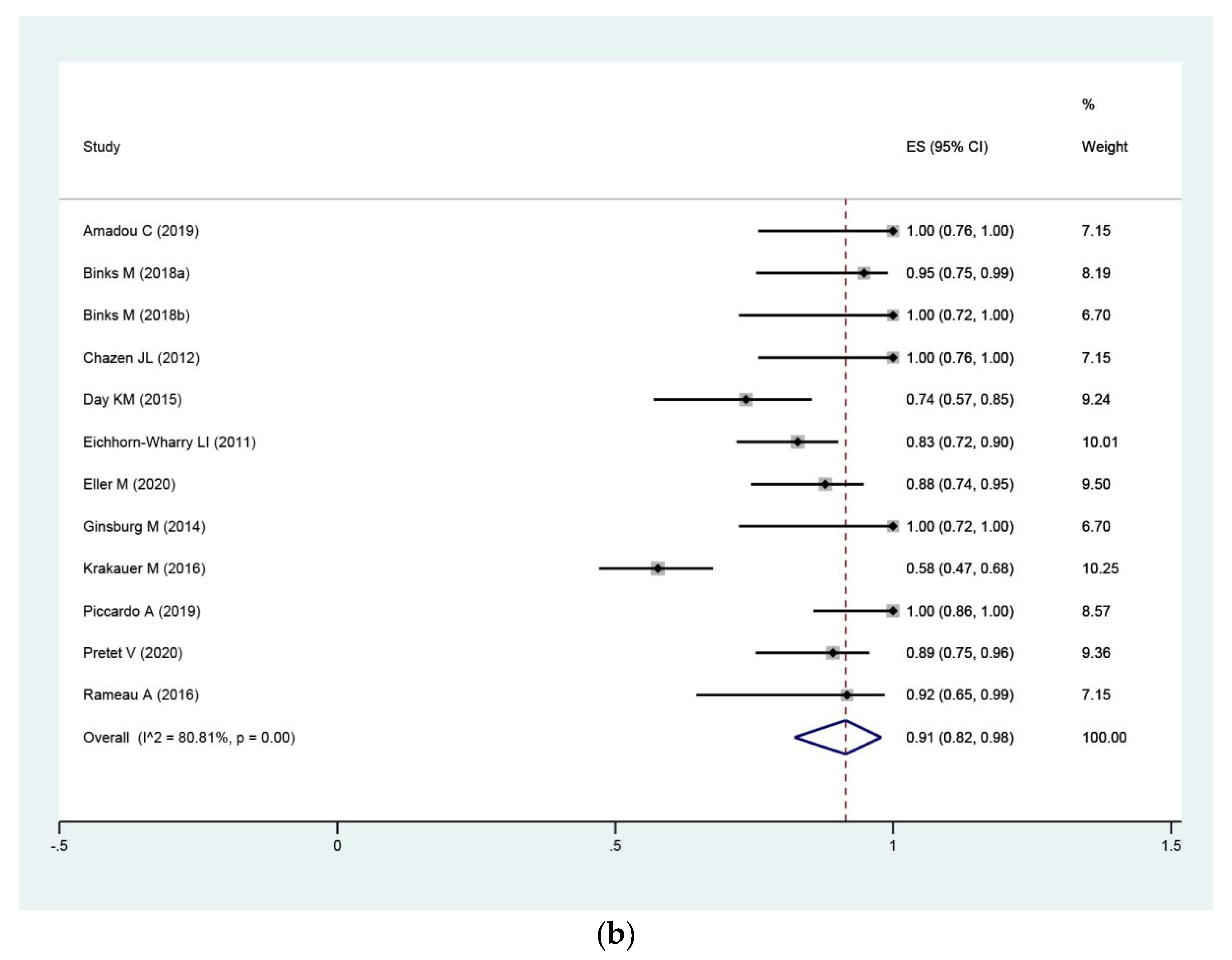
3.4.2. Per-Patient Level Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bunch, P.M.; Kelly, H.R. Preoperative Imaging Techniques in Primary Hyperparathyroidism: A Review. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 929–937. [Google Scholar] [CrossRef]
- Fraser, W.D. Hyperparathyroidism. Lancet 2009, 374, 145–158. [Google Scholar] [CrossRef]
- Yeh, M.W.; Ituarte, P.H.; Zhou, H.C.; Nishimoto, S.; Liu, I.L.; Harari, A.; Haigh, P.I.; Adams, A.L. Incidence and prevalence of primary hyperparathyroidism in a racially mixed population. J. Clin. Endocrinol. Metab. 2013, 98, 1122–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunch, P.M.; Randolph, G.W.; Brooks, J.A.; George, V.; Cannon, J.; Kelly, H.R. Parathyroid 4D CT: What the Surgeon Wants to Know. Radiographics 2020, 40, 1383–1394. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Wang, T.S.; Ruan, D.T.; Lee, J.A.; Asa, S.L.; Duh, Q.Y.; Doherty, G.M.; Herrera, M.F.; Pasieka, J.L.; Perrier, N.D.; et al. The American Association of Endocrine Surgeons Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA Surg. 2016, 151, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Bilezikian, J.P.; Brandi, M.L.; Eastell, R.; Silverberg, S.J.; Udelsman, R.; Marcocci, C.; Potts, J.T., Jr. Guidelines for the management of asymptomatic primary hyperparathyroidism: Summary statement from the Fourth International Workshop. J. Clin. Endocrinol. Metab. 2014, 99, 3561–3569. [Google Scholar] [CrossRef]
- Khan, A.A.; Hanley, D.A.; Rizzoli, R.; Bollerslev, J.; Young, J.E.; Rejnmark, L.; Thakker, R.; D’Amour, P.; Paul, T.; Van Uum, S.; et al. Primary hyperparathyroidism: Review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos. Int. 2017, 28, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Udelsman, R.; Donovan, P.I. Open minimally invasive parathyroid surgery. World J. Surg. 2004, 28, 1224–1226. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, S.E.; Hunter, G.J.; Hamberg, L.M.; Schellingerhout, D.; Doherty, D.B.; Ayers, G.D.; Shapiro, S.E.; Edeiken, B.S.; Truong, M.T.; Evans, D.B.; et al. Improved preoperative planning for directed parathyroidectomy with 4-dimensional computed tomography. Surgery 2006, 140, 932–941. [Google Scholar] [CrossRef]
- Hoang, J.K.; Sung, W.K.; Bahl, M.; Phillips, C.D. How to perform parathyroid 4D CT: Tips and traps for technique and interpretation. Radiology 2014, 270, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Acar, N.; Haciyanli, M.; Coskun, M.; Erdogan, N.K.; Celik, S.C.; Haciyanli, S.G.; Gur, E.O. Diagnostic value of four-dimensional computed tomography and four-dimensional magnetic resonance imaging in primary hyperparathyroidism when first-line imaging was inadequate. Ann. R Coll. Surg. Engl. 2020, 102, 294–299. [Google Scholar] [CrossRef]
- Eichhorn-Wharry, L.I.; Carlin, A.M.; Talpos, G.B. Mild hypercalcemia: An indication to select 4-dimensional computed tomography scan for preoperative localization of parathyroid adenomas. Am. J. Surg. 2011, 201, 334–338. [Google Scholar] [CrossRef]
- Yeh, R.; Tay, Y.K.D.; Tabacco, G.; Dercle, L.; Kuo, J.H.; Bandeira, L.; McManus, C.; Leung, D.K.; Lee, J.A.; Bilezikian, J.P. Diagnostic performance of 4D CT and sestamibi SPECT/CT in localizing parathyroid adenomas in primary hyperparathyroidism. Radiology 2019, 291, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Wang, T.S.; Farrokhyar, F.; Roman, S.A.; Sosa, J.A. A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann. Surg. Oncol. 2012, 19, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Wan, Q.C.; Li, J.F.; Tang, L.L.; Lv, J.; Xie, L.J.; Li, J.P.; Qin, L.P.; Cheng, M.H. Comparing the diagnostic accuracy of 4D CT and 99mTc-MIBI SPECT/CT for localizing hyperfunctioning parathyroid glands: A systematic review and meta-analysis. Nucl. Med. Commun. 2021, 42, 225–233. [Google Scholar] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Thompson, S.G. Why sources of heterogeneity in meta-analysis should be investigated. BMJ 1994, 309, 1351–1355. [Google Scholar] [CrossRef]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef]
- Amadou, C.; Bera, G.; Ezziane, M.; Chami, L.; Delbot, T.; Rouxel, A.; Leban, M.; Herve, G.; Menegaux, F.; Leenhardt, L.; et al. 18F-Fluorocholine PET/CT and Parathyroid 4D Computed Tomography for Primary Hyperparathyroidism: The Challenge of Reoperative Patients. World J. Surg. 2019, 43, 1232–1242. [Google Scholar] [CrossRef] [PubMed]
- Binks, M.; Burrows, D.; Littlejohn, D. A rural perspective on minimally invasive parathyroidectomy: Optimal preoperative imaging and patient outcomes. ANZ J. Surg. 2018, 89, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Chazen, J.L.; Gupta, A.; Dunning, A.; Phillips, C.D. Diagnostic accuracy of 4D-CT for parathyroid adenomas and hyperplasia. AJNR Am. J. Neuroradiol. 2012, 33, 429–433. [Google Scholar] [CrossRef] [Green Version]
- Day, K.M.; Elsayed, M.; Beland, M.D.; Monchik, J.M. The utility of 4-dimensional computed tomography for preoperative localization of primary hyperparathyroidism in patients not localized by sestamibi or ultrasonography. Surgery 2015, 157, 534–539. [Google Scholar] [CrossRef]
- Eller, M.; Dave, A.; Johnson, C.; Fingeret, A.L. Accuracy of 4-Dimensional Computed Tomography for Localization in Primary Hyperparathyroidism. J. Surg. Res. 2020, 257, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, M.; Christoforidis, G.A.; Zivin, S.P.; Obara, P.; Wroblewski, K.; Angelos, P.; Grogan, R.H.; Kaplan, E.L. Adenoma localization for recurrent or persistent primary hyperparathyroidism using dynamic four-dimensional CT and venous sampling. J. Vasc. Interv. Radiol. 2015, 26, 79–86. [Google Scholar] [CrossRef]
- Hinson, A.M.; Lee, D.R.; Hobbs, B.A.; Fitzgerald, R.T.; Bodenner, D.L.; Stack, B.C. Preoperative 4D CT Localization of Nonlocalizing Parathyroid Adenomas by Ultrasound and SPECT-CT. Otolaryngol. Head Neck Surg. 2015, 153, 775–778. [Google Scholar] [CrossRef]
- Krakauer, M.; Wieslander, B.; Myschetzky, P.S.; Lundstrøm, A.; Bacher, T.; Sørensen, C.H.; Trolle, W.; Nygaard, B.; Bennedbæk, F.N. A Prospective Comparative Study of Parathyroid Dual-Phase Scintigraphy, Dual-Isotope Subtraction Scintigraphy, 4D-CT, and Ultrasonography in Primary Hyperparathyroidism. J. Med. Imaging Radiat. Oncol. 2016, 41, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, S.H.S.; Brooks, K.A.; Knackstedt, M.I.; Eguia, A.A.; Low, G.M.; Jacks, A.E.; Asi, K.W.; Patino, M.O.; Friedman, E.R.; Karni, R.J. 4D-CT facilitates focused parathyroidectomy in patients with primary hyperparathyroidism by maintaining a high negative-predictive value for uninvolved quadrants. Am. J. Otolaryngol. 2020, 41, 102683. [Google Scholar] [CrossRef]
- Piccardo, A.; Trimboli, P.; Rutigliani, M.; Puntoni, M.; Foppiani, L.; Bacigalupo, L.; Crescenzi, A.; Bottoni, G.; Treglia, G.; Paparo, F.; et al. Additional value of integrated F-18-choline PET/4D contrast-enhanced CT in the localization of hyperfunctioning parathyroid glands and correlation with molecular profile. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Pretet, V.; Rotania, M.; Helali, M.; Ignat, M.; Vix, M.; Imperiale, A. F-18-Fluorocholine PET and Multiphase CT Integrated in Dual Modality PET/4D-CT for Preoperative Evaluation of Primary Hyperparathyroidism. J. Clin. Med. 2020, 9, 2005. [Google Scholar] [CrossRef] [PubMed]
- Rameau, A.; Eng, S.; Vu, J.; Saket, R.; Jun, P.; Friduss, M. Four-dimensional computed tomography scan utility in parathyroidectomy for primary hyperparathyroidism with low baseline intact parathyroid hormone. Laryngoscope 2017, 127, 1476–1482. [Google Scholar] [CrossRef]
- Suh, Y.J.; Choi, J.Y.; Kim, S.J.; Chun, I.K.; Yun, T.J.; Lee, K.E.; Kim, J.H.; Cheon, G.J.; Youn, Y.K. Comparison of 4D CT, Ultrasonography, and Tc-99m Sestamibi SPECT/CT in Localizing Single-Gland Primary Hyperparathyroidism. Otolaryngol. Head Neck Surg. 2015, 152, 438–443. [Google Scholar] [CrossRef]
- Wong, K.K.; Fig, L.M.; Gross, M.D.; Dwamena, B.A. Parathyroid adenoma localization with 99mTc-sestamibi SPECT/CT: A meta-analysis. Nucl. Med. Commun. 2015, 36, 363–375. [Google Scholar] [CrossRef]
- Mortenson, M.M.; Evans, D.B.; Lee, J.E.; Hunter, G.J.; Shellingerhout, D.; Vu, T.; Edeiken, B.S.; Feng, L.; Perrier, N.D. Parathyroid exploration in the reoperative neck: Improved preoperative localization with 4D-computed tomography. J. Am. Coll. Surg. 2008, 206, 888–895; discussion 895–886. [Google Scholar] [CrossRef]
- Hamidi, M.; Sullivan, M.; Hunter, G.; Hamberg, L.; Cho, N.L.; Gawande, A.A.; Doherty, G.M.; Moore, F.D.; Nehs, M.A. 4D-CT is Superior to Ultrasound and Sestamibi for Localizing Recurrent Parathyroid Disease. Ann. Surg. Oncol. 2018, 25, 1403–1409. [Google Scholar] [CrossRef]
- Gough, I. Reoperative parathyroid surgery: The importance of ectopic location and multigland disease. ANZ J. Surg. 2006, 76, 1048–1050. [Google Scholar] [CrossRef] [PubMed]
- Jaskowiak, N.; Norton, J.A.; Alexander, H.R.; Doppman, J.L.; Shawker, T.; Skarulis, M.; Marx, S.; Spiegel, A.; Fraker, D.L. A prospective trial evaluating a standard approach to reoperation for missed parathyroid adenoma. Ann. Surg. 1996, 224, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Bergenfelz, A.O.; Wallin, G.; Jansson, S.; Eriksson, H.; Martensson, H.; Christiansen, P.; Reihner, E. Results of surgery for sporadic primary hyperparathyroidism in patients with preoperatively negative sestamibi scintigraphy and ultrasound. Langenbecks Arch. Surg. 2011, 396, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Tanny, S.T.; Einsiedel, P.; Lichtenstein, M.; Stella, D.L.; Phal, P.M.; Miller, J.A. Four-Dimensional Computed Tomography: Clinical Impact for Patients with Primary Hyperparathyroidism. Ann. Surg. Oncol. 2018, 25, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Forghani, R.; Roskies, M.; Liu, X.; Tan, X.; Mlynarek, A.; Payne, R.J.; Nair, J.R.; Hier, M.P.; Levental, M. Dual-Energy CT Characteristics of Parathyroid Adenomas on 25-and 55-Second 4D-CT Acquisitions: Preliminary Experience. J. Comput. Assist. Tomogr. 2016, 40, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Lubitz, C.C.; Hunter, G.J.; Hamberg, L.M.; Parangi, S.; Ruan, D.; Gawande, A.; Gaz, R.D.; Randolph, G.W.; Moore, F.D., Jr.; Hodin, R.A.; et al. Accuracy of 4-dimensional computed tomography in poorly localized patients with primary hyperparathyroidism. Surgery 2010, 148, 1129–1137. [Google Scholar] [CrossRef]
- Raghavan, P.; Durst, C.R.; Ornan, D.A.; Mukherjee, S.; Wintermark, M.; Patrie, J.T.; Xin, W.; Shada, A.L.; Hanks, J.B.; Smith, P.W.; et al. Dynamic CT for parathyroid disease: Are multiple phases necessary? AJNR Am. J. Neuroradiol. 2016, 35, 1959–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.J.; Sicuro, P.; Alseidi, A.; Blackmore, C.C.; Ryan, J.A. Two-phase (low-dose) computed tomography is as effective as 4D-CT for identifying enlarged parathyroid glands. Int. J. Surg. 2015, 14, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Cotoi, L.; Amzar, D.; Sporea, I.; Borlea, A.; Navolan, D.; Varcus, F.; Stoian, D. Shear Wave Elastography versus Strain Elastography in Diagnosing Parathyroid Adenomas. Int. J. Endocrinol. 2020, 2020, 3801902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, G.; Piper, K.; Keller, J.M.; Mayo, M.L.; Puett, D.; Earp, K.M.; Malchoff, C.D. Shear wave elastography and parathyroid adenoma: A new tool for diagnosing parathyroid adenomas. Eur. J. Radiol. 2016, 85, 1586–1593. [Google Scholar] [CrossRef] [Green Version]
- Chandramohan, A.; Therese, M.; Abhraham, D.; Paul, T.V.; Mazhuvanchary, P.J. Can ARFI elastography be used to differentiate parathyroid from thyroid lesions? J. Endocrinol. Investig. 2018, 41, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Cuderman, A.; Senica, K.; Rep, S.; Hocevar, M.; Kocjan, T.; Sever, M.J.; Zaletel, K.; Lezaic, L. (18)F-Fluorocholine PET/CT in Primary Hyperparathyroidism: Superior Diagnostic Performance to Conventional Scintigraphic Imaging for Localization of Hyperfunctioning Parathyroid Glands. J. Nucl. Med. 2020, 61, 577–583. [Google Scholar] [CrossRef]
- Traub-Weidinger, T.; Mayerhoefer, M.E.; Koperek, O.; Mitterhauser, M.; Duan, H.; Karanikas, G.; Niederle, B.; Hoffmann, M. 11C-methionine PET/CT imaging of 99mTc-MIBI-SPECT/CT-negative patients with primary hyperparathyroidism and previous neck surgery. J. Clin. Endocrinol. Metab. 2014, 99, 4199–4205. [Google Scholar] [CrossRef] [Green Version]
- Treglia, G.; Piccardo, A.; Imperiale, A.; Strobel, K.; Kaufmann, P.A.; Prior, J.O.; Giovanella, L. Diagnostic performance of choline PET for detection of hyperfunctioning parathyroid glands in hyperparathyroidism: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 751–765. [Google Scholar] [CrossRef] [PubMed]
- Caldarella, C.; Treglia, G.; Isgro, M.A.; Giordano, A. Diagnostic performance of positron emission tomography using (1)(1)C-methionine in patients with suspected parathyroid adenoma: A meta-analysis. Endocrine 2013, 43, 78–83. [Google Scholar] [CrossRef]
- Argiro, R.; Diacinti, D.; Sacconi, B.; Iannarelli, A.; Diacinti, D.; Cipriani, C.; Pisani, D.; Romagnoli, E.; Biffoni, M.; Di Gioia, C.; et al. Diagnostic accuracy of 3T magnetic resonance imaging in the preoperative localisation of parathyroid adenomas: Comparison with ultrasound and 99mTc-sestamibi scans. Eur. Radiol. 2018, 28, 4900–4908. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Country | Study Design | Patient No. | Age | F/M | Prior Neck Surgery | Reference Standard |
|---|---|---|---|---|---|---|---|
| Acar N (2020) | Turkey | R | 17 (33) | 59.5 | 16/1 | No | histology + follow up |
| Amadou C (2019) | France | R | 19 (29) | NA | NA | Yes | histology, US-guided FNA |
| Binks M (2018) | Australia | R | 13, 21 (165) * | NA | NA | NA | histology + follow up |
| Chazen JL (2012) | USA | R | 25 (35) | NA | NA | Yes | histology |
| Day KM (2015) | USA | R | 37 (37) | 63 | NA | Yes | histology + IOPTH |
| Eichhorn-Wharry LI (2011) | USA | NA | 135 (135) | 59.2 ± 13 | 109/26 | Yes | histology |
| Eller M (2020) | USA | R | 51 (100) | NA | NA | No | operation + histology |
| Ginsburg M (2015) | USA | R | 22 (28) | NA | NA | Yes | histology |
| Hinson AM (2015) | USA | R | 19 (19) | 66 | 16/3 | No | histology + follow up |
| Krakauer M (2016) | Denmark | P | 91 (91) | 66 | 67/24 | No | surgical findings + histology |
| Naqvi SHS (2020) | USA | R | 68 (68) | 65.5 | NA | NA | surgical findings + histology |
| Piccardo A (2019) | Italy | P | 31 (44) | NA | NA | NA | histology + follow up |
| Pretet V (2020) | France | R | 44 (50) | NA | NA | Yes | histology + IOPTH + follow up |
| Rameau A (2016) | USA | R | 14 (14) | 57.6 | 12/2 | No | surgical reports + histology |
| Suh YJ (2015) | Korea | R | 38 (38) | 55.8 ±13.2 | 27/11 | No | surgical reports + histology |
| Yeh R (2019) | USA | R | 400 (400) | 61 ± 14 | 319/81 | No | surgical reports + histology |
| Source | Machine Model | Detector | Product | Injection Rate (mL/s) | Dose | Slice Thickness | Scan Phase | Imaging Procedure |
|---|---|---|---|---|---|---|---|---|
| Acar N (2020) | Siemens Somatom | 128 | Iodine | NA | 1 mL/kg | NA | 4 | 2 |
| Amadou C (2019) | NA | NA | NA | NA | NA | NA | 3 | 2 |
| Binks M (2018) | NA | NA | NA | NA | NA | NA | 3 | both |
| Chazen JL (2012) | GE LightSpeed | 16, 64 | Omnipaque | 4 | 2 mL/kg 120 mL max | 1.25 mm | 3 | 1 |
| Day KM (2015) | GE LightSpeed | 64 | Omnipaque | 3 | 100 mL | 0.625 mm | both | 2 |
| Eichhorn-Wharry LI (2011) | GE 16, VCT Lightspeed | 16 | Optiray | NA | 100 mL | 1.25 mm | 3 | 1 |
| Eller M (2020) | NA | NA | NA | NA | NA | NA | NA | 2 |
| Ginsburg M (2015) | Philips Brilliance | 64, 256 | Omnipaque | 4 | 120 mL | 0.9 mm | 4 | 2 |
| Hinson AM (2015) | Philips | 64 | nonionic contrast | 3 | 75 mL | NA | 4 | 2 |
| Krakauer M (2016) | Philips Skylight | 16 | Omnipaque | 3.5 | 100 mL | 2 mm | 3 | 1 |
| Naqvi SHS (2020) | NA | NA | NA | NA | NA | NA | NA | 1 |
| Piccardo A (2019) | NA | 16 | Iohexol, Iodine | 3.3–4 | 80–100 mL 350 mg | 1.25 mm | 3 | 2 |
| Pretet V (2020) | Philips Biograph | 128 | Iomeron | 2.5–3 | 75 mL | 1 mm | 4 | 2 |
| Rameau A (2016) | GE LightSpeed, VCT | 16, 64 | Omnipaque | 4 | 100–120 mL | 1.25 mm | 3 | 1 |
| Suh YJ (2015) | Philips Brilliance | 64 | Xenetics | NA | 90 mL | 2 mm | 4 | 1 |
| Yeh R (2019) | Siemens Symbia T | 16 | Omnipaque | 4 | 75 mL | 1 mm | 3 | 1 |
| Source | Patient No. | True Positives | False Positives | False Negatives | True Negatives | LB | PB |
|---|---|---|---|---|---|---|---|
| Acar N (2020) | 17 (33) | 9 | 0 | 9 | 51 | √ | |
| Amadou C (2019) | 19 (29) | 12 | 3 | 4 | 2 | √ | |
| 12 | 0 | 7 | 0 | √ | |||
| Binks M (2018a) | 21 (165) | 18 | 1 | 3 | 0 | √ | |
| Binks M (2018b) | 13 (165) | 10 | 0 | 3 | 0 | √ | |
| Chazen JL (2012) | 25 (35) | 12 | 0 | 2 | 11 | √ | |
| Day KM (2015) | 37 (37) | 25 | 9 | 3 | 0 | √ | |
| Eichhorn-Wharry LI (2011) | 135 (135) | 53 | 11 | 33 | NA | √ | |
| Eller M (2020) | 51 (100) | 36 | 5 | 5 | 5 | √ | |
| Ginsburg M (2015) | 22 (28) | 10 | 0 | 10 | 2 | √ | |
| Hinson AM (2015) | 19 (19) | 13 | 5 | 4 | 54 | √ | |
| Krakauer M (2016) | 91 (91) | 56 | 37 | 41 | 230 | √ | |
| 49 | 36 | 0 | 0 | √ | |||
| Naqvi SHS (2020) | 68 (68) | 60 | 9 | 14 | 194 | √ | |
| Piccardo A (2019) | 31 (44) | 23 | 0 | 8 | 0 | √ | |
| Pretet V (2020) | 44 (50) | 33 | 6 | 17 | 0 | √ | |
| 33 | 4 | 7 | 0 | √ | |||
| Rameau A (2016) | 14 (14) | 16 | 1 | 3 | 0 | √ | |
| 11 | 1 | 2 | 0 | √ | |||
| Suh YJ (2015) | 38 (38) | 35 | 5 | 3 | 109 | √ | |
| Yeh R (2019) | 400 (400) | 414 | 47 | 108 | 1031 | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, L.; Yao, J.; Hao, P.; Yang, Y.; Liu, Z.; Peng, R. Diagnostic Role of Four-Dimensional Computed Tomography for Preoperative Parathyroid Localization in Patients with Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 664. https://doi.org/10.3390/diagnostics11040664
Sun L, Yao J, Hao P, Yang Y, Liu Z, Peng R. Diagnostic Role of Four-Dimensional Computed Tomography for Preoperative Parathyroid Localization in Patients with Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis. Diagnostics. 2021; 11(4):664. https://doi.org/10.3390/diagnostics11040664
Chicago/Turabian StyleSun, Lixin, Jian Yao, Pan Hao, Yuanyuan Yang, Zhimou Liu, and Ruchen Peng. 2021. "Diagnostic Role of Four-Dimensional Computed Tomography for Preoperative Parathyroid Localization in Patients with Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis" Diagnostics 11, no. 4: 664. https://doi.org/10.3390/diagnostics11040664
APA StyleSun, L., Yao, J., Hao, P., Yang, Y., Liu, Z., & Peng, R. (2021). Diagnostic Role of Four-Dimensional Computed Tomography for Preoperative Parathyroid Localization in Patients with Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis. Diagnostics, 11(4), 664. https://doi.org/10.3390/diagnostics11040664