
Morphology and Position of the Right Atrioventricular Valve in Relation to Right Atrial Structures

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Dissection and Measurements
2.3. Statistical Analysis
3. Results
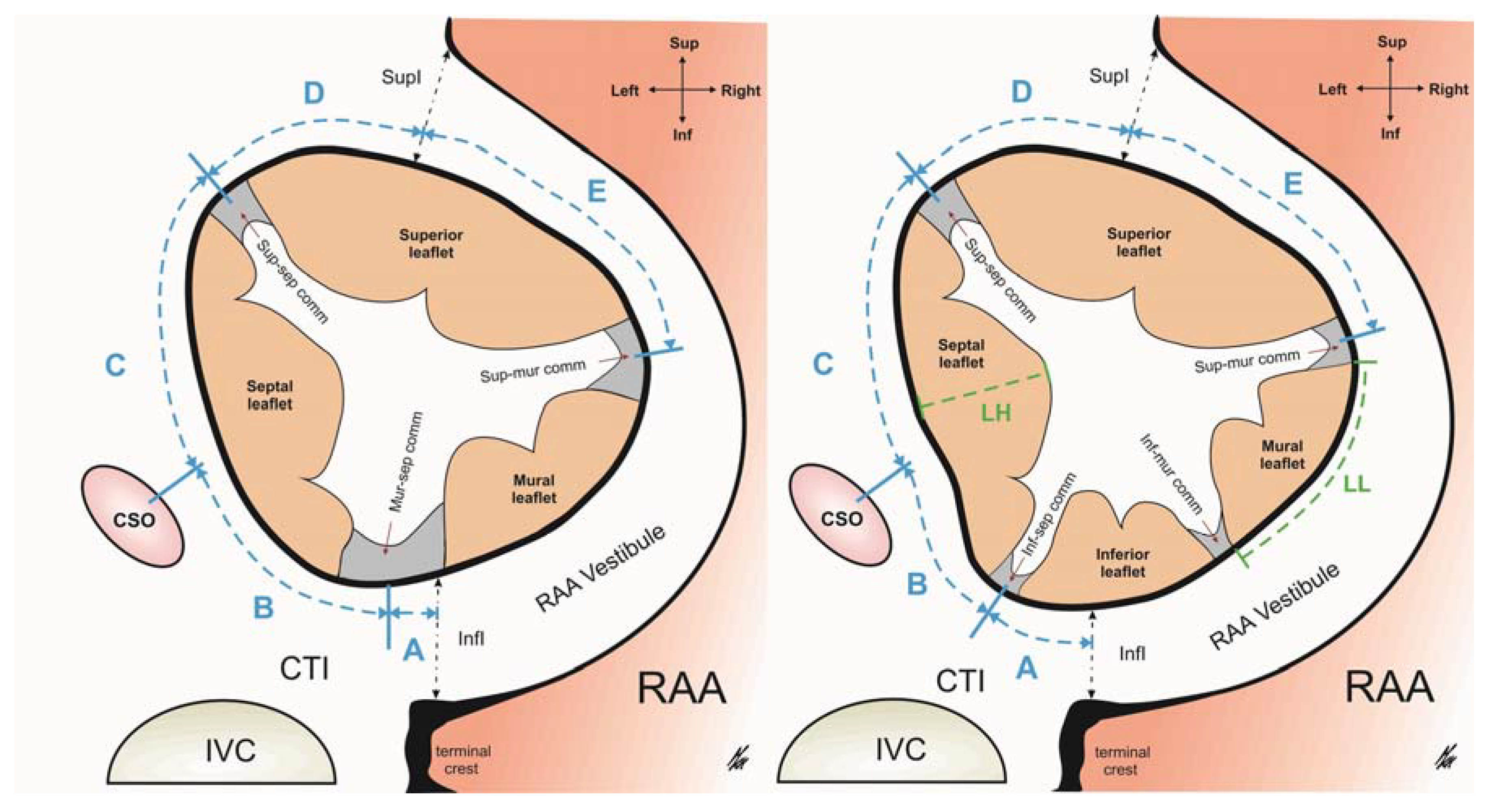
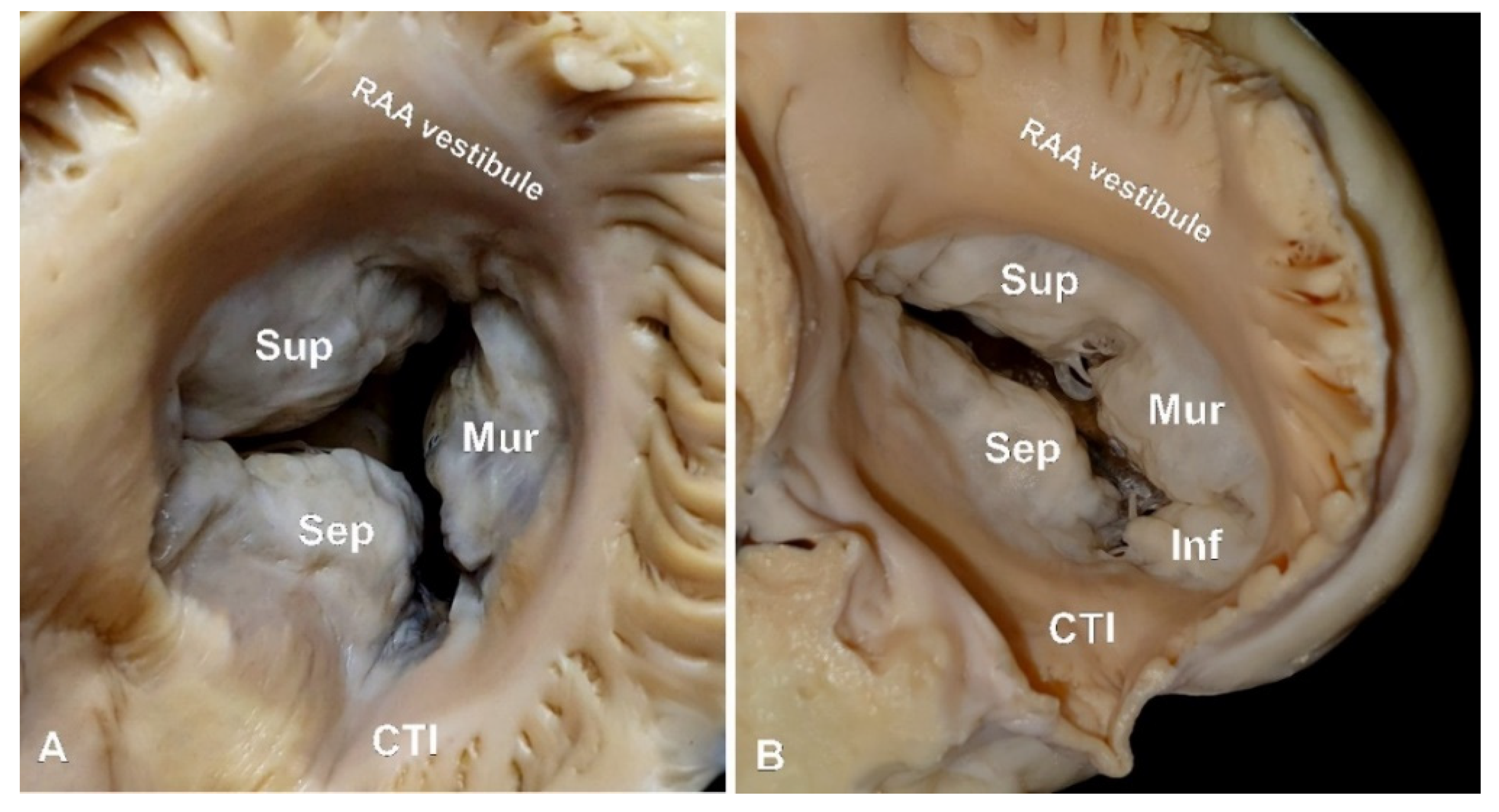
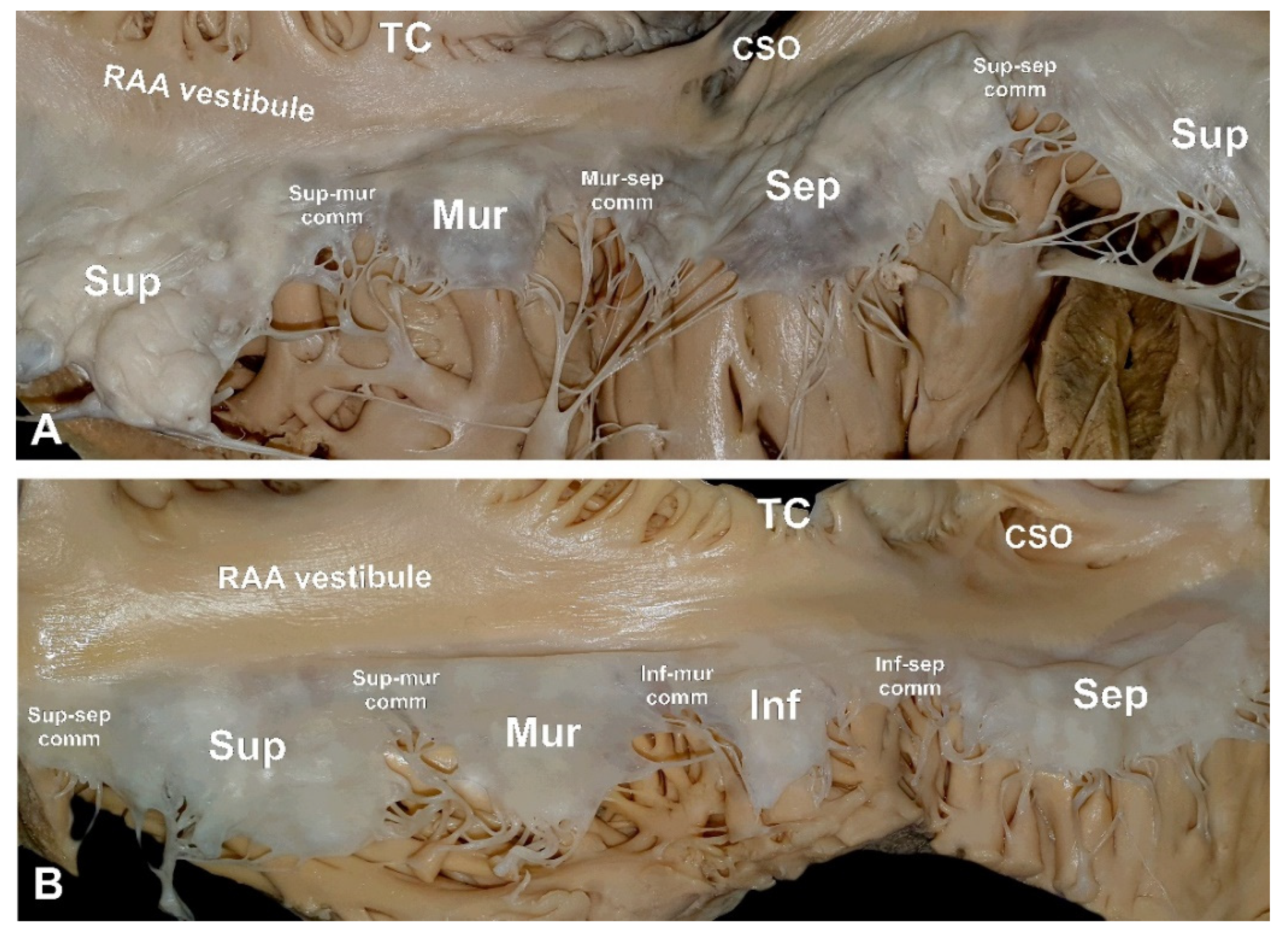
3.1. The RAV Morphology
3.2. The Spatial Position of the RAV
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antunes, M.J.; Barlow, J.B. Management of tricuspid valve regurgitation. Heart 2007, 52, 271–276. [Google Scholar]
- Van Praet, K.M.; Stamm, C.; Starck, C.T.; Sündermann, S.; Meyer, A.; Montagner, M.; Nazari Shafti, T.Z.; Unbehaun, A.; Jacobs, S.; Falk, V.; et al. An overview of surgical treatment modalities and emerging transcatheter interventions in the management of tricuspid valve regurgitation. Expert Rev. Cardiovasc. Ther. 2018, 16, 75–89. [Google Scholar] [CrossRef]
- Chang, B.C.; Lim, S.H.; Yi, G.; Hong, Y.S.; Lee, S.; Yoo, K.Y.; Kang, M.S.; Cho, B.C. Long-term clinical results of tricuspid valve replacement. Ann. Thorac Surg. 2006, 81, 1317–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassileva, C.M.; Shabosky, J.; Boley, T.; Markwell, S.; Hazelrigg, S. Tricuspid valve surgery: The past 10 years from the Nationwide Inpatient Sample (NIS) database. J. Thorac Cardiovasc. Surg. 2012, 143, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Asmarats, L.; Puri, R.; Latib, A.; Navia, J.L.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Interventions: Landscape, Challenges and Future Directions. J. Am. Coll Cardiol. 2018, 71, 2935–2956. [Google Scholar] [CrossRef] [PubMed]
- Arsalan, M.; Walther, T.; Smith, R.L.; Grayburn, P.A. Tricuspid regurgitation diagnosis and treatment. Eur. Heart J. 2017, 71, 2935–2956. [Google Scholar] [CrossRef] [Green Version]
- Rodes-Cabau, J.; Hahn, R.T.; Latib, A.; Laule, M.; Lauten, A.; Maisano, F.; Schofer, J.; Campelo-Parada, F.; Puri, R.; Vahanian, A. Transcatheter Therapies for Treating Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2016, 67, 1829–1845. [Google Scholar] [CrossRef]
- Besler, C.; Meduri, C.U.; Lurz, P. Transcatheter treatment of functional tricuspid regurgitation using the Trialign device. Interv. Cardiol. Rev. 2018, 13, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Muntane-Carol, G.; Alperi, A.; Faroux, L.; Bédard, E.; Philippon, F.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Intervention: Coaptation Devices. Front. Cardiovasc. Med. 2020, 7, 139. [Google Scholar] [CrossRef]
- Holda, M.K.; Zhingre Sanchez, J.D.; Bateman, M.G.; Iaizzo, P.A. Right Atrioventricular Valve Leaflet Morphology Redefined. JACC Cardiovasc. Interv. 2019, 12, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.P.; Pluchinotta, F.R. Tricuspid Valve: Embryology and Anatomy. In The Tricuspid Valve in Congenital Heart Disease, 1st ed.; Springer: Milan, Italy, 2014; pp. 1–11. [Google Scholar]
- Dahou, A.; Levin, D.; Reisman, M.; Hahn, R.T. Anatomy and Physiology of the Tricuspid Valve. JACC Cardiovasc. Imaging 2019, 12, 458–468. [Google Scholar] [CrossRef]
- Bateman, M.G.; Quill, J.L.; Hill, A.J.; Iaizzo, P.A. The Clinical Anatomy and Pathology of the Human Atrioventricular Valves: Implications for Repair or Replacement. J. Cardiovasc. Transl. Res. 2013, 6, 155–165. [Google Scholar] [CrossRef]
- Hill, A.J. Attitudinally Correct Cardiac Anatomy. In Handbook of Cardiac Anatomy, Physiology, and Devices, 3rd ed.; Springer: Cham, Switzerland, 2015; pp. 15–21. [Google Scholar]
- Krawczyk-Ozog, A.; Holda, M.K.; Sorysz, D.; Koziej, M.; Siudak, Z.; Dudek, D.; Klimek-Piotrowska, W. Morphologic variability of the mitral valve leaflets. J. Thorac. Cardiovasc. Surg 2017, 154, 1927–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krawczyk-Ozog, A.; Holda, M.K.; Bolechała, F.; Siudak, Z.; Sorysz, D.; Dudek, D.; Klimek-Piotrowska, W. Anatomy of the mitral subvalvular apparatus. J. Thorac. Cardiovasc. Surg 2018, 155, 2002–2010. [Google Scholar] [CrossRef]
- Van Rosendael, P.J.; Kamperidis, V.; Kong, W.K.F.; Van Rosendael, A.R.; Van der Kley, F.; Marsan, N.A.; Delgado, V.; Bax, J.J. Computed tomography for planning transcatheter tricuspid valve therapy. Eur. Heart J. 2017, 38, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Saremi, F.; Hassani, C.; Millan-Nunez, V.; Sanchez-Quintana, D. Imaging Evaluation of Tricuspid Valve: Analysis of Morphology and Function with CT and MRI. Am. J. Roentgenol. 2015, 204, 531–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anwar, A.M.; Geleijnse, M.L.; Soliman, O.I.I.; McGhie, J.S.; Frowijn, R.; Nemes, A.; Van den Bosch, A.E.; Galema, T.W.; Ten Cate, F.J. Assessment of normal tricuspid valve anatomy in adults by real-time three-dimensional echocardiography. Int. J. Cardiovasc. Imaging 2007, 23, 717–724. [Google Scholar] [CrossRef] [Green Version]
- Owais, K.; Taylor, C.E.; Jiang, L.; Khabbaz, K.R.; Montealegre-Gallegos, M.; Matyal, R.; Gorman, J.H.; Gorman, R.C.; Mahmood, F. Tricuspid annulus: A three-dimensional deconstruction and reconstruction. Ann. Thorac. Surg 2014, 98, 1536–1542. [Google Scholar] [CrossRef]
- Holda, J.; Slodowska, K.; Tyrak, K.; Bolechała, F.; Jasińska, K.A.; Koziej, M.; Hołda, M.K.; Walocha, J.A. Topographical anatomy of the right atrial appendage vestibule and its isthmuses. J. Cardiovasc. Electrophysiol. 2020, 31, 3199–3206. [Google Scholar] [CrossRef] [PubMed]
- Klimek-Piotrowska, W.; Holda, M.K.; Koziej, M.; Hołda, J.; Piątek, K.; Tyrak, K.; Bolechała, F. Clinical Anatomy of the Cavotricuspid Isthmus and Terminal Crest. PLoS ONE 2016, 11, e0163383. [Google Scholar] [CrossRef] [Green Version]
- Holda, M.K.; Klimek-Piotrowska, W.; Koziej, M.; Mazur, M. Anatomical variations of the coronary sinus valve (Thebesian valve): Implications for electrocardiological procedures. Europace 2015, 17, 921–927. [Google Scholar] [PubMed] [Green Version]
- Klimek-Piotrowska, W.; Holda, M.K.; Koziej, M.; Salapa, K.; Piątek, K.; Holda, J. Geometry of Koch’s triangle. Europace 2017, 19, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Holda, J.; Słodowska, K.; Strona, M.; Bolechała, F.; Jasińska, K.A.; Malinowska, K.; Koziej, M.; Walocha, J.A.; Hołda, M.K. Mutual arrangements of coronary blood vessels within the right atrial appendage vestibule. Authorea 2021, 1, 1–8. [Google Scholar]
- Schofer, J.; Bijuklic, K.; Tiburtius, C.; Hansen, L.; Groothuis, A.; Hahn, R.T. First-in-human transcatheter tricuspid valve repair in a patient with severely regurgitant tricuspid valve. J. Am. Coll. Cardiol. 2015, 65, 1190–1195. [Google Scholar] [CrossRef] [Green Version]
- Latib, A.; Agricola, E.; Pozzoli, A.; Denti, P.; Taramasso, M.; Spagnolo, P.; Juliard, J.M.; Brochet, E.; Ou, P.; Enriquez-Sarano, M.; et al. First-in-man implantation of a tricuspid annular remodeling device for functional tricuspid regurgitation. JACC Cardiovasc. Interv. 2015, 8, 211–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, A.; McCarthy, K.P.; Sanchez-Quintana, D.; Yen Ho, S. Right atrial appendage and vestibule: Further anatomical insights with implications for invasive electrophysiology. Europeace 2013, 15, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Holda, M.K.; Klimek-Piotrowska, W.; Koziej, M.; Piątek, K.; Hołda, J. Influence of different fixation protocols on the preservation and dimensions of cardiac tissue. J. Anat. 2016, 229, 334–340. [Google Scholar] [CrossRef]
- Holda, M.K.; Holda, J.; Koziej, M.; Tyrak, K.; Klimek-Piotrowska, W. The influence of fixation on the cardiac tissue in a 1-year observation of swine hearts. Anat. Histol. Embryol. 2018, 47, 501–509. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | 3-Leaflet Valves (n = 134) | 4-Leaflet Valves (n = 66) | p-Value | |
|---|---|---|---|---|
| Sex (% females) | 20.9 | 24.2 | 0.597 | |
| Age (years) | 47.1 ± 18.2 (18–94) | 46.5 ± 18.4 (21–87) | 0.827 | |
| BMI (kg/m2) | 26.3 ± 4.8 (15.2–39.6) | 27.5 ± 4.1 (17.4–37.8) | 0.083 | |
| Heart weight (g) | 407.9 ± 86.5 (230.0–606.5) | 419.3 ± 75.8 (274.5–620.0) | 0.363 | |
| Valve perimeter (mm) | 109.3 ± 11.3 (86.6–156.8) | 119.2 ± 11.1 (96.5–143.4) | <0.001 | |
| Leaflet length (mm) | superior leaflet | 30.1 ± 9.2 (12.6–71.0) | 28.8 ± 9.0 (11.5–50.5) | 0.09 |
| septal leaflet | 30.5 ± 5.7 (17.7–46.6) | 27.0 ± 5.7 (17.8–39.4) | 0.005 | |
| mural leaflet | 17.5 ± 6.2 (5.9–44.5) | 14.8 ± 5.5 (7.2–28.0) | <0.001 | |
| inferior leaflet * | - | 14.3 ± 4.6 (8.2–26.5) | - | |
| Leaflet height (mm) | superior leaflet | 12.6 ± 4.2 (3.5–23.7) | 13.7 ± 5.1 (4.6–26.7) | 0.11 |
| septal leaflet | 11.8 ± 3.9 (3.3–20.8) | 14.3 ± 4.5 (5.2–22.8) | <0.001 | |
| mural leaflet | 11.9 ± 3.6 (4.0–20.7) | 13.6 ± 4.0 (4.4–23.8) | 0.003 | |
| inferior leaflet * | - | 12.1 ± 8.6 (2.3–19.6) | - | |
| Commissure length (mm) | supero-septal | 9.6 ± 3.4 (5.1–21.5) | 8.6 ± 4.7 (4.2–24.5) | 0.17 |
| supero-mural | 9.9 ± 4.0 (3.5–21.4) | 7.5 ± 2.2 (4.0–14.3) | <0.001 | |
| muro-septal ** | 14.0 ± 4.8 (4.5–25.9) | - | - | |
| infero-septal * | - | 7.9 ± 3.0 (2.9–18.2) | - | |
| infero-mural * | - | 7.7 ± 2.4 (3.5–13.5) | - | |
| A—RAAV inferior isthmus to muro-septal ** or infero-septal * commissure (mm) † | 5.8 ± 9.4 (−15.6–29.7) | 13.5 ± 6.4 (0.0–27.9) | <0.001 | |
| B—coronary sinus ostium to muro-septal ** or infero-septal * commissure (mm) ‡ | 16.1 ± 9.0 (−12.7–33.2) | 7.7 ± 6.3 (-10.5–22.6) | <0.001 | |
| C—coronary sinus ostium to supero-septal commissure (mm) | 20.1 ± 5.6 (5.3–36.7) | 20.5 ± 5.1 (9.8–29.2) | 0.62 | |
| D—RAAV superior isthmus to supero-septal commissure (mm) | 7.3 ± 3.8 (1.3–14.3) | 6.2 ± 5.3 (1.4–14.8) | 0.09 | |
| E—RAAV superior isthmus to supero-mural commissure (mm) | 33.9 ± 11.2 (17.5–72.7) | 31.1 ± 9.6 (11.9–51.6) | 0.08 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hołda, J.; Słodowska, K.; Malinowska, K.; Strona, M.; Mazur, M.; Jasińska, K.A.; Matuszyk, A.; Koziej, M.; Walocha, J.A.; Hołda, M.K. Morphology and Position of the Right Atrioventricular Valve in Relation to Right Atrial Structures. Diagnostics 2021, 11, 960. https://doi.org/10.3390/diagnostics11060960
Hołda J, Słodowska K, Malinowska K, Strona M, Mazur M, Jasińska KA, Matuszyk A, Koziej M, Walocha JA, Hołda MK. Morphology and Position of the Right Atrioventricular Valve in Relation to Right Atrial Structures. Diagnostics. 2021; 11(6):960. https://doi.org/10.3390/diagnostics11060960
Chicago/Turabian StyleHołda, Jakub, Katarzyna Słodowska, Karolina Malinowska, Marcin Strona, Małgorzata Mazur, Katarzyna A. Jasińska, Aleksandra Matuszyk, Mateusz Koziej, Jerzy A. Walocha, and Mateusz K. Hołda. 2021. "Morphology and Position of the Right Atrioventricular Valve in Relation to Right Atrial Structures" Diagnostics 11, no. 6: 960. https://doi.org/10.3390/diagnostics11060960
APA StyleHołda, J., Słodowska, K., Malinowska, K., Strona, M., Mazur, M., Jasińska, K. A., Matuszyk, A., Koziej, M., Walocha, J. A., & Hołda, M. K. (2021). Morphology and Position of the Right Atrioventricular Valve in Relation to Right Atrial Structures. Diagnostics, 11(6), 960. https://doi.org/10.3390/diagnostics11060960