
Alzheimer’s Disease and Frontotemporal Dementia: A Robust Classification Method of EEG Signals and a Comparison of Validation Methods

 ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database Description and Data Acquisition
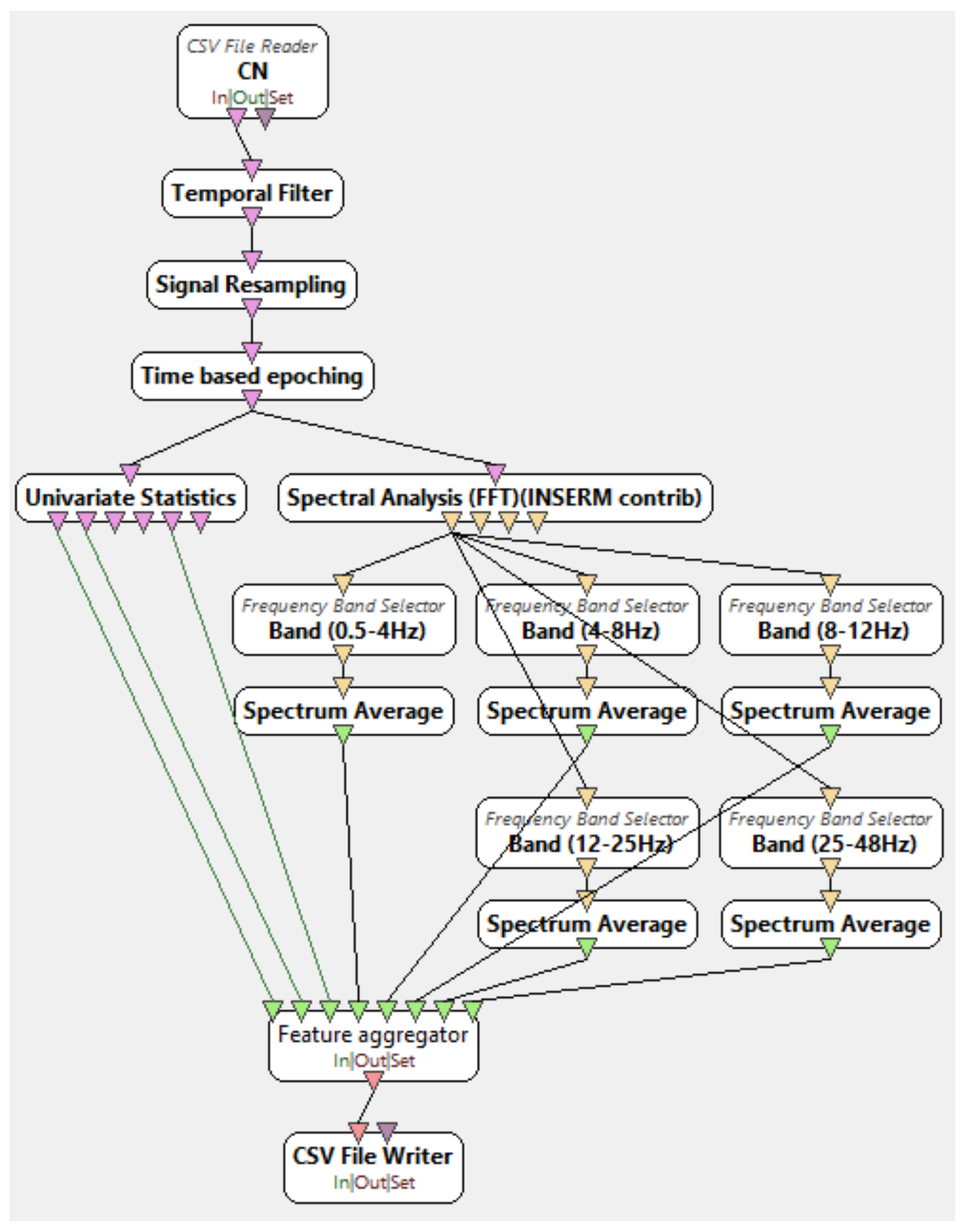
2.2. Signal Processing and Feature Extraction
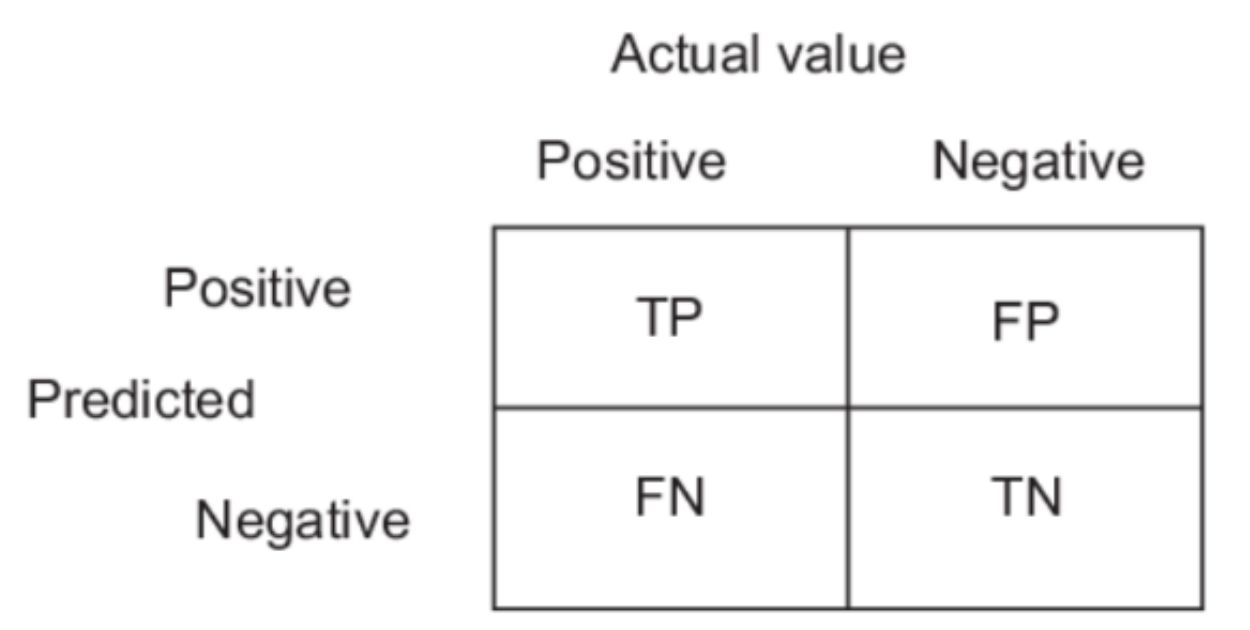
2.3. Classification
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Oliveira, A.M.; Radanovic, M.; De Mello, P.C.H.; Buchain, P.C.; Vizzotto, A.D.B.; Celestino, D.L.; Stella, F.; Piersol, C.; Forlenza, O.V. Nonpharmacological Interventions to Reduce Behavioral and Psychological Symptoms of Dementia: A Systematic Review. BioMed Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- Wimo, A.; Winblad, B.; Aguero-Torres, H.; von Strauss, E. The Magnitude of Dementia Occurrence in the World. Alzheimer Dis. Assoc. Disord. 2003, 17, 63–67. [Google Scholar] [CrossRef]
- Lattante, S.; Ciura, S.; Rouleau, G.A.; Kabashi, E. Defining the genetic connection linking amyotrophic lateral sclerosis (ALS) with frontotemporal dementia (FTD). Trends Genet. 2015, 31, 263–273. [Google Scholar] [CrossRef]
- Kirshner, H. Frontotemporal dementia and primary progressive aphasia, a review. Neuropsychiatr. Dis. Treat. 2014, 10, 1045–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodges, J.R.; Patterson, K.; Oxbury, S.; Funnell, E. Semantic dementia. Brain 1992, 115, 1783–1806. [Google Scholar] [CrossRef]
- Perry, R.J.; Hodges, J.R. Differentiating frontal and temporal variant frontotemporal dementia from Alzheimer’s disease. Neurology 2000, 54, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Yener, G.G.; Leuchter, A.F.; Jenden, D.; Read, S.L.; Cummings, J.L.; Miller, B.L. Quantitative EEG in Frontotemporal Dementia. Clin. Electroencephalogr. 1996, 27, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Salat, D.H.; Chen, J.J.; Van Der Kouwe, A.J.W.; Greve, D.N.; Fischl, B.; Rosas, H.D. Hippocampal degeneration is associated with temporal and limbic gray matter/white matter tissue contrast in Alzheimer’s disease. NeuroImage 2011, 54, 1795–1802. [Google Scholar] [CrossRef] [Green Version]
- Mendez, M.F.; Perryman, K.M.; Miller, B.L.; Cummings, J.L. Behavioral differences between frontotemporal dementia and Alzheimer’s disease: A comparison on the BEHAVE-AD rating scale. Int. Psychogeriatr. 1998, 10, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Mantzavinos, V. Biomarkers for Alzheimer’s Disease Diagnosis. Curr. Alzheimer Res. 2017, 14, 1149–1154. [Google Scholar] [CrossRef] [Green Version]
- Frisoni, G.B.; Fox, N.C.; Jack, C.R., Jr.; Scheltens, P.; Thompson, P.M. The clinical use of structural MRI in Alzheimer disease. Nat. Rev. Neurol. 2010, 6, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Bradley, K.M.; O’Sullivan, V.T.; Soper, N.D.W.; Nagy, Z.; King, E.M.; Smith, D.; Shepstone, B.J. Cerebral perfusion SPET correlated with Braak pathological stage in Alzheimer’s disease. Brain 2002, 125, 1772–1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, P.M.; Araki, S.S.; Sandberg, E.A.; Neumann, P.J.; Gazelle, G.S. Cost-Effectiveness of PET in the Diagnosis of Alzheimer Disease. Radiology 2003, 228, 515–522. [Google Scholar] [CrossRef]
- Reitz, C. Meta-analysis of the Association Between Variants in SORL1 and Alzheimer Disease. Arch. Neurol. 2011, 68, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homan, R.W. The 10-20 Electrode System and Cerebral Location. Am. J. EEG Technol. 1988, 28, 269–279. [Google Scholar] [CrossRef]
- Román, G.C.; Erkinjuntti, T.; Wallin, A.; Pantoni, L.; Chui, H.C. Subcortical ischaemic vascular dementia. Lancet Neurol. 2002, 1, 426–436. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; Van Boxtel, M.; Breteler, M.M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.; van der Flier, W.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Tzimourta, K.D.; Tzallas, A.T.; Giannakeas, N.; Astrakas, L.G.; Tsalikakis, D.G.; Angelidis, P.; Tsipouras, M.G. A robust methodology for classification of epileptic seizures in EEG signals. Health Technol. 2019, 9, 135–142. [Google Scholar] [CrossRef]
- Galasko, D.; Hansen, L.A.; Katzman, R.; Wiederholt, W.; Masliah, E.; Terry, R.; Hill, L.R.; Lessin, P.; Thal, L.J. Clinical-Neuropathological Correlations in Alzheimer’s Disease and Related Dementias. Arch. Neurol. 1994, 51, 888–895. [Google Scholar] [CrossRef]
- Albrecht, J.; Hanna, M.; Kim, D.; Perfetto, E.M. Predicting Diagnosis of Alzheimer’s Disease and Related Dementias Using Administrative Claims. J. Manag. Care Spéc. Pharm. 2018, 24, 1138–1145. [Google Scholar] [CrossRef]
- Moms, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; Van Belle, G.; Fillenbaum, G.; Mellits, E.D.; Clark, C. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part, I. Clinical and neuropsychological assesment of Alzheimer’s disease. Neurology 1989, 39, 1159. [Google Scholar] [CrossRef]
- Petrosian, A.; Prokhorov, D.; Lajara-Nanson, W.; Schiffer, R. Recurrent neural network-based approach for early recognition of Alzheimer’s disease in EEG. Clin. Neurophysiol. 2001, 112, 1378–1387. [Google Scholar] [CrossRef]
- Saletu, B.; Anderer, P.; Paulus, E.; Grünberger, J.; Wicke, L.; Neuhold, A.; Fischhof, P.K.; Litschauer, G. EEG Brain Mapping in Diagnostic and Therapeutic Assessment of Dementia. Alzheimer Dis. Assoc. Disord. 1991, 5, S57–S75. [Google Scholar] [CrossRef] [PubMed]
- Signorino, M.; Pucci, E.; Belardinelli, N.; Nolfe, G.; Angeleri, F. EEG spectral analysis in vascular and Alzheimer dementia. Electroencephalogr. Clin. Neurophysiol. 1995, 94, 313–325. [Google Scholar] [CrossRef]
- Pucci, E.; Cacchiò, G.; Angeloni, R.; Belardinelli, N.; Nolfe, G.; Signorino, M.; Angeleri, F. EEG spectral analysis in Alzheimer’s disease and different degenerative dementias. Arch. Gerontol. Geriatr. 1998, 26, 283–297. [Google Scholar] [CrossRef]
- Gordon, E.B.; Sim, M. The E.E.G. in presenile dementia. J. Neurol. Neurosurg. Psychiatry 1967, 30, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Oltu, B.; Akşahin, M.F.; Kibaroğlu, S. A novel electroencephalography based approach for Alzheimer’s disease and mild cognitive impairment detection. Biomed. Signal Process. Control. 2021, 63, 102223. [Google Scholar] [CrossRef]
- Hsu, C.F.; Chao, H.-H.; Yang, A.C.; Yeh, C.-W.; Hsu, L.; Chi, S. Discrimination of Severity of Alzheimer’s Disease with Multiscale Entropy Analysis of EEG Dynamics. Appl. Sci. 2020, 10, 1244. [Google Scholar] [CrossRef] [Green Version]
- Tzimourta, K.D.; Afrantou, T.; Ioannidis, P.; Karatzikou, M.; Tzallas, A.T.; Giannakeas, N.; Astrakas, L.G.; Angelidis, P.; Glavas, E.; Grigoriadis, N.; et al. Analysis of electroencephalographic signals complexity regarding Alzheimer’s Disease. Comput. Electr. Eng. 2019, 76, 198–212. [Google Scholar] [CrossRef]
- Fiscon, G.; Weitschek, E.; Cialini, A.; Felici, G.; Bertolazzi, P.; De Salvo, S.; Bramanti, A.; Bramanti, P.; De Cola, M.C. Combining EEG signal processing with supervised methods for Alzheimer’s patients classification. BMC Med. Inform. Decis. Mak. 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Safi, M.S.; Safi, S.M.M. Early detection of Alzheimer’s disease from EEG signals using Hjorth parameters. Biomed. Signal Process. Control 2021, 65, 102338. [Google Scholar] [CrossRef]
- Tzimourta, K.D.; Christou, V.; Tzallas, A.T.; Giannakeas, N.; Astrakas, L.G.; Angelidis, P.; Tsalikakis, D.; Tsipouras, M.G. Machine Learning Algorithms and Statistical Approaches for Alzheimer’s Disease Analysis Based on Resting-State EEG Recordings: A Systematic Review. Int. J. Neural Syst. 2021, 31, 2130002. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Y.; Wang, J.; Zheng, X. Comparison of classification methods on EEG signals based on wavelet packet decomposition. Neural Comput. Appl. 2015, 26, 1217–1225. [Google Scholar] [CrossRef]
- Dottori, M.; Sedeño, L.; Caro, M.M.; Alifano, F.; Hesse, E.; Mikulan, E.; García, A.M.; Ruiz-Tagle, A.; Lillo, P.; Slachevsky, A.; et al. Towards affordable biomarkers of frontotemporal dementia: A classification study via network’s information sharing. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotte, F.; Congedo, M.; Lécuyer, A.; Lamarche, F.; Arnaldi, B. A review of classification algorithms for EEG-based brain–computer interfaces. J. Neural Eng. 2007, 4, R1–R13. [Google Scholar] [CrossRef]
- Morabito, F.C.; Campolo, M.; Ieracitano, C.; Ebadi, J.M.; Bonanno, L.; Bramanti, A.; Desalvo, S.; Mammone, N.; Bramanti, P. Deep convolutional neural networks for classification of mild cognitive impaired and Alzheimer’s disease patients from scalp EEG recordings. In Proceedings of the 2016 IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a better tomorrow (RTSI), Bologna, Italy, 7–9 September 2016; pp. 1–6. [Google Scholar]
- Nishida, K.; Yoshimura, M.; Isotani, T.; Yoshida, T.; Kitaura, Y.; Saito, A.; Mii, H.; Kato, M.; Takekita, Y.; Suwa, A.; et al. Differences in quantitative EEG between frontotemporal dementia and Alzheimer’s disease as revealed by LORETA. Clin. Neurophysiol. 2011, 122, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, M.; Nancy, A.; Vijaykumar, S. Alzheimer’s Disease Diagnosis by using Dimensionality Reduction Based on Knn Classifier. Biomed. Pharmacol. J. 2017, 10, 1823–1830. [Google Scholar] [CrossRef]
- Siuly, S.; Wang, H.; Zhang, Y. Detection of motor imagery EEG signals employing Naïve Bayes based learning process. Measurement 2016, 86, 148–158. [Google Scholar] [CrossRef]
- Seixas, F.L.; Zadrozny, B.; Laks, J.; Conci, A.; Saade, D.C.M. A Bayesian network decision model for supporting the diagnosis of dementia, Alzheimer’s disease and mild cognitive impairment. Comput. Biol. Med. 2014, 51, 140–158. [Google Scholar] [CrossRef] [Green Version]
- Tzimourta, K.D.; Giannakeas, N.; Tzallas, A.T.; Astrakas, L.G.; Afrantou, T.; Ioannidis, P.; Grigoriadis, N.; Angelidis, P.; Tsalikakis, D.G.; Tsipouras, M.G. EEG Window Length Evaluation for the Detection of Alzheimer’s Disease over Different Brain Regions. Brain Sci. 2019, 9, 81. [Google Scholar] [CrossRef] [Green Version]
- Renard, Y.; Lotte, F.; Gibert, G.; Congedo, M.; Maby, E.; Delannoy, V.; Bertrand, O.; Lécuyer, A. OpenViBE: An Open-Source Software Platform to Design, Test, and Use Brain–Computer Interfaces in Real and Virtual Environments. Presence Teleoperators Virtual Environ. 2010, 19, 35–53. [Google Scholar] [CrossRef] [Green Version]
- Kurlowicz, L.; Wallace, M. The Mini-Mental State Examination (MMSE). J. Gerontol. Nurs. 1999, 25, 8–9. [Google Scholar] [CrossRef]
- Morris, J.C. Clinical Dementia Rating: A Reliable and Valid Diagnostic and Staging Measure for Dementia of the Alzheimer Type. Int. Psychogeriatr. 1997, 9, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Babiloni, C.; Triggiani, A.I.; Elizio, R.; Ecordone, S.; Etattoli, G.; Bevilacqua, V.; Soricelli, A.; Ferri, R.; Nobili, F.; Egesualdo, L.; et al. Classification of Single Normal and Alzheimer’s Disease Individuals from Cortical Sources of Resting State EEG Rhythms. Front. Neurosci. 2016, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzallas, A.T.; Tsipouras, M.G.; Fotiadis, D.I. Automatic Seizure Detection Based on Time-Frequency Analysis and Artificial Neural Networks. Comput. Intell. Neurosci. 2007, 2007, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Isler, Y.; Narin, A.; Ozer, M. Comparison of the Effects of Cross-validation Methods on Determining Performances of Classifiers Used in Diagnosing Congestive Heart Failure. Meas. Sci. Rev. 2015, 15, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Häfner, M.; Liedlgruber, M.; Maimone, S.; Uhl, A.; Vecsei, A.; Wrba, F. Evaluation of cross-validation protocols for the classification of endoscopic images of colonic polyps. In Proceedings of the 2012 25th IEEE International Symposium on Computer-Based Medical Systems (CBMS), Rome, Italy, 20–22 June 2012; pp. 1–6. [Google Scholar] [CrossRef]
- Pascual-Marqui, R.D.; Lehmann, D.; Koenig, T.; Kochi, K.; Merlo, M.C.; Hell, D.; Koukkou, M. Low resolution brain electromagnetic tomography (LORETA) functional imaging in acute, neuroleptic-naive, first-episode, productive schizophrenia. Psychiatry Res. Neuroimag. 1999, 90, 169–179. [Google Scholar] [CrossRef]
- Lindau, M.; Jelic, V.; Johansson, S.-E.; Andersen, C.; Wahlund, L.-O.; Almkvist, O. Quantitative EEG Abnormalities and Cognitive Dysfunctions in Frontotemporal Dementia and Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2003, 15, 106–114. [Google Scholar] [CrossRef]
- Relationship between EEG Alpha3/Alpha2 Ratio and the Nucleus Accumbens in Subjects with Mild Cognitive Impairment. J. Neurol. Neurophysiol. 2013, 4. [CrossRef]
- Caso, F.; Cursi, M.; Magnani, G.; Fanelli, G.; Falautano, M.; Comi, G.; Leocani, L.; Minicucci, F. Quantitative EEG and LORETA: Valuable tools in discerning FTD from AD? Neurobiol. Aging 2012, 33, 2343–2356. [Google Scholar] [CrossRef] [PubMed]
- Babiloni, C.; Del Percio, C.; Lizio, R.; Noce, G.; Lopez, S.; Soricelli, A.; Ferri, R.; Nobili, F.; Arnaldi, D.; Famà, F.; et al. Abnormalities of resting-state functional cortical connectivity in patients with dementia due to Alzheimer’s and Lewy body diseases: An EEG study. Neurobiol. Aging 2018, 65, 18–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Gender (Male/Female) | Age | MMSE | CDR | Disease Duration in Months | |
|---|---|---|---|---|---|
| AD | 6/4 | 70.5 (7.1) | 19.7 (2.76) | 1 (0.54) | 24 (9.88) |
| FTD | 6/4 | 67.5 (4.5) | 21.5 (1.83) | 0.75 (0.26) | 26 (9.24) |
| CN | 4/4 | 68.5 (7.2) | 30 (0) | - | - |
| Accuracy of Classification Problem | Decision Trees | Random Forests | AΝΝ | SVM | Naïve Bayes | kNN |
|---|---|---|---|---|---|---|
| AD/CN | 96% | 99.1% | 95% | 96.2% | 80% | 96% |
| FTD/CN | 94.2% | 98% | 98% | 97% | 77% | 97% |
| AD/FTD | 93.8% | 97.7% | 90% | 91% | 69% | 95% |
| Sensitivity of Classification Problem | Decision Trees | Random Forests | AΝΝ | SVM | Naïve Bayes | kNN |
| AD/CN | 96.6% | 98.6% | 96% | 98% | 94% | 96% |
| FTD/CN | 94.1% | 98% | 98.5% | 97% | 98% | 98% |
| AD/FTD | 95.6% | 97.8% | 91% | 96% | 80% | 96% |
| Specificity of Classification Problem | Decision Trees | Random Forests | AΝΝ | SVM | Naïve Bayes | kNN |
| AD/CN | 95% | 99% | 94% | 94.4% | 58% | 96% |
| FTD/CN | 94.4% | 98% | 95% | 97% | 62% | 99% |
| AD/FTD | 91.3% | 97.5% | 89.1% | 86% | 54% | 94% |
| Classification | AD/CN | FTD/CN | AD/FTD | |||
| Algorithm | MEAN | SD | MEAN | SD | MEAN | SD |
| Decision trees | 78.50% | 5.8 | 79.60% | 11.2 | 73% | 11 |
| Random forests | 77.07% | 7.1 | 86.30% | 7.1 | 64% | 12.6 |
| ANN | 73% | 9.4 | 69.20% | 14.1 | 61% | 15.89 |
| SVM | 68.00% | 11.1 | 75% | 12.6 | 68% | 18 |
| Naïve Bayes | 63% | 14 | 73.80% | 25 | 52% | 21.3 |
| kNN | 60% | 11.3 | 67.30% | 9.8 | 51% | 18.2 |
| AD/CN | FTD/CN | |||
| Sensitivity | Specificity | Sensitivity | Specificity | |
| Decision trees | 82.40% | 74% | 82.20% | 77.45% |
| Random forests | 78.70% | 76% | 87% | 83% |
| Writers | Year | Sample (AD/FTDFTD/CN) | Methodology | Classification Problem | Results | ||
|---|---|---|---|---|---|---|---|
| ACC | SENS | SPEC | |||||
| Lindau et al. [50] | 2003 | 16-19-0 | Power spectrum of EEG rhythms, cohesion, dominant rhythm | AD/FTD | 93.30 | - | - |
| Nishida et al. [37] | 2011 | 19-19-22 | EEG rhythms energy, sLORETTA, kNN | FTD/CN AD/CN FTD/AD | 85.80 92.80 89.80 | 55.00 74.00 74.00 | 84.00 73.00 63.00 |
| Caso et al. [52] | 2012 | 39-39-39 | Relative power of EEG rhythms, sLORETTA, ANOVA analysis | AD + FTD/CN AD/FTD | - - | 44.87 48.72 | 85 85 |
| Dottori et al. [34] | 2017 | 13-13-25 | Connectivity features, SVM | AD + FTD/CN AD/FTD AD/CN | 54.00 73.00 73.00 | - - - | - - - |
| Fiscon D. et al. [30] | 2018 | 86-0-23 | Discrete Fourier transform, wavelet analysis, decision trees | AD/CN | 83 | ||
| Safi M, et al. [31] | 2021 | 51-0-35 | Hjorth parameters, discrete wavelet transform, SVM, kNN | AD/CN | 97.6 | ||
| Proposed Methodology | 2021 | 10-10-8 | Energy, mean, variance, IQR, random forests, decision trees | AD/CN FTD/CN | 78.5 86.3 | 82.4 87 | 74 83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miltiadous, A.; Tzimourta, K.D.; Giannakeas, N.; Tsipouras, M.G.; Afrantou, T.; Ioannidis, P.; Tzallas, A.T. Alzheimer’s Disease and Frontotemporal Dementia: A Robust Classification Method of EEG Signals and a Comparison of Validation Methods. Diagnostics 2021, 11, 1437. https://doi.org/10.3390/diagnostics11081437
Miltiadous A, Tzimourta KD, Giannakeas N, Tsipouras MG, Afrantou T, Ioannidis P, Tzallas AT. Alzheimer’s Disease and Frontotemporal Dementia: A Robust Classification Method of EEG Signals and a Comparison of Validation Methods. Diagnostics. 2021; 11(8):1437. https://doi.org/10.3390/diagnostics11081437
Chicago/Turabian StyleMiltiadous, Andreas, Katerina D. Tzimourta, Nikolaos Giannakeas, Markos G. Tsipouras, Theodora Afrantou, Panagiotis Ioannidis, and Alexandros T. Tzallas. 2021. "Alzheimer’s Disease and Frontotemporal Dementia: A Robust Classification Method of EEG Signals and a Comparison of Validation Methods" Diagnostics 11, no. 8: 1437. https://doi.org/10.3390/diagnostics11081437
APA StyleMiltiadous, A., Tzimourta, K. D., Giannakeas, N., Tsipouras, M. G., Afrantou, T., Ioannidis, P., & Tzallas, A. T. (2021). Alzheimer’s Disease and Frontotemporal Dementia: A Robust Classification Method of EEG Signals and a Comparison of Validation Methods. Diagnostics, 11(8), 1437. https://doi.org/10.3390/diagnostics11081437