
The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania

 ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
- -
- Type 1, which includes endometrioid and mucinous carcinoma (usually corelated with long term enhanced levels of estrogen, thus conducting to persistent proliferative stimulation of the endometrium); PTEN, KRAS, and PAX2 gene alterations are common as well as atypical endometrial hyperplasia/endometrioid intraepithelial neoplasia, which is regarded as the precursor lesion).
- -
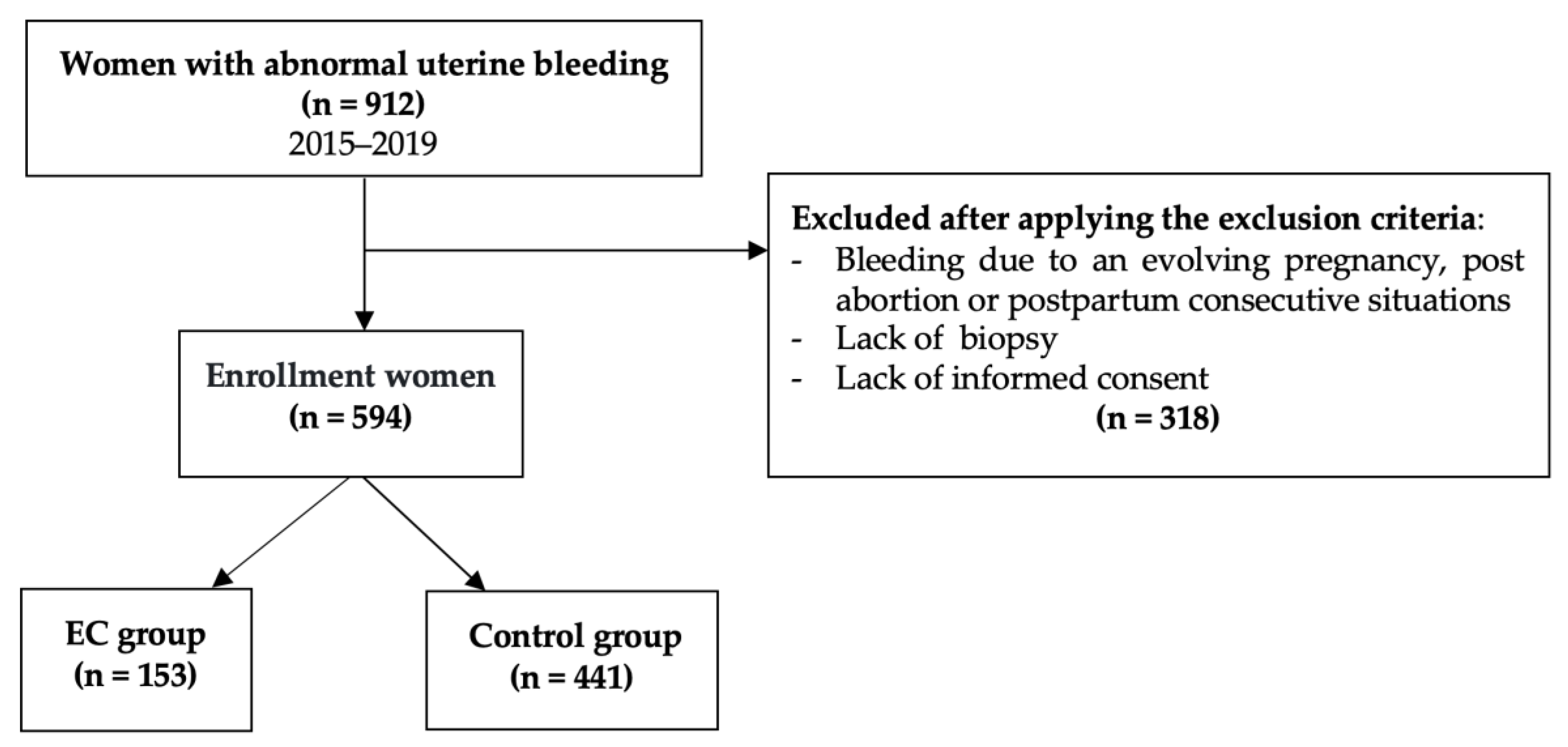
2. Materials and Methods
2.1. Study Design
- Clinical and histopathological findings;
- The presence of common histopathological associations and its relevance, if it exists;
- Common features for each of the identified cohorts: EC, EH, other lesions;
- The correlations between IETA ultrasonographical scores and the histopathological findings.
2.2. Endometrial Cancers Characterization
2.3. IETA Characteristics in Endometrial Pathology
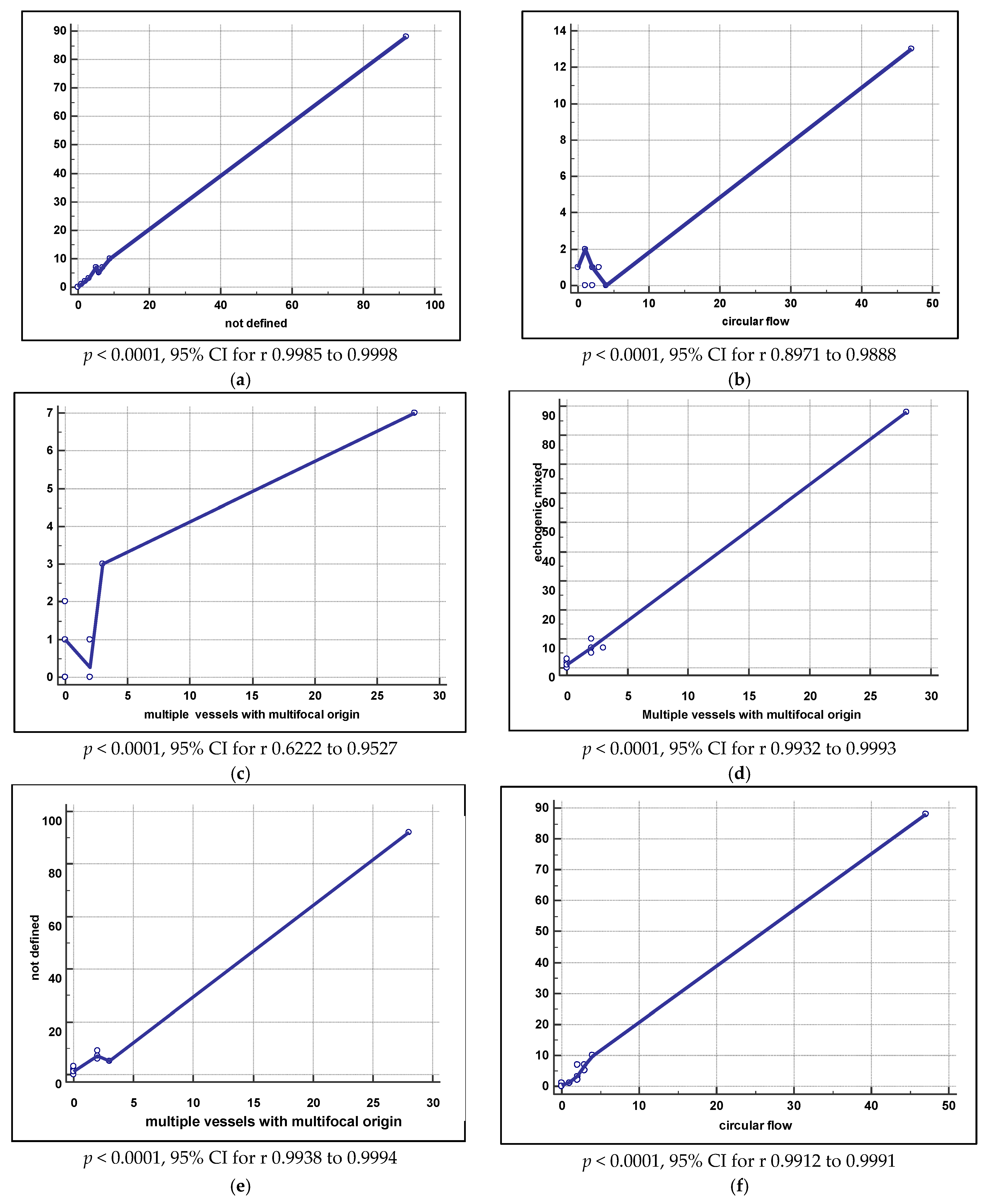
2.4. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Histopathological Results
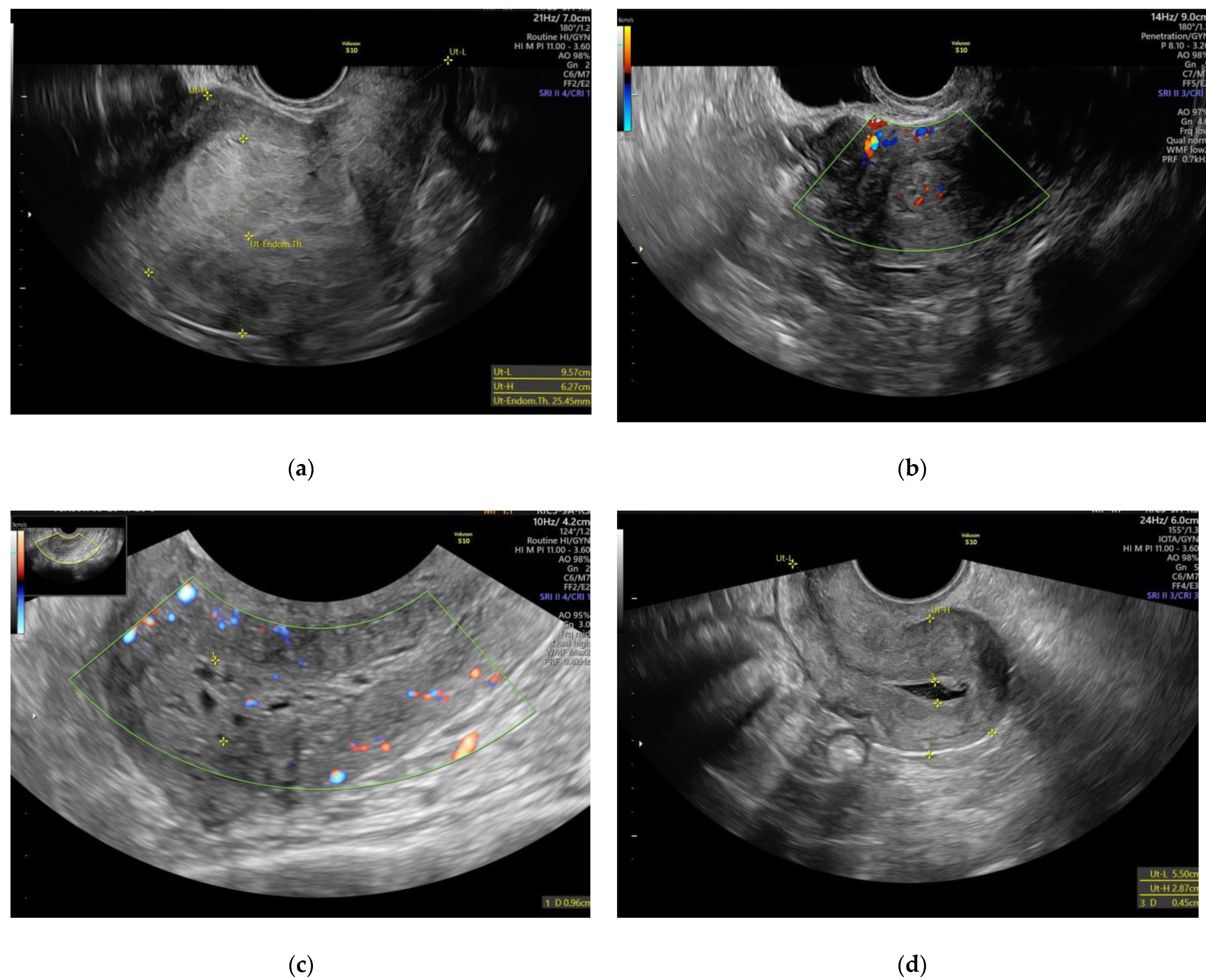
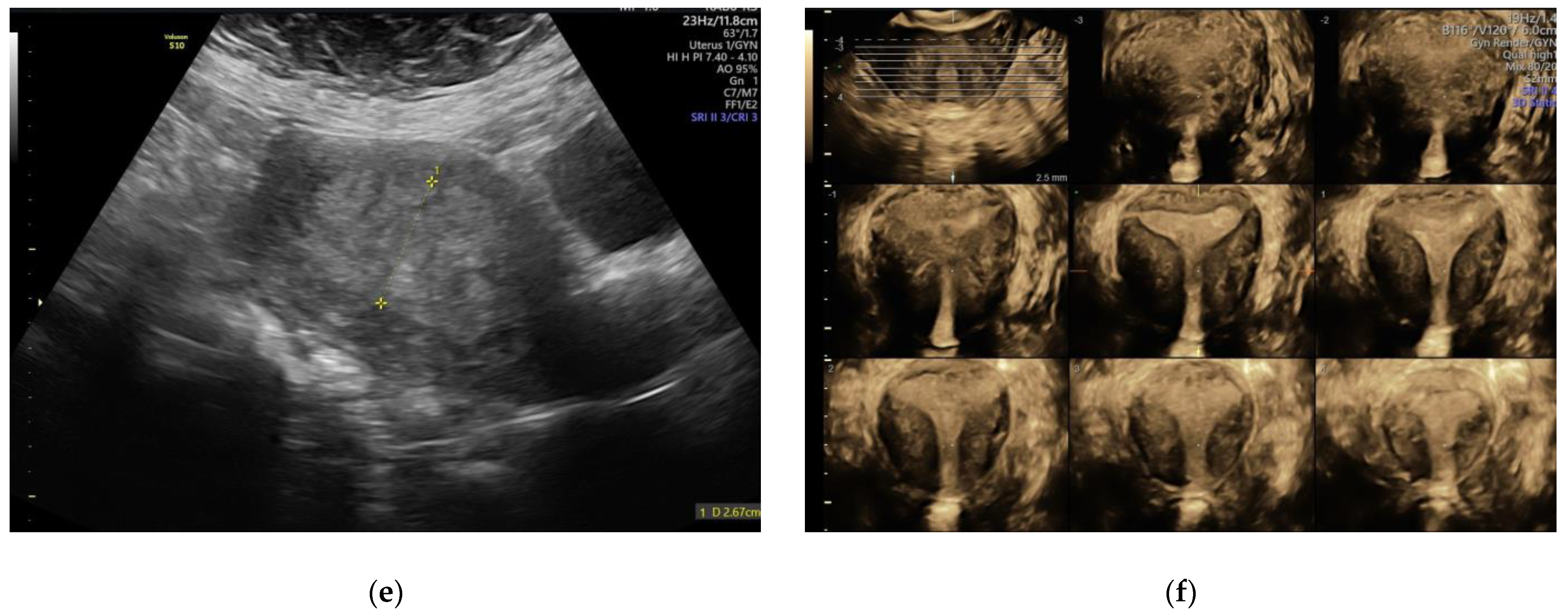
3.2. IETA Ultrasound Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.-B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II Endometrial Cancers: Have They Different Risk Factors? J. Clin. Oncol. 2013, 31, 2607–2618. [Google Scholar] [CrossRef]
- Clement, P.B.; Young, R.H. Endometrioid Carcinoma of the Uterine Corpus: A Review of Its Pathology With Emphasis on Recent Advances and Problematic Aspects. Adv. Anat. Pathol. 2002, 9, 145–184. [Google Scholar] [CrossRef]
- Banno, K.; Kisu, I.; Yanokura, M.; Tsuji, K.; Masuda, K.; Ueki, A.; Kobayashi, Y.; Yamagami, W.; Nomura, H.; Tominaga, E.; et al. Biomarkers in endometrial cancer: Possible clinical applications (Review). Oncol. Lett. 2012, 3, 1175–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, F.P.G.; Timmerman, D.; Bourne, T.; Valentin, L.; Epstein, E.; Goldstein, S.R.; Marret, H.; Parsons, A.K.; Gull, B.; Istre, O.; et al. Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: A consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound Obstet. Gynecol. 2010, 35, 103–112. [Google Scholar] [CrossRef]
- Epstein, E.; Fischerova, D.; Valentina, C.; Testa, A.C.; Franchi, D.; Sladkevicius, P.; Frühauf, F.; Lindqvist, P.G.; Mascilini, F.; Fruscio, R.; et al. Ultrasound characteristics of endometrial cancer as defined by International Endometrial Tumor Analysis (IETA) consensus nomenclature: Prospective multicenter study. Ultrasound Obstet. Gynecol. 2018, 51, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Hebbar, S.; Chaya, V.; Rai, L.; Ramachandran, A. Factors Influencing Endometrial Thickness in Postmenopausal Women. Ann. Med Health Sci. Res. 2014, 4, 608–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tit, D.M.; Bungau, S.; Iovan, C.; Cseppento, D.C.N.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the Hormone Replacement Therapy and of Soy Isoflavones on Bone Resorption in Postmenopause. J. Clin. Med. 2018, 7, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid-Nicholson, M.; Iyengar, P.; Hummer, A.J.; Linkov, I.; Asher, M.; Soslow, R. Immunophenotypic diversity of endometrial adenocarcinomas: Implications for differential diagnosis. Mod. Pathol. 2006, 19, 1091–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djordjevic, B.; Westin, S.N.; Broaddus, R.R. Application of Immunohistochemistry and Molecular Diagnostics to Clinically Relevant Problems in Endometrial Cancer. Surg. Pathol. Clin. 2012, 5, 859–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.F.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours: Female Genital Tumours, 5th ed.; International Agency for Research on Cancer Publications: Lyon, France, 2020; Volume 4. [Google Scholar]
- Zhang, S.; Gong, T.-T.; Liu, F.-H.; Jiang, Y.-T.; Sun, H.; Ma, X.-X.; Zhao, Y.-H.; Wu, Q.-J. Global, Regional, and National Burden of Endometrial Cancer, 1990–2017: Results from the Global Burden of Disease Study, 2017. Front. Oncol. 2019, 9, 9. [Google Scholar] [CrossRef]
- Bell, D.W.; O’Hara, A.J. The genomics and genetics of endometrial cancer. Adv. Genom. Genet. 2012, 2, 33–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahboubi, E.; Eyler, N.; Wynder, E.L. Epidemiology of Cancer of the Endometrium. Clin. Obstet. Gynecol. 1982, 25, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherman, M.E. Theories of Endometrial Carcinogenesis: A Multidisciplinary Approach. Mod. Pathol. 2000, 13, 295–308. [Google Scholar] [CrossRef] [Green Version]
- Hecht, J.L.; Mutter, G.L. Molecular and Pathologic Aspects of Endometrial Carcinogenesis. J. Clin. Oncol. 2006, 24, 4783–4791. [Google Scholar] [CrossRef]
- Lax, S.F. Pathology of Endometrial Carcinoma. Adv. Exp. Med. Biol. 2017, 943, 75–96. [Google Scholar] [CrossRef]
- Talhouk, A.; McAlpine, J.N. New classification of endometrial cancers: The development and potential applications of genomic-based classification in research and clinical care. Gynecol. Oncol. Res. Pr. 2016, 3, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Sanderson, P.A.; Critchley, H.O.; Williams, A.R.; Arends, M.J.; Saunders, P.T. New concepts for an old problem: The diagnosis of endometrial hyperplasia. Hum. Reprod. Updat. 2016, 23, 232–254. [Google Scholar] [CrossRef] [PubMed]
- Vandermeulen, L.; Cornelis, A.; Rasmussen, C.; Timmerman, D.; Bosch, T.V.D. Guiding histological assessment of uterine lesions using 3D in vitro ultrasonography and stereotaxis. Facts Views Vis. ObGyn 2017, 9, 77–84. [Google Scholar]
- Whitaker, L.; Critchley, H.O. Abnormal uterine bleeding. Best Pr. Res. Clin. Obstet. Gynaecol. 2016, 34, 54–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Chen, X.; Xia, H.; Wang, L.; Zhao, H.; Xu, B.; Zhang, A.; Zhang, W. Promotion of the occurrence of endometrioid carcinoma by S100 calcium binding protein P. BMC Cancer 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Yasuda, M.; Katoh, T.; Hori, S.; Suzuki, K.; Ohno, K.; Maruyama, M.; Matsui, N.; Miyazaki, S.; Ogane, N.; Kameda, Y. Endometrial intraepithelial carcinoma in association with polyp: Review of eight cases. Diagn. Pathol. 2013, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, K.; Leitao, M.M., Jr.; Wynveen, C.A.; Sica, G.L.; Shia, J.; Shi, W.; Soslow, R. p53 overexpression in morphologically ambiguous endometrial carcinomas correlates with adverse clinical outcomes. Mod. Pathol. 2009, 23, 80–92. [Google Scholar] [CrossRef]
- Günakan, E.; Atak, Z.; Albayrak, M.; Kurban, Y.; Şimşek, G.G. Endometrial histopathology results and evaluation of endometrial cancer risk in geriatric women. Menopausal Rev. 2018, 17, 18–21. [Google Scholar] [CrossRef]
- Bray, F.; Silva, I.D.S.; Moller, H.; Weiderpass, E. Endometrial Cancer Incidence Trends in Europe: Underlying Determinants and Prospects for Prevention. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1132–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, S.D.; Newton, K.M.; Clinton, W.L.; Epplein, M.; Garcia, R.; Allison, K.; Voigt, L.F.; Weiss, N.S. Incidence of endometrial hyperplasia. Am. J. Obstet. Gynecol. 2009, 200, 678.e1–678.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faria, S.; Sagebiel, T.; Devine, C.; Lal, C.; Balachandran, A.; Bhosale, P. Imaging in endometrial carcinoma. Indian J. Radiol. Imaging 2015, 25, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, L.; Qi, W.; Shen, D.; Li, X.; Wang, J.; Wei, L. Clinical implications and prognostic value of five biomarkers in endometrial carcinoma. Chin. Ger. J. Clin. Oncol. 2013, 12, 586–591. [Google Scholar] [CrossRef]
- Furau, A.; Craina, M.L.; Furau, C.; Luca, T.C.; Andor, B.C.; Radu, D.; Moleriu, L.C.; Bonte, D.C.; Toader, D.O.; Furau, G. The Association of Body Mass Index and Ki67 Values in Patients with Endometrial Carcinoma. Rev. Chim. 2019, 70, 3277–3280. [Google Scholar] [CrossRef]
- Jacobs, I.; Gentry-Maharaj, A.; Burnell, M.; Manchanda, R.; Singh, N.; Sharma, A.; Ryan, A.; Seif, M.W.; Amso, N.; Turner, G.; et al. Sensitivity of transvaginal ultrasound screening for endometrial cancer in postmenopausal women: A case-control study within the UKCTOCS cohort. Lancet Oncol. 2011, 12, 38–48. [Google Scholar] [CrossRef]
- Gruboeck, K.; Jurkovic, D.; Lawton, F.; Savvas, M.; Tailor, A.; Campbell, S. The diagnostic value of endometrial thickness and volume measurements by three-dimensional ultrasound in patients with postmenopausal bleeding. Ultrasound Obstet. Gynecol. 1996, 8, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Sladkevicius, P.; Installé, A.; Bosch, T.V.D.; Timmerman, D.; Benacerraf, B.; Jokubkiene, L.; Di Legge, A.; Votino, A.; Zannoni, L.; De Moor, B.; et al. International Endometrial Tumor Analysis (IETA) terminology in women with postmenopausal bleeding and sonographic endometrial thickness ≥4.5 mm: Agreement and reliability study. Ultrasound Obstet. Gynecol. 2018, 51, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Tataru, A.-L.; Furau, G.; Afilon, J.; Ionescu, C.; Dimitriu, M.; Bratu, O.G.; Tit, D.M.; Bungau, S.; Furau, C. The Situation of Cervical Cancers in the Context of Female Genital Cancer Clustering and Burden of Disease in Arad County, Romania. J. Clin. Med. 2019, 8, 96. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age (years) | 56 (13–91) |
| Age at menopause (years) | 49 (32–68) |
| Body mass index (kg/m2) | 27.23 (17–38) |
| Parity | 2 (0–9) |
| 0 | 72 (12.1) |
| 1 | 104 (17.5) |
| ≥2 | 418 (70.4) |
| Use of hormone replacement therapy or local estrogens | 11 (1.85) |
| Postmenopausal | 446 (75.1) |
| Perimenopausal | 78 (13.1) |
| Reproductive age | 70 (11.78) |
| Diagnosis | Cases | % | Average Age | SD |
|---|---|---|---|---|
| EC Type | ||||
| Mucinous adenocarcinoma | 1 | 0.65 | 58.00 | - |
| Pavement-cell carcinoma | 1 | 0.65 | 85.00 | - |
| Serous endometrioid adenocarcinoma | 6 | 3.92 | 68.33 | 6.861 |
| Carcinosarcoma of the uterus | 2 | 1.31 | 78.50 | 3.536 |
| Squamous cell carcinoma | 4 | 2.61 | 68.75 | 8.302 |
| Endometrioid carcinoma with moderate differentiation | 1 | 0.65 | 68.00 | - |
| Undifferentiated endometrial carcinoma | 2 | 1.31 | 59.50 | 2.121 |
| Mixed cell endometrial carcinoma | 3 | 1.96 | 60.00 | 5.568 |
| Endometrial intraepithelial carcinoma (EIC) | 2 | 1.31 | 56.50 | 6.364 |
| Adenocarcinoma with squamous differentiation | 8 | 5.23 | 62.50 | 9.636 |
| Clear-cell endometrial endometrioid adenocarcinoma | 7 | 4.58 | 64.00 | 3.830 |
| Endometrioid adenocarcinoma | 101 | 66.01 | 63.66 | 8.998 |
| Villoglandular (papillary) endometrioid adenocarcinoma | 10 | 6.54 | 64.90 | 10.290 |
| Endometrioid carcinoma with secretory change | 2 | 1.31 | 66.00 | 4.243 |
| Endometrial serous carcinoma | 3 | 1.96 | 64.67 | 3.786 |
| Total | 153 | 100 | 64.17 | 8.794 |
| Other Lesions | ||||
| Typical EH | 133 | 22.39 | 49.70 | 10.279 |
| Atypical EH | 14 | 2.35 | 58.07 | 12.413 |
| Adenomyosis/endometriosis | 16 | 2.69 | 46.60 | 7.635 |
| Leiomyoma | 133 | 22.39 | 54.69 | 10.543 |
| Cervical dysplasia | 4 | 0.67 | 56.17 | 11.900 |
| Endometritis | 22 | 3.70 | 56.91 | 13.698 |
| Ovarian cyst | 10 | 16.83 | 51.05 | 13.683 |
| Cervicitis | 13 | 2.18 | 58.33 | 13.172 |
| Endometrial polyps | 96 | 16.16 | 53.95 | 11.137 |
| Group p < 0.0001 | Endometrial Echogenity | Total (no/%) | |||
|---|---|---|---|---|---|
| Inh | Inh NNRCA | NRCA | Hom | ||
| Other | 1/1 | 39/45 | 37/56 | 101/64 | 178° (42.4) |
| EC | 110/99 | 21/24 | 16/24 | 6/4 | 153° (36.4) |
| Atypical EH | 0 | 2/2 | 3/5 | 6/4 | 11° (2.6) |
| Typical EH | 0 | 24/28 | 10/15 | 44/28 | 78° (18.6) |
| Total (no/%) | 111/26.40 | 86/20.50 | 66/15.70 | 157/37.40 | 420 |
| Group p < 0.0001 | Endometrial-Myometrial Junction | Total (no/%) | ||
|---|---|---|---|---|
| Undefined | Irregular | Regular | ||
| Other | 61/27 | 18/32 | 99/71 | 178° (42.4) |
| EC | 130/58 | 21/37 | 2/1 | 153° (36.4) |
| Atypical EH | 3/1,33 | 4/7 | 4/3 | 11° (2.6) |
| Typical EH | 30/13,39 | 14/25 | 34/25 | 78° (18.6) |
| Total (no/%) | 224/53.30 | 57/13.60 | 139/33.19 | 420/100 |
| Group p < 0.0001 | Vessel Aspect | Total (no/%) | |||
|---|---|---|---|---|---|
| Dominant Vessels | Without Branching | Focal Origin | Multifocal Origin | ||
| Other | 1/1.5 | 163/64 | 13/22 | 1/2.6 | 178/42.4 |
| EC | 67/98.6 | 14/5.5 | 35/58 | 37/97 | 153/36.4 |
| Atypical EH | 0 | 11/4.3 | 0 | 0 | 11/2.6 |
| Typical EH | 0 | 66/26 | 12/20 | 0 | 78/18.6 |
| Total (no/%) | 68/16.20 | 254/60.50 | 60/14.30 | 38/9.00 | 420/100 |
| Group p < 0.0001 | Intracavitary Fluid | Total | ||
|---|---|---|---|---|
| Mixt Echogenity | Absent | Ground Glass | ||
| Other | 73/30 41.0% RT 30.4% CT 17.4% GT | 85/73 47.8% RT 72.6% CT 20.2% GT | 20/32 11.2% RT 31.7% CT 4.8% GT | 178/42.4 |
| EC | 128/53 83.7% RT 53.3% CT 30.5% GT | 1/1 0.7% RT 0.9% CT 0.2% GT | 24/38 15.7% RT 38.1% CT 5.7% GT | 153/36.4 |
| Atypical EH | 4/2 36.4% RT 1.7% CT 1.0% GT | 4/3 36.4% RT 3.4% CT 1.0% GT | 3/5 27.3% RT 4.8% CT 0.7% GT | 11/2.6 |
| Typical EH | 35/15 44.9% RT 14.6% CT 8.3% GT | 2723 34.6% RT 23.1% CT 6.4% GT | 16/25 20.5% RT 25.4% CT 3.8% GT | 78/18.6 |
| Total (no/%) | 240/57.1 | 117/27.9 | 63/15.0 | 420/100 |
| Group p < 0.0001 | IETA Doppler Score for the Uterine Artery | Total (no/%) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Other | 120/66 | 25/49 | 32/42 | 1/1 | 178/42.4 |
| EC | 5/3 | 11/22 | 27/35 | 110/99 | 153/36.4 |
| Atypical EH | 6/3 | 3/6 | 2/2 | 0 | 11/2.6 |
| Typical EH | 50/28 | 12/23 | 16/21 | 0 | 78/18.6 |
| Total (no/%) | 181/43.10 | 51/12.10 | 77/18.30 | 111/26.40 | 420/100 |
| Characteristics | Values (no/Total (%) |
|---|---|
| Stage of cancer for 153 cases | |
| IA | 139 (90.8) |
| IC | 7 (4.6) |
| II | 7(4.6) |
| Histological type | |
| Endometrioid | 136/153 (88.9) |
| Grade 1 | 32/136 (23.5) |
| Grade 2 | 83/136 (61.0) |
| Grade 3 | 21/136 (15.5) |
| Non-endometrioid/Grade | 17/153 (11.1) |
| Grade 1 | 2/17 (11.8) |
| Grade 2 | 11/17 (64.7) |
| Grade 3 | 4/17 (23.5) |
| Non-endometrioid/Types | |
| Serous | 5/17 (29.4) |
| Carcinosarcoma | 2/17 (11.8) |
| Clear-cell carcinoma | 4/17 (23.5) |
| Mixed-cell carcinoma | 4/17 (23.5) |
| Undifferentiated | 2/17 (11.8) |
| Ultrasound Feature | AUC (95%CI) | P (Area = 0.5) | SE | SP | PPV° (%) (95%CI) | NPV° (%) (95%CI) | Accuracy |
|---|---|---|---|---|---|---|---|
| Endometrioid Tumors (n = 136) | |||||||
| Endometrial midline appearance | |||||||
| Linear midline | 0.73 (0.68–0.77) | <0.0001 | 98.53 | 48.24 | 47.25 (41.28–53.27) | 98.58 (94.95–99.83) | 64.52 |
| Non-linear midline | 0.53 (0.48–0.57) | 0.074 | 90.44 | 15.49 | 33.49 (28.65–38.60) | 77.49 (64.50–87.48) | 39.75 |
| Not defined midline | 0.76 (0.72–0.80) | <0.0001 | 88.97 | 63.73 | 53.58 (46.80–60.26) | 92.46 (87.85–95.74) | 71.90 |
| Endometrial morphology | |||||||
| Heterogeneous with irregular cystic areas | 0.55 (0.50–0.60) | 0.0056 | 86.76 | 23.94 | 14.56 (8.44–22.77) | 92.36 (76.84–98.81) | 44.28 |
| Heterogeneous with regular cystic areas | 0.57 (0.52–0.62) | <0.0001 | 94.12 | 20.42 | 35.75 (30.75–40.99) | 88.06 (77.75–94.73) | 44.28 |
| Heterogenous | 0.88 (0.84–0.91) | <0.0001 | 77.94 | 98.24 | 95.42 (89.65–98.49) | 90.44 (86.61–93.47) | 91.66 |
| Homogeneous | 0.75 (0.71–0.79) | <0.0001 | 97.06 | 53.87 | 49.75 (43.54–55.96) | 97.49 (93.68–99.32) | 67.85 |
| Vascular pattern | |||||||
| Multiple vessels with focal origin | 0.56 (0.51–0.61) | 0.0008 | 23.53 | 90.14 | 97.33 (86.04–99.93) | 74.41 (69.73–78.71) | 68.57 |
| Multiple vessels with multifocal origin | 0.63 (0.58–0.68) | <0.0001 | 27.21 | 99.65 | 97.33 (86.04–99.93) | 74.41 (69.73–78.71) | 76.19 |
| Without branching | 0.91 (0.88–0.93) | <0.0001 | 95.59 | 87.32 | 78.01 (70.90–84.08) | 97.67 (94.99–99.15) | 89.99 |
| Circular flow | 0.71 (0.66–0.75) | <0.0001 | 44.85 | 97.54 | 89.56 (79.69–95.6) | 78.98 (74.35–83.11) | 80.47 |
| Intrauterine fluid (IUF) | |||||||
| No fluid | 0.70 (0.66–0.74) | <0.0001 | 100 | 41.2 | 44.45 (38.77–50.25) | 100 (96.91–100) | 60.23 |
| “Ground glass” | 0.51 (0.47–0.56) | 0.3033 | 87.5 | 16.2 | 32.94 (28.09–38.09) | 73.36 (60.73–83.71) | 39.28 |
| Mixt | 0.72 (0.67–0.76) | <0.0001 | 87.5 | 57.39 | 49.14 (42.64–55.66) | 90.70 (85.49–94.51) | 67.13 |
| IETA DOPPLER score | 0.94 (0.91–0.96) | <0.0001 | 76.47 | 97.54 | 52.24 (29.61–74.22) | 99.15 (97.68–99.80) | 90.71 |
| Non-endometrioid tumors (n = 17) | |||||||
| Endometrial midline appearance | |||||||
| Linear midline | 0.67 (0.625–0.71) | <0.0001 | 100 | 34.49 | 5.09 (2.83–8.36) | 100 (97.39–100) | 37.13 |
| Non-linear midline | 0.67 (0.62–0.71) | 0.0055 | 47.06 | 87.84 | 11.98 (4.84–23.44) | 97.92 (95.87–99.12) | 86.19 |
| Not defined midline | 0.50 (0.45–0.55) | 0.9744 | 47.06 | 53.35 | 3.42 (1.35–7.03) | 96.62 (93.34–98.57) | 53.09 |
| Endometrial morphology | |||||||
| Heterogeneous with irregular cystic areas | 0.51 (0.46–0.56) | 0.7621 | 82.35 | 20.6 | 3.52 (1.81–6.10) | 97.07 (90.95–99.50) | 23.09 |
| Heterogeneous with regular cystic areas | 0.66(0.61–0.70) | 0.0095 | 47.06 | 85.61 | 10.32 (4.15–20.37) | 97.86 (95.77–99.10) | 84.05 |
| Heterogenous | 0.51 (0.46–0.56) | 0.7803 | 76.47 | 26.55 | 3.53 (1.77–6.24) | 96.97 (91.84–99.29) | 28.56 |
| Homogeneous | 0.63 (0.58–0.68) | 0.0015 | 88.24 | 38.46 | 4.80 (2.55–8.13) | 98.93 (95.81–99.90) | 40.47 |
| Vascular pattern | |||||||
| Fluid ground glass | 0.63 (0.58–0.68) | 0.0281 | 41.18 | 86.1 | 9.44 (3.5–19.558) | 97.65 (95.49–98.95) | 84.28 |
| Multiple vessels with focal origin | 0.51 (0.46–0.56) | 0.7176 | 17.65 | 85.86 | 4.20 (0.71–12.81) | 96.73 (94.33–98.31) | 83.10 |
| Multiple vessels with multifocal origin | 0.54 (0.49– 0.59) | <0.0001 | 100 | 9.43 | 3.74 (2.074–6.167) | 100 (90.808–100) | 13.08 |
| Without branching | 0.57 (0.52–0.61) | 0.2714 | 52.94 | 61.04 | 4.56 (1.934–8.953) | 97.35 (94.55–98.95) | 60.71 |
| Circular flow | 0.6 (0.551– 0.647) | 0.0994 | 35.29 | 84.62 | 7.0505 (2.24–15.999) | 97.5344 (95.323–98.885) | 82.62 |
| Intrauterine fluid (IUF) | |||||||
| Fluid mixt | 0.52 (0.47–0.57) | 0.7307 | 47.06 | 57.32 | 3.73 (1.48–7.64) | 96.85 (93.78–98.67) | 56.90 |
| “Ground glass” | 0.63 (0.58–0.68) | 0.0281 | 41.18 | 86.10 | 9.44(3.5–19.55) | 97.65 (95.49–98.95) | 84.28 |
| No fluid | 0.61 (0.56–0.66) | 0.0003 | 94.12 | 28.78 | 4.44 (2.41–7.41) | 99.28 (95.58–99.99) | 31.41 |
| IETA DOPPLER score | 0.61 (0.56–0.66) | 0.0523 | 82.35 | 44.17 | 4.93(2.55–8.50) | 98.61 (95.64–99.76) | 45.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furau, A.M.; Toma, M.M.; Ionescu, C.; Furau, C.; Bungau, S.; Dimitriu, M.; Tit, D.M.; Furau, G.; Petre, I.; Craina, M. The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania. Diagnostics 2021, 11, 1342. https://doi.org/10.3390/diagnostics11081342
Furau AM, Toma MM, Ionescu C, Furau C, Bungau S, Dimitriu M, Tit DM, Furau G, Petre I, Craina M. The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania. Diagnostics. 2021; 11(8):1342. https://doi.org/10.3390/diagnostics11081342
Chicago/Turabian StyleFurau, Alexandru Marius, Mirela Marioara Toma, Cringu Ionescu, Cristian Furau, Simona Bungau, Mihai Dimitriu, Delia Mirela Tit, Gheorghe Furau, Izabella Petre, and Marius Craina. 2021. "The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania" Diagnostics 11, no. 8: 1342. https://doi.org/10.3390/diagnostics11081342
APA StyleFurau, A. M., Toma, M. M., Ionescu, C., Furau, C., Bungau, S., Dimitriu, M., Tit, D. M., Furau, G., Petre, I., & Craina, M. (2021). The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania. Diagnostics, 11(8), 1342. https://doi.org/10.3390/diagnostics11081342