
Nourin-Dependent miR-137 and miR-106b: Novel Biomarkers for Early Diagnosis of Myocardial Ischemia in Coronary Artery Disease Patients



 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Demographic Characteristics of Participants
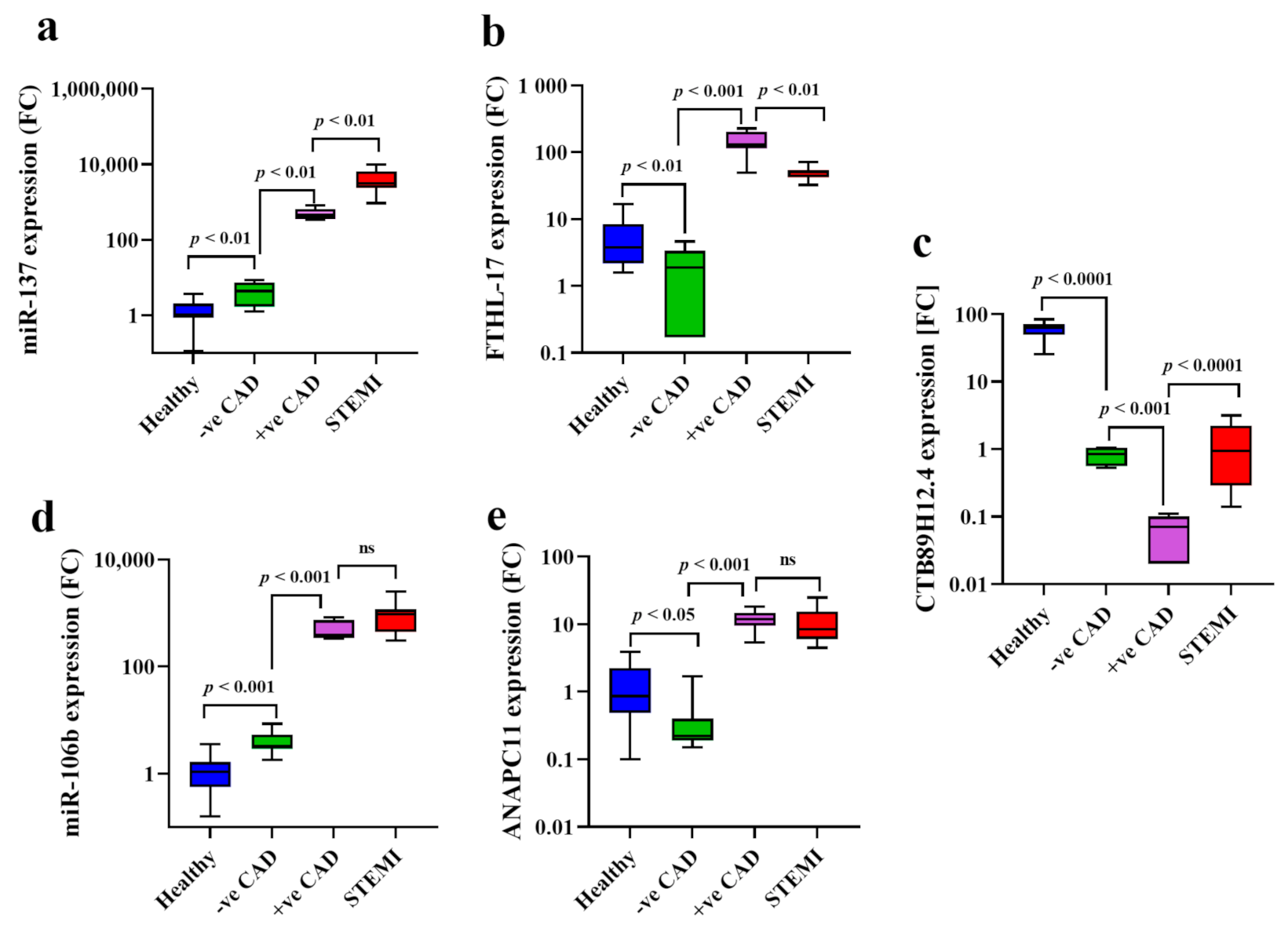
2.2. Nourin Network Gene Expression Profiles in Patients Suspected of Myocardial Ischemia
2.2.1. Assessment of CTB89H12.4/miR-137/FTHL-17 Network “Post-Stress Test”
2.2.2. Assessment of CTB89H12.4/miR-106b-5p/ ANAPC11 Network” Post-Stress Test”
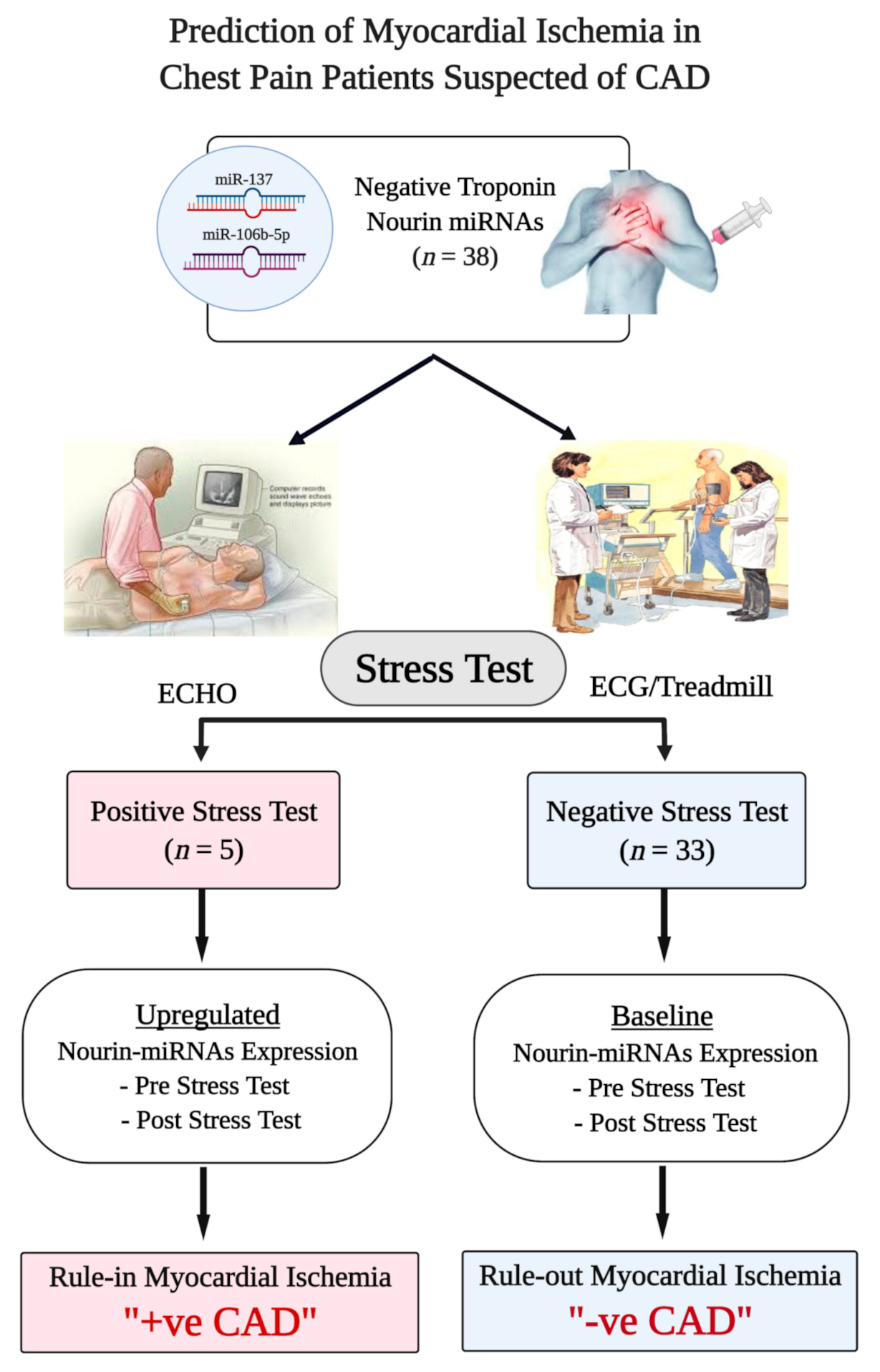
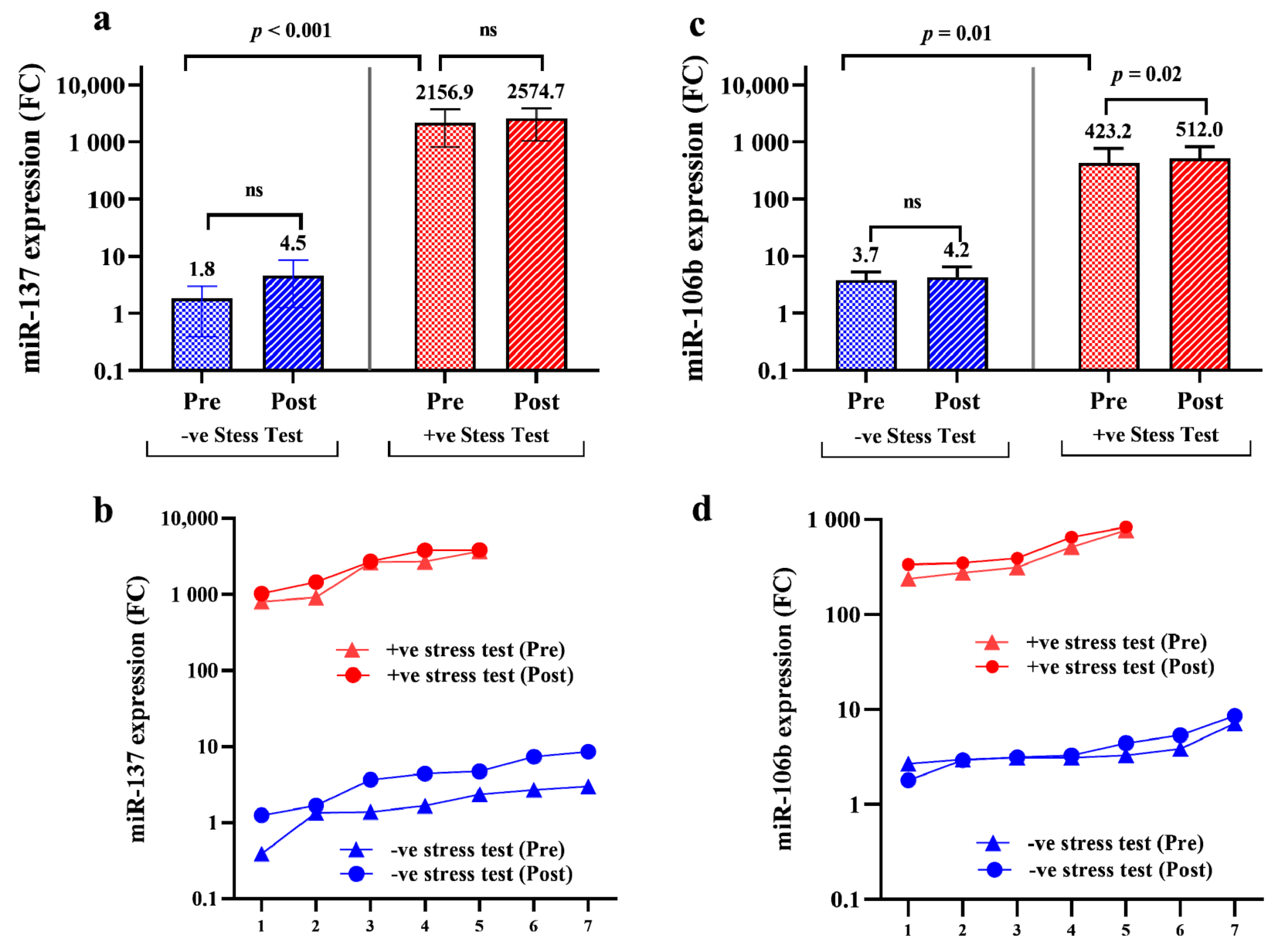
2.3. Assessment of Nourin-Dependent miR-137 and miR-106b Gene Expression Profiles “Pre-Stress Test” and “Post-Stress Test” (30 Minutes After Termination) in Chest Pain Patients Suspected of Myocardial Ischemia
3. Discussion
4. Subjects & Methods
4.1. Bioinformatics Analysis
4.2. Study Design and Protocol
4.2.1. Study Participants
4.2.2. Study Protocol
4.3. Dobutamine Stress Test Protocol
4.3.1. Dobutamine Stress Echocardiography
4.3.2. Stress ECG Protocol
4.4. Gene Amplification Analysis
4.5. Troponin Measurement
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [Green Version]
- Stepinska, J.; Lettino, M.; Ahrens, I.; Bueno, H.; Garcia-Castrillo, L.; Khoury, A.; Lancellotti, P.; Mueller, C.; Muenzel, T.; Oleksiak, A.; et al. Diagnosis and risk stratification of chest pain patients in the emergency department: Focus on acute coronary syndromes. A position paper of the Acute Cardiovascular Care Association. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 76–89. [Google Scholar] [CrossRef] [Green Version]
- Kossaify, A.; Bassil, E.; Kossaify, M. Stress Echocardiography: Concept and Criteria, Structure and Steps, Obstacles and Outcomes, Focused Update and Review. Cardiol. Res. 2020, 11, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Deepti, S.; Roy, A.; Patel, C.D.; Tandon, N.; Naik, N.; Singh, S.; Sharma, G.; Bahl, V.K. Assessment of asymptomatic ischemic heart disease using stress myocardial perfusion imaging in patients with type 2 diabetes mellitus. Indian Heart J. 2018, 70, S157–S160. [Google Scholar] [CrossRef]
- Murthy, V.L.; Bateman, T.M.; Chen, W.; Malhotra, S.; Miller, E.J.; Ruddy, T.D.; Dilsizian, V. Impact of the ISCHEMIA Trial on Stress Nuclear Myocardial Perfusion Imaging. J. Nucl. Med. 2020, 61, 962–964. [Google Scholar] [CrossRef]
- Garzillo, C.L.; Hueb, W.; Gersh, B.; Rezende, P.C.; Lima, E.G.; Favarato, D.; Ramires, J.A.F.; Filho, R.K. Association Between Stress Testing–Induced Myocardial Ischemia and Clinical Events in Patients With Multivessel Coronary Artery Disease. JAMA Intern. Med. 2019, 179, 1345. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.-Y.; Lee, K.-Y.; Chun, E.J.; Lee, W.-W.; Park, E.K.; Chang, H.-J.; Choi, S.I. Comparison of Stress Perfusion MRI and SPECT for Detection of Myocardial Ischemia in Patients With Angiographically Proven Three-Vessel Coronary Artery Disease. Am. J. Roentgenol. 2010, 195, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G. Myocardial ischemia: Lack of coronary blood flow, myocardial oxygen supply-demand imbalance, or what? Am. J. Physiol. Circ. Physiol. 2019, 316, H1439–H1446. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G.; Gersh, B.J. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: A continual challenge. Eur. Heart J. 2016, 38, 224–784. [Google Scholar] [CrossRef]
- Reed, G.W.; Rossi, J.E.; Cannon, C.P. Acute myocardial infarction. Lancet 2017, 389, 197–210. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Ferry, A.V.; Mills, N.L. Cardiac Biomarkers and the Diagnosis of Myocardial Infarction in Women. Curr. Cardiol. Rep. 2017, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Giannitsis, E.; Gopi, V. Biomarkers for infarct diagnosis and rapid rule-out/rule-in of acute myocardial infarction. Herz 2020, 45, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, I.; Yardim, M. Biomarkers in acute myocardial infarction: Current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Tao, Y.; Zhang, L.; Xu, W.; Zhou, X. Diagnostic and prognostic value of biomarkers in acute myocardial infarction. Postgrad. Med. J. 2019, 95, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, S.A.; Poston, R.; Todd, R.; Helmy, T.; Almaghraby, A.M.; Elbayoumi, T.; Kreutzer, D.L.; Taegtmeyer, H.; Elgebaly, S. Cyclocreatine protects against ischemic injury and enhances cardiac recovery during early reperfusion. Expert Rev. Cardiovasc. Ther. 2019, 17, 683–697. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, S.A.; Hashmi, F.H.; Houser, S.L.; Allam, M.E.; Doyle, K. Cardiac-derived neutrophil chemotactic factors: Detection in coronary sinus effluents of patients undergoing myocardial revascularization. J. Thorac. Cardiovasc. Surg. 1992, 103, 952–959. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Elgebaly, S. Cardiac derived neutrophil chemotactic factors; preliminary biochemical characterization. J. Mol. Cell. Cardiol. 1989, 21, 585–593. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Van Buren, C.; Todd, R.; Poston, R.; Rabie, M.A.; Mohamed, A.F.; Ahmed, L.A.; Sayed, N.S.E. Abstract 13311: Cyclocreatine Phosphate: A Novel Mechanism for Preventing Development of Heart Failure. Circulation 2020, 142, A13311. [Google Scholar] [CrossRef]
- Elgebaly, S.A. Nourexal: A Novel Anti-inflammatory/Antiapoptotic Therapy Against Reperfusion Injury. J. Clin. Exp. Cardiol. 2016, 7, 33. [Google Scholar]
- Elgebaly, S.; Christenson, R.; Kandil, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Eldeeb, H.; Ali, M.; Sharafieh, R.; Klueh, U.; et al. Nourin-Dependent miR-137 and miR-106b: Novel Early Inflammatory Diagnostic Biomarkers for Unstable Angina Patients. Biomolecules 2021, 11, 368. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Sharafieh, R.; Klueh, U.; Kreutzer, D.L. Abstract 13051: Nourin-dependent Mirna-137: A Novel Early Diagnostic Biomarker for Unstable Angina Patients. Circulation 2020, 142, A13051. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; Elkhazragy, N.; Rashed, L.; Yacoub, B.; Sharafieh, R.; Klueh, U.; Kreutzer, D.L. Abstract 13103: Nourin-dependent Mirna-106b: A Novel Early Inflammatory Diagnostic Biomarker for Cardiac Injury. Circulation 2020, 142, A13103. [Google Scholar] [CrossRef]
- Elgebaly, S.; Todd, R.; Kreutzer, D.; Christenson, R.; El-Khazragy, N.; Arafa, R.; Rabie, M.; Mohamed, A.; Ahmed, L.; El Sayed, N. Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure. Int. J. Mol. Sci. 2021, 22, 3575. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, S.; Christenson, R.; Schiffmann, E.; Yi, Q.; Kreutzer, D. Early identification of cardiac ischemia patients in the emergency department. Catheter. Cardiovasc. Interv. 2013, 81, S2–S3. [Google Scholar]
- Zaghloul, A.; Iorgoveanu, C.; Balakumaran, K.; Balanescu, D.V.; Donisan, T. Limitations of Coronary Computed Tomography Angiography in Predicting Acute Coronary Syndrome in a Low to Intermediate-risk Patient with Chest Pain. Cureus 2018, 10, e2649. [Google Scholar] [CrossRef] [Green Version]
- Rahsepar, A.A.; Arbab-Zadeh, A. Cardiac CT vs. Stress Testing in Patients with Suspected Coronary Artery Disease: Review and Expert Recommendations. Curr. Cardiovasc. Imaging Rep. 2015, 8, 29. [Google Scholar] [CrossRef] [Green Version]
- Arbab-Zadeh, A. Stress Testing and Non-Invasive Coronary Angiography in Patients with Suspected Coronary Artery Disease: Time for a New Paradigm. Heart Int. 2012, 7, e2. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, Y.; Zhao, Y.; Wang, Y.; Ding, H.; Xue, S.; Li, P. Circulating miRNAs as biomarkers for early diagnosis of coronary artery disease. Expert Opin. Ther. Pat. 2018, 28, 591–601. [Google Scholar] [CrossRef]
- Adamson, P.D.; Hunter, A.; Madsen, D.M.; Shah, A.S.V.; McAllister, D.A.; Pawade, T.A.; Williams, M.C.; Berry, C.; Boon, N.A.; Flather, M.; et al. High-Sensitivity Cardiac Troponin I and the Diagnosis of Coronary Artery Disease in Patients With Suspected Angina Pectoris. Circ. Cardiovasc. Qual. Outcomes 2018, 11. [Google Scholar] [CrossRef]
- Wongpraparut, N.; Piyophirapong, S.; Maneesai, A.; Sribhen, K.; Krittayaphong, R.; Bsc, R.P.; White, H.D. High-Sensitivity Cardiac Troponin T in Stable Patients Undergoing Pharmacological Stress Testing. Clin. Cardiol. 2015, 38, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Schulz, O.; Paul-Walter, C.; Lehmann, M.; Abraham, K.; Berghöfer, G.; Schimke, I.; Jaffe, A.S. Usefulness of Detectable Levels of Troponin, Below the 99th Percentile of the Normal Range, as a Clue to the Presence of Underlying Coronary Artery Disease. Am. J. Cardiol. 2007, 100, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Morrow, D.A.; De Lemos, J.A.; Jarolim, P.; Braunwald, E. Detection of acute changes in circulating troponin in the setting of transient stress test-induced myocardial ischaemia using an ultrasensitive assay: Results from TIMI 35. Eur. Heart J. 2008, 30, 162–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurz, K.; Giannitsis, E.; Zehelein, J.; Katus, H.A. Highly Sensitive Cardiac Troponin T Values Remain Constant after Brief Exercise- or Pharmacologic-Induced Reversible Myocardial Ischemia. Clin. Chem. 2008, 54, 1234–1238. [Google Scholar] [CrossRef] [Green Version]
- Samaha, E.; Avila, A.; Helwani, M.A.; Ben Abdallah, A.; Jaffe, A.S.; Scott, M.G.; Nagele, P. High-Sensitivity Cardiac Troponin After Cardiac Stress Test: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e008626. [Google Scholar] [CrossRef] [Green Version]
- Elbaz, M.; Faccini, J.; Laperche, C.; Grousset, E.; Roncalli, J.; Ruidavets, J.-B.; Vindis, C. Identification of a miRNA Based-Signature Associated with Acute Coronary Syndrome: Evidence from the FLORINF Study. J. Clin. Med. 2020, 9, 1674. [Google Scholar] [CrossRef]
- Wang, L.; Jin, Y. Noncoding RNAs as Biomarkers for Acute Coronary Syndrome. BioMed Res. Int. 2020, 2020, 3298696. [Google Scholar] [CrossRef]
- Kaur, A.; Mackin, S.T.; Schlosser, K.; Wong, F.L.; Elharram, M.; Delles, C.; Stewart, D.J.; Dayan, N.; Landry, T.; Pilote, L. Systematic review of microRNA biomarkers in acute coronary syndrome and stable coronary artery disease. Cardiovasc. Res. 2019, 116, 1113–1124. [Google Scholar] [CrossRef]
- Zhang, P.; Liang, T.; Chen, Y.; Wang, X.; Wu, T.; Xie, Z.; Luo, J.; Yu, Y.; Yu, H. Circulating Exosomal miRNAs as Novel Biomarkers for Stable Coronary Artery Disease. BioMed Res. Int. 2020, 2020, 1–11. [Google Scholar] [CrossRef]
- Kumar, D.; Narang, R.; Sreenivas, V.; Rastogi, V.; Bhatia, J.; Saluja, D.; Srivastava, K. Circulating miR-133b and miR-21: Potential non-invasive diagnostic biomarkers of coronary artery disease. Eur. Heart J. 2020, 41, 41. [Google Scholar] [CrossRef]
- Melak, T.; Baynes, H.W. Circulating microRNAs as possible biomarkers for coronary artery disease: A narrative review. EJIFCC 2019, 30, 179–194. [Google Scholar]
- Singh, S.; De Ronde, M.W.J.; Kok, M.G.M.; Beijk, M.A.; De Winter, R.J.; Van Der Wal, A.C.; Sondermeijer, B.M.; Meijers, J.C.M.; Creemers, E.E.; Pinto-Sietsma, S.-J. MiR-223-3p and miR-122-5p as circulating biomarkers for plaque instability. Open Heart 2020, 7, e001223. [Google Scholar] [CrossRef]
- Zhao, T.; Qiu, Z.; Gao, Y. MiR-137-3p exacerbates the ischemia-reperfusion injured cardiomyocyte apoptosis by targeting KLF15. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2019, 393, 1013–1024. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, D.; Xie, P.; Ren, G.; Sun, G.; Zeng, X.; Sun, X. MiR-106b and MiR-15b Modulate Apoptosis and Angiogenesis in Myocardial Infarction. Cell. Physiol. Biochem. 2012, 29, 851–862. [Google Scholar] [CrossRef]
- Cortigiani, L.; Picano, E.; Coletta, C.; Chiarella, F.; Mathias, W.; Gandolfo, N.; De Alcantara, M.; Mazzoni, V.; Gensini, G.F.; Landi, P. Safety, feasibility, and prognostic implications of pharmacologic stress echocardiography in 1482 patients evaluated in an ambulatory setting. Am. Heart J. 2001, 141, 621–629. [Google Scholar] [CrossRef]
- Rozanski, A.; Gransar, H.; Hayes, S.W.; Min, J.; Friedman, J.D.; Thomson, L.E.; Berman, D.S. Temporal Trends in the Frequency of Inducible Myocardial Ischemia During Cardiac Stress Testing: 1991 to 2009. J. Am. Coll. Cardiol. 2013, 61, 1054–1065. [Google Scholar] [CrossRef] [Green Version]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thomas, G.S.; Voros, S.; McPherson, J.A.; Lansky, A.J.; Winn, M.E.; Bateman, T.M.; Elashoff, M.R.; Lieu, H.D.; Johnson, A.M.; Daniels, S.E.; et al. A Blood-Based Gene Expression Test for Obstructive Coronary Artery Disease Tested in Symptomatic Nondiabetic Patients Referred for Myocardial Perfusion Imaging the COMPASS Study. Circ. Cardiovasc. Genet. 2013, 6, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Bates, E.R.; Tamis-Holland, J.E.; Bittl, J.A.; O’Gara, P.T.; Levine, G.N. PCI Strategies in Patients With ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease. J. Am. Coll. Cardiol. 2016, 68, 1066–1081. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Jones, P.; Weintraub, W.S.; Mancini, G.J.; Sedlis, S.; Maron, D.J.; Teo, K.; Hartigan, P.; Kostuk, W.; Berman, D.; et al. Predicting the Benefits of Percutaneous Coronary Intervention on 1-Year Angina and Quality of Life in Stable Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e003971. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy (n = 16) | ECHO/ECG Stress Test | STEMI (n = 16) | p-Value | |
|---|---|---|---|---|---|
| Negative (n = 7) | Positive (n = 5) | ||||
| Age (Years) Mean ± SD | 32.9 ± 9.9 | 53.5 ± 9.9 | 55 ± 4.8 | 54.4 ± 12.7 | 0.001 |
| Sex: Males: n (%) | 16 (100) | 3 (43) | 4 (80) | 12 (75) | 0.014 |
| Risk Factors BMI (kg/m2) Mean Smoking: n (%) Diabetes Mellitus: n (%) Hypertension: n (%) Dyslipidemia: n (%) | 26.8 ± 4.7 8 (50) --- --- --- | 31.0 2 (29) 2 (40) 4 (57) 3 (43) | 30.0 --- 5 (71) 2 (40) 2 (40) | 31.4 ± 4.8 10 (52.5) 6 (37.5) 7 (43) 5 (31) | 0.145 0.09 0.15 0.82 0.6 |
| Variable | Negative Control | Post-ECHO/ECG Stress Test | Positive Control | |
|---|---|---|---|---|
| Healthy (n = 16) Median (min–max) | Negative (n = 7) Median (min–max) | Positive (n = 5) Median (min–max) | STEMI (n = 16) Median (min-max) | |
| miR-137 (log10) | 1.05 (0.1–3.7) | 4.5 (1.5–5.0) | 2575 (917–3774) | 3163 (936–9878) |
| miR-106b (log10) | 1.08 (0.2–3.6) | 3.3 (1.8–8.5) | 512 (305–803) | 953 (307–2504) |
| FTHL-17 (log10) | 3.8 (1.6–16.7) | 1.9 (0.2–4.6) | 131 (49–228) | 50 (33–76) |
| ANAPC11 (log10) | 0.9 (0.1–3.9) | 0.2 (0.15–1.7) | 11.9 (5.4–18.0) | 8.4 (4.5–25.0) |
| CTB89H12.4 (log10) | 65 (26–83) | 0.8 (0.5–1.1) | 0.07 (0.02–0.1) | 0.9 (0.14–3.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; Ibrahim, M.; Rizk, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Eldeeb, H.; Ali, M.M.; et al. Nourin-Dependent miR-137 and miR-106b: Novel Biomarkers for Early Diagnosis of Myocardial Ischemia in Coronary Artery Disease Patients. Diagnostics 2021, 11, 703. https://doi.org/10.3390/diagnostics11040703
Elgebaly SA, Christenson RH, Kandil H, Ibrahim M, Rizk H, El-Khazragy N, Rashed L, Yacoub B, Eldeeb H, Ali MM, et al. Nourin-Dependent miR-137 and miR-106b: Novel Biomarkers for Early Diagnosis of Myocardial Ischemia in Coronary Artery Disease Patients. Diagnostics. 2021; 11(4):703. https://doi.org/10.3390/diagnostics11040703
Chicago/Turabian StyleElgebaly, Salwa A., Robert H. Christenson, Hossam Kandil, Mohsen Ibrahim, Hussien Rizk, Nashwa El-Khazragy, Laila Rashed, Beshoy Yacoub, Heba Eldeeb, Mahmoud M. Ali, and et al. 2021. "Nourin-Dependent miR-137 and miR-106b: Novel Biomarkers for Early Diagnosis of Myocardial Ischemia in Coronary Artery Disease Patients" Diagnostics 11, no. 4: 703. https://doi.org/10.3390/diagnostics11040703
APA StyleElgebaly, S. A., Christenson, R. H., Kandil, H., Ibrahim, M., Rizk, H., El-Khazragy, N., Rashed, L., Yacoub, B., Eldeeb, H., Ali, M. M., & Kreutzer, D. L. (2021). Nourin-Dependent miR-137 and miR-106b: Novel Biomarkers for Early Diagnosis of Myocardial Ischemia in Coronary Artery Disease Patients. Diagnostics, 11(4), 703. https://doi.org/10.3390/diagnostics11040703