
A Rapid, Simple, Trace, Cost-Effective, and High-Throughput Stable Isotope-Dilution Liquid Chromatography–Tandem Mass Spectrometry Method for Serum Methylmalonic Acid Quantification and Its Clinical Applications
 ,
,
Abstract
:Highlights
- An established method for trace, simple, rapid, cheap, sensitive, accurate, robust, and high-throughput for methylmalonic acid quantification.
- Good chromatographic separation of MMA and its intrinsic isomer and good signals of MMA were achieved using a simple isocratic elution strategy.
- Materials and reagents that are complex or not always accessible and procedures in previous methods such as derivatization, multistep SPE, incubations, evaporations, drying, or reconstitutions are not required in this MMA quantification method.
- This method is suitable for large-scale MMA testing.
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Samples
2.3. Calibrators, Internal Standard (IS), and Quality Control (QC) Materials Preparation
2.4. Sample Preparation
2.5. LC-MS/MS Conditions
2.6. Method Validation
2.6.1. Limits of Detection (LOD) and Limits of Quantification (LOQ)
2.6.2. Analytical Precision and Recovery
2.6.3. Matrix Effect
2.7. Method Applications
2.8. Statistical Analysis
3. Results
3.1. Optimization of the Mobile Phase Strategy
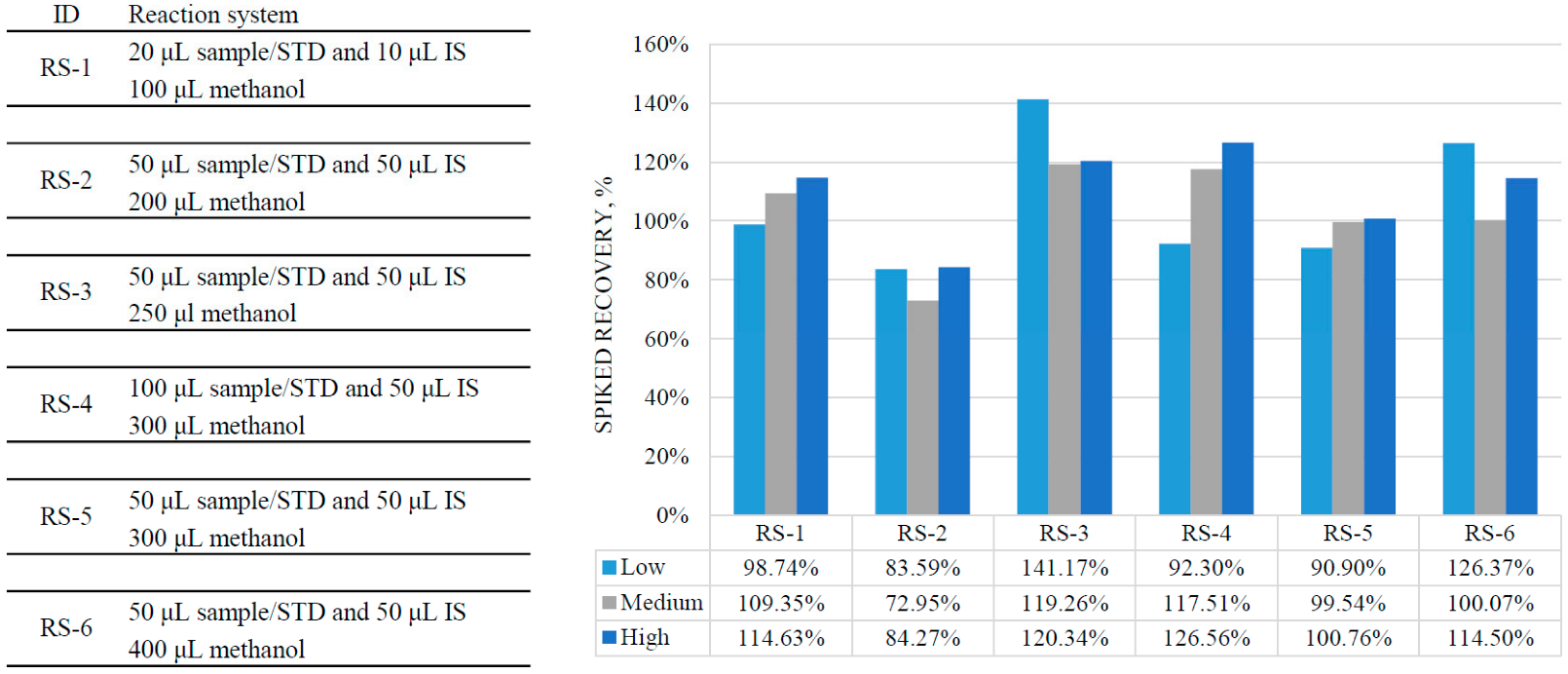
3.2. Optimization of Sample Preparation
3.3. Method Validation
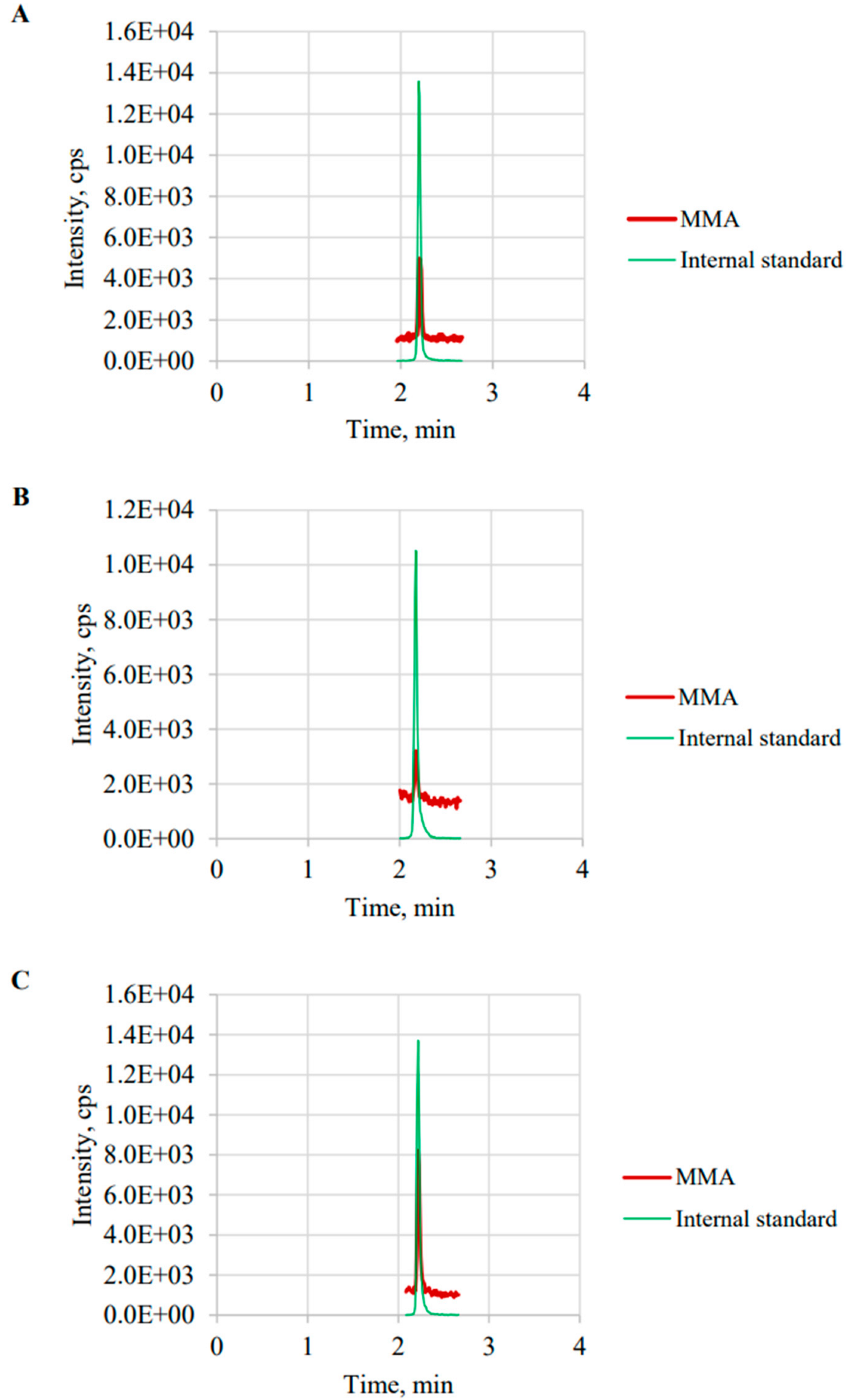
3.3.1. Chromatographic Separation
3.3.2. Linearity, LOD, and LOQ
3.3.3. Precision and Recovery
3.3.4. Matrix Effect
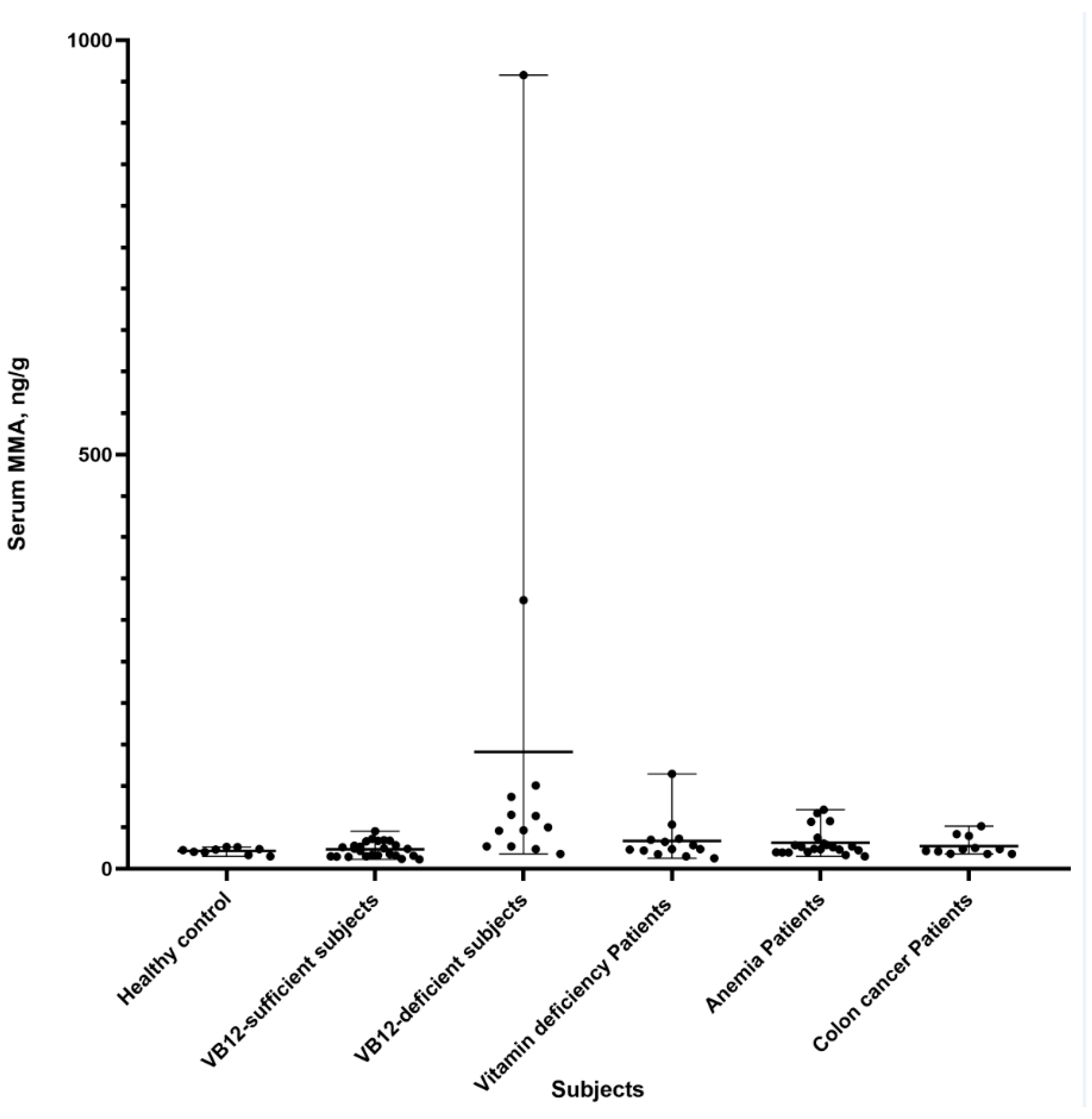
3.4. Clinical Application
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cox, E.V.; White, A.M. Methylmalonic acid excretion: An index of vitamin-B12 deficiency. Lancet 1962, 2, 853–856. [Google Scholar] [CrossRef]
- Rosenberg, L.E.; Lilljeqvist, A.; Hsia, Y.E. Methylmalonic aciduria: Metabolic block localization and vitamin B 12 dependency. Science 1968, 162, 805–807. [Google Scholar] [CrossRef] [PubMed]
- Hunt, A.; Harrington, D.; Robinson, S. Vitamin B12 deficiency. BMJ 2014, 349, g5226. [Google Scholar] [CrossRef] [PubMed]
- Stabler, S. Vitamin B12 deficiency. N. Engl. J. Med. 2013, 368, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Haijes, H.A.; Jans, J.J.M.; Tas, S.Y.; Verhoeven-Duif, N.M.; van Hasselt, P.M. Pathophysiology of propionic and methylmalonic acidemias. Part 1: Complications. J. Inherit. Metab. Dis. 2019, 42, 730–744. [Google Scholar] [CrossRef] [PubMed]
- Elin, R.J.; Winter, W.E. Methylmalonic acid: A test whose time has come? Arch. Pathol. Lab. Med. 2001, 125, 824–827. [Google Scholar] [CrossRef]
- Allen, L. How common is vitamin B-12 deficiency? Am. J. Clin. Nutr. 2009, 89, S693–S696. [Google Scholar] [CrossRef]
- Longo, N.; Sass, J.O.; Jurecka, A.; Vockley, J. Biomarkers for drug development in propionic and methylmalonic acidemias. J. Inherit. Metab. Dis. 2022, 45, 132–143. [Google Scholar] [CrossRef]
- Devalia, V.; Hamilton, M.; Molloy, A. Guidelines for the diagnosis and treatment of cobalaminand folate disorders. Br. J. Haematol. 2014, 166, 496–513. [Google Scholar] [CrossRef]
- Mastropaolo, W.; Wilson, M.A. Effect of light on serum B12 and folate stability. Clin. Chem. 1993, 39, 913. [Google Scholar] [CrossRef]
- Reineks, E.Z.; Hughes, A.; Wang, S. Effect of storage temperature or collection tube type on blood methylmalonic acid concentrations measured by gas chromatography-mass spectrometry. Clin. Chem. Lab. Med. 2010, 48, 1351–1353. [Google Scholar] [CrossRef] [PubMed]
- Monsen, A.L.; Refsum, H.; Markestad, T.; Ueland, P.M. Cobalamin status and its biochemical markers methylmalonic acid and homocysteine in different age groups from 4 days to 19 years. Clin. Chem. 2003, 49, 2067–2075. [Google Scholar] [CrossRef]
- Holleland, G.; Schneede, J.; Ueland, P.M.; Lund, P.K.; Refsum, H.; Sandberg, S. Cobalamin deficiency in general practice. Assessment of the diagnostic utility and cost-benefit analysis of methylmalonic acid determination in relation to current diagnostic strategies. Clin. Chem. 1999, 45, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Blom, H.J.; van Rooij, A.; Hogeveen, M. A simple high-throughput method for the determination of plasma methylmalonic acid by liquid chromatography-tandem mass spectrometry. Clin. Chem. Lab. Med. 2007, 45, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Valente, E.; Scott, J.; Ueland, P.; Cunningham, C.; Casey, M.; Molloy, A. Diagnostic accuracy of holotranscobalamin, methylmalonic acid, serum cobalamin, and other indicators of tissue vitamin B12 status in the elderly. Clin. Chem. 2011, 57, 856–863. [Google Scholar] [CrossRef]
- Sobczynńska-Malefora, A.; Gorska, R.; Pelisser, M.; Ruwona, P.; Witchlow, B.; Harrington, D. An audit of holotranscobalamin (“Active” B12) and methylmalonic acid assays for the assessment of vitamin B12 status: Application in a mixed patient population. Clin. Biochem. 2014, 47, 82–86. [Google Scholar] [CrossRef]
- Banerjee, S. Empowering Clinical Diagnostics with Mass Spectrometry. ACS Omega 2020, 5, 2041–2048. [Google Scholar] [CrossRef]
- McCann, M.T.; Thompson, M.M.; Gueron, I.C.; Lemieux, B.; Giguère, R.; Tuchman, M. Methylmalonic acid quantification by stable isotope dilution gas chromatography-mass spectrometry from filter paper urine samples. Clin. Chem. 1996, 42 Pt 1, 910–914. [Google Scholar] [CrossRef]
- Inoue, Y.; Ohse, M. Prenatal diagnosis of methylmalonic aciduria by measuring methylmalonic acid in dried amniotic fluid on filter paper using gas chromatography-mass spectrometry. Anal. Bioanal. Chem. 2011, 400, 1953–1958. [Google Scholar] [CrossRef]
- Stabler, S.P.; Marcell, P.D.; Podell, E.R.; Allen, R.H.; Lindenbaum, J. Assay of methylmalonic acid in the serum of patients with cobalamin deficiency using capillary gas chromatography-mass spectrometry. J. Clin. Investig. 1986, 77, 1606–1612. [Google Scholar] [CrossRef] [Green Version]
- Magera, M.J.; Helgeson, J.K.; Matern, D.; Rinaldo, P. Methylmalonic acid measured in plasma and urine by stable-isotope dilution and electrospray tandem mass spectrometry. Clin. Chem. 2000, 46, 1804–1810. [Google Scholar] [CrossRef] [PubMed]
- Kushnir, M.M.; Komaromy-Hiller, G.; Shushan, B.; Urry, F.M.; Roberts, W.L. Analysis of dicarboxylic acids by tandem mass spectrometry. High-throughput quantitative measurement of methylmalonic acid in serum, plasma, and urine. Clin. Chem. 2001, 47, 1993–2002. [Google Scholar] [CrossRef]
- Schmedes, A.; Brandslund, I. Analysis of methylmalonic acid in plasma by liquid chromatography-tandem mass spectrometry. Clin. Chem. 2006, 52, 754–757. [Google Scholar] [CrossRef] [PubMed]
- la Marca, G.; Malvagia, S.; Pasquini, E.; Innocenti, M.; Donati, M.A.; Zammarchi, E. Rapid 2nd-tier test for measurement of 3-OH-propionic and methylmalonic acids on dried blood spots: Reducing the false-positive rate for propionylcarnitine during expanded newborn screening by liquid chromatography-tandem mass spectrometry. Clin. Chem. 2007, 53, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Lakso, H.A.; Appelblad, P.; Schneede, J. Quantification of methylmalonic acid in human plasma with hydrophilic interaction liquid chromatography separation and mass spectrometric detection. Clin. Chem. 2008, 54, 2028–2035. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, V.M.; Kok, F. Determination of serum methylmalonic acid by alkylative extraction and liquid chromatography coupled to tandem mass spectrometry. Anal. Biochem. 2008, 381, 67–73. [Google Scholar] [CrossRef]
- Fasching, C.; Singh, J. Quantitation of methylmalonic acid in plasma using liquid chromatography-tandem mass spectrometry. Methods Mol. Biol. 2010, 603, 371–378. [Google Scholar]
- Pedersen, T.L.; Keyes, W.R.; Shahab-Ferdows, S.; Allen, L.H.; Newman, J.W. Methylmalonic acid quantification in low serum volumes by UPLC-MS/MS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2011, 879, 1502–1506. [Google Scholar] [CrossRef]
- Yuan, C.; Gabler, J.; El-Khoury, J.M.; Spatholt, R.; Wang, S. Highly sensitive and selective measurement of underivatized methylmalonic acid in serum and plasma by liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2012, 404, 133–140. [Google Scholar] [CrossRef]
- Fu, X.; Xu, Y.K.; Chan, P.; Pattengale, P.K. Simple, Fast, and Simultaneous Detection of Plasma Total Homocysteine, Methylmalonic Acid, Methionine, and 2-Methylcitric Acid Using Liquid Chromatography and Mass Spectrometry (LC/MS/MS). JIMD Rep. 2013, 10, 69–78. [Google Scholar]
- Hempen, C.; Wanschers, H.; van der Sluijs Veer, G. A fast liquid chromatographic tandem mass spectrometric method for the simultaneous determination of total homocysteine and methylmalonic acid. Anal. Bioanal. Chem. 2008, 391, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Kushnir, M.M.; Nelson, G.J.; Frank, E.L.; Rockwood, A.L. High-Throughput Analysis of Methylmalonic Acid in Serum, Plasma, and Urine by LC-MS/MS. Method for Analyzing Isomers without Chromatographic Separation. Methods Mol. Biol. 2016, 1378, 159–173. [Google Scholar]
- Ambati, C.S.; Yuan, F.; Abu-Elheiga, L.A.; Zhang, Y.; Shetty, V. Identification and Quantitation of Malonic Acid Biomarkers of In-Born Error Metabolism by Targeted Metabolomics. J. Am. Soc. Mass Spectrom 2017, 28, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Zou, Y.; Tang, Y.; Wang, D.; Zhou, W.; Yu, S.; Qiu, L. High-throughput analysis of total homocysteine and methylmalonic acid with the efficiency to separate succinic acid in serum and urine via liquid chromatography tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2022, 1193, 123135. [Google Scholar] [CrossRef] [PubMed]
- Ueyanagi, Y.; Setoyama, D.; Kawakami, D.; Mushimoto, Y.; Matsumoto, S.; Hotta, T.; Kang, D. Fully Automated Quantitative Measurement of Serum Organic Acids via LC-MS/MS for the Diagnosis of Organic Acidemias: Establishment of an Automation System and a Proof-of-Concept Validation. Diagnostics 2021, 11, 2195. [Google Scholar] [CrossRef]
- Boutin, M.; Presse, N.; Martineau, T.; Perreault, A.; Gaudreau, P.; Auray-Blais, C. Mass spectrometry analysis of urinary methylmalonic acid to screen for metabolic vitamin B12 deficiency in older adults. Bioanalysis 2020, 12, 693–705. [Google Scholar]
- Boutin, M.; Presse, N.; Allard, D.; Martineau, T.; Gaudreau, P.; Auray-Blais, C. Methylmalonic acid analysis using urine filter paper samples to screen for metabolic vitamin B12 deficiency in older adults. Bioanalysis 2022, 14, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Bergström, M. Validation of an automated UPLC-MS/MS method for methylmalonic acid in serum/plasma and its application on clinical samples. Scand. J. Clin. Lab Investig. 2022, 82, 342–347. [Google Scholar] [CrossRef]
- CLSI. C-62A: Liquid Chromatography-Mass Spectrometry Methods, Approved Guideline; Linical and Laboratory Standards Institute: Wayne, PA, USA, 2014. [Google Scholar]
- Yu, S.; Wang, D.; Ma, X.; Zhang, Y.; Sun, D.; Zou, Y.; Yu, J.; Zhang, F.; Yang, G.; Xie, S.; et al. Analytical and Clinical Performance of a Liquid Chromatography-Tandem Mass Spectrometry Method for Measuring Gastrin Subtypes G34 and G17 in Serum. Clin. Chem. 2021, 67, 1220–1229. [Google Scholar] [CrossRef]
- Lindberg, M.; Borgstrøm Hager, H.; Brokner, M. Week-to-week biological variation of methylmalonic acid and homocysteine in healthy women. Scand. J. Clin. Lab Investig. 2019, 79, 247–250. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Materials and Method Procedures | Precision, Accuracy, LOD, and LOQ | Method Characteristics | |||
|---|---|---|---|---|---|---|
| LC-MS/MS Platform | Reagents | Sample Preparation | LC-MS/MS Parameters | |||
| Magera et al. (2000) [21] | API 3000 (Perkin-Elmer Sciex) with two Perkin-Elmer Series 200M pumps |
|
|
|
|
|
| Kushnir et al. (2001) [22] | API 2000 (Applied Biosystems/ MDS SCIEX, Foster City, USA) tandem mass spectrometer with a PE series 200 HPLC system (Perkin-Elmer Analytical Instruments) |
|
|
|
|
|
| Schmedes et al. (2006) [23] | Micromass Quattro Micro tandem mass spectrometer with a Waters 2795 Alliance HPLC system |
|
|
|
|
|
| la Marca et al. (2007) [24] | Applied Biosystems/MDS Sciex API 4000™ Triple-Quad Mass Spectrometer equipped with an Agilent 1100 Quaternary Capillary Pump |
|
|
|
|
|
| Blom et al. (2007) [14] | Micromass Quattro LC (Waters) with an Agilent HP1100 HPLC (Amsterdam, the Netherlands) |
|
|
|
|
|
| Lakso et al. (2008) [25] | Agilent1100 LC/MSD |
|
|
|
|
|
| Carvalho et al. (2008) [26] | Waters QuattroMicro tandemmass spectrometerequipped with an atmosphericpressure chemicalionization(APCI) probe and two ShimadzuLC-10ATvp HPLC pumps |
|
|
|
|
|
| Fasching et al. (2010) [27] | Waters Acquity LC-MS/MS System (Waters Corp, Milford, MA) |
|
|
|
|
|
| Pedersen et al. (2011) [28] | Initial work was performed on a Micromass Quattro MicroTM atmospheric pressure ionization (API) triple quadrupole tandem mass spectrometer (Waters Corp), and later, transferred to an API 4000 QTrap (AB SCIEX, Foster City, CA) Acquity ultra-high-performance liquid chromatography (UPLC) unit (Waters Corp.,Milford, MA) |
|
|
|
|
|
| Yuan et al.(2012) [29] | TSQ Quantum Access triple quadrupole mass spectrometer(ThermoFisher Scientific) with a transcend TLX-4 multichannel HPLC system (ThermoFisher Scientific) A Cyclone-MAX TurboFlow column (50 × 0.5 mm, ThermoFisher Scientific) was used for online extraction, and a mixing column (Agilent, Santa Clara, CA, USA) was placedbetween the injector and the TurboFlow column |
|
|
|
|
|
| Fu et al. (2013) [30] | A triple-quadrupole MS/MS system (Applied Biosystem/MDS SCIEX API 4000 Qtrap) was coupled with a Shimadzu HPLC system and a Leap Technologies auto sampler |
|
|
|
|
|
| Hempen et al. (2015) [31] | Shimadzu high-performance LC (HPLC) system coupled to a Q-Trap 3200 mass spectrometer from Applied Biosystems |
|
|
|
|
|
| Kushnir et al. (2016) [32] | Triple quadrupole mass spectrometer AB3200 with TurboVion source (AB Sciex, Foster City, CA) with built-in switchingvalve; binary HPLC pump series 1260 (Agilent Technologies, SantaClara, CA), vacuum degasser, autosampler CTC PAL(Carrboro, NC) equipped with fast wash station |
|
|
|
|
|
| Ambati et al. (2017) [33] | Agilent 6490 triple-quadrupole mass spectrometer (Agilent, Santa Clara, CA, USA) with an Agilent 1290 seriesbinary pump, online degasser, autosampler, and thermostat column compartment (Agilent Technologies, Waldbronn, Germany) |
|
|
|
|
|
| Ma et al. (2022) [34] | A Waters Acquity I-Class UPLC system (Binary Solvent Manager, Thermostatic Column Manager, and FTN Sample Manager) and a Waters TQ-XS triple quadrupole MS/MS system were used which were controlled by MassLynx 4.2 software (Waters, Milford, MA, USA) |
|
|
|
|
|
| Ueyanagi et al. (2022) [35] | LCMSTM-8040 system (Shimadzu Corp., Kyoto, Japan) coupled with CLAM-2030 |
|
|
|
|
|
| Boutin et al. (2022, May) [36,37] | Xevo TQ-S micro (Waters Corporation) tande mmass spectrometer, the UPLC system used was an Acquity I-Class (Waters Corporation) equipped with a flow-through needle injector |
|
|
|
|
|
| Zheng et al. (2022, July) [38] | Xevo TQ-MSmicro mass spectrometer (Waters, Manchester, UK) equipped with a UniSprayTM interface and a Waters Acquity UPLC I-Class Plus system (Waters, Milford, MA) |
|
|
|
|
|
| Jin et al. (method in this study) | 6500 Plus triple quadrupole mass spectrometer (AB Sciex, USA) coupled with an ExionLC™ AD ultra-high-performance liquid chromatography system (Applied Biosystems, CA, USA) |
|
|
|
|
|
| Serum Pools | Mean Recovery ± SD | MMA Imprecision | |||||
|---|---|---|---|---|---|---|---|
| Added, ng/g | Detected, ng/g | Recovery, % | Intra-Assay CV | Inter-Assay CV | Total CV | ||
| Level 1 | 0 | 29.62 ± 1.61 | - | 5.27 | 1.42 | 5.47 | |
| Level 2 | 14.95 | 44.69 ± 1.76 | 101.51 ± 5.74 | 3.09 | 2.69 | 4.10 | |
| Level 3 | 25.36 | 52.94 ± 2.30 | 92.40 ± 3.40 | 3.86 | 2.17 | 4.43 | |
| Level 4 | 37.20 | 68.92 ± 2.16 | 105.95 ± 1.95 | 3.83 | 1.55 | 3.22 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, L.; Liu, Z.; Zhou, W.; Zeng, J.; Wu, M.; Zhang, Y.; Zhang, T.; He, F.; Zhang, C. A Rapid, Simple, Trace, Cost-Effective, and High-Throughput Stable Isotope-Dilution Liquid Chromatography–Tandem Mass Spectrometry Method for Serum Methylmalonic Acid Quantification and Its Clinical Applications. Diagnostics 2022, 12, 2273. https://doi.org/10.3390/diagnostics12102273
Jin L, Liu Z, Zhou W, Zeng J, Wu M, Zhang Y, Zhang T, He F, Zhang C. A Rapid, Simple, Trace, Cost-Effective, and High-Throughput Stable Isotope-Dilution Liquid Chromatography–Tandem Mass Spectrometry Method for Serum Methylmalonic Acid Quantification and Its Clinical Applications. Diagnostics. 2022; 12(10):2273. https://doi.org/10.3390/diagnostics12102273
Chicago/Turabian StyleJin, Lizi, Zhenni Liu, Weiyan Zhou, Jie Zeng, Minhang Wu, Yu Zhang, Tianjiao Zhang, Falin He, and Chuanbao Zhang. 2022. "A Rapid, Simple, Trace, Cost-Effective, and High-Throughput Stable Isotope-Dilution Liquid Chromatography–Tandem Mass Spectrometry Method for Serum Methylmalonic Acid Quantification and Its Clinical Applications" Diagnostics 12, no. 10: 2273. https://doi.org/10.3390/diagnostics12102273
APA StyleJin, L., Liu, Z., Zhou, W., Zeng, J., Wu, M., Zhang, Y., Zhang, T., He, F., & Zhang, C. (2022). A Rapid, Simple, Trace, Cost-Effective, and High-Throughput Stable Isotope-Dilution Liquid Chromatography–Tandem Mass Spectrometry Method for Serum Methylmalonic Acid Quantification and Its Clinical Applications. Diagnostics, 12(10), 2273. https://doi.org/10.3390/diagnostics12102273