
Novel App-Based Portable Spirometer for the Early Detection of COPD

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
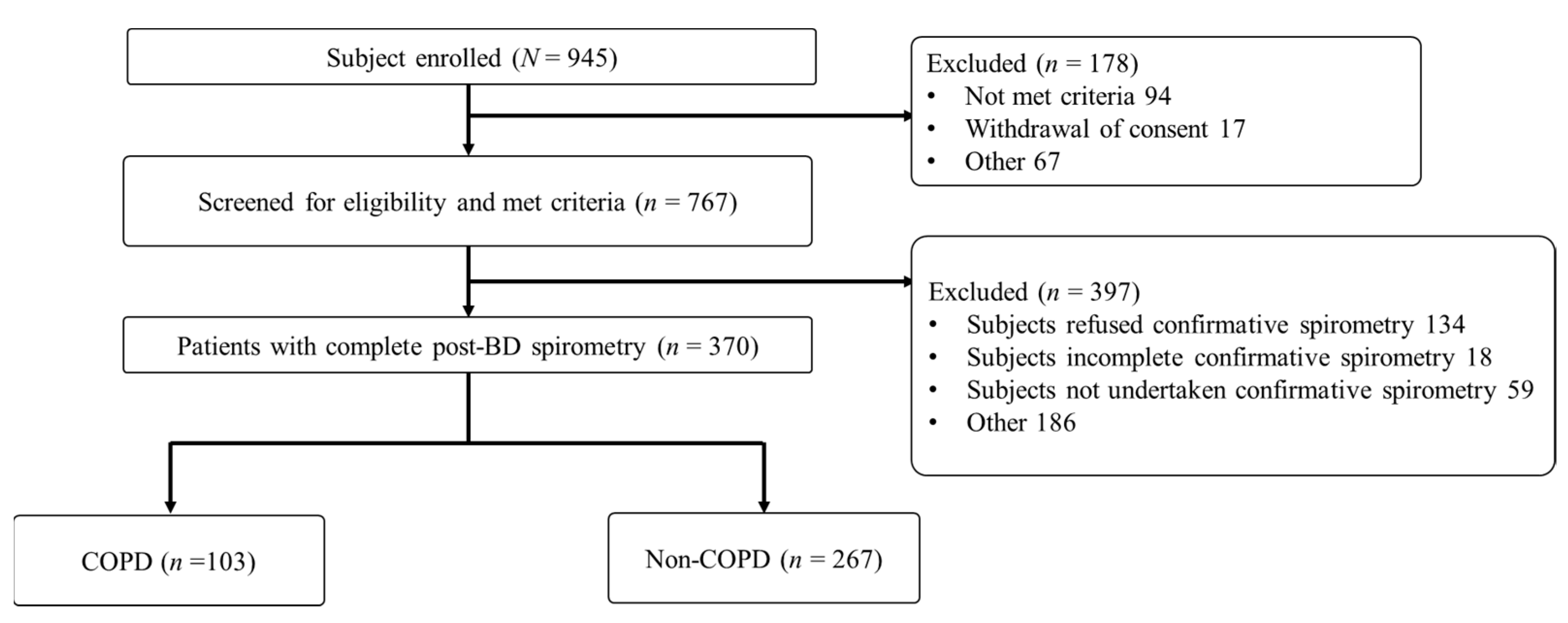
2.2. Study Participants
2.3. Study Procedures
2.4. Devices and System
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Study Participants
3.2. Agreement between Post-BD FEV1/FVC Ratios Measured Using the Confirmatory Spirometry and Pre-BD FEV1/FVC Ratios Measured Using Spirobank Smart
3.3. ROC Curves and Diagnostic Accuracy for the Pre-BD FEV1/FVC Ratios Measured Using Spirobank Smart
3.4. GOLD Classification and CAT Score of Participants Based on the FEV1 Values Obtained Using Confirmatory Spirometry and Spirobank Smart
3.5. Associations of FEV1/FVC Determined Using Spirobank Smart and the Participant Characteristic Variables with the COPD Incidence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COPD | chronic obstructive pulmonary disease |
| FVC | forced vital capacity |
| FEV1 | forced expiratory volume in 1 s |
| FEV6 | forced expiratory volume in 6 s |
| ROC | receiver operating characteristic |
| AUROC | area under the ROC curve |
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Contreras-Garza, B.M.; Xiong, W.; Guo, X.; Orozco-Hernández, J.P.; Pacheco-Gallego, M.; Montoya-Martínez, J.J.; Celli, B.R.; A Wedzicha, J. Update on Clinical Aspects of COPD. N. Engl. J. Med. 2019, 381, 2484–2486. [Google Scholar] [CrossRef]
- Hwang, S.L.; Lin, Y.C.; Guo, S.E.; Chi, M.C.; Chou, C.T.; Lin, C.M. Prevalence of chronic obstructive pulmonary disease in Southwest-ern Taiwan: A population-based study. J. Respir. Pulm. Med. 2016, 3, 1–4. [Google Scholar]
- Diab, N.; Gershon, A.S.; Sin, D.D.; Tan, W.C.; Bourbeau, J.; Boulet, L.P.; Aaron, S.D. Underdiagnosis and Overdiagnosis of Chronic Ob-structive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2018, 198, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.; Thomas, M. Screening for COPD: The gap between logic and evidence. Eur. Respir. Rev. 2017, 26, 160113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Roisin, R.; Rabe, K.F.; Vestbo, J.; Vogelmeier, C.; Agustí, A.; all previous and current members of the Science Commit-tee and the Board of Directors of GOLD (goldcopd.org/committees/). Global Initiative for Chronic Obstructive Lung Disease (GOLD) 20th Anniversary: A brief history of time. Eur. Respir. J. 2017, 50, 1700671. [Google Scholar] [CrossRef] [Green Version]
- Heffler, E.; Crimi, C.; Mancuso, S.; Campisi, R.; Puggioni, F.; Brussino, L.; Crimi, N. Misdiagnosis of asthma and COPD and underuse of spirometry in primary care unse-lected patients. Respir. Med. 2018, 142, 48–52. [Google Scholar] [CrossRef]
- Fujita, M.; Nagashima, K.; Takahashi, S.; Suzuki, K.; Fujisawa, T.; Hata, A. Handheld flow meter improves COPD detectability regardless of using a conventional questionnaire: A split-sample validation study. Respirology 2019, 25, 191–197. [Google Scholar] [CrossRef]
- Blain, E.; Craig, T. The Use of Spirometry in a Primary Care Setting. J. Allergy Clin. Immunol. 2008, 121, S81. [Google Scholar] [CrossRef] [Green Version]
- Schermer, T.R.; Vatsolaki, M.; Behr, R.; Grootens, J.; Cretier, R.; Akkermans, R.; Denis, J.; Poels, P.; Bemt, L.V.D. Point of care microspirometry to facilitate the COPD diagnostic process in primary care: A clustered randomised trial. NPJ Prim. Care Respir. Med. 2018, 28, 17. [Google Scholar] [CrossRef]
- US Preventive Services Task Force (USPSTF); Siu, A.L.; Bibbins-Domingo, K.; Grossman, D.C.; Davidson, K.W.; Epling, J.W., Jr.; García, F.A.; Gillman, M.; Kemper, A.R.; Krist, A.H.; et al. Screening for Chronic Obstructive Pulmo-nary Disease: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 1372–1377. [Google Scholar] [PubMed] [Green Version]
- Guirguis-Blake, J.M.; Senger, C.A.; Webber, E.M.; Mularski, R.A.; Whitlock, E.P. Screening for Chronic Obstructive Pulmonary Dis-ease: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 1378–1393. [Google Scholar] [CrossRef] [Green Version]
- Yawn, B.P.; Martinez, F.J. POINT: Can Screening for COPD Improve Outcomes? Yes. Chest 2020, 157, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Hemmingsen, U.B.; Stycke, M.; Dollerup, J.; Poulsen, P.B. Guideline-Based Early Detection of Chronic Obstructive Pulmonary Disease in Eight Danish Municipalities: The TOP-KOM Study. Pulm. Med. 2017, 2017, 7620397. [Google Scholar] [CrossRef]
- Martinez, F.J.; O’Connor, G.T. Screening, Case-Finding, and Outcomes for Adults with Unrecognized COPD. JAMA 2016, 315, 1343–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra, V.H.; Mezquita, M.Á.H.; Cobos, L.P.; Sánchez, M.G.; Castellanos, R.D.; Sánchez, S.J.; Pérez, R.C.; Ferrero, M. Usefulness of The Piko-6 Portable Device for Early COPD Detection in Primary Care. Utilidad del dispositivo portátil Piko-6 para la detección precoz de la enfermedad pul-monar obstructiva crónica en atención primaria. Arch Bronconeumol. 2018, 54, 460–466. [Google Scholar] [CrossRef]
- Sichletidis, L.; Spyratos, D.; Papaioannou, M.; Chloros, D.; Tsiotsios, A.; Tsagaraki, V.; Haidich, A.B. A combination of the IPAG questionnaire and PiKo-6® flow meter is a val-uable screening tool for COPD in the primary care setting. Prim. Care Respir. J. 2011, 20, 184–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjeldgaard, P.; Lykkegaard, J.; Spillemose, H.; Ulrik, C.S. Multicenter study of the COPD-6 screening device: Feasible for early detection of chronic obstructive pulmonary disease in primary care? Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2323–2331. [Google Scholar] [CrossRef] [Green Version]
- Dickens, A.P.; Fitzmaurice, D.A.; Adab, P.; Sitch, A.; Riley, R.D.; Enocson, A.; Jordan, R.E. Accuracy of Vitalograph lung monitor as a screening test for COPD in primary care. NPJ Prim. Care Respir. Med. 2020, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ramos Hernández, C.; Núñez Fernández, M.; Pallares Sanmartín, A.; Mouronte Roibas, C.; Cerdeira Domínguez, L.; Botana Rial, M.I.; Cid, N.B.; Villar, A.F. Validation of the portable Air-Smart Spirometer. PLoS ONE 2018, 13, e0192789. [Google Scholar] [CrossRef]
- Exarchos, K.P.; Gogali, A.; Sioutkou, A.; Chronis, C.; Peristeri, S.; Kostikas, K. Validation of the portable Bluetooth® Air Next spi-rometer in patients with different respiratory diseases. Respir. Res. 2020, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Ring, B.; Burbank, A.J.; Mills, K.; Ivins, S.; Dieffenderfer, J.; Hernandez, M.L. Validation of an app-based portable spirometer in ad-olescents with asthma. J. Asthma 2019, 58, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Degryse, J.; Buffels, J.; Van Dijck, Y.; Decramer, M.; Nemery, B. Accuracy of office spirometry performed by trained primary-care physicians using the MIR Spirobank Smart hand-held spirometer. Respiration 2012, 83, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.; Stanojevic, S.; Cole, T.; Baur, X.; Hall, G.; Culver, B.; Enright, P.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Tinkelman, D.G.; Price, D.B.; Nordyke, R.J.; Halbert, R.J. COPD screening efforts in primary care: What is the yield? Prim. Care Respir. J. 2007, 16, 41–48. [Google Scholar] [CrossRef]
- Hang, L.W.; Hsu, J.Y.; Chang, C.J.; Wang, H.C.; Cheng, S.L.; Lin, C.H.; Chan, M.C.; Wang, C.C.; Perng, D.W.; Yu, C.J. Predictive factors war-rant screening for obstructive sleep apnea in COPD: A Taiwan National Survey. Int. J. Chronic Obstr. Pulm. Dis. 2016, 30, 665–673. [Google Scholar]
- Su, K.-C.; Ko, H.-K.; Chou, K.-T.; Hsiao, Y.-H.; Su, V.Y.-F.; Perng, D.-W.; Kou, Y.R. An accurate prediction model to identify undiagnosed at-risk patients with COPD: A cross-sectional case-finding study. NPJ Prim. Care Respir. Med. 2019, 29, 22. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Lee, C.M.; Park, J.Y.; Kim, J.H.; Park, S.H.; Jang, S.H.; Jung, K.; Yoo, K.H.; Park, Y.B.; Rhee, C.K.; et al. Active case finding strategy for chronic obstructive pulmonary disease with handheld spi-rometry. Medicine 2016, 95, e5683. [Google Scholar] [CrossRef]
- Frith, P.; Crockett, A.; Beilby, J.; Marshall, D.; Attewell, R.; Ratnanesan, A.; Gavagna, G. Simplified COPD screening: Validation of the PiKo-6® in primary care. Prim. Care Respir. J. 2011, 20, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Melbye, H.; Medbø, A.; Crockett, A. The FEV1/FEV6 ratio is a good substitute for the FEV1/FVC ratio in the elderly. Prim. Care Respir. J. 2006, 15, 294–298. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Gong, W.; Tian, Y.; Zhou, J. FEV1/FEV6 in Primary Care Is a Reliable and Easy Method for the Diagnosis of COPD. Respir. Care 2015, 61, 349–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, T.; Ikitimur, H.D.; Koc, N.; Yildirim, N. The role of FEV6 in the detection of airway obstruction. Respir. Med. 2005, 99, 103–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.J. The lower limit of normal versus a fixed ratio to assess airflow limitation: Will the debate ever end? Eur. Respir. J. 2018, 51, 1800403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enright, P.; Brusasco, V. Counterpoint: Should we abandon FEV₁/FVC <0.70 to detect airway obstruction? Yes. Chest 2010, 138, 1040–1042. [Google Scholar]
- Swanney, M.P.; Ruppel, G.; Enright, P.L.; Pedersen, O.F.; Crapo, R.O.; Miller, M.R.; Jensen, R.L.; Falaschetti, E.; Schouten, J.P.; Hankinson, J.L.; et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax 2008, 63, 1046–1051. [Google Scholar] [CrossRef] [Green Version]
- Güder, G.; Brenner, S.; Angermann, C.E.; Ertl, G.; Held, M.; Sachs, A.P.; Lammers, J.-W.; Zanen, P.; Hoes, A.W.; Störk, S.; et al. GOLD or lower limit of normal definition? a comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study. Respir. Res. 2012, 13, 13. [Google Scholar] [CrossRef] [Green Version]
- van den Bemt, L.; Wouters, B.C.; Grootens, J.; Denis, J.; Poels, P.J.; Schermer, T.R. Diagnostic accuracy of pre-bronchodilator FEV1/FEV6 from microspirometry to detect airflow obstruction in primary care: A randomised cross-sectional study. NPJ Prim. Care Respir. Med. 2014, 14, 14033. [Google Scholar] [CrossRef] [Green Version]
- Lewer, D.; McKee, M.; Gasparrini, A.; Reeves, A.; De Oliveira, C. Socioeconomic position and mortality risk of smoking: Evidence from the English Longitudinal Study of Ageing (ELSA). Eur. J. Public Health 2017, 27, 1068–1073. [Google Scholar] [CrossRef] [Green Version]
- Bikov, A.; Lange, P.; Anderson, J.A.; Brook, R.D.; Calverley, P.M.A.; Celli, B.R.; Cowans, N.J.; Crim, C.; Dixon, I.J.; Martinez, F.J.; et al. FEV1 is a stronger mortality predictor than FVC in patients with moderate COPD and with an increased risk for cardiovascular disease. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 1135–1142. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-COPD | COPD | Total | p-Value |
|---|---|---|---|---|
| Sample size | 267 | 103 | 370 | - |
| Age (mean ± SD) | 59.0 ± 9.0 | 65.7 ± 9.8 | 60.9 ± 9.7 | <0.001 |
| <55 years | 93 (34.8%) | 17 (16.5%) | 110 (29.7%) | <0.001 |
| 55–59 years | 46 (17.2%) | 9 (8.7%) | 55 (14.9%) | |
| 60–64 years | 56 (21%) | 17 (16.5%) | 73 (19.7%) | |
| ≥65 years | 72 (27%) | 60 (58.3%) | 132 (35.7%) | |
| Gender | ||||
| Male | 253 (94.8%) | 96 (93.2%) | 349 (94.3%) | 0.536 |
| Female | 14 (5.2%) | 7 (6.8%) | 21 (5.7%) | |
| BMI | 25.81 ± 3.86 | 24.38 ± 4.13 | 25.41 ± 3.98 | 0.001 |
| Cough | ||||
| No | 24 (9.0%) | 4 (3.9%) | 28 (7.6%) | 0.096 |
| Yes | 243 (91.0%) | 99 (96.1%) | 342 (92.4%) | |
| Phlegm | ||||
| No | 30 (11.2%) | 9 (8.7%) | 39 (10.5%) | 0.483 |
| Yes | 237 (88.8%) | 94 (91.3%) | 331 (89.5%) | |
| Breathless | ||||
| No | 91 (34.1%) | 24 (23.3%) | 115 (31.1%) | 0.045 |
| Yes | 176 (65.9%) | 79 (76.7%) | 255 (68.9%) | |
| CAT | 9 ± 6 | 12 ± 7 | 10 ± 6 | |
| 0–9 | 160 (59.9%) | 43 (41.7%) | 203 (54.9%) | 0.001 |
| 10–19 | 94 (35.2%) | 44 (42.7%) | 138 (37.3%) | |
| 20–29 | 12 (4.5%) | 15 (14.6%) | 27 (7.3%) | |
| 30–40 | 1 (0.4%) | 1 (1.0%) | 2 (0.5%) | |
| Smoking pack-years | 39.4 ± 27.5 | 48.6 ± 29.3 | 42.6 ± 28.3 | 0.001 |
| <50 | 216 (80.9%) | 67 (65.0%) | 283 (76.5%) | <0.001 |
| ≥50 | 51(19.1%) | 36 (35.0%) | 87 (23.5%) | |
| Pre-bronchodilator FEV1/FVC determined using Spirobank Smart | 81.78 ± 7.44 | 63.57 ± 13.37 | 76.71 ± 12.49 | <0.001 |
| Post-bronchodilator FEV1/FVC determined using a diagnostic spirometer | 81.28 ± 7.19 | 59.06 ± 9.04 | 75.1 ± 12.62 | <0.001 |
| Device Cutoff Ratio (FEV1/FVC) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | AUROC (95% CI) |
|---|---|---|---|---|---|
| <70% | 70.90% | 95.88% | 86.90% | 89.50% | 0.834 (0.779–0.889) |
| <71% | 73.80% | 94.01% | 82.60% | 90.30% | 0.839 (0.786–0.892) |
| <72% | 77.70% | 93.63% | 82.50% | 91.60% | 0.857 (0.806–0.907) |
| <73% | 80.60% | 92.88% | 81.40% | 92.50% | 0.867 (0.819–0.916) |
| <74% | 82.50% | 92.13% | 80.20% | 93.20% | 0.873 (0.827–0.920) |
| <75% | 86.40% | 84.64% | 68.50% | 94.20% | 0.855 (0.810–0.901) |
| <76% | 87.40% | 82.02% | 65.20% | 94.40% | 0.847 (0.801–0.893) |
| GOLD Grade | Diagnostic Spirometer | Spirobank Smart | ||
|---|---|---|---|---|
| n (%) | CAT Score | n (%) | CAT Score | |
| GOLD I | 25 (24.3%) | 10 ± 5 | 16 (15.5%) | 10 ± 4 |
| GOLD II | 53 (51.5%) | 12 ± 7 | 59 (57.3%) | 11 ± 6 |
| GOLD III | 22 (21.3%) | 11 ± 6 | 22 (21.4%) | 13 ± 8 |
| GOLD IV | 3 (2.9%) | 21 ± 19 | 6 (5.8%) | 18 ± 12 |
| Total | 103 (100%) | 12 ± 7 | 103 (100%) | 12 ± 7 |
| Variables | Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|
| Portable spirometer: FEV1/FVC< 74% | 55.14 (28.13–108.77) | <0.001 | 58.58 (27.29–125.75) | <0.001 |
| Smoking PY ≥ 50 | 2.28 (1.37–3.78) | 0.001 | 1.31 (0.57–2.98) | 0.535 |
| Age category | ||||
| Age < 55 | 1 | 1 | ||
| 55 ≤ age < 60 | 1.07 (0.44–2.59) | 0.864 | 1.12 (0.32–3.886) | 0.864 |
| 60 ≤ age < 65 | 1.66 (0.79–3.51) | 0.185 | 3.23 (1.04–10.07) | 0.04 |
| Age ≥ 65 | 4.56 (2.45–8.48) | <0.001 | 5.82 (2.22–15.27) | <0.001 |
| CAT category | ||||
| 0–9 | 1 | 1 | ||
| 10–19 | 1.74 (1.07–2.85) | 0.027 | 1.39 (0.65–2.98) | 0.393 |
| 20–29 | 4.65 (2.03–10.67) | <0.001 | 3.43 (0.99–11.29) | 0.052 |
| 30–40 | 3.72 (0.23–60.71) | 0.356 | 5.89 (0.06–613.56) | 0.535 |
| BMI | 0.907 (0.85–0.97) | 0.002 | ||
| Gender (male) | 0.759 (0.30–1.94) | 0.759 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Cheng, S.-L.; Wang, H.-C.; Hsu, W.-H.; Lee, K.-Y.; Perng, D.-W.; Lin, H.-I.; Lin, M.-S.; Tsai, J.-R.; Wang, C.-C.; et al. Novel App-Based Portable Spirometer for the Early Detection of COPD. Diagnostics 2021, 11, 785. https://doi.org/10.3390/diagnostics11050785
Lin C-H, Cheng S-L, Wang H-C, Hsu W-H, Lee K-Y, Perng D-W, Lin H-I, Lin M-S, Tsai J-R, Wang C-C, et al. Novel App-Based Portable Spirometer for the Early Detection of COPD. Diagnostics. 2021; 11(5):785. https://doi.org/10.3390/diagnostics11050785
Chicago/Turabian StyleLin, Ching-Hsiung, Shih-Lung Cheng, Hao-Chien Wang, Wu-Huei Hsu, Kang-Yun Lee, Diahn-Warng Perng, Hen-I. Lin, Ming-Shian Lin, Jong-Rung Tsai, Chin-Chou Wang, and et al. 2021. "Novel App-Based Portable Spirometer for the Early Detection of COPD" Diagnostics 11, no. 5: 785. https://doi.org/10.3390/diagnostics11050785
APA StyleLin, C. -H., Cheng, S. -L., Wang, H. -C., Hsu, W. -H., Lee, K. -Y., Perng, D. -W., Lin, H. -I., Lin, M. -S., Tsai, J. -R., Wang, C. -C., Lin, S. -H., Wang, C. -Y., Chen, C. -Z., Yang, T. -M., Liu, C. -L., Wang, T. -Y., & Lin, M. -C. (2021). Novel App-Based Portable Spirometer for the Early Detection of COPD. Diagnostics, 11(5), 785. https://doi.org/10.3390/diagnostics11050785