
Limitation of Screening of Different Variants of SARS-CoV-2 by RT-PCR



Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. RT-PCR SARS-CoV-2 and Variants Detection
2.3. NGS Sequencing
3. Results
3.1. Prevalence of SARS-CoV-2 Variants




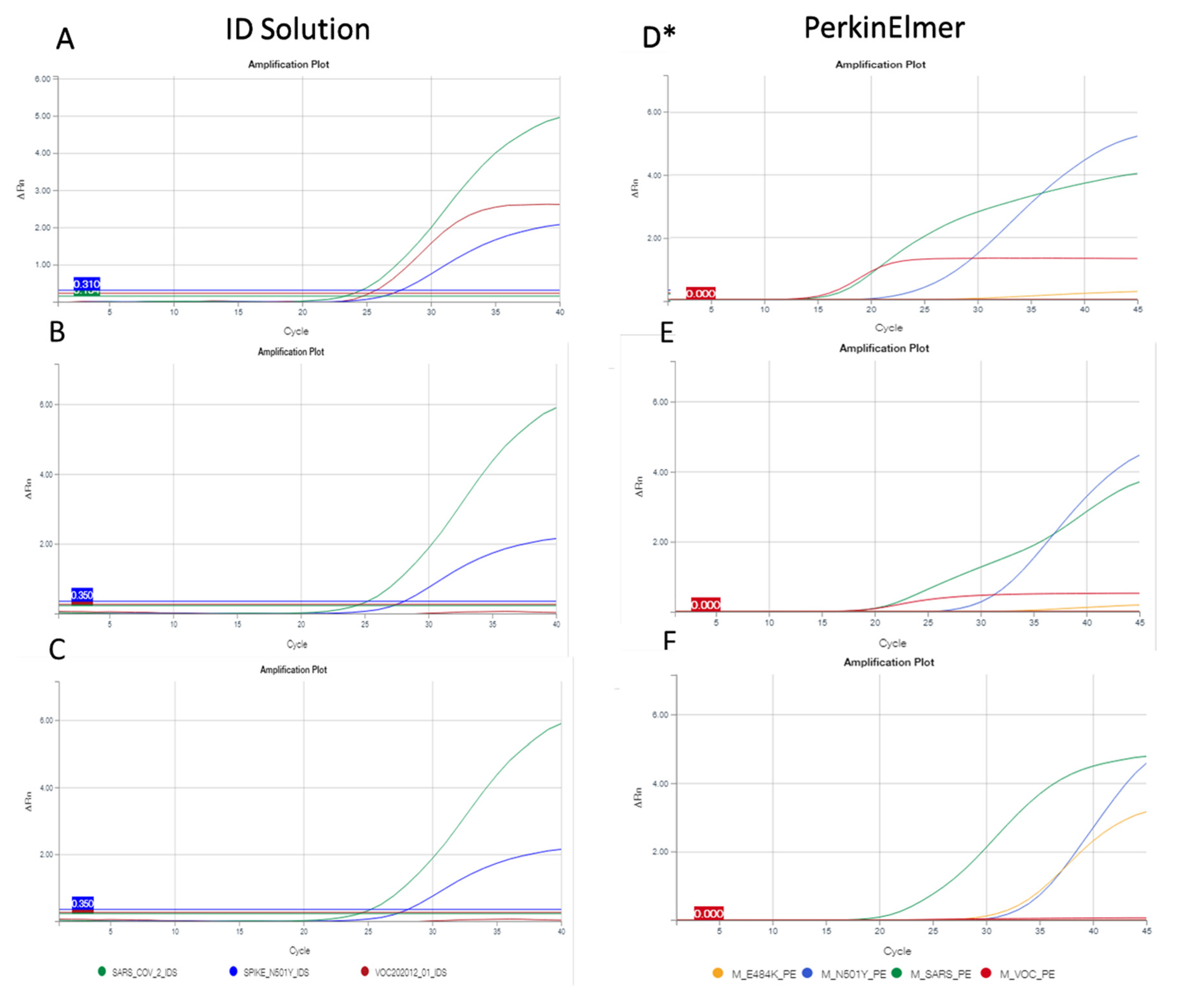
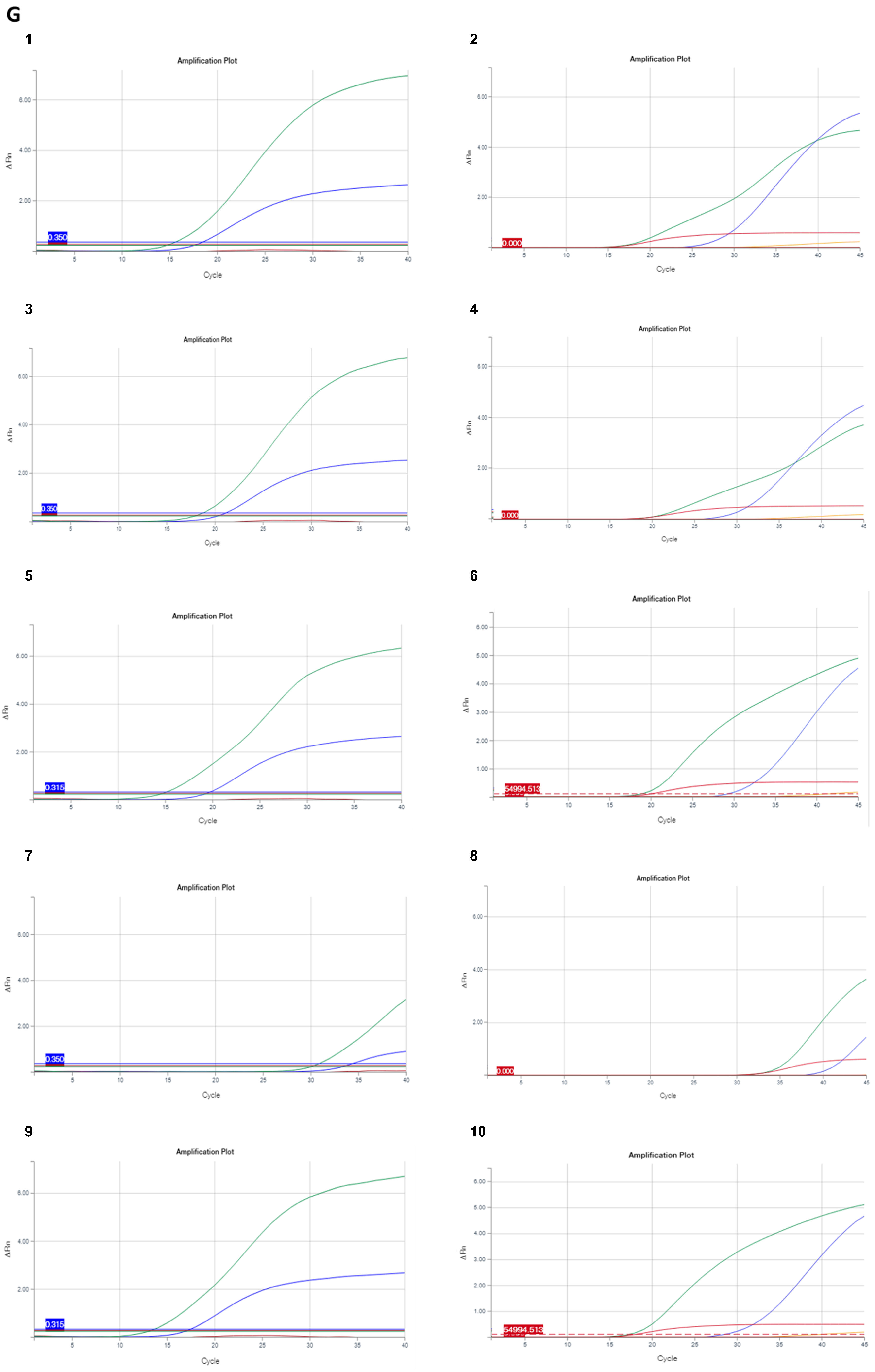
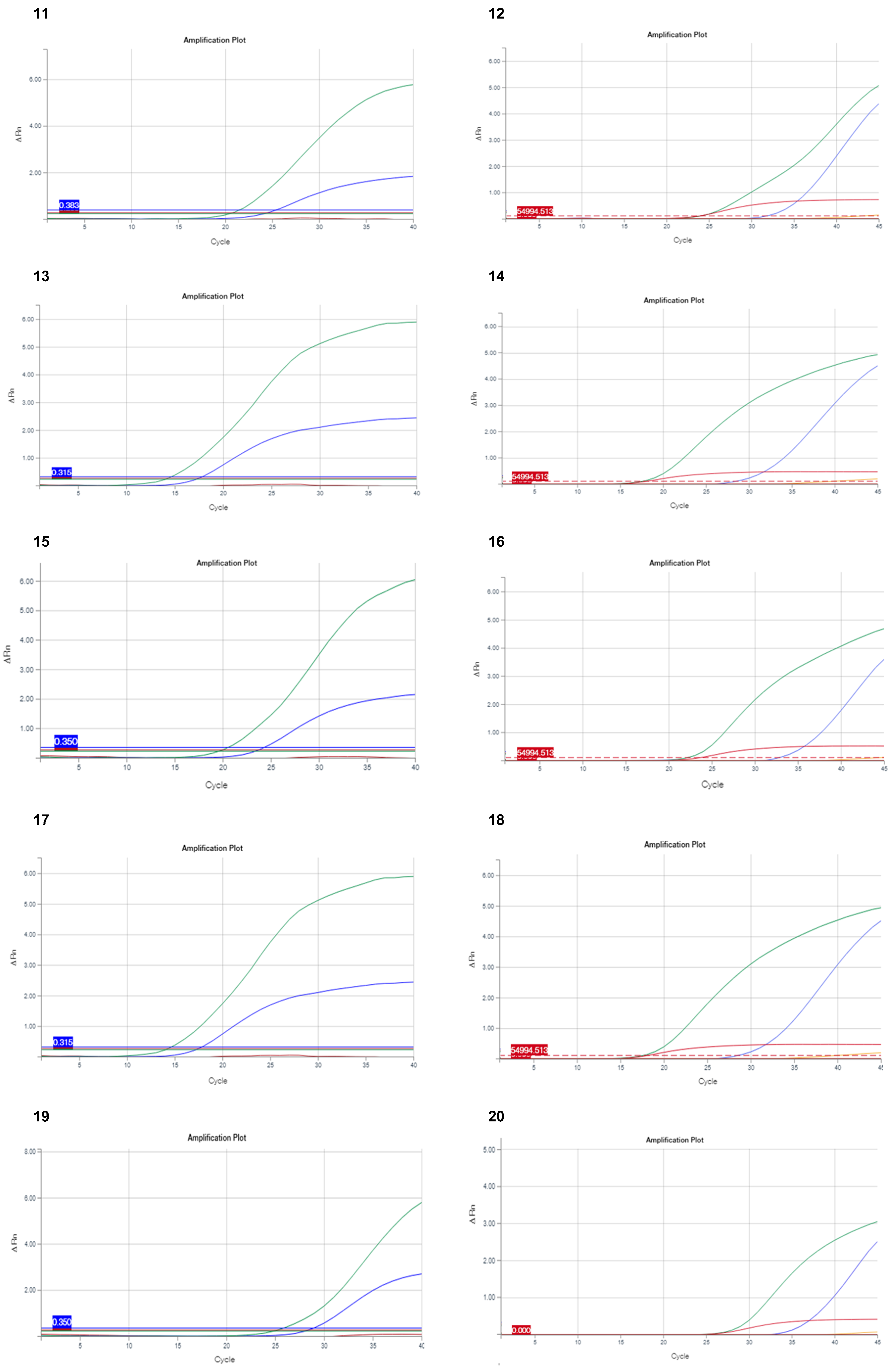
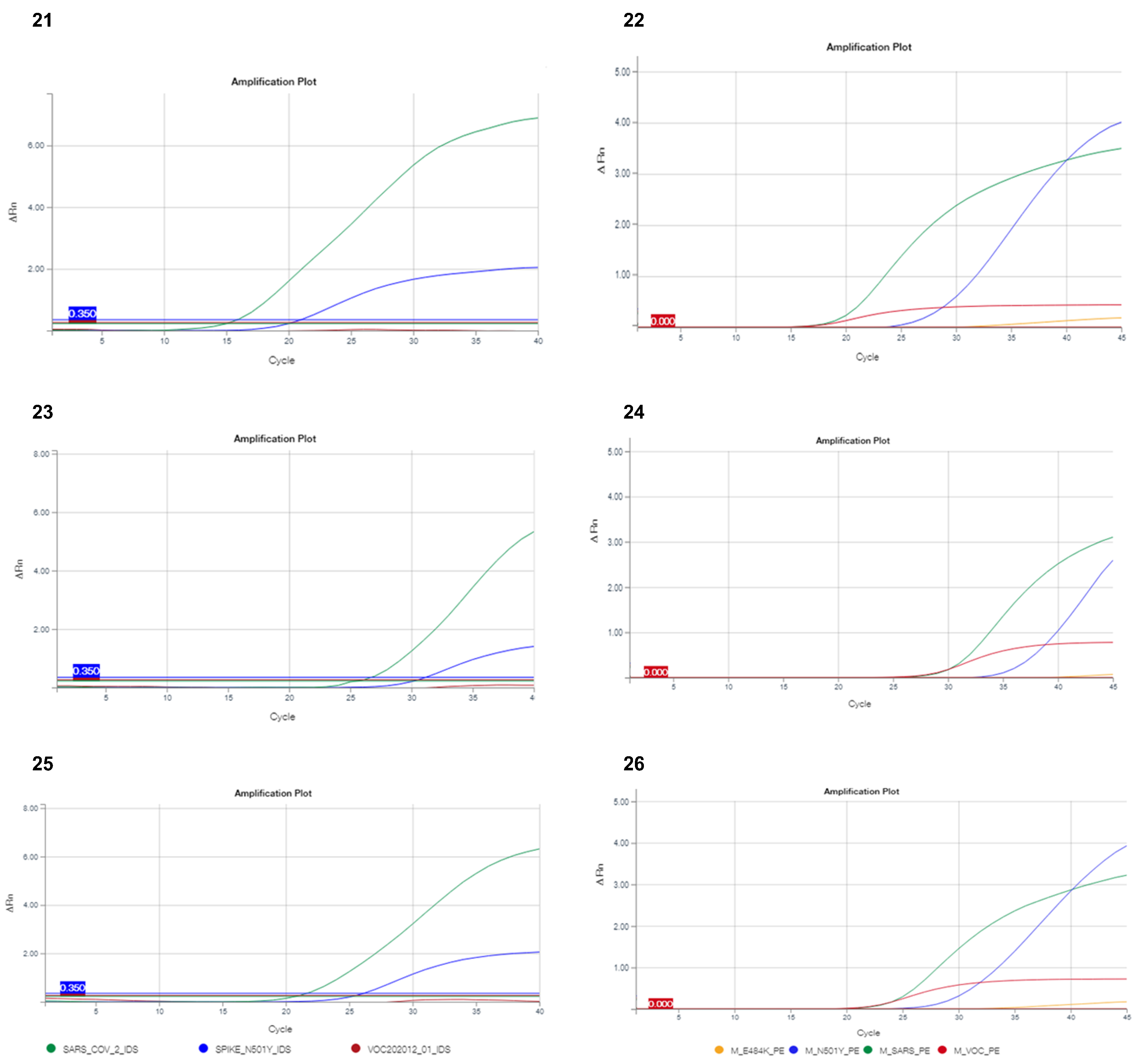
3.2. Problems in the Detection of Variants Using Multiplex RT-PCR
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking changes in SARS-CoV-2 spike: Evidence that D614G increases infectivity of the COVID-19 virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef] [PubMed]
- Preliminary Genomic Characterisation of an Emergent SARS-CoV-2 Lineage in the UK Defined by a Novel Set of Spike Mutations. Available online: https://virological.org/t/preliminary-genomic-characterisation-of-an-emergent-sars-cov-2-lineage-in-the-uk-defined-by-a-novel-set-of-spike-mutations/563 (accessed on 30 May 2021).
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; du Plessus, L.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2021, 6, 415. [Google Scholar] [CrossRef] [PubMed]
- Tegally, H.; Wilkinson, E.; Lessells, R.J.; Giandhari, J.; Pillay, S.; Msomi, N.; Mlisana, K.; Bhiman, J.N.; von Gottberg, A.; Walaza, S.; et al. Sixteen novel lineages of SARS-CoV-2 in South Africa. Nat. Med. 2021, 27, 440–446. [Google Scholar] [CrossRef]
- Faria, N.R.; Mellan, T.A.; Whittaker, C.; Claro, I.M.; Candido, D.D.S.; Mishra, S.; Crispim, M.A.E.; Sales, F.C.S.; Hawryluk, I.; McCrone, J.T.; et al. Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil. Science 2021, 372, 815–821. [Google Scholar] [CrossRef]
- Galloway, S.E.; Paul, P.; MacCannell, D.R.; Johansson, M.A.; Brooks, J.T.; MacNeil, A.; Slayto, R.B.; Tong, S.; Silk, B.J.; Armstrong, G.L.; et al. Emergence of SARS-CoV-2 B.1.1.7 lineage—United States, December 29, 2020–January 12, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 95–99. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 3 June 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 30 May 2021).
- Bal, A.; Destras, G.; Gaymard, A.; Stefic, K.; Marlet, J.; Eymieux, S.; Regue, H.; Semanas, Q.; d’Aubarede, C.; Billaud, G.; et al. Two-step strategy for the identification of SARS-CoV-2 variant of concern 202012/01 and other variants with spike deletion H69–V70, France, August to December 2020. Eurosurveillance 2021, 26, 2100008. [Google Scholar] [CrossRef]
- Weisblum, Y.; Schmidt, F.; Zhang, F.; DaSilva, J.; Poston, D.; Lorenzi, J.C.; Muecksch, F.; Rutkowska, M.; Hoffmann, H.H.; Michailidis, E.; et al. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. ELife 2020, 9, e61312. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Dejnirattisai, W.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Evidence of escape of SARS-CoV-2 variant B.1.351 from natural and vaccine-induced sera. Cell 2021, 184, 2348–2361.e6. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Werner, A.P.; Koch, M.; Choi, A.; Narayanan, E.; Stewart-Jones, G.B.E.; Colpitts, T.; Bennett, H.; Boyoglu-Barnum, S.; Shi, W.; et al. Serum neutralizing activity elicited by mRNA-1273 vaccine. N. Engl. J. Med. 2021, 384, 1468–1470. [Google Scholar] [CrossRef] [PubMed]
- Haim-Boukobza, S.; Roquebert, B.; Trombert-Paolantoni, S.; Lecorche, E.; Verdurme, L.; Foulongne, V.; Selinger, C.; Michalakis, Y.; Sofonea, M.T.; Alizon, S. Detecting rapid spread of SARS-CoV-2 variants, France, January 26–February 16, 2021. Emerg. Infect. Dis. 2021, 27, 1496–1499. [Google Scholar] [CrossRef]
- Yan, Y.; Chang, L.; Luo, W.; Liu, J.; Guo, F.; Wang, L. Comparison of seven commercial severe acute respiratory syndrome coronavirus 2 nucleic acid detection reagents with pseudovirus as quality control material. J. Mol. Diagn. 2021, 23, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Ion AmpliSeqTM Library Kit Plus USER GUIDE. Available online: http://tools.thermofisher.com/content/sfs/manuals/MAN0017003_IonAmpliSeqLibaryKitPlus_UG.pdf (accessed on 30 May 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Area, I.; Nieto, J.J. Forecasting the effects of the new SARS-CoV-2 variant in Europe. Sci. World J. 2021, 2021, 5553240. [Google Scholar] [CrossRef] [PubMed]
- Funk, T.; Pharris, A.; Spiteri, G.; Bundle, N.; Melidou, A.; Carr, M.; Gonzalez, G.; Garcia-Leon, A.; Crispie, F.; O’Connor, L.; et al. Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: Data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance 2021, 26, 2100348. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Giorgi, E.E.; Marichannegowda, M.H.; Foley, B.; Xiao, C.; Kong, X.P.; Chen, Y.; Gnanakaran, S.; Korber, B.; Gao, F. Emergence of SARS-CoV-2 through recombination and strong purifying selection. Sci. Adv. 2020, 6, eabb9153. [Google Scholar] [CrossRef]
- Kami, W.; Kinjo, T.; Arakaki, W.; Oki, H.; Motooka, D.; Nakamura, S.; Fujita, J. Rapid and simultaneous identification of three mutations by the Novaplex™ SARS-CoV-2 variants I assay kit. J. Clin. Virol. 2021, 141, 104877. [Google Scholar] [CrossRef] [PubMed]
- Vega-Magaña, N.; Sánchez-Sánchez, R.; Hernández-Bello, J.; Venancio-Landeros, A.A.; Peña-Rodríguez, M.; Vega-Zepeda, R.A.; Galindo-Ornelas, B.; Díaz-Sánchez, M.; García-Chagollán, M.; Macedo-Ojeda, G.; et al. RT-qPCR assays for rapid detection of the N501Y, 69-70del, K417N, and E484K SARS-CoV-2 mutations: A screening strategy to identify variants with clinical impact. Front. Cell. Infect. Microbiol. 2021, 11, 672562. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Miller, J.A.; Verghese, M.; Sibai, M.; Solis, D.; Mfuh, K.O.; Jiang, B.; Iwai, N.; Mar, M.; Huang, C.; et al. Multiplex SARS-CoV-2 genotyping RT-PCR for population-level variant screening and epidemiologic surveillance. J. Clin. Microbiol. 2021, JCM0085921. [Google Scholar] [CrossRef]
- Amato, L.; Jurisic, L.; Puglia, I.; Di Lollo, V.; Curini, V.; Torzi, G.; Girolamo, A.D.; Mangone, I.; Mancinelli, A.; Decaro, N.; et al. Multiple detection and spread of novel strains of the SARS-CoV-2 B.1.177 (B.1.177.75) lineage that test negative by a commercially available nucleocapsid gene real-time RT-PCR. Emerg. Microbes. Infect. 2021, 10, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jean, S.; Eltringham, R.; Madison, J.; Snyder, P.; Tu, H.; Jones, D.M.; Leber, A.L. Mutation-specific SARS-CoV-2 PCR screen: Rapid and accurate detection of variants of concern and the identification of a newly emerging variant with spike L452R mutation. J. Clin. Microbiol. 2021, JCM-00926. [Google Scholar] [CrossRef]
- SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html (accessed on 30 May 2021).
- DGS-URGENT N 2021_12: Stratégie de Freinage de la Propagation des Variants du SARS-CoV-2: Renforcement Spécifique sur les Variants d’Interet 20H/501Y.V2 et 20J/501Y.V3. Available online: https://solidarites-sante.gouv.fr/ministere/declarations-publiques-d-interets/direction-generale-de-la-sante-dgs (accessed on 30 May 2021).
- Verghese, M.; Jiang, B.; Iwai, N.; Mar, M.; Sahoo, M.K.; Yamamoto, F.; Mfuh, K.O.; Miller, J.; Wang, H.; Zehnder, J.; et al. A SARS-CoV-2 Variant with L452R and E484Q Neutralization Resistance Mutations. J. Clin. Microbiol. 2021, 59, e0074121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mutation | Virus Name Gisaid | Number GISAID | Coverage | Coverage (%) |
|---|---|---|---|---|
| S71F | hCoV-19/France/OCC-NI-2104021309/2021 | EPI_ISL_1972901 | 5835 | 5179/5179 (100%) |
| hCoV-19/France/OCC-NI-2104041142/2021 | EPI_ISL_1972902 | 5867 | 1558/1559 (99.9%) | |
| hCoV-19/France/OCC-NI-2103280925/2021 | EPI_ISL_1972903 | 3039 | 1879/1882 (99.9%) | |
| hCoV-19/France/OCC-NI-2104011273/2021 | EPI_ISL_1915508 | 4574 | 3247/3250 (99.9%) | |
| hCoV-19/France/OCC-NI-2103271225/2021 | EPI_ISL_1915509 | 6630 | 6049/6060 (99.8%) | |
| hCoV-19/France/OCC-NI-2103301082/2021 | EPI_ISL_1972904 | 5392 | 2602/2604 (99.9%) | |
| hCoV-19/France/OCC-NI-2103281047/2021 | EPI_ISL_1972905 | 2468 | 1737/1740 (99.9%) | |
| hCoV-19/France/OCC-NI-2104091053/2021 | EPI_ISL_1915510 | 7209 | 6393/6398 (99.9%) | |
| hCoV-19/France/OCC-NI-2103222347/2021 | EPI_ISL_1524908 | 3770 | 3268/3269 (99.9%) | |
| hCoV-19/France/OCC-NI-2104270876/2021 | EPI_ISL_2131449 | 5376 | 5866/5873 (99.9%) | |
| hCoV-19/France/OCC-NI-2104290828/2021 | EPI_ISL_2131450 | 7257 | 6255/6258 (99.9%) | |
| A67S | hCoV-19/France/OCC-NI-2104262513/2021 | EPI_ISL_2131448 | 4244 | 5229/5242 (99.7%) |
| hCoV-19/France/OCC-NI-2104241354/2021 | EPI_ISL_2131447 | 3690 | 3123/3126 (99.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boudet, A.; Stephan, R.; Bravo, S.; Sasso, M.; Lavigne, J.-P. Limitation of Screening of Different Variants of SARS-CoV-2 by RT-PCR. Diagnostics 2021, 11, 1241. https://doi.org/10.3390/diagnostics11071241
Boudet A, Stephan R, Bravo S, Sasso M, Lavigne J-P. Limitation of Screening of Different Variants of SARS-CoV-2 by RT-PCR. Diagnostics. 2021; 11(7):1241. https://doi.org/10.3390/diagnostics11071241
Chicago/Turabian StyleBoudet, Agathe, Robin Stephan, Sophie Bravo, Milène Sasso, and Jean-Philippe Lavigne. 2021. "Limitation of Screening of Different Variants of SARS-CoV-2 by RT-PCR" Diagnostics 11, no. 7: 1241. https://doi.org/10.3390/diagnostics11071241
APA StyleBoudet, A., Stephan, R., Bravo, S., Sasso, M., & Lavigne, J. -P. (2021). Limitation of Screening of Different Variants of SARS-CoV-2 by RT-PCR. Diagnostics, 11(7), 1241. https://doi.org/10.3390/diagnostics11071241