
Renal Diseases Associated with Hematologic Malignancies and Thymoma in the Absence of Renal Monoclonal Immunoglobulin Deposits


Abstract
:1. Introduction
2. Epidemiology
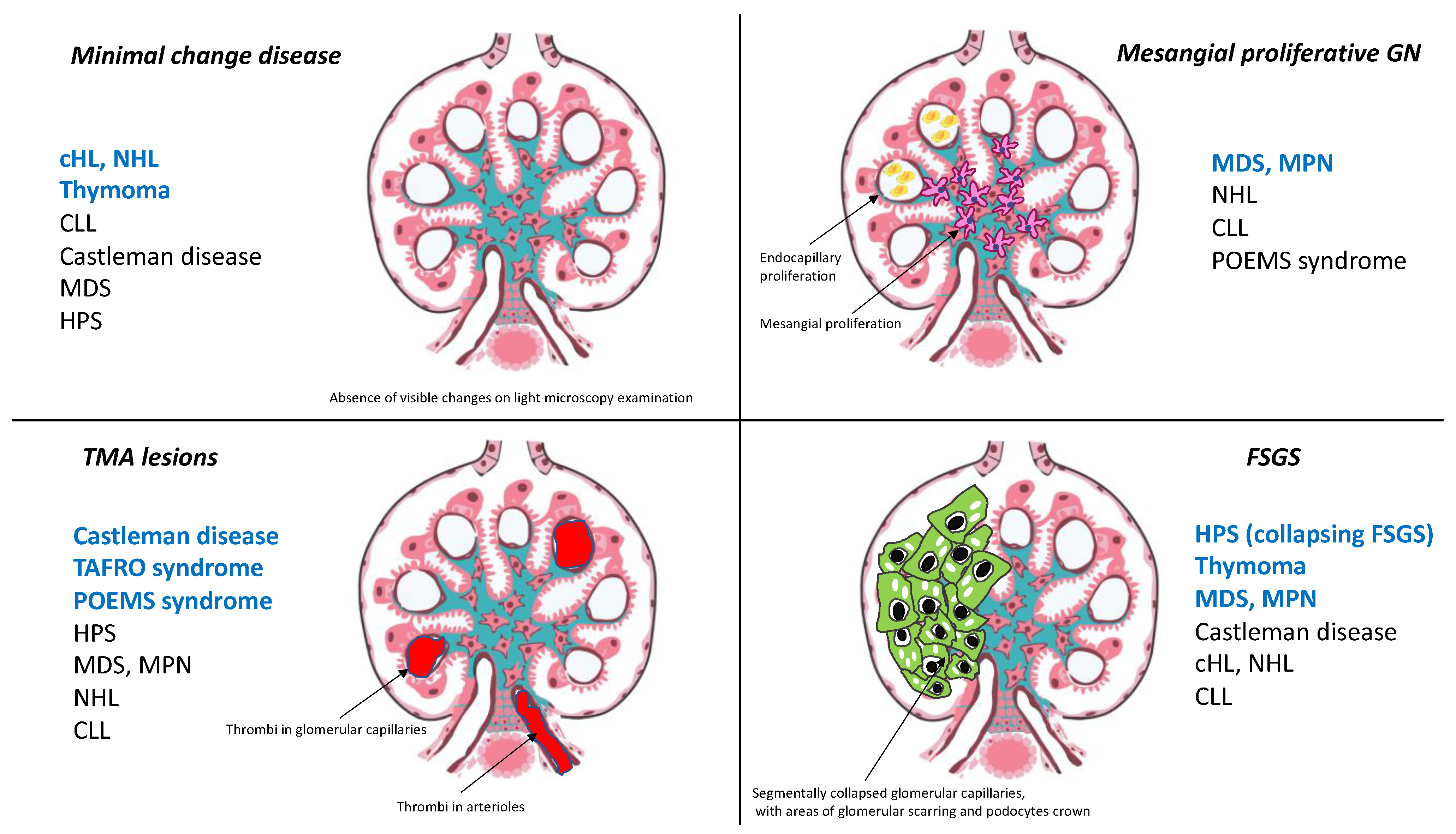
3. Hodgkin Lymphoma and Glomerular Disease: The Singular Case of Minimal Change Disease
4. Glomerular Diseases Associated with Non-Hodgkin Lymphoma
5. Lymphomatous Infiltration of Renal Parenchyma
6. Glomerulopathies Related to Myeloproliferative Neoplasms and Myelodysplastic Syndromes
7. Castleman Disease and POEMS-Related Renal Diseases
8. Renal Lesions Occurring in Patients with Hemophagocytic Syndrome
9. Acquired Thymic Disease-Associated Nephropathy
10. Conclusions
Funding
Conflicts of Interest
References
- Rosner, M.H.; Jhaveri, K.D.; McMahon, B.A.; Perazella, M.A. Onconephrology: The intersections between the kidney and cancer. CA Cancer J. Clin. 2021, 71, 47–77. [Google Scholar] [CrossRef] [PubMed]
- Luciano, R.L.; Brewster, U.C. Kidney involvement in leukemia and lymphoma. Adv. Chronic Kidney Dis. 2014, 21, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Lien, Y.-H.H.; Lai, L.-W. Pathogenesis, diagnosis and management of paraneoplastic glomerulonephritis. Nat. Rev. Nephrol. 2011, 7, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, N.; Bridoux, F.; Batuman, V.; Chaidos, A.; Cockwell, P.; D’Agati, V.D.; Dispenzieri, A.; Fervenza, F.C.; Fermand, J.-P.; Gibbs, S.; et al. The evaluation of monoclonal gammopathy of renal significance: A consensus report of the International Kidney and Monoclonal Gammopathy Research Group. Nat. Rev. Nephrol. 2019, 15, 45–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shingarev, R.; Glezerman, I.G. Kidney complications of immune checkpoint inhibitors: A review. Am. J. Kidney Dis. 2019, 74, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Estrada, C.C.; Maldonado, A.; Mallipattu, S.K. Therapeutic inhibition of VEGF signaling and associated nephrotoxicities. J. Am. Soc. Nephrol. 2019, 30, 187–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, P.M. Paraneoplastic glomerulopathies: New insights into an old entity. Kidney Int. 1999, 56, 355–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cambier, J.-F.; Ronco, P. Onco-nephrology: Glomerular diseases with cancer. Clin. J. Am. Soc. Nephrol. 2012, 7, 1701–1712. [Google Scholar] [CrossRef] [Green Version]
- El Karoui, K.; Vuiblet, V.; Dion, D.; Izzedine, H.; Guitard, J.; Frimat, L.; Delahousse, M.; Remy, P.; Boffa, J.-J.; Pillebout, E.; et al. Renal involvement in Castleman disease. Nephrol. Dial. Transplant. 2011, 26, 599–609. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.; Lv, J.; Dong, Y.; Wang, S.; Su, T.; Zhou, F.; Zou, W.; Zhao, M.; Zhang, H. Renal involvement in a large cohort of Chinese patients with Castleman disease. Nephrol. Dial. Transplant. 2011, 27, iii119–iii125. [Google Scholar] [CrossRef] [Green Version]
- Au, W.Y.; Chan, K.W.; Lui, S.L.; Lam, C.C.; Kwong, Y.L. Focal segmental glomerulosclerosis and mesangial sclerosis associated with myeloproliferative disorders. Am. J. Kidney Dis. 1999, 34, 889–893. [Google Scholar] [CrossRef]
- Büttner-Herold, M.; Sticht, C.; Wiech, T.; Porubsky, S. Renal disease associated with myeloproliferative neoplasms and myelodysplastic syndrome/myeloproliferative neoplasms. Histopathology 2021, 78, 738–748. Available online: https://www.onlinelibrary.wiley.com/doi/abs/10.1111/his.14282 (accessed on 7 January 2021). [CrossRef]
- Karras, A. What nephrologists need to know about hemophagocytic syndrome. Nat. Rev. Nephrol. 2009, 5, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M.J. Cancer statistics, 2007. CA Cancer J. Clin. 2007, 57, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, N.; Wadsworth, J.; Wijnen, M.; Gabriel, R. Prevalence, concentration, and prognostic importance of proteinuria in patients with malignancies. Br. Med. J. Clin. Res. Ed. 1988, 296, 1295–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puolijoki, H.; Mustonen, J.; Pettersson, E.; Pasternack, A.; Lahdensuo, A. Proteinuria and haematuria are frequently present in patients with lung cancer. Nephrol. Dial. Transplant. 1989, 4, 947–950. [Google Scholar] [CrossRef] [PubMed]
- Da’As, N.; Polliack, A.; Cohen, Y.; Amir, G.; Darmon, D.; Kleinman, Y.; Goldfarb, A.W.; Ben-Yehuda, D. Kidney involvement and renal manifestations in non-Hodgkin’s lymphoma and lymphocytic leukemia: A retrospective study in 700 patients. Eur. J. Haematol. 2001, 67, 158–164. [Google Scholar] [CrossRef]
- Li, S.-J.; Chen, H.-P.; Chen, Y.-H.; Zhang, L.-H.; Tu, Y.-M.; Liu, Z.-H. Renal involvement in non-hodgkin lymphoma: Proven by renal biopsy. PLoS ONE 2014, 9, e95190. [Google Scholar] [CrossRef]
- Poitou-Verkinder, A.-L.; Francois, A.; Drieux, F.; Lepretre, S.; Legallicier, B.; Moulin, B.; Godin, M.; Guerrot, D. The spectrum of kidney pathology in B-cell chronic lymphocytic leukemia / small lymphocytic lymphoma: A 25-year multicenter experience. PLoS ONE 2015, 10, e0119156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhaveri, K.D.; Shah, H.H.; Calderon, K.; Campenot, E.S.; Radhakrishnan, J. Glomerular diseases seen with cancer and chemotherapy: A narrative review. Kidney Int. 2013, 84, 34–44. [Google Scholar] [CrossRef] [Green Version]
- Wanchoo, R.; Ramirez, C.B.; Barrientos, J.; Jhaveri, K.D. Renal involvement in chronic lymphocytic leukemia. Clin. Kidney J. 2018, 11, 670–680. [Google Scholar] [CrossRef] [Green Version]
- Obrador, G.T.; Price, B.; O’Meara, Y.; Salant, D.J. Acute renal failure due to lymphomatous infiltration of the kidneys. J. Am. Soc. Nephrol. 1997, 8, 1348–1354. [Google Scholar] [PubMed]
- Xiao, J.C.; Walz-Mattmüller, R.; Ruck, P.; Horny, H.P.; Kaiserling, E. Renal involvement in myeloproliferative and lymphoproliferative disorders. A study of autopsy cases. Gen. Diagn. Pathol. 1997, 142, 147–153. [Google Scholar] [PubMed]
- Javaugue, V.; Debiais-Delpech, C.; Nouvier, M.; Gand, E.; Chauvet, S.; Ecotiere, L.; Desport, E.; Goujon, J.-M.; Delwail, V.; Guidez, S.; et al. Clinicopathological spectrum of renal parenchymal involvement in B-cell lymphoproliferative disorders. Kidney Int. 2019, 96, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Said, S.M.; Leung, N.; Sethi, S.; Cornell, L.D.; Fidler, M.E.; Grande, J.P.; Herrmann, S.; Tefferi, A.; D’Agati, V.D.; Nasr, S.H. Myeloproliferative neoplasms cause glomerulopathy. Kidney Int. 2011, 80, 753–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaunat, O.; Delahousse, M.; Fakhouri, F.; Martinez, F.; Stephan, J.-L.; Noël, L.-H.; Karras, A. Nephrotic syndrome associated with hemophagocytic syndrome. Kidney Int. 2006, 69, 1892–1898. [Google Scholar] [CrossRef] [Green Version]
- Rieu, P.; Noël, L.H.; Droz, D.; Beaufils, H.; Gessain, A.; Hermine, O.; Lesavre, P. Glomerular involvement in lymphoproliferative disorders with hyperproduction of cytokines (Castleman, POEMS). Adv. Nephrol. Necker Hosp. 2000, 30, 305–331. [Google Scholar] [PubMed]
- Frizzera, G.; Peterson, B.A.; Bayrd, E.D.; Goldman, A. A systemic lymphoproliferative disorder with morphologic features of Castleman’s disease: Clinical findings and clinicopathologic correlations in 15 patients. J. Clin. Oncol. 1985, 3, 1202–1216. [Google Scholar] [CrossRef]
- Schmitz, R.; Stanelle, J.; Hansmann, M.-L.; Küppers, R. Pathogenesis of classical and lymphocyte-predominant Hodgkin lymphoma. Ann. Rev. Pathol. 2009, 4, 151–174. [Google Scholar] [CrossRef]
- Plager, J.; Stutzman, L. Acute nephrotic syndrome as a manifestation of active Hodgkin’s disease. Am. J. Med. 1971, 50, 56–66. [Google Scholar] [CrossRef]
- Kramer, P.; Sizoo, W.; E Twiss, E. Nephrotic syndrome in Hodgkin’s disease. Report of five cases and review of the literature. Neth. J. Med. 1981, 24, 114–119. [Google Scholar]
- Eagen, J.W.; Lewis, E.J. Glomerulopathies of neoplasia. Kidney Int. 1977, 11, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Audard, V.; Larousserie, F.; Grimbert, P.; Abtahi, M.; Sotto, J.-J.; Delmer, A.; Boue, F.; Nochy, D.; Brousse, N.; Delarue, R.; et al. Minimal change nephrotic syndrome and classical Hodgkin’s lymphoma: Report of 21 cases and review of the literature. Kidney Int. 2006, 69, 2251–2260. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, N.; Batwara, R.; McCarthy, E.T.; Sharma, R.; Sharma, M.; Savin, V.J. Serum permeability activity in steroid-resistant minimal change nephrotic syndrome is abolished by treatment of Hodgkin disease. Am. J. Kidney Dis. 2007, 50, 826–829. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, A.V.; Zimmerman, S.W.; Burkholder, P.M. Nephrotic syndrome in Hodgkin’s disease. Evidence for pathogenesis alternative to immune complex deposition. Am. J. Med. 1976, 61, 471–477. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Audard, V.; Fan, Q.; Pawlak, A.; Lang, P.; Sahali, D. Immunopathogenesis of idiopathic nephrotic syndrome with relapse. Contrib. Nephrol. 2011, 169, 94–106. [Google Scholar] [PubMed] [Green Version]
- Kapp, U.; Yeh, W.-C.; Patterson, B.; Elia, A.J.; Kägi, D.; Ho, A.; Hessel, A.; Tipsword, M.; Williams, A.; Mirtsos, C.; et al. Interleukin 13 is secreted by and stimulates the growth of Hodgkin and Reed-Sternberg cells. J. Exp. Med. 1999, 189, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Skinnider, B.F.; Elia, A.J.; Gascoyne, R.D.; Trümper, L.H.; Von Bonin, F.; Kapp, U.; Patterson, B.; E Snow, B.; Mak, T.W. Interleukin 13 and interleukin 13 receptor are frequently expressed by Hodgkin and Reed-Sternberg cells of Hodgkin lymphoma. Blood 2001, 97, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Van Den Berg, J.G.; Aten, J.; Chand, M.A.; Claessen, N.; Dijkink, L.; Wijdenes, J.; Lakkis, F.G.; Wenning, J.J. Interleukin-4 and interleukin-13 act on glomerular visceral epithelial cells. J. Am. Soc. Nephrol. 2000, 11, 413–422. [Google Scholar] [PubMed]
- Lai, K.-W.; Wei, C.-L.; Tan, L.-K.; Tan, P.-H.; Chiang, G.S.; Lee, C.G.; Jordan, S.C.; Yap, H.-K. Overexpression of interleukin-13 induces minimal-change—Like nephropathy in rats. J. Am. Soc. Nephrol. 2007, 18, 1476–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, S.; Yokote, T.; Kobayashi, K.; Hirata, Y.; Akioka, T.; Hiraoka, N.; Oka, S.; Miyoshi, T.; Takubo, T.; Tsuji, M.; et al. Minimal-change nephrotic syndrome preceding Hodgkin lymphoma by 5 years with expression of tumor necrosis factor α in Hodgkin-Reed-Sternberg cells. Hum. Pathol. 2010, 41, 1196–1199. [Google Scholar] [CrossRef] [PubMed]
- Sahali, D.; Sendeyo, K.; Mangier, M.; Audard, V.; Zhang, S.Y.; Lang, P.; Ollero, M.; Pawlak, A. Immunopathogenesis of idiopathic nephrotic syndrome with relapse. Semin. Immunopathol. 2014, 36, 421–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audard, V.; Zhang, S.-Y.; Copie-Bergman, C.; Rucker-Martin, C.; Ory, V.; Candelier, M.; Baia, M.; Lang, P.; Pawlak, A.; Sahali, D. Occurrence of minimal change nephrotic syndrome in classical Hodgkin lymphoma is closely related to the induction of c-mip in Hodgkin-Reed Sternberg cells and podocytes. Blood 2010, 115, 3756–3762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kofman, T.; Zhang, S.-Y.; Copie-Bergman, C.; Moktefi, A.; Raimbourg, Q.; Francois, H.; Karras, A.; Plaisier, E.; Painchart, B.; Favre, G.; et al. Minimal change nephrotic syndrome associated with non-Hodgkin lymphoid disorders: A retrospective study of 18 cases. Medicine 2014, 93, 350–358. [Google Scholar] [CrossRef]
- Hallek, M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am. J. Hematol. 2019, 94, 1266–1287. [Google Scholar] [CrossRef] [Green Version]
- Strati, P.; Nasr, S.H.; Leung, N.; Hanson, C.A.; Chaffee, K.G.; Schwager, S.M.; Achenbach, S.J.; Call, T.G.; Parikh, S.A.; Ding, W.; et al. Renal complications in chronic lymphocytic leukemia and monoclonal B-cell lymphocytosis: The Mayo Clinic experience. Haematologica 2015, 100, 1180–1188. [Google Scholar] [CrossRef] [Green Version]
- Moulin, B.; Ronco, P.M.; Mougenot, B.; Francois, A.; Fillastre, J.-P.; Mignon, F. Glomerulonephritis in chronic lymphocytic leukemia and related B-cell lymphomas. Kidney Int. 1992, 42, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Scott, R.B. Leukaemia. Lancet 1957, 272, 1162–1167. [Google Scholar] [CrossRef]
- Seney, F.D.; Federgreen, W.R.; Stein, H.; Kashgarian, M. A review of nephrotic syndrome associated with chronic lymphocytic leukemia. Arch Intern. Med. 1986, 146, 137–141. [Google Scholar] [CrossRef]
- Van Wynsberghe, M.; Lenain, P.; Drieux, F.; Guerrot, D.; Bertrand, D. Monoclonal B lymphocytosis and minimal change disease: A new monoclonal B-cell disorder of renal significance? J. Nephrol. 2017, 31, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Vial, R.; Daniel, L.; Devos, M.; Bouchacourt, B.; Cazajous, G.; Sichez, H.; Mazodier, K.; Lankester, M.; Gobert, P.; Seguier, J.; et al. Chronic lymphoid leukemia and renal complication: Report on 10 cases from Marseille over 16 years. Rev. Med. Interne 2018, 39, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Kastritis, E. How I treat Waldenström macroglobulinemia. Blood 2019, 134, 2022–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audard, V.; Georges, B.; Vanhille, P.; Toly-Ndour, C.; Deroure, B.; Fakhouri, F.; Cuvelier, R.; Belenfant, X.; Surin, B.; Aucouturier, P.; et al. Renal lesions associated with IgM-secreting monoclonal proliferations: Revisiting the disease spectrum. Clin. J. Am. Soc. Nephrol. 2008, 3, 1339–1349. [Google Scholar] [CrossRef] [PubMed]
- Chauvet, S.; Bridoux, F.; Ecotière, L.; Javaugue, V.; Sirac, C.; Arnulf, B.; Thierry, A.; Quellard, N.; Milin, S.; Bender, S.; et al. Kidney diseases associated with monoclonal immunoglobulin M–secreting B-cell lymphoproliferative disorders: A case series of 35 patients. Am. J. Kidney Dis. 2015, 66, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Higgins, L.; Nasr, S.H.; Said, S.M.; Kapoor, P.; Dingli, D.; King, R.L.; Rajkumar, S.V.; Kyle, R.A.; Kourelis, T.; Gertz, M.A.; et al. Kidney involvement of patients with Waldenström macroglobulinemia and other IgM-producing B cell lymphoproliferative disorders. Clin. J. Am. Soc. Nephrol. 2008, 13, 1037–1046. [Google Scholar] [CrossRef]
- Vos, J.M.; Gustine, J.; Rennke, H.G.; Hunter, Z.; Manning, R.J.; Dubeau, T.E.; Meid, K.; Minnema, M.C.; Kersten, M.-J.; Treon, S.P.; et al. Renal disease related to Waldenström macroglobulinaemia: Incidence, pathology and clinical outcomes. Br. J. Haematol. 2016, 175, 623–630. [Google Scholar] [CrossRef]
- Da Silva, W.F., Jr.; de Farias Pinho, L.L.; de Farias, C.L.G.; Torres, V.; Costalonga, E.C.; Filho, G.C.; de Abreu Testagrossa, L.; Rocha, V.; Buccheri, V. Renal infiltration presenting as acute kidney injury in Hodgkin lymphoma—A case report and review of the literature. Leuk. Res. Rep. 2018, 10, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Uprety, D.; Peterson, A.; Shah, B.K. Renal failure secondary to leukemic infiltration of kidneys in CLL—A case report and review of literature. Ann. Hematol. 2013, 92, 271–273. [Google Scholar] [CrossRef]
- Corlu, L.; Rioux-Leclercq, N.; Ganard, M.; Decaux, O.; Houot, R.; Vigneau, C. Renal dysfunction in patients with direct infiltration by B-cell lymphoma. Kidney Int. Rep. 2019, 4, 688–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Törnroth, T.; Heiro, M.; Marcussen, N.; Franssila, K. Lymphomas diagnosed by percutaneous kidney biopsy. Am. J. Kidney Dis. 2003, 42, 960–971. [Google Scholar] [CrossRef] [PubMed]
- Attias, P.; Moktefi, A.; Matignon, M.; Dupuis, J.; Debiais-Delpech, C.; Grimbert, P.; Lang, P.; Audard, V. Monotypic plasma cell interstitial nephritis as the only clinical manifestation in a patient with previously undiagnosed indolent multiple myeloma: A case report. Medicine 2016, 95, e4391. [Google Scholar] [CrossRef] [PubMed]
- Spivak, J.L. Myeloproliferative neoplasms. N. Engl. J. Med. 2017, 376, 2168–2181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, A.S.; Møller, J.B.; Hasselbalch, H.C. Chronic kidney disease in patients with the Philadelphia-negative chronic myeloproliferative neoplasms. Leuk. Res. 2014, 38, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Benn, C.L.; Dua, P.; Gurrell, R.; Loudon, P.; Pike, A.; Storer, R.I.; Vangjeli, C. Physiology of hyperuricemia and urate-lowering treatments. Front. Med. 2018, 5, 160. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5990632/ (accessed on 27 October 2020). [CrossRef] [Green Version]
- Özpolat, T.; Kayar, Y. Acute renal infarction: A presentation of essential thrombocytosis. Kidney Int. 2017, 92, 1292. [Google Scholar] [CrossRef] [PubMed]
- Carobbio, A.; Ferrari, A.; Masciulli, A.; Ghirardi, A.; Barosi, G.; Barbui, T. Leukocytosis and thrombosis in essential thrombocythemia and polycythemia vera: A systematic review and meta-analysis. Blood Adv. 2019, 3, 1729–1737. [Google Scholar] [CrossRef]
- Agarwal, A.; Morrone, K.; Bartenstein, M.; Zhao, Z.J.; Verma, A.; Goel, S. Bone marrow fibrosis in primary myelofibrosis: Pathogenic mechanisms and the role of TGF-β. Stem Cell Investig. 2016, 3, 5. [Google Scholar] [PubMed]
- Steurer, M.; Zoller, H.; Augustin, F.; Fong, D.; Heiss, S.; Strasser-Weippl, K.; Gastl, G.; Tzankov, A. Increased angiogenesis in chronic idiopathic myelofibrosis: Vascular endothelial growth factor as a prominent angiogenic factor. Hum. Pathol. 2007, 38, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Pippin, J.W.; Terada, Y.; Shankland, S.J. The cyclin-dependent kinase inhibitor p21 is required for TGF-beta1-induced podocyte apoptosis. Kidney Int. 2005, 68, 1618–1629. [Google Scholar] [CrossRef] [Green Version]
- Schiffer, M.; Bitzer, M.; Roberts, I.S.; Kopp, J.B.; ten Dijke, P.; Mundel, P.; Bottinger, E. Apoptosis in podocytes induced by TGF-beta and Smad7. J. Clin. Investig. 2001, 108, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Belliere, J.; Colombat, M.; Kounde, C.; Recher, C.; Ribes, D.; Huart, A.; Chauveau, D.; Demas, V.; Luquet, I.; Beyne-Rauzy, O.; et al. Kidney involvement in patients with chronic myelomonocytic leukemia or BCR-ABL–Negative myeloproliferative neoplasms. Kidney Int. Rep. 2021, 6, 737–745. Available online: https://kireports.org/article/S2468-0249(20)31802-7/abstract (accessed on 7 January 2021). [CrossRef] [PubMed]
- Alexander, M.P.; Nasr, S.H.; Kurtin, P.J.; Casey, E.T.; Hernandez, L.P.H.; E Fidler, M.; Sethi, S.; Cornell, L.D. Renal extramedullary hematopoiesis: Interstitial and glomerular pathology. Mod. Pathol. 2015, 28, 1574–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquet, F.; Pavic, M.; Ninet, J.; Hot, A. Auto-immune diseases and cancers. Second part: Auto-immune diseases complicating cancers and their treatment. Rev. Med. Interne 2014, 35, 656–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saitoh, T.; Murakami, H.; Uchiumi, H.; Moridaira, K.; Maehara, T.; Matsushima, T.; Tsukamoto, N.; Tamura, J.; Karasawa, M.; Naruse, T.; et al. Myelodysplastic syndromes with nephrotic syndrome. Am. J. Hematol. 1999, 60, 200–204. [Google Scholar] [CrossRef]
- Pinheiro, R.F.; Silva, M.R.R.; Chauffaille, M.D.L.L. The 5q- syndrome and autoimmune phenomena: Report of three cases. Leuk. Res. 2006, 30, 507–510. [Google Scholar] [CrossRef]
- Morschhauser, F.; Wattel, E.; Pagniez, D.; Lovi, V.; Rose, C.; Bauters, F.; Fenaux, P. Glomerular injury in chronic myelomonocytic leukemia. Leuk. Lymphoma 1995, 18, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Bogdanović, R.; Kuzmanović, M.; Marković-Lipkovski, J.; Ognjanović, M.; Mićić, D.; Stanković, I.; Stajic, N.; Nikolic, V.; Bunjevacki, G. Glomerular involvement in myelodysplastic syndromes. Pediatr. Nephrol. 2001, 16, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Schwotzer, N.; Provot, F.; Ville, S.; Daniel, L.; Le Fur, A.; Kissling, S.; Jourde-Chiche, N.; Karras, A.; Moreau, A.; Augusto, J.-F.; et al. Spectrum of kidney involvement in patients with myelodysplastic syndromes. Kidney Int. Rep. 2021, 6, 746–754. Available online: https://www.kireports.org/article/S2468-0249(20)31864-7/abstract (accessed on 7 January 2021). [CrossRef]
- Dispenzieri, A.; Fajgenbaum, D.C. Overview of Castleman disease. Blood 2020, 135, 1353–1364. [Google Scholar] [CrossRef]
- Yuan, X.-G.; Hu, W.; Chen, F.-F.; Huang, B.-F.; Zhao, X.-Y. Renal complications of Castleman’s disease: Report of two cases and analysis of 75 cases. Clin. Exp. Nephrol. 2011, 15, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C. Novel insights and therapeutic approaches in idiopathic multicentric Castleman disease. Hematology 2018, 2018, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagayama, Y.; Yamano, M.; Yagame, M.; Nariyama, T.; Takahashi, M.; Kawamoto, M.; Matsui, K. TAFRO syndrome as a cause of glomerular microangiopathy: A case report and literature review. BMC Nephrol. 2019, 20, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, H.; Sawa, N.; Watanabe, S.; Ikuma, D.; Sekine, A.; Kawada, M.; Yamanouchi, M.; Hasegawa, E.; Suwabe, T.; Hoshino, J.; et al. The clinical and histopathological feature of renal manifestation of TAFRO syndrome. Kidney Int. Rep. 2020, 5, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Dispenzieri, A. POEMS Syndrome: 2019 Update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2019, 94, 812–827. [Google Scholar] [CrossRef] [Green Version]
- Dispenzieri, A.; Kyle, R.A.; Lacy, M.Q.; Rajkumar, S.V.; Therneau, T.M.; Larson, D.R.; Greipp, P.R.; Witzig, T.E.; Basu, R.; Suarez, G.A.; et al. POEMS syndrome: Definitions and long-term outcome. Blood 2003, 101, 2496–2506. [Google Scholar] [CrossRef]
- Jourde-Chiche, N.; Dussol, B.; Daniel, L. Kidney involvement in hematologic malignancies. Diagnostic approach. Rev. Med. Interne 2010, 31, 685–696. [Google Scholar] [CrossRef]
- Nakamoto, Y.; Imai, H.; Yasuda, T.; Wakui, H.; Miura, A.B. A spectrum of clinicopathological features of nephropathy associated with POEMS syndrome. Nephrol. Dial. Transplant. 1999, 14, 2370–2386. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yan, Y.; Sui, Z.; Dong, B.; Zuo, L. A case report of POEMS syndrome with renal involvement as immunotactoid glomerulopathy. Medicine 2018, 97, e9920. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5851753/ (accessed on 3 January 2021). [CrossRef]
- Lambotte, O.; Dürrbach, A.; Ammor, M.; Paradis, V.; Djeffal, R.; Machover, D.; Charpentier, B. Association of a POEMS syndrome and light chain deposit disease: First case report. Clin. Nephrol. 2001, 55, 482–486. [Google Scholar] [PubMed]
- Janka, G.E. Hemophagocytic syndromes. Blood Rev. 2007, 21, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, S.; Woo, P.; Murray, K.J. Macrophage activation syndrome: A potentially fatal complication of rheumatic disorders. Arch. Dis. Child. 2001, 85, 421–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, J.B.; Nelson, G.W.; Sampath, K.; Johnson, R.C.; Genovese, G.; An, P.; Friedman, D.; Briggs, W.; Dart, R.; Korbet, S.; et al. APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J. Am. Soc. Nephrol. 2011, 22, 2129–2137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amoura, A.; Moktefi, A.; Halfon, M.; Karras, A.; Rafat, C.; Gibier, J.-B.; Gleeson, P.J.; Servais, A.; Argy, N.; Maillé, P.; et al. Malaria, Collapsing glomerulopathy, and focal and segmental glomerulosclerosis. Clin. J. Am. Soc. Nephrol. 2020, 15, 964–972. Available online: https://cjasn.asnjournals.org/content/early/2020/05/21/CJN.00590120 (accessed on 3 January 2021). [CrossRef] [PubMed]
- Santoriello, D.; Hogan, J.; D’Agati, V.D. Hemophagocytic syndrome with histiocytic glomerulopathy and intraglomerular hemophagocytosis. Am. J. Kidney Dis. 2016, 67, 978–983. [Google Scholar] [CrossRef]
- Eirin, A.; Irazabal, M.V.; Fervenza, F.C.; Sethi, S. Histiocytic glomerulopathy associated with macrophage activation syndrome. Clin. Kidney J. 2015, 8, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, M.E.; Goodfellow, J.A. A practical approach to managing patients with Myasthenia Gravis—Opinions and a review of the literature. Front. Neurol. 2020, 11, 60. Available online: www.ncbi.nlm.nih.gov/pmc/articles/PMC7358547/ (accessed on 30 October 2020). [CrossRef] [PubMed]
- Hoffacker, V.; Schultz, A.; Tiesinga, J.J.; Gold, R.; Schalke, B.; Nix, W.; Kiefer, R.; Müller-Hermelink, H.K.; Marx, A. Thymomas alter the T-cell subset composition in the blood: A potential mechanism for thymoma-associated autoimmune disease. Blood 2000, 96, 3872–3879. [Google Scholar] [CrossRef]
- Karras, A.; De Montpreville, V.; Fakhouri, F.; Grünfeld, J.-P.; Lesavre, P. Renal and thymic pathology in thymoma-associated nephropathy: Report of 21 cases and review of the literature. Nephrol. Dial. Transplant. 2005, 20, 1075–1082. [Google Scholar] [CrossRef] [Green Version]
- Le Berre, L.; Hervé, C.; Buzelin, F.; Usual, C.; Soulillou, J.-P.; Dantal, J. Renal macrophage activation and Th2 polarization precedes the development of nephrotic syndrome in Buffalo/Mna rats. Kidney Int. 2005, 68, 2079–2090. [Google Scholar] [CrossRef] [Green Version]
- Le Berre, L.; Godfrin, Y.; Günther, E.; Buzelin, F.; Perretto, S.; Smit, H.; Kerjachki, D.; Usal, C.; Cuturi, C.; Soulillou, J.-P.; et al. Extrarenal effects on the pathogenesis and relapse of idiopathic nephrotic syndrome in Buffalo/Mna rats. J. Clin. Investig. 2002, 109, 491–498. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hematological Malignancies | Ig Deposits Non-Related Glomerular Diseases Reported in the Literature |
|---|---|
| Thymoma | MCD, MN, ANCA+ crescentic GN, FSGS, TMA |
| Castleman | TMA, crescentic GN, MCD, FSGS, AA amyloidosis |
| TAFRO syndrome | MPGN-like and TMA-like lesion, glomerular endotheliopathy without thrombi |
| POEMS syndrome | TMA-like lesion, mesangial proliferative GN, endarteritis-like lesion |
| HPS | FSGS, MCD, TMA, Histiocytosis glomerulopathy |
| Myelodysplastic syndrome | Mesangial proliferative GN, FSGS, MCD, IR-like GN, TMA, IgAN, MN, C3 glomerulopathy, fibrillary GN |
| MPN disorders | Mesangial proliferative GN, FSGS, TMA, MPN-related glomerulopathy (specific pattern) |
| PV | FSGS, mesangial proliferative GN, IgAN, TMA, EMH, AML infiltration, IR-like GN |
| CML | MCD, MPGN, MN, IgAN, TMA |
| CMML | IR-like GN, TMA, monocyte (CD61+) infiltration within glomerulus |
| PMF | FSGS, mesangioproliferative GN, EMH, IR-like GN |
| ET | FSGS, mesangioproliferative GN, IgAN, TMA |
| Hodgkin lymphoma | AA amyloidosis, MCD, FSGS, MN, MPGN and anti-GBM or pauci-immune crescentic GN |
| Non-Hodgkin lymphoma | MPGN, crescentic GN, MCD, FSGS, MN, TMA, mesangial proliferative GN |
| CLL/SLL/MBL | MPGN, MN, MCD, FSGS, crescentic GN, mesangial proliferative GN, TMA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morel, A.; Meuleman, M.-S.; Moktefi, A.; Audard, V. Renal Diseases Associated with Hematologic Malignancies and Thymoma in the Absence of Renal Monoclonal Immunoglobulin Deposits. Diagnostics 2021, 11, 710. https://doi.org/10.3390/diagnostics11040710
Morel A, Meuleman M-S, Moktefi A, Audard V. Renal Diseases Associated with Hematologic Malignancies and Thymoma in the Absence of Renal Monoclonal Immunoglobulin Deposits. Diagnostics. 2021; 11(4):710. https://doi.org/10.3390/diagnostics11040710
Chicago/Turabian StyleMorel, Antoine, Marie-Sophie Meuleman, Anissa Moktefi, and Vincent Audard. 2021. "Renal Diseases Associated with Hematologic Malignancies and Thymoma in the Absence of Renal Monoclonal Immunoglobulin Deposits" Diagnostics 11, no. 4: 710. https://doi.org/10.3390/diagnostics11040710
APA StyleMorel, A., Meuleman, M. -S., Moktefi, A., & Audard, V. (2021). Renal Diseases Associated with Hematologic Malignancies and Thymoma in the Absence of Renal Monoclonal Immunoglobulin Deposits. Diagnostics, 11(4), 710. https://doi.org/10.3390/diagnostics11040710