
Accuracy of Pretreatment Ultrasonography Assessment of Intra-Abdominal Spread in Epithelial Ovarian Cancer: A Prospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Imaging Technique (Index Test)
2.4. Surgery and Histology (Reference Standard)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| EFSUMB | European Federation of Societes for Ultrasound in Medicine and Biology |
| EOC | epithelial ovarian cancer |
| ESGO | European Society of Gynecological Oncology |
| F-FDG PET | 18F-fluorodeoxyglucose positron emission tomography |
| FIGO | International Federation of Gynecology and Obstetrics |
| FN | false negative |
| MI | mutual information |
| MRI | magnetic resonance imaging |
| NPV | negative predictive value |
| PPV | positive predictive value |
| PS-ECOG | Eastern Cooperative Oncology Group Performance Status |
| STARD | Standards for Reporting Diagnostic Accuracy |
| TP | true positive |
References
- Colombo, N.; Sessa, C.; Bois, A.D.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Int. J. Gynecol. Cancer 2019, 30, 672–705. [Google Scholar] [CrossRef] [Green Version]
- ECIS—European Cancer Information System. 2021. Available online: https://ecis.jrc.ec.europa.eu/ (accessed on 27 July 2021).
- Gill, S.E.; McGree, M.E.; Weaver, A.L.; Cliby, W.A.; Langstraat, C.L. Optimizing the treatment of ovarian cancer: Neoadjuvant chemotherapy and interval debulking versus primary debulking surgery for epithelial ovarian cancers likely to have suboptimal resection. Gynecol. Oncol. 2017, 144, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Bookman, M.A. Optimal primary therapy of ovarian cancer. Ann. Oncol. 2016, 27 (Suppl. S1), i58–i62. [Google Scholar] [CrossRef]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of Deficits as a Proxy Measure of Aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Janco, J.M.; Mariani, A.; Bakkum-Gamez, J.N.; Langstraat, C.L.; Weaver, A.L.; McGree, M.E.; Cliby, W.A. Risk-prediction model of severe postoperative complications after primary debulking surgery for advanced ovarian cancer. Gynecol. Oncol. 2016, 140, 15–21. [Google Scholar] [CrossRef]
- Inci, M.G.; Anders, L.; Woopen, H.; Richter, R.; Guzel, D.; Armbrust, R.; Sehouli, J. Frailty Index for prediction of surgical outcome in ovarian cancer: Results of a prospective study. Gynecol. Oncol. 2021, 161, 396–401. [Google Scholar] [CrossRef]
- Kaijser, J. Towards an evidence-based approach for diagnosis and management of adnexal masses: Findings of the International Ovarian Tumour Analysis (IOTA) studies. Facts Views Vis. Obstet. Gynaecol. 2015, 7, 42–59. [Google Scholar]
- Meys, E.M.; Kaijser, J.F.; Kruitwagen, R.; Slangen, B.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.; Timmerman, D.; Van Gorp, T. Subjective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur. J. Cancer 2016, 58, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Forstner, R.; Hricak, H.; Occhipinti, K.A.; Powell, C.B.; Frankel, S.D.; Stern, J.L. Ovarian cancer: Staging with CT and MR imaging. Radiology 1995, 197, 619–626. [Google Scholar] [CrossRef]
- Michielsen, K.; Dresen, R.; Vanslembrouck, R.; De Keyzer, F.; Amant, F.; Mussen, E.; Leunen, K.; Berteloot, P.; Moerman, P.; Vergote, I.; et al. Diagnostic value of whole body diffusion-weighted MRI compared to computed tomography for pre-operative assessment of patients suspected for ovarian cancer. Eur. J. Cancer 2017, 83, 88–98. [Google Scholar] [CrossRef]
- Testa, A.C.; Ludovisi, M.; Mascilini, F.; Di Legge, A.; Malaggese, M.; Fagotti, A.; Fanfani, F.; Salerno, M.G.; Ercoli, A.; Scambia, G.; et al. Ultrasound evaluation of intra-abdominal sites of disease to predict likelihood of suboptimal cytoreduction in advanced ovarian cancer: A prospective study. Ultrasound Obstet. Gynecol. 2011, 39, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, V.; Fischerova, D.; Semeradova, I.; Slama, J.; Dundr, P.; Dusek, L.; Cibula, D.; Zikan, M. Prospective Evaluation of Ultrasound Accuracy in the Detection of Pelvic Carcinomatosis in Patients with Ovarian Cancer. Ultrasound Med. Biol. 2016, 42, 2196–2202. [Google Scholar] [CrossRef]
- Fischerova, D.; Zikan, M.; Semeradova, I.; Slama, J.; Kocian, R.; Dundr, P.; Němejcová, K.; Burgetova, A.; Dušek, L.; Cibula, D. Ultrasound in preoperative assessment of pelvic and abdominal spread in patients with ovarian cancer: A prospective study. Ultrasound Obstet. Gynecol. 2017, 49, 263–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zikan, M.; Fischerova, D.; Semeradova, I.; Slama, J.; Dundr, P.; Weinberger, V.; Dusek, L.; Cibula, D. Accuracy of ultrasound in prediction of rectosigmoid infiltration in epithelial ovarian cancer. Ultrasound Obstet. Gynecol. 2017, 50, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Caparros, M.; Arraiza, M.; Mínguez, J.Á.; Guerriero, S.; Chiva, L.; Jurado, M. Pre-operative assessment of intra-abdominal disease spread in epithelial ovarian cancer: A comparative study between ultrasound and computed tomography. Int. J. Gynecol. Cancer 2019, 29, 227–233. [Google Scholar] [CrossRef] [PubMed]
- De Blasis, I.; Moruzzi, M.C.; Moro, F.; Mascilini, F.; Cianci, S.; Alletti, S.G.; Turco, L.C.; Garganese, G.; Scambia, G.; Testa, A.C. Role of ultrasound in advanced peritoneal malignancies. Minerva Med. 2019, 110, 292–300. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerová, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [Green Version]
- Stukan, M.; Badocha, M.; Ratajczak, K. Development and validation of a model that includes two ultrasound parameters and the plasma D-dimer level for predicting malignancy in adnexal masses: An observational study. BMC Cancer 2019, 19, 564. [Google Scholar] [CrossRef] [PubMed]
- Education and Practical Standards Committee, European Federation of Societies for Ultrasound in Medicine and Biology. Minimum training recommendations for the practice of medical ultrasound. Ultraschall Med. Eur. J. Ultrasound 2006, 27, 79–95. [Google Scholar] [CrossRef] [Green Version]
- Fischerova, D. Ultrasound scanning of the pelvis and abdomen for staging of gynecological tumors: A review. Ultrasound Obstet. Gynecol. 2011, 38, 246–266. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.C.; Van Holsbeke, C.; Mascilini, F.; Timmerman, D. Dynamic and interactive gynecological ultrasound examination. Ultrasound Obstet. Gynecol. 2009, 34, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Valentin, L.; Bourne, T.H.; Collins, W.P.; Verrelst, H.; Vergote, I.; International Ovarian Tumor Analysis (IOTA) Group. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: A consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound. Obstet. Gynecol. 2000, 16, 500–505. [Google Scholar] [CrossRef]
- Aletti, G.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. Am. J. Obstet. Gynecol. 2007, 197, 676.e1–676.e7. [Google Scholar] [CrossRef]
- Prat, J. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynecol. Obstet. 2013, 124, 1–5. [Google Scholar] [CrossRef]
- Fagotti, A.; Vizzielli, G.; DE Iaco, P.; Surico, D.; Buda, A.; Mandato, V.D.; Petruzzelli, F.; Ghezzi, F.; Garzarelli, S.; Mereu, L.; et al. A multicentric trial (Olympia–MITO 13) on the accuracy of laparoscopy to assess peritoneal spread in ovarian cancer. Am. J. Obstet. Gynecol. 2013, 209, 462.e1–462.e11. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 20 April 2021).
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; De Vet, H.C.W.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [Green Version]
- Bujang, M.A.; Adnan, T.H. Requirements for Minimum Sample Size for Sensitivity and Specificity Analysis. J. Clin. Diagn. Res. 2016, 10, YE01–YE06. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in diagnostic test studies of biomedical informatics. J. Biomed. Inform. 2014, 48, 193–204. [Google Scholar] [CrossRef] [Green Version]
- Wimberger, P.; Wehling, M.; Lehmann, N.; Kimmig, R.; Schmalfeldt, B.; Burges, A.; Harter, P.; Pfisterer, J.; Du Bois, A. Influence of Residual Tumor on Outcome in Ovarian Cancer Patients With FIGO Stage IV Disease: An exploratory analysis of the AGO-OVAR (Arbeitsgemeinschaft Gynaekologische Onkologie Ovarian Cancer Study Group). Ann. Surg. Oncol. 2010, 17, 1642–1648. [Google Scholar] [CrossRef]
- Stukan, M.; Alcazar, J.L.; Gębicki, J.; Epstein, E.; Liro, M.; Sufliarska, A.; Szubert, S.; Guerriero, S.; Braicu, E.I.; Szajewski, M.; et al. Ultrasound and Clinical Preoperative Characteristics for Discrimination Between Ovarian Metastatic Colorectal Cancer and Primary Ovarian Cancer: A Case-Control Study. Diagnostics 2019, 9, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stukan, M.; Bugalho, A.; Kumar, A.; Kowalewska, J.; Świetlik, D.; Buda, N.; Pietrzak-Stukan, M.; Dudziak, M. Lung and Intercostal Upper Abdomen Ultrasonography for Staging Patients with Ovarian Cancer: A Method Description and Feasibility Study. Diagnostics 2020, 10, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagotti, A.; Ferrandina, M.G.; Fanfani, F.; Ercoli, A.; Lorusso, D.; Rossi, M.; Scambia, G. A Laparoscopy-Based Score To Predict Surgical Outcome in Patients With Advanced Ovarian Carcinoma: A Pilot Study. Ann. Surg. Oncol. 2006, 13, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Widschwendter, P.; Blersch, A.; Friedl, T.W.P.; Janni, W.; Kloth, C.; De Gregorio, A.; De Gregorio, N. CT Scan in the Prediction of Lymph Node Involvement in Ovarian Cancer—A Retrospective Analysis of a Tertiary Gyneco-Oncological Unit. Geburtshilfe Frauenheilkd 2020, 80, 518–525. [Google Scholar] [CrossRef] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Definition | Figure | Video |
|---|---|---|---|
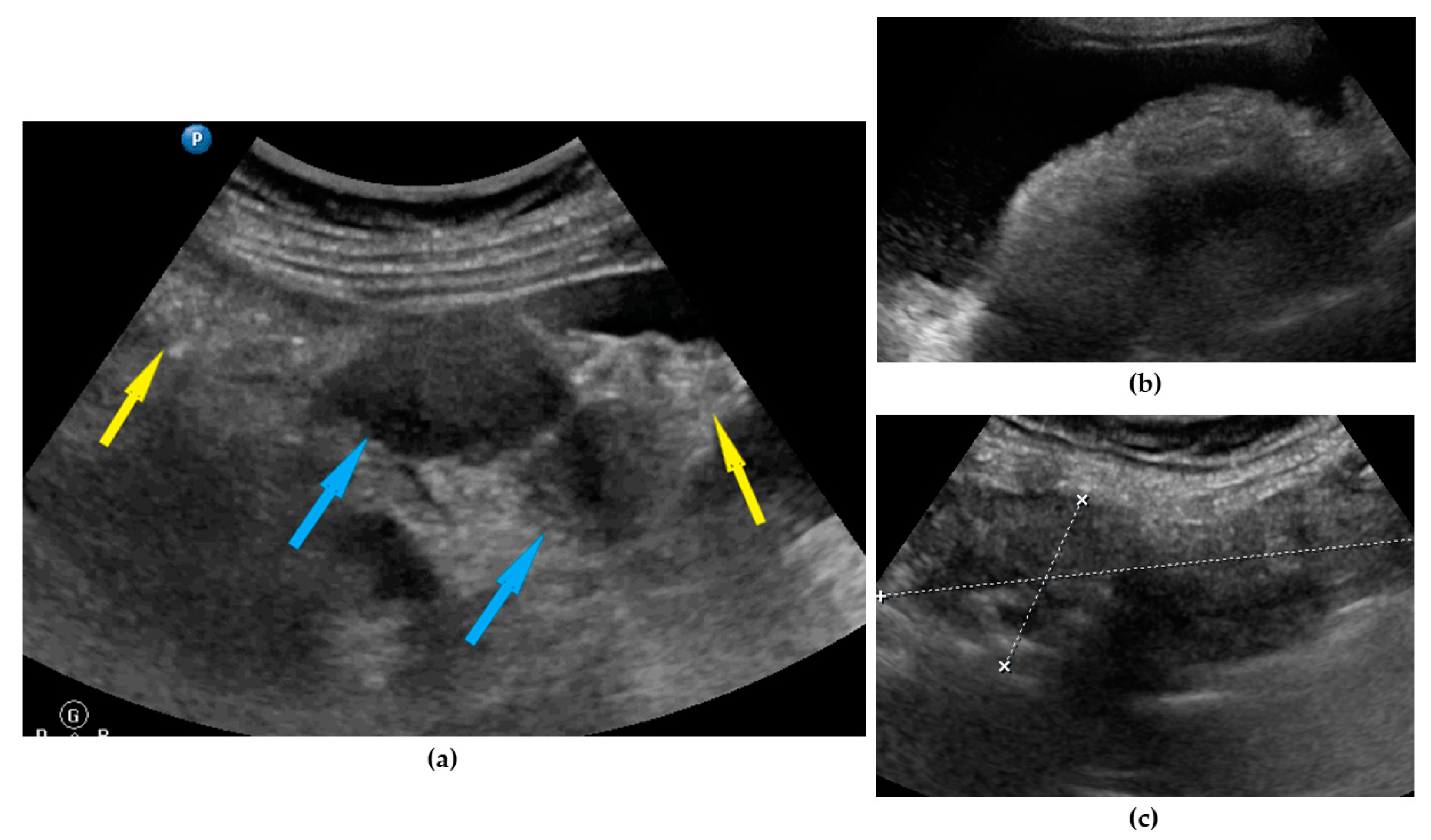
| Omentum | Focal infiltration of omentum: hypoechogenic nodules with discrete vascularization. Diffuse infiltration: omental cake appears as a nodular, perfuse, and non-peristaltic tumor that is located between the anterior abdominal wall and bowel loops. | Figure 1 | Video S1 |
| Small bowel mesentery root | Involvement is suspected when bowel loops have poor mobility and are “fixed together” in the dynamic ultrasound examination with a cauliflower-like image. | Figure 2 | Video S2 |
| Peritoneum, abdomen | Abdomen carcinomatosis manifest as hypoechogenic lesions over the peritoneal surface of the paracollic gutters or internal abdominal wall. | Figure 3 | Video S3 |
| Peritoneum, pelvis | Pelvic carcinomatosis manifests as hypoechogenic lesions over the peritoneal surface of the pelvic wall: laterally, in the pouch of Douglas (no rectum involvement) or the bladder in the uterine serosa. | Figure 4 | Video S4 |
| Ascites | Fluid outside the pouch of Douglas, recorded as being present or absent 1 | Figure 5 | Video S5 |
| Liver, parenchymal lesions | Single or multiple focal parenchymal lesions (with a “halo“ sign, necrosis, and indistinct borders) in the liver. | Figure 6 | Video S6 |
| Liver hilum | Presence of nodules or rigid structures in the region of the hepatic hilum. | Figure 7 | Video S7 |
| Spleen, parenchymal lesions | Single or multiple focal parenchymal lesions (with a “halo“ sign, necrosis, and indistinct borders) in the spleen. | Figure 8 | Video S8 |
| Spleen, hilum | Presence of nodules or rigid structures in the region of the spleen hilum. | Figure 9 | Video S9 |
| Diaphragm, right | Carcinomatosis manifests as hypoechogenic lesions over the peritoneal surface of the right diaphragm. | Figure 10 | Video S10 |
| Diaphragm, left | Carcinomatosis manifests as hypoechogenic lesions over the peritoneal surface of the left diaphragm. | Figure 11 | Video S11 |
| Frozen pelvis | Massive pelvic involvement: hypoechogenic tissue in the peritoneum in the pouch of Douglas, forming cohesion between ovarian masses, bowel, uterus, and posterior pelvic wall. It manifests in the dynamic ultrasound examination: absence of sliding sign between the rectum and uterus/ovaries and between the uterus, urinary bladder, and pelvic walls. | Figure 12 | Video S12 |
| Rectum-sigmoid | Suspected involvement of the rectosigmoid wall manifests as the presence of metastases over the wall of the rectum or sigmoid. | Figure 13 | Video S13 |
| Stage prediction | Subjective prediction of disease stage: early (FIGO IA–IIA) or advanced (FIGO IIB–IVB). | - | - |
| Surgical complexity prediction | Subjective prediction of surgical complexity, defined as described elsewhere 2, if open surgery with cytoreduction attempted or full staging. | - | - |
| Residual disease prediction | Subjective prediction of residual disease after surgery if debulking surgery is attempted. Note: residual disease prediction based on ultrasonography was made without stratification into advanced or early disease. | - | - |
| Parameter | Data |
|---|---|
| Age, years, median (range) | 62 (32–82) |
| BMI 1, kg/m2, median (range) | 26.8 (15.8–38.4) |
| CA125 2, U/mL, median (range) | 454 (20–20,050) |
| D-dimer, ng/mL, median (range) | 3416 (160–25,000) |
| ASA 3 score, n (%) | |
| I | 2 (1.5%) |
| II | 108 (82.4%) |
| III | 21 (16.1%) |
| Performance status 4 | |
| 0 | 23 (17.6%) |
| 1 | 81 (61.8%) |
| 2 | 23 (17.6%) |
| 3 | 4 (3.0%) |
| FIGO 5 stage | |
| I | 13 (9.8%) |
| IIA | 1 (0.7%) |
| IIB | 10 (7.5%) |
| IIIA1 | 8 (6.0%) |
| IIIB | 12 (9.0%) |
| IIIC | 64 (48.5%) |
| IVA | 9 (6.8%) |
| IVB | 15 (11.7) |
| Histology, type | |
| Serous | 95 (71.9%) |
| Endometrioid | 13 (9.8%) |
| Clear Cell | 7 (5.3%) |
| Mucinous | 7 (5.3%) |
| Non-differentiated | 3 (2.4%) |
| Mixed | 7 (5.3%) |
| Histology, grade | |
| G1 | 6 (4.5%) |
| G2 | 6 (4.5%) |
| G3 | 120 (91.0%) |
| Surgery | |
| Open (PDS 6/IDS 7 or full staging) | 113 (85.6%) |
| Diagnostic laparoscopy | 19 (14.4%) |
| Surgical complexity 8 | |
| for open surgery, FIGO 5 IIB-IVB | |
| low | 16 (16%) |
| intermediate | 41 (41%) |
| high | 43 (43%) |
| Residual disease | |
| for open surgery, FIGO 5 IIB-IVB | |
| R0 (complete macroscopic resection) | 66 (66%) |
| R < 1 cm | 7 (7%) |
| R > 1 cm | 27 (27%) |
| Parameter | Ultrasound |
|---|---|
| Omentum | |
| No involvement | 56 (42.4%) |
| Nodules | 7 (5.3%) |
| Gross involvement | 69 (52.3%) |
| Small bowel mesentery root involvement, n (%) | 17 (12.9%) |
| Peritoneum, abdomen, lesions, n (%) | 46 (34.8%) |
| Peritoneum, pelvis, lesions, n (%) | 88 (66.7%) |
| Ascites, yes, n (%) | 65 (49.2%) |
| Liver, parenchymal lesions detected, n (%) | 4 (3.0%) |
| Liver hilum involvement, n (%) | 9 (6.8%) |
| Spleen, parenchymal lesions detected, n (%) | 1 (0.7%) |
| Spleen, hilum involvement, n (%) | 39 (29.5%) |
| Diaphragm, right, lesions, n (%) | 52 (39.4%) |
| Diaphragm, left, lesions, n (%) | 12 (9.0%) |
| Frozen pelvis detected, n (%) | 31 (23.5%) |
| Rectum-sigmoid involvement, n (%) | 70 (53.0%) |
| Stage prediction 1 | |
| early | 31 (23.5%) |
| advanced | 101 (76.5%) |
| Surgical complexity prediction 2 | |
| low | 1 (0.7%) |
| intermediate | 58 (43.9%) |
| high | 73 (55.4%) |
| Residual disease prediction 3 | |
| R0 (no macroscopic disease) | 98 (74.9%) |
| R < 1 cm | 9 (6.8%) |
| R > 1 cm | 25 (18.3%) |
| Parameter | Sensitivity % | Specificity % | PPV 1 % | NPV 2 % | Accuracy % | p |
|---|---|---|---|---|---|---|
| Omentum, gross involvement | 96.9 | 89.4 | 89.9 | 96.7 | 93.1 | <0.001 |
| Omentum, small nodules | 17.4 | 97.2 | 57.1 | 84.6 | 83.1 | |
| Small bowel mesentery root | 95.5 | 92.3 | 99.1 | 70.6 | 95.2 | <0.001 |
| Peritoneum, abdomen | 87.7 | 53.4 | 59.5 | 84.8 | 68.5 | <0.001 |
| Peritoneum, pelvis | 80.0 | 81.2 | 55.8 | 93.2 | 80.9 | <0.001 |
| Ascites | 95.5 | 96.9 | 97.0 | 95.4 | 96.2 | <0.001 |
| Liver, parenchymal | 99.2 | 100 | 100 | 75.0 | 99.2 | <0.001 |
| Liver hilum | 99.1 | 42.1 | 91.1 | 88.9 | 90.9 | <0.001 |
| Spleen, parenchymal 3 | 100 | 100 | 100 | 100 | 100 | 0.008 |
| Spleen, hilum | 90.3 | 76.9 | 90.3 | 76.9 | 86.4 | <0.001 |
| Diaphragm, right | 90.0 | 59.5 | 58.4 | 90.4 | 71.3 | <0.001 |
| Diaphragm, left | 94.8 | 20.6 | 77.1 | 58.3 | 75.4 | 0.01 |
| Frozen pelvis | 94.8 | 76.5 | 91.9 | 83.9 | 90.0 | <0.001 |
| Rectum | 81.4 | 91.9 | 91.9 | 81.4 | 86.4 | <0.001 |
| Stage prediction 4 | 88.0 | 75.0 | 94.1 | 58.1 | 85.6 | <0.001 |
| Surgical complexity prediction 5 | 83.7 | 72.9 | 65.5 | 87.9 | 77.0 | <0.001 |
| Residual disease prediction 6 | 41.2 | 97.5 | 87.5 | 79.4 | 80.5 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomasińska, A.; Stukan, M.; Badocha, M.; Myszewska, A. Accuracy of Pretreatment Ultrasonography Assessment of Intra-Abdominal Spread in Epithelial Ovarian Cancer: A Prospective Study. Diagnostics 2021, 11, 1600. https://doi.org/10.3390/diagnostics11091600
Tomasińska A, Stukan M, Badocha M, Myszewska A. Accuracy of Pretreatment Ultrasonography Assessment of Intra-Abdominal Spread in Epithelial Ovarian Cancer: A Prospective Study. Diagnostics. 2021; 11(9):1600. https://doi.org/10.3390/diagnostics11091600
Chicago/Turabian StyleTomasińska, Agnieszka, Maciej Stukan, Michał Badocha, and Aleksandra Myszewska. 2021. "Accuracy of Pretreatment Ultrasonography Assessment of Intra-Abdominal Spread in Epithelial Ovarian Cancer: A Prospective Study" Diagnostics 11, no. 9: 1600. https://doi.org/10.3390/diagnostics11091600
APA StyleTomasińska, A., Stukan, M., Badocha, M., & Myszewska, A. (2021). Accuracy of Pretreatment Ultrasonography Assessment of Intra-Abdominal Spread in Epithelial Ovarian Cancer: A Prospective Study. Diagnostics, 11(9), 1600. https://doi.org/10.3390/diagnostics11091600