
An Overview of Cytomegalovirus Infection in Pregnancy

 , , ,
, , ,  and
and 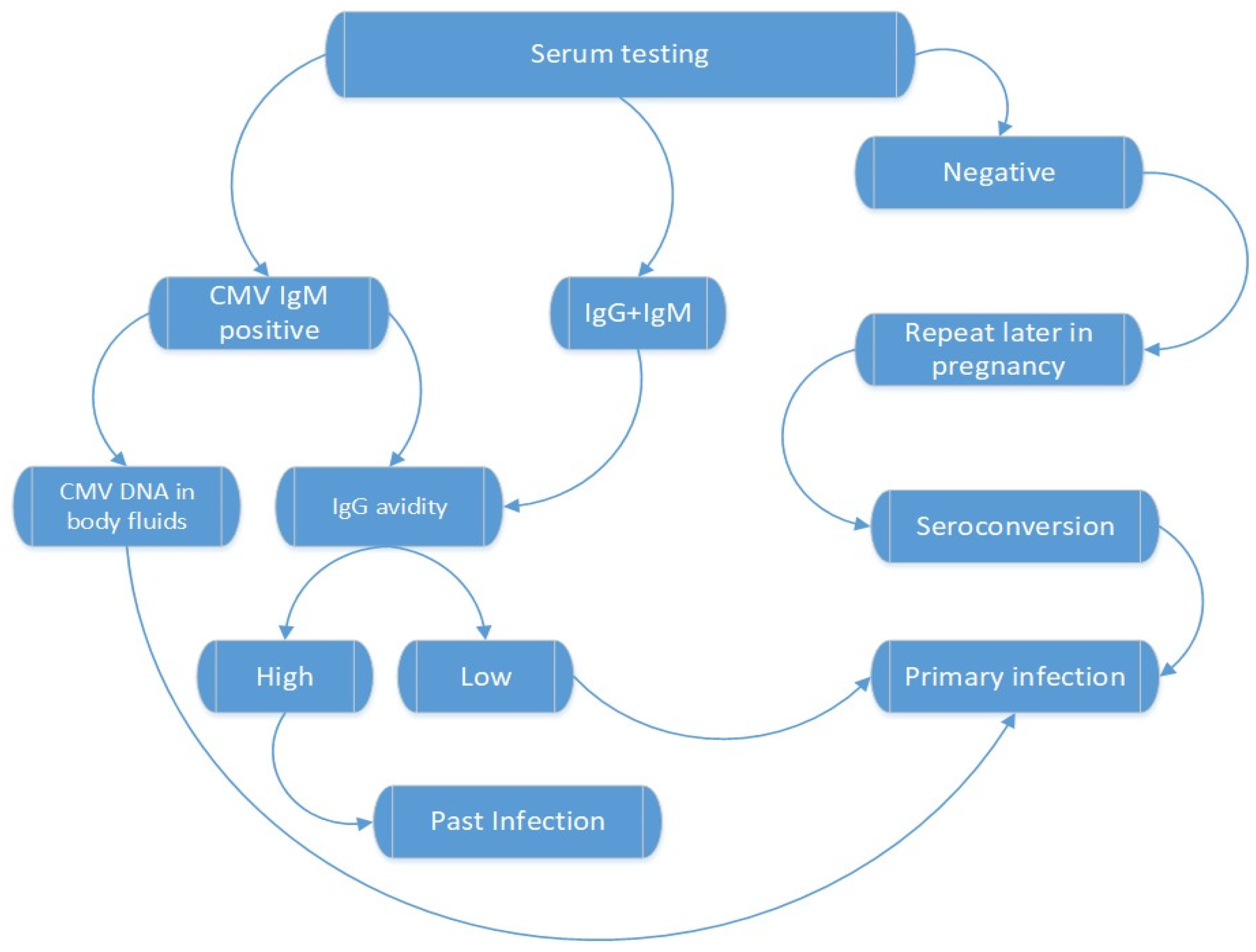{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Background
3.2. Epidemiology
3.3. Clinical Manifestation
3.4. Diagnosis
3.5. Management and Treatment
3.6. CMV Infection in Pregnancy
3.7. Transmission of the Infection
3.8. Diagnosis of Fetal Infection
3.9. Maternal Serum Testing
3.10. CMV Confirmation
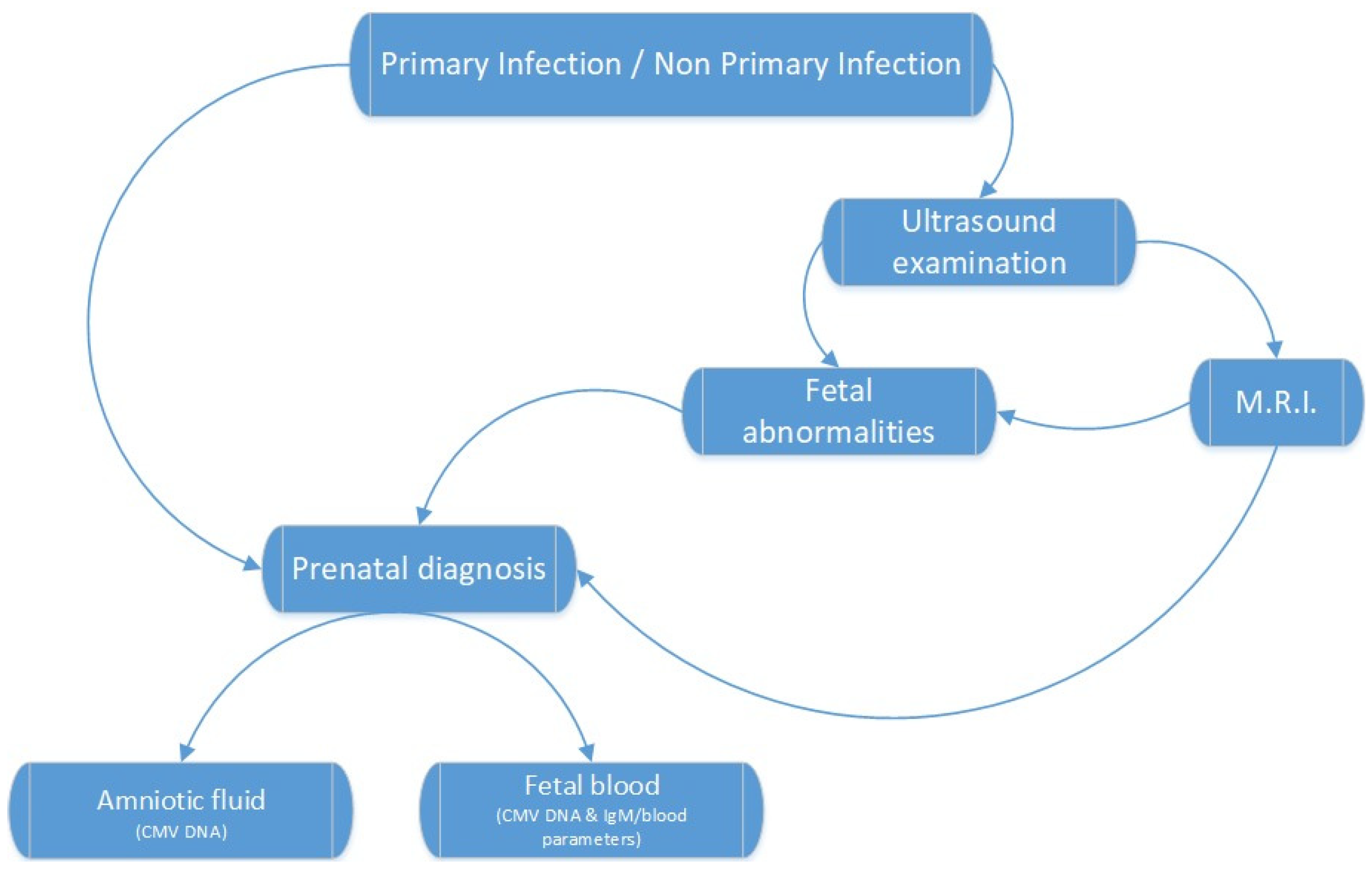
3.11. Fetal Diagnosis
3.12. Amniocentesis and Cordocentesis
3.13. Fetal Imaging Diagnosis
3.14. Prevention and Management of CMV Infection
3.15. Fetal Outcome and Prognosis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, M.; Shorman, M. Cytomegalovirus. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: https://www.ncbi.nlm.nih.gov/books/NBK459185/ (accessed on 5 June 2022).
- Bennett, J.; Dolin, R.; Blaser, M. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 9th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2015. [Google Scholar]
- Pass, R.F.; Arav-Boger, R. Maternal and fetal cytomegalovirus infection: Diagnosis, management, and prevention. F1000Research 2018, 7, 255. [Google Scholar] [CrossRef] [PubMed]
- Saldan, A.; Forner, G.; Mengoli, C.; Gussetti, N.; Palù, G.; Abate, D. Testing for Cytomegalovirus in Pregnancy. J. Clin. Microbiol. 2017, 55, 693–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boucoiran, I.; Yudin, M.; Poliquin, V.; Caddy, S.; Gantt, S.; Castillo, E. Guideline No. 420: Cytomegalovirus Infection in Pregnancy. J. Obstet. Gynaecol. Can. 2021, 43, 893–908. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.H.; Hao, J.D.; Li, W.Y.; Tian, J.; Zhao, J.; Zeng, Y.M.; Dong, G.Q. Congenital cytomegalovirus infection and the risk of hearing loss in childhood: A PRISMA-compliant meta-analysis. Medicine 2021, 100, e27057. [Google Scholar] [CrossRef]
- Kagan, K.O.; Hamprecht, K. Cytomegalovirus infection in pregnancy. Arch Gynecol. Obstet. 2017, 296, 15–26. [Google Scholar] [CrossRef] [PubMed]
- About Cytomegalovirus (CMV). Available online: https://www.cdc.gov/cmv/overview.html (accessed on 12 August 2021).
- Haidar, G.; Boeckh, M.; Singh, N. Cytomegalovirus Infection in Solid Organ and Hematopoietic Cell Transplantation: State of the Evidence. J. Infect. Dis. 2020, 221 (Suppl. 1), S23–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, P.; Reeves, M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat. Rev. Microbiol. 2021, 19, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Acosta, E.; Bowlin, T.; Brooks, J.; Chiang, L.; Hussein, I.; Kimberlin, D.; Kauvar, L.M.; Leavitt, R.; Prichard, M.; Whitley, R. Advances in the Development of Therapeutics for Cytomegalovirus Infections. J. Infect. Dis. 2020, 221 (Suppl. 1), S32–S44. [Google Scholar] [CrossRef] [Green Version]
- Ramchandar, N.; Ding, Y.; Farnaes, L.; Dimmock, D.; Hobbs, C.; Kingsmore, S.F.; Bainbridge, M. Diagnosis of cytomegalovirus infection from clinical whole genome sequencing. Sci. Rep. 2020, 10, 11020. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; de la Camara, R.; Robin, C.; Crocchiolo, R.; Einsele, H.; Hill, J.A.; Hubacek, P.; Navarro, D.; Cordonnier, C.; Ward, K.N.; et al. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect. Dis. 2019, 19, e260–e272. [Google Scholar] [CrossRef]
- Sufiawati, I.; Herrera, R.; Mayer, W.; Cai, X.; Borkakoti, J.; Lin, V.; Rosbe, K.; Tugizov, S.M. Human Immunodeficiency Virus (HIV) and Human Cytomegalovirus (HCMV) Coinfection of Infant Tonsil Epithelium May Synergistically Promote both HIV-1 and HCMV Spread and Infection. J. Virol. 2021, 95, e0092121. [Google Scholar] [CrossRef]
- Chen, K.; Cheng, M.P.; Hammond, S.P.; Einsele, H.; Marty, F.M. Antiviral prophylaxis for cytomegalovirus infection in allogeneic hematopoietic cell transplantation. Blood Adv. 2018, 2, 2159–2175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardiner, B.J.; Herrick, K.W.; Bailey, R.C.; Chow, J.K.; Snydman, D.R. Reactivation of Latent Cytomegalovirus Infection after Major Surgery: Risk Factors and Outcomes. Surg. Infect. 2019, 20, 416–423. [Google Scholar] [CrossRef]
- Meesing, A.; Razonable, R.R. New Developments in the Management of Cytomegalovirus Infection After Transplantation. Drugs 2018, 78, 1085–1103. [Google Scholar] [CrossRef]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef]
- Mocanu, A.G.; Gorun, F.; Ciohat, I.; Navolan, D.; Malita, D.; Vilibic-Cavlek, T.; Dahma, G.; Neamtu, R.; Popescu, D.; Cioca, A.; et al. Simultaneous Seroprevalence to Toxoplasma gondii, Cytomegalovirus and Rubella Virus in Childbearing Women from Western Romania. Medicina 2021, 57, 927. [Google Scholar] [CrossRef] [PubMed]
- Navti, O.B.; Al-Belushi, M.; Konje, J.C.; FRCOG. Cytomegalovirus infection in pregnancy—An update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 216–222. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus infection during pregnancy: State of the science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef]
- Adler, S.P.; Reddehase, M.J. Pediatric roots of cytomegalovirus recurrence and memory inflation in the elderly. Med. Microbiol. Immunol. 2019, 208, 323–328. [Google Scholar] [CrossRef]
- Pesch, M.H.; Saunders, N.A.; Abdelnabi, S. Cytomegalovirus Infection in Pregnancy: Prevention, Presentation, Management and Neonatal Outcomes. J. Midwifery Women’s Health 2021, 66, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Mussi-Pinhata, M.M.; Yamamoto, A.Y. Natural History of Congenital Cytomegalovirus Infection in Highly Seropositive Pop-ulations. J. Infect. Dis. 2020, 221 (Suppl. 1), S15–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaudoin, M.L.; Renaud, C.; Boucher, M.; Kakkar, F.; Gantt, S.; Boucoiran, I. Perspectives of women on screening and prevention of CMV in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 409–413. [Google Scholar] [CrossRef]
- Fitzpatrick, D.; Holmes, N.E.; Hui, L. A systematic review of maternal TORCH serology as a screen for suspected fetal infection. Prenat. Diagn. 2022, 42, 87–96. [Google Scholar] [CrossRef]
- Tanimura, K.; Yamada, H. Maternal and neonatal screening methods for congenital cytomegalovirus infection. J. Obstet. Gynaecol. Res. 2019, 45, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Fowler, K.B.; Boppana, S.B. Congenital cytomegalovirus infection. Semin. Perinatol. 2018, 42, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Karageorgou, I.; Kossyvakis, A.; Jiménez, J.; Garcia, I.; Mentis, A.A. Cytomegalovirus DNA detection in pregnant women with a high IgG avidity index: A valuable tool for diagnosing non-primary infections? J. Matern. Fetal Neonatal Med. 2022, 9, 1–7. [Google Scholar] [CrossRef]
- Maltezou, P.G.; Kourlaba, G.; Kourkouni, Ε.; Luck, S.; Blázquez-Gamero, D.; Ville, Y.; Lilleri, D.; Dimopoulou, D.; Karalexi, M.; Papae-vangelou, V. Maternal type of CMV infection and sequelae in infants with congenital CMV: Systematic review and me-ta-analysis. J. Clin. Virol. 2020, 129, 104518. [Google Scholar] [CrossRef] [PubMed]
- Enders, G.; Daiminger, A.; Bäder, U.; Exler, S.; Schimpf, Y.; Enders, M. The value of CMV IgG avidity and immunoblot for timing the onset of primary CMV infection in pregnancy. J. Clin. Virol. 2013, 56, 102–107. [Google Scholar] [CrossRef]
- Balegamire, S.J.; Renaud, C.; Mâsse, B.; Zinszer, K.; Gantt, S.; Giguere, Y.; Forest, J.-C.; Boucoiran, I. Frequency, timing and risk factors for primary maternal cytomegalovirus infection during pregnancy in Quebec. PLoS ONE 2021, 16, e0252309. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Magny, J.F.; Couderc, S.; Pichon, C.; Parodi, M.; Bussières, L.; Guilleminot, T.; Ghout, I.; Ville, Y. Risk Factors for Congenital Cytomegalovirus Infection Following Primary and Nonprimary Maternal Infection: A Prospective Neonatal Screening Study Using Polymerase Chain Reaction in Saliva. Clin. Infect. Dis. 2017, 65, 398–404. [Google Scholar] [CrossRef]
- Mathias, C.R.; Joung, S.J.S. Diagnostic challenges in congenital cytomegalovirus infection in pregnancy: A case report. Case Rep. Women’s Health 2019, 22, e00119. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R.; Inoue, N.; Pinninti, S.G.; Boppana, S.B.; Lazzarotto, T.; Gabrielli, L.; Simonazzi, G.; Pellett, P.E.; Schmid, D.S. Clinical Diagnostic Testing for Human Cytomegalovirus Infections. J. Infect. Dis. 2020, 221 (Suppl. 1), S74–S85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsico, C.; Kimberlin, D.W. Congenital Cytomegalovirus infection: Advances and challenges in diagnosis, prevention and treatment. Ital. J. Pediatr. 2017, 43, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnouts, L.; Van Mechelen, K.; Laroche, S.; Meuwissen, M.; Boudewyns, A.; Martens, M.; Mahieu, L. Non-primary CMV infection not always innocent. A case-report and literature review. Acta Clin. Belg. 2022, 77, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, K.; Yamada, H. Potential Biomarkers for Predicting Congenital Cytomegalovirus Infection. Int. J. Mol. Sci. 2018, 19, 3760. [Google Scholar] [CrossRef] [Green Version]
- Soper, D.E. Congenital Cytomegalovirus Infection: An Obstetrician’s Point of View. Clin. Infect. Dis. 2013, 57 (Suppl. S4), S171–S173. [Google Scholar] [CrossRef]
- Nagel, A.; Dimitrakopoulou, E.; Teig, N.; Kern, P.; Lücke, T.; Michna, D.; Korn, K.; Steininger, P.; Shahada, K.; Neumann, K.; et al. Characterization of a universal screening approach for congenital CMV infection based on a highly-sensitive, quantitative, multiplex real-time PCR assay. PLoS ONE 2020, 15, e0227143. [Google Scholar] [CrossRef]
- Davis, N.L.; King, C.C.; Kourtis, A.P. Cytomegalovirus infection in pregnancy. Birth Defects Res. 2017, 109, 336–346. [Google Scholar] [CrossRef] [Green Version]
- Lagrou, K.; Bodeus, M.; Van Ranst, M.; Goubau, P. Evaluation of the New Architect Cytomegalovirus Immunoglobulin M (IgM), IgG, and IgG Avidity Assays. J. Clin. Microbiol. 2009, 47, 1695–1699. [Google Scholar] [CrossRef] [Green Version]
- Ebina, Y.; Minematsu, T.; Sonoyama, A.; Morioka, I.; Inoue, N.; Tairaku, S.; Nagamata, S.; Tanimura, K.; Morizane, M.; Deguchi, M.; et al. The IgG avidity value for the prediction of congenital cytomegalovirus infection in a prospective cohort study. J. Périnat. Med. 2014, 42, 755–759. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Ville, Y. Is it time for routine prenatal serological screening for congenital cytomegalovirus? Prenat. Diagn. 2020, 40, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Vorontsov, O.; Levitt, L.; Lilleri, D.; Vainer, G.W.; Kaplan, O.; Schreiber, L.; Arossa, A.; Spinillo, A.; Furione, M.; Alfi, O.; et al. Amniotic fluid biomarkers predict the severity of congenital cytomegalovirus infec-tion. J. Clin. Investig. 2022, 132, e157415. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D. Acute Perinatal Infection and the Evidenced-Based Risk of Intrauterine Diagnostic Testing: A Structured Review. Fetal Diagn. Ther. 2020, 47, 653–664. [Google Scholar] [CrossRef]
- Dinsmoor, M.J.; Fette, L.M.; Hughes, B.L.; Rouse, D.J.; Saade, G.R.; Reddy, U.M.; Allard, D.; Mallett, G.; Thom, E.A.; Gyamfi-Bannerman, C.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units (MFMU) Network. Amniocentesis to diagnose congenital cyto-megalovirus infection following maternal primary infection. Am. J. Obstet. Gynecol. MFM 2022, 4, 100641. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D.; Gagnon, A.; Audibert, F.; Campagnolo, C.; Carroll, J.; Brock, J.-A.; Chong, K.; Johnson, J.-A.; MacDonald, W.; Okun, N.; et al. Prenatal Diagnosis Procedures and Techniques to Obtain a Diagnostic Fetal Specimen or Tissue: Maternal and Fetal Risks and Benefits. J. Obstet. Gynaecol. Can. 2015, 37, 656–668. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Stirnemann, J.; Sellier, Y.; Guilleminot, T.; Dejean, A.; Magney, J.-F.; Couderc, S.; Jacquemard, F.; Ville, Y. Feasibility of predicting the outcome of fetal infection with cytomegalovirus at the time of prenatal diagnosis. Am. J. Obstet. Gynecol. 2016, 215, 342-e1. [Google Scholar] [CrossRef] [Green Version]
- Rouse, D.J.; Fette, L.M.; Hughes, B.L.; Saade, G.R.; Dinsmoor, M.J.; Reddy, U.M.; Pass, R.; Allard, D.; Mallett, G.; Clifton, R.G.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. Noninvasive Prediction of Congenital Cytomegalovirus Infection After Maternal Primary Infection. Obstet. Gynecol. 2022, 139, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Hawkins-Villarreal, A.; Moreno-Espinosa, A.L.; Eixarch, E.; Marcos, M.A.; Martinez-Portilla, R.J.; Salazar, L.; Garcia-Otero, L.; Lopez, M.; Borrell, A.; Figueras, F.; et al. Blood parameters in fetuses infected with cytomegalovirus according to the severity of brain damage and trimester of pregnancy at cordocentesis. J. Clin. Virol. 2019, 119, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Faure-Bardon, V.; Millischer, A.E.; Deloison, B.; Sonigo, P.; Grévent, D.; Salomon, L.; Stirnemann, J.; Nicloux, M.; Magny, J.F.; Leruez-Ville, M.; et al. Refining the prognosis of fetuses infected with Cytomegalovirus in the first trimester of preg-nancy by serial prenatal assessment: A single-centre retrospective study. BJOG 2020, 127, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Komvilaisak, P.; Komvilaisak, R.; Jetsrisuparb, A.; Wiangnon, S.; Jirapradittha, J.; Kiatchoosakun, P.; Fucharoen, G. Fetal Anemia Causing Hydrops Fetalis From an Alpha-Globin Variant: Homozygous Hemoglobin Constant Spring. J. Pediatr. Hematol. Oncol. 2018, 40, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Zavattoni, M.; Rustico, M.; Tassis, B.; Lombardi, G.; Furione, M.; Piralla, A.; Baldanti, F. Risk of congenital disease in 46 infected fetuses according to gestational age of primary human cytomegalovirus infection in the mother. J. Med. Virol. 2016, 88, 120–126. [Google Scholar] [CrossRef]
- van der Knoop, B.J.; Zonnenberg, I.A.; Verbeke, J.I.M.L.; de Vries, L.S.; Pistorius, L.R.; van Weissenbruch, M.M.; Vermeulen, R.J.; de Vries, J.I.P. Additional value of advanced neurosonography and magnetic resonance imaging in fetuses at risk for brain damage. Ultrasound Obstet. Gynecol. 2020, 56, 348–358. [Google Scholar] [CrossRef] [Green Version]
- Khalil, A.; Sotiriadis, A.; Chaoui, R.; da Silva Costa, F.; D’Antonio, F.; Heath, P.T.; Jones, C.; Malinger, G.; Odibo, A.; Prefumo, F.; et al. ISUOG Practice Guidelines: Role of ultrasound in congenital infection. Ultrasound Obstet Gynecol. 2020, 56, 128–151. [Google Scholar] [CrossRef] [PubMed]
- Diogo, M.C.; Glatter, S.; Binder, J.; Kiss, H.; Prayer, D. The MRI spectrum of congenital cytomegalovirus infection. Prenat. Diagn. 2020, 40, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Imafuku, H.; Yamada, H.; Uchida, A.; Deguchi, M.; Shirakawa, T.; Sasagawa, Y.; Shi, Y.; Fujioka, K.; Morioka, I.; Tanimura, K. Clinical and ultrasound features associated with congenital cytomegalovirus infection as potential predictors for targeted newborn screening in high-risk pregnancies. Sci. Rep. 2020, 10, 19706. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, K.; Uchida, A.; Imafuku, H.; Tairaku, S.; Fujioka, K.; Morioka, I.; Yamada, H. The Current Challenges in Developing Biological and Clinical Predictors of Congenital Cytomegalovirus Infection. Int. J. Mol. Sci. 2021, 22, 13487. [Google Scholar] [CrossRef]
- Fumagalli, M.; Parodi, A.; Ramenghi, L.; Limperopoulos, C.; Steggerda, S.; Agut, T.; eurUS.brain group. Ultrasound of acquired posterior fossa abnormalities in the newborn. Pediatr. Res. 2020, 87 (Suppl. 1), 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, H.S.; Kwak, D.W.; Oh, S.-Y.; Choi, S.K.; Hong, J.S.; Hwang, H.S.; Park, H.S.; Seol, H.-J.; Kim, M.Y.; Kim, S.J.; et al. Clinical significance of soft markers in second trimester ultrasonography for pregnant Korean women: A multicenter study and literature review. Obstet. Gynecol. Sci. 2022, 65, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Blázquez-Gamero, D.; Soriano-Ramos, M.; Martínez de Aragón, A.; Baquero-Artigao, F.; Frick, M.A.; Noguera-Julian, A.; Alonso-Ojembarrena, A.; Moliner Calderón, E.; Rives Ferreiro, M.T.; Filgueira Posse, A.; et al. Role of Magnetic Resonance Imaging and Cranial Ul-trasonography in Congenital Cytomegalovirus Infection. Pediatr. Infect. Dis. J. 2019, 38, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Keymeulen, A.; De Leenheer, E.; Casaer, A.; Cossey, V.; Herregods, N.; Laroche, S.; Mahieu, L.; Van Mol, C.; Vanhaesebrouck, S.; Walle, C.V.; et al. Cranial ultrasound and MRI: Complementary or not in the diagnostic assessment of children with con-genital CMV infection? Eur. J. Pediatr. 2022, 181, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Hawkins-Villarreal, A.; Moreno-Espinosa, A.L.; Martinez-Portilla, R.J.; Castillo, K.; Hahner, N.; Nakaki, A.; Trigo, L.; Picone, O.; Siauve, N.; Figueras, F.; et al. Fetal Liver Volume Assessment Using Magnetic Resonance Imaging in Fetuses with Cytomegalovirus Infection. Front. Med. 2022, 9, 889976. [Google Scholar] [CrossRef]
- Gabrielli, L.; Bonasoni, M.P.; Chiereghin, A.; Piccirilli, G.; Borgatti, E.C.; Simonazzi, G.; Salfi, N.C.M.; Tamagnini, I.; Lazzarotto, T. Pathophysiology of Hyperechogenic Bowel in Congenitally Human Cytomegalovirus Infected Fetuses. Microorganisms 2020, 8, 779. [Google Scholar] [CrossRef] [PubMed]
- Prodan, N.; Sonek, J.; Wagner, P.; Hoopmann, M.; Abele, H.; Hamprecht, K.; Kagan, K.O. Splenic artery blood flow as a potential marker for materno-fetal transmission of a primary CMV infection. Arch. Gynecol. Obstet. 2019, 299, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Uenaka, M.; Morizane, M.; Tanimura, K.; Deguchi, M.; Kanzawa, M.; Itoh, T.; Yamada, H. Histopathological analysis of placentas with congenital cytomegalovirus infection. Placenta 2019, 75, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Pereira, L.; Tabata, T.; Petitt, M.; Fang-Hoover, J. Congenital cytomegalovirus infection undermines early development and functions of the human placenta. Placenta 2017, 59 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef] [PubMed]
- Tsuge, M.; Hida, A.I.; Minematsu, T.; Honda, N.; Oshiro, Y.; Yokoyama, M.; Kondo, Y. Prospective Cohort Study of Congenital Cytomegalovirus Infection during Pregnancy with Fetal Growth Restriction: Serologic Analysis and Placental Pathology. J. Pediatr. 2019, 206, 42–48. [Google Scholar] [CrossRef]
- Yefet, E.; Ben Shmuel, M.D.Y.; Nachum, Z. The association between polyhydramnios and CMV infection-retrospective cohort study. J. Matern. Neonatal Med. 2021, 34, 3716–3722. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-Y.; Fang, F. Congenital human cytomegalovirus infection and neurologic diseases in newborns. Chin. Med. J. 2019, 132, 2109–2118. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine (SMFM); Hughes, B.L.; Gyamfi-Bannerman, C. Diagnosis and antenatal management of congenital cytomegalovirus infection. Am. J. Obstet. Gynecol. 2016, 214, B5–B11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, T.; Sueda, Y.; Okada, K.; Kitaura, T.; Yamaguchi, K.; Makino, H.; Naka-moto, M.; Chikumi, H.; Yamasaki, A. Splenic Infarction in Acute Cytomegalovirus and Human Parvovirus Concomitant Infection. Case Rep. Infect. Dis. 2018, 2018, 7027656. [Google Scholar] [CrossRef]
- Britt, W.J. Maternal Immunity and the Natural History of Congenital Human Cytomegalovirus Infection. Viruses 2018, 10, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleiss, M.R.; Permar, S.R.; Plotkin, S.A. Progress toward Development of a Vaccine against Congenital Cytomegalovirus In-fection. Clin. Vaccine Immunol. 2017, 24, e00268–e00317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotkin, S.A.; Wang, D.; Oualim, A.; Diamond, D.J.; Kotton, C.N.; Mossman, S.; Carfi, A.; Anderson, D.; Dormitzer, P.R. The Status of Vaccine Development Against the Human Cytomegalovirus. J. Infect. Dis. 2020, 221 (Suppl. 1), S113–S122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerna, G.; Lilleri, D. Human Cytomegalovirus Congenital (cCMV) Infection Following Primary and Nonprimary Maternal Infection: Perspectives of Prevention through Vaccine Development. Vaccines 2020, 8, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demmler-Harrison, G.J.; Miller, J.A.; Houston Congenital Cytomegalovirus Longitudinal Study Group. Maternal cytomegal-ovirus immune status and hearing loss outcomes in congenital cytomegalovirus-infected offspring. PLoS ONE 2020, 15, e0240172. [Google Scholar] [CrossRef]
- Jenks, C.M.; Hoff, S.R.; Mithal, L.B. Congenital Cytomegalovirus Infection: Epidemiology, Timely Diagnosis, and Management. Neoreviews 2021, 22, e606–e613. [Google Scholar] [CrossRef]
- Blázquez-Gamero, D.; Izquierdo, A.G.; del Rosal, T.; Baquero-Artigao, F.; Méndez, N.I.; Soriano-Ramos, M.; Conejo, P.R.; González-Tomé, M.I.; García-Burguillo, A.; Pérez, N.P.; et al. Prevention and treatment of fetal cytomegalovirus infection with cytomegalovirus hyperimmune globulin: A multicenter study in Madrid. J. Matern. Neonatal Med. 2019, 32, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Struble, E.B.; Murata, H.; Komatsu, T.; Scott, D. Immune Prophylaxis and Therapy for Human Cytomegalovirus Infection. Int. J. Mol. Sci. 2021, 22, 8728. [Google Scholar] [CrossRef]
- Tol, I.; Heath, P.T.; Khalil, A. Prevention strategies for congenital cytomegalovirus infection. Curr. Opin. Infect. Dis. 2021, 34, 546–551. [Google Scholar] [CrossRef]
- Thigpen, J. Congenital Cytomegalovirus-History, Current Practice, and Future Opportunities. Neonatal Netw. 2020, 39, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.L.; Clifton, R.G.; Rouse, D.J.; Saade, G.R.; Dinsmoor, M.J.; Reddy, U.M.; Pass, R.; Allard, D.; Mallett, G.; Fette, L.M.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. A Trial of Hyperimmune Globulin to Prevent Congenital Cytomegalovirus Infection. N. Engl. J. Med. 2021, 385, 436–444. [Google Scholar] [CrossRef]
- Nigro, G. Hyperimmune globulin in pregnancy for the prevention of congenital cytomegalovirus disease. Expert Rev. Anti-Infect. Ther. 2017, 15, 977–986. [Google Scholar] [CrossRef]
- Ross, S.A.; Kimberlin, D. Clinical outcome and the role of antivirals in congenital cytomegalovirus infection. Antivir. Res. 2021, 191, 105083. [Google Scholar] [CrossRef]
- Zammarchi, L.; Lazzarotto, T.; Andreoni, M.; Campolmi, I.; Pasquini, L.; Di Tommaso, M.; Simonazzi, G.; Tomasoni, L.R.; Castelli, F.; Galli, L.; et al. Management of cytomegalovirus infection in pregnancy: Is it time for valacyclovir? Clin. Microbiol. Infect. 2020, 26, 1151–1154. [Google Scholar] [CrossRef]
- Chiopris, G.; Veronese, P.; Cusenza, F.; Procaccianti, M.; Perrone, S.; Daccò, V.; Colombo, C.; Esposito, S. Congenital Cytomegalo-virus Infection: Update on Diagnosis and Treatment. Microorganisms 2020, 8, 1516. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, A.R.; Gordevicius, J.; Paul, E.N.; Houck, C.; George, S.; Galvis, M.L.E.; Sha, Q.; Brundin, P.; Pospisilik, J.A.; Racicot, K.; et al. Maternal Herpesviridae infection during pregnancy alters midbrain dopaminergic signatures in adult offspring. Neurobiol. Dis. 2022, 169, 105720. [Google Scholar] [CrossRef] [PubMed]
- Andronaco, D.W. Congenital Cytomegalovirus and Hearing Loss. J. Obstet. Gynecol. Neonatal Nurs. 2020, 49, 293–304. [Google Scholar] [CrossRef]
- Xia, W.; Yan, H.; Zhang, Y.; Wang, C.; Gao, W.; Lv, C.; Wang, W.; Liu, Z. Congenital Human Cytomegalovirus Infection Inducing Sensorineural Hearing Loss. Front. Microbiol. 2021, 12, 649690. [Google Scholar] [CrossRef] [PubMed]
- Auriti, C.; De Rose, D.U.; Santisi, A.; Martini, L.; Piersigilli, F.; Bersani, I.; Ronchetti, M.P.; Caforio, L. Pregnancy and viral infections: Mechanisms of fetal damage, diagnosis and prevention of neonatal adverse outcomes from cytomegalovirus to SARS-CoV-2 and Zika virus. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166198. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef]
- Ronchi, A.; Zeray, F.; Lee, L.E.; Owen, K.E.; Shoup, A.G.; Garcia, F.; Vazquez, L.N.; Cantey, J.B.; Varghese, S.; Pugni, L.; et al. Evaluation of clinically asymptomatic high risk infants with congenital cytomegalovirus infection. J. Perinatol. 2020, 40, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Buca, D.; Di Mascio, D.; Rizzo, G.; Giancotti, A.; D’Amico, A.; Leombroni, M.; Makatsarya, A.; Familiari, A.; Liberati, M.; Nappi, L.; et al. Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Cadena-Mota, S.; Muñoz-Escalante, J.C.; Martínez-Rodríguez, L.E.; Bernal-Silva, S.; Tello-Martínez, N.; Torre-Rodríguez, I.; Hernández-Sánchez, P.G.; Castillo-Martínez, F.; Escalante-Padrón, F.; Lima-Rogel, V.; et al. Incidence of congenital and postnatal cytomegalovirus infection during the first year of life in Mexican preterm infants. J. Med. Virol. 2022, 94, 3349–3358. [Google Scholar] [CrossRef]
- Jin, H.D.; Demmler-Harrison, G.J.; Coats, D.K.; Paysse, E.A.; Bhatt, A.; Edmond, J.C.; Yen, K.G.; Steinkuller, P.; Miller, J.; Congenital CMV Longitudinal Study Group. Long-term Visual and Ocular Sequelae in Patients with Congenital Cytomegalovirus Infection. Pediatr. Infect. Dis. J. 2017, 36, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.D.; Demmler-Harrison, G.J.; Miller, J.; Edmond, J.C.; Coats, D.K.; Paysse, E.A.; Bhatt, A.R.; Yen, K.G.; Klingen, J.T.; Steinkuller, P.; et al. Cortical Visual Impairment in Congenital Cytomegalovirus Infection. J. Pediatr. Ophthalmol. Strabismus 2019, 56, 194–202. [Google Scholar] [CrossRef]
- Divya, D.V.; Prasad, M.G.S.; Radhakrishna, A.N.; Reddy, S.P.; Pratyusha, K.; Kumar, K.V.K.S.; Sandeep, R.V. The Serological Evidence of Cytomegalovirus Infection as a Potent Aetiological Factor for Cleft Lip/Palate, Mental Retardation and Deafness. J. Clin. Diagn Res. 2017, 11, ZC51–ZC54. [Google Scholar] [CrossRef]
- Teissier, N.; Bernard, S.; Quesnel, S.; Van Den Abbeele, T. Audiovestibular consequences of congenital cytomegalovirus infection. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 413–418. [Google Scholar] [CrossRef]
- Sebghati, M.; Khalil, A. New evidence on prognostic features, prevention and treatment of congenital Cytomegalovirus infection. Curr. Opin. Obstet. Gynecol. 2020, 32, 342–350. [Google Scholar] [CrossRef]
- Kimberlin, D.W.; Lin, C.Y.; Sanchez, P.J.; Demmler, G.J.; Dankner, W.; Shelton, M.; Jacobs, R.F.; Vaudry, W.; Pass, R.F.; Kiell, J.M.; et al. Effect of ganciclovir therapy on hearing in symptomatic congenital cytomegalovirus disease involving the central nervous system: A randomized, controlled trial. J. Pediatr. 2003, 143, 16–25. [Google Scholar] [CrossRef]
- Hernandez-Alvarado, N.; Shanley, R.; Schleiss, M.R.; Ericksen, J.; Wassenaar, J.; Webo, L.; Bodin, K.; Parsons, K.; Osterholm, E.A. Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting. Viruses 2021, 13, 1897. [Google Scholar] [CrossRef]
- Minihan, L.; Lee Oei, J.; Bajuk, B.; Palasanthiran, P. Postnatal Cytomegalovirus Infection: Is it Important? A 10-Year Retrospec-tive Case-control Study of Characteristics and Outcomes in Very Preterm and Very Low Birth Weight Infants. Pediatr. Infect. Dis. J. 2022, 41, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Mehedintu, C.; Isopescu, F.; Ionescu, O.-M.; Petca, A.; Bratila, E.; Cirstoiu, M.M.; Carp-Veliscu, A.; Frincu, F. Diagnostic Pitfall in Atypical Febrile Presentation in a Patient with a Pregnancy-Specific Dermatosis—Case Report and Literature Review. Medicina 2022, 58, 847. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plotogea, M.; Isam, A.J.; Frincu, F.; Zgura, A.; Bacinschi, X.; Sandru, F.; Duta, S.; Petca, R.C.; Edu, A. An Overview of Cytomegalovirus Infection in Pregnancy. Diagnostics 2022, 12, 2429. https://doi.org/10.3390/diagnostics12102429
Plotogea M, Isam AJ, Frincu F, Zgura A, Bacinschi X, Sandru F, Duta S, Petca RC, Edu A. An Overview of Cytomegalovirus Infection in Pregnancy. Diagnostics. 2022; 12(10):2429. https://doi.org/10.3390/diagnostics12102429
Chicago/Turabian StylePlotogea, Mihaela, Al Jashi Isam, Francesca Frincu, Anca Zgura, Xenia Bacinschi, Florica Sandru, Simona Duta, Razvan Cosmin Petca, and Antoine Edu. 2022. "An Overview of Cytomegalovirus Infection in Pregnancy" Diagnostics 12, no. 10: 2429. https://doi.org/10.3390/diagnostics12102429
APA StylePlotogea, M., Isam, A. J., Frincu, F., Zgura, A., Bacinschi, X., Sandru, F., Duta, S., Petca, R. C., & Edu, A. (2022). An Overview of Cytomegalovirus Infection in Pregnancy. Diagnostics, 12(10), 2429. https://doi.org/10.3390/diagnostics12102429