


Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients—A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
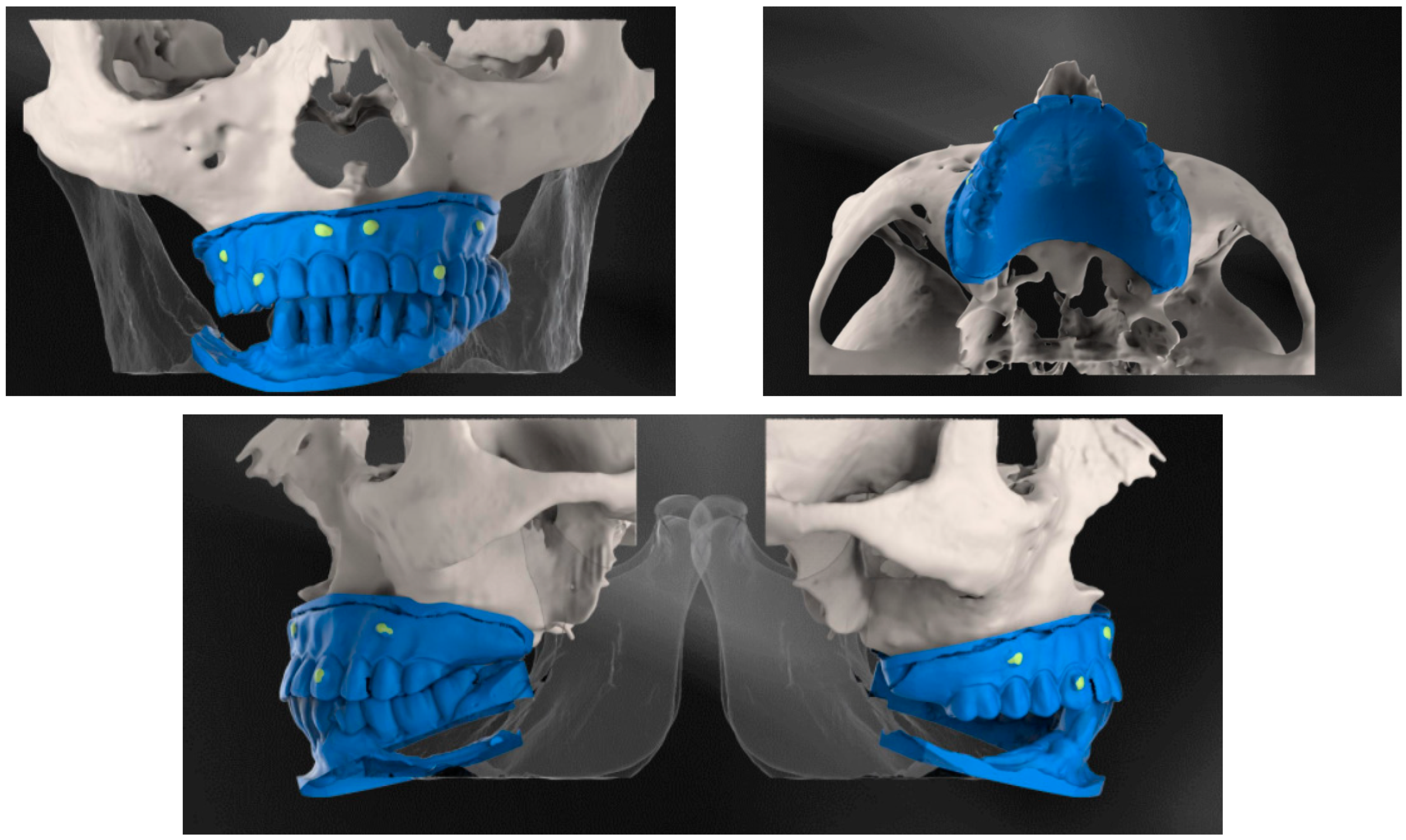
2.2. Preoperative and CBCT
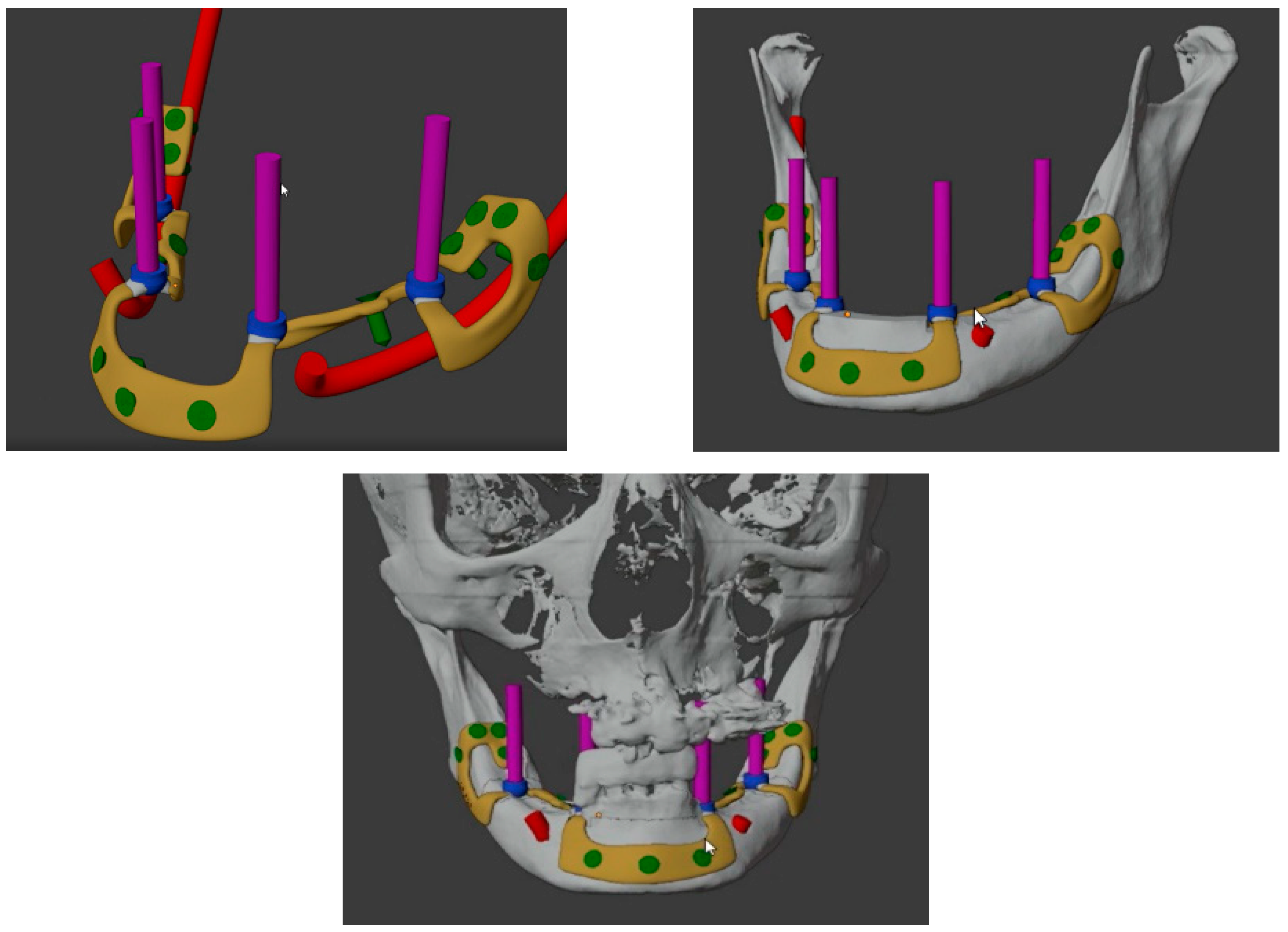
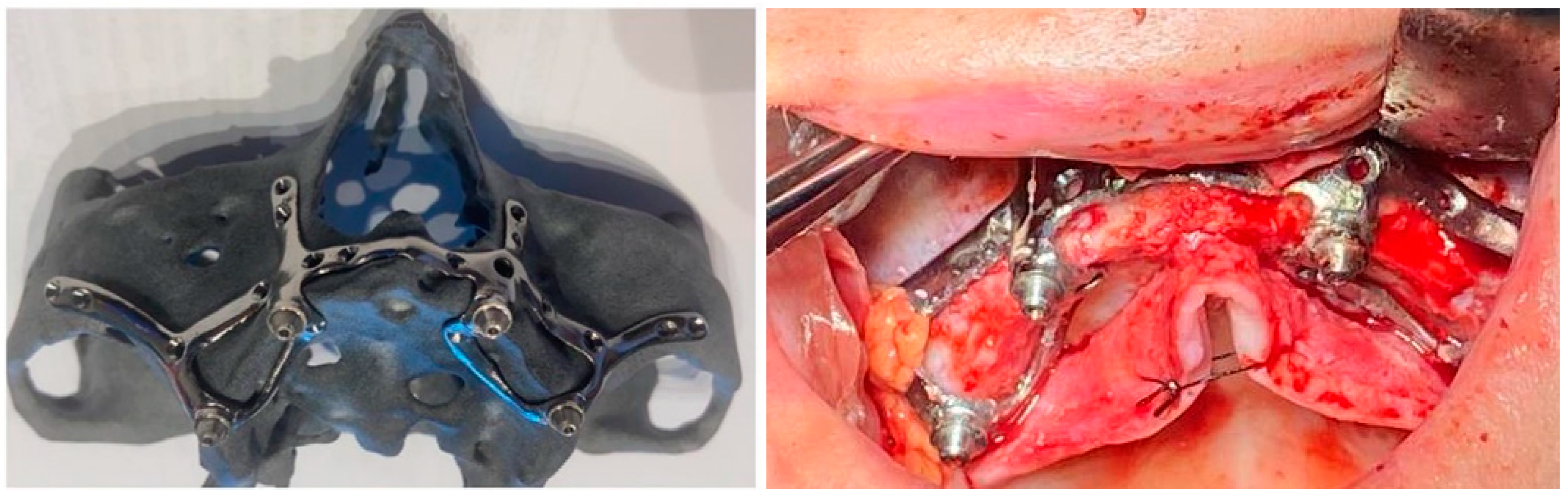
2.3. Design and Fabrication of the Custom-Made Subperiosteal Implants
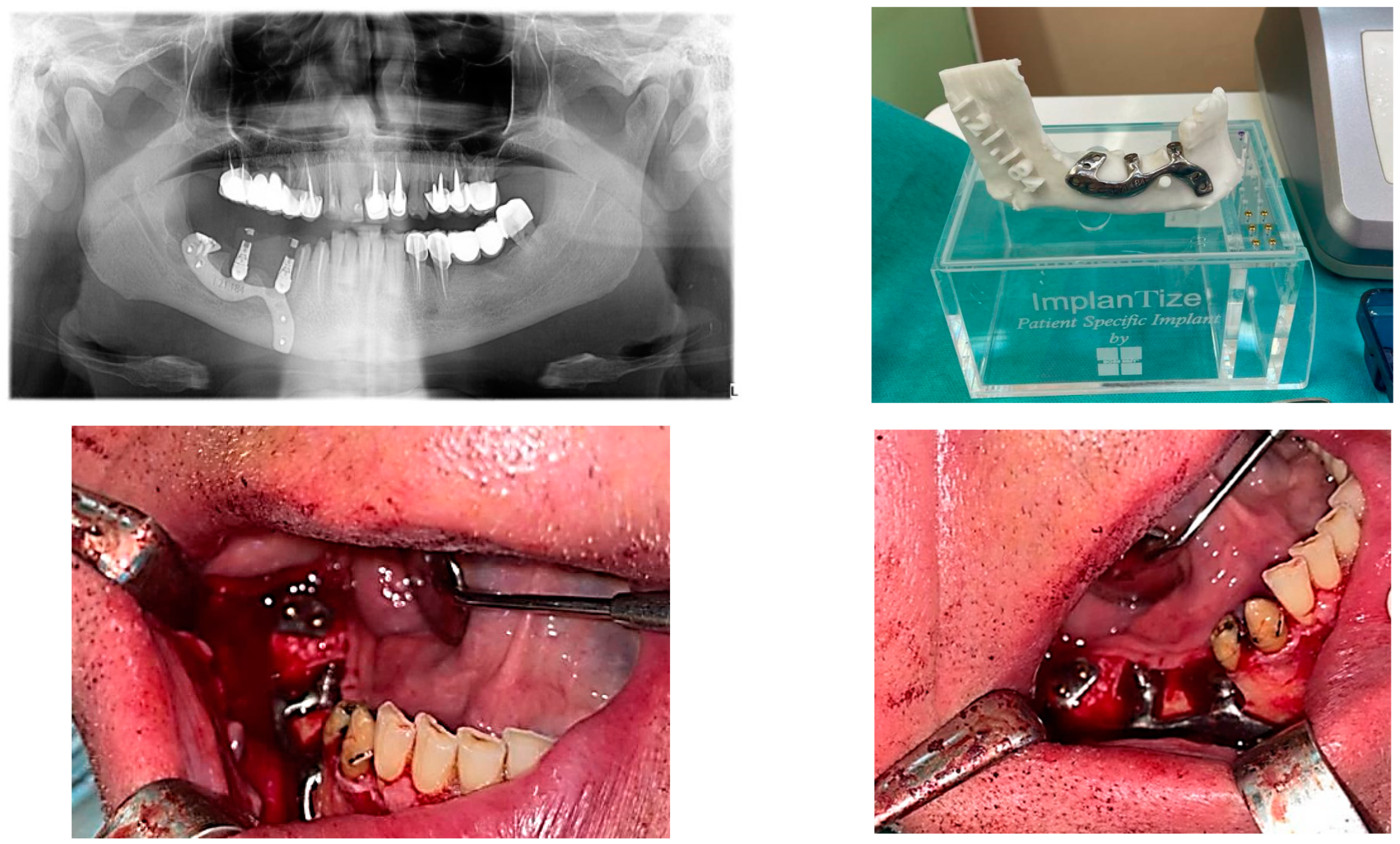
2.4. Surgical and Prosthetic Procedure
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mangano, C.; Mangano, F.; Shibli, J.A.; Ricci, M.; Sammons, R.L.; Figliuzzi, M. Morse taper connection implants supporting “planned” maxillary and mandibular bar-retained overdentures: A 5-year prospective multicenter study. Clin. Oral Implant. Res. 2011, 22, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Müller, F.; On behalf of the Roxolid Study Group; Al-Nawas, B.; Storelli, S.; Quirynen, M.; Hicklin, S.; Castro-Laza, J.; Bassetti, R.; Schimmel, M. Small-diameter titanium grade IV and titanium-zirconium implants in edentulous mandibles: Five-year results from a double-blind, randomized controlled trial. BMC Oral Health 2015, 15, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, C.; Iaculli, F.; Piattelli, A.; Mangano, F. Fixed restorations supported by Morse-taper connection implants: A retrospective clinical study with 10–20 years of follow-up. Clin. Oral Implant. Res. 2015, 26, 1229–1236. [Google Scholar] [CrossRef]
- Esposito, M.; Ardebili, Y.; Worthington, H.V. Interventions for replacing missing teeth: Different types of dental implants. Cochrane Database Syst. Rev. 2014, 7, CD003815. [Google Scholar] [CrossRef] [PubMed]
- Rocchietta, I.; Fontana, F.; Simion, M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: A systematic review. J. Clin. Periodontol. 2008, 35, 203–215. [Google Scholar] [CrossRef]
- Aloy-Prósper, A.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: A systematic review. Med. Oral Patol. Oral Y Cir. Buccal 2015, 20, e251–e258. [Google Scholar] [CrossRef]
- Felice, P.; Marchetti, C.; Iezzi, G.; Piattelli, A.; Worthington, H.; Pellegrino, G.; Esposito, M. Vertical ridge augmentation of the atrophic posterior mandible with interpositional bloc grafts: Bone from the iliac crest vs. bovine anorganic bone. Clinical and histological results up to one year after loading from a randomized-controlled clinical trial. Clin. Oral Implant. Res. 2009, 20, 1386–1393. [Google Scholar] [CrossRef]
- Schneider, D.; Weber, F.E.; Grunder, U.; Andreoni, C.; Burkhardt, R.; Jung, R.E. A randomized controlled clinical multicenter trial comparing the clinical and histological performance of a new, modified polylactide-co-glycolide acid membrane to an expanded polytetrafluorethylene membrane in guided bone regeneration procedures. Clin. Oral Implant. Res. 2014, 25, 150–158. [Google Scholar] [CrossRef]
- Anitua, E.; Begoña, L.; Orive, G. Clinical evaluation of split-crest technique with ultrasonic bone surgery for narrow ridge expansion: Status of soft and hard tissues and implant success. Clin. Implant Dent. Relat. Res. 2013, 15, 176–187. [Google Scholar] [CrossRef]
- Baas, E.M.; van Gemert, B.P.; Bierenbroodspot, F.; Milstein, D.M.; de Lange, J. Patient discomfort and other side effects after bilateral sagittal split osteotomy or distraction osteogenesis of the mandible: A randomized clinical trial. Int. J. Oral Maxillofac. Surg. 2015, 44, 1119–1124. [Google Scholar] [CrossRef]
- Mangano, C.; Hamis, S.; Perrotti, V.; Shibli, J.A.; Mangano, F.; Ricci, L.; Piattelli, A.; Iezzi, G. Maxillary sinus grafting with biphasic calcium phosphate ceramics: Clinical and histologic evaluation in man. Int. J. Oral Maxillofac. Implant. 2013, 28, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Mangano, C.; Sinjari, B.; Shibli, J.A.; Mangano, F.; Hamisch, S.; Piattelli, A.; Iezzi, G. A Human Clinical, Histological, Histomorphometrical, and Radiographical Study on Biphasic HA-Beta-TCP 30/70 in Maxillary Sinus Augmentation. Clin. Implant Dent. Relat. Res. 2015, 17, 610–618. [Google Scholar] [CrossRef]
- Linkow, L.I.; Wagner, J.R.; Chanavaz, M. Tripodal mandibular subperiosteal implant: Basic sciences, operational procedures, and clinical data. J. Oral Implantol. 1998, 24, 16–36. [Google Scholar] [CrossRef]
- Linkow, L.I.; Ghalili, R. Ramus hinges for excessive movements of the condyles: A new dimension in mandibular tripodal subperiosteal implants. J. Oral Implantol. 1999, 25, 11–17. [Google Scholar] [CrossRef]
- Linkow, L.I. Use of a tripodal mandibular subperiosteal implant with ramus hinges for facial asymmetry. J. Oral Implantol. 2000, 26, 120–123. [Google Scholar] [CrossRef]
- Silvestri, K.D.; Carlotti, A.E. Subperiosteal implant: Serving the dental profession for over 50 years. Rhode Isl. Dent. J. 1995, 28, 11–23. [Google Scholar]
- Kurtzman, G.M.; Schwartz, K. The subperiosteal implant as a viable long-term treatment modality in the severely atrophied mandible: A patient’s 40-year case history. J. Oral Implantol. 1995, 21, 35–39. [Google Scholar] [PubMed]
- Bodine, R.L.; Yanase, R.T.; Bodine, A. Forty years of experience with subperiosteal implant dentures in 41 edentulous patients. J. Prosthet. Dent. 1996, 75, 33–44. [Google Scholar] [CrossRef]
- Moore, D.J.; Hansen, P.A. A descriptive 18-year retrospective review of subperiosteal implants for patients with severely atrophied edentulous mandibles. J. Prosthet. Dent. 2004, 92, 145–150. [Google Scholar] [CrossRef]
- Weiss, C.M.; Reynolds, T. A collective conference on the utilization of subperiosteal implants in implant dentistry. J. Oral Implantol. 2000, 26, 127–128. [Google Scholar] [CrossRef]
- Schou, S.; Pallesen, L.; Hjørting-Hansen, E.; Pedersen, C.S.; Fibaek, B. A 41-year history of a mandibular subperiosteal implant. Clin. Oral Implant. Res. 2000, 11, 171–178. [Google Scholar] [CrossRef]
- van Steenberghe, D.; Brånemark, P.I.; Quirynen, M.; De Mars, G.; Naert, I. The rehabilitation of oral defects by osseointegrated implants. J. Clin. Periodontol. 1991, 18, 488–493. [Google Scholar] [CrossRef]
- van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef]
- Antohi, C.; Salceanu, M.; Aminov, L.; Martu, M.-A.; Dascalu, C.G.; Dodi, G.; Stoica, G.; Bandol, G.; Iancu, D.; Dobrovat, B.; et al. Assessment of Systemic and Maxillary Bone Loss in Cancer Patients with Endo-Periodontal Lesions Using Dkk-1 Biomarker and Dental Radiological Examinations. Appl. Sci. 2022, 12, 5235. [Google Scholar] [CrossRef]
- Dumitrescu, A.; Martu, M.-A.; Nemtoi, A.; Sirghe, A.; Chelaru, L.; Tatarciuc, D.; Dumitrescu, A.-M.; Haba, D. Association between Cone-Beam Computed Tomography and Histological and Immunohistochemical Features in Periapical Lesions Correlated with Thickened Maxillary Sinus Mucosa. Medicina 2021, 57, 840. [Google Scholar] [CrossRef]
- Martu, C.; Martu, M.-A.; Maftei, G.-A.; Diaconu-Popa, D.A.; Radulescu, L. Odontogenic Sinusitis: From Diagnosis to Treatment Possibilities—A Narrative Review of Recent Data. Diagnostics 2022, 12, 1600. [Google Scholar] [CrossRef] [PubMed]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Sonmez, N.; Gultekin, P.; Turp, V.; Akgungor, G.; Sen, D.; Mijiritsky, E. Evaluation of five CAD/CAM materials by microstructural characterization and mechanical tests: A comparative in vitro study. BMC Oral Health 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.; Chambrone, L.; Van Noort, R.; Miller, C.; Hatton, P.; Mangano, C. Direct metal laser sintering titanium dental implants: A review of the current literature. Int. J. Biomater. 2014, 2014, 461534. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Giavatto Ma Giannatiempo, J.; Lizio, G.; Corinaldesi, G. Custom-Made Titanium Mesh for Maxillary Bone Augmentation With Immediate Implants and Delayed Loading. J. Oral. Implantol. 2019, 45, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Connors, C.A.; Liacouras, P.C.; Grant, G.T. Custom Titanium Ridge Augmentation Matrix (CTRAM): A Case Report. Int. J. Periodontics Restor. Dent. 2016, 36, 707–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.G.; De Franco, M.; Caprioglio, A.; Macchi, A.; Piattelli, A.; Mangano, C. Immediate, non-submerged, root-analogue direct laser metal sintering (DLMS) implants: A 1-year prospective study on 15 patients. Lasers Med. Sci. 2014, 29, 1321–1328. [Google Scholar] [CrossRef]
- Mangano, F.; Bazzoli, M.; Tettamanti, L.; Farronato, D.; Maineri, M.; Macchi, A.; Mangano, C. Custom-made, selective laser sintering (SLS) blade implants as a non-conventional solution for the prosthetic rehabilitation of extremely atrophied posterior mandible. Lasers Med. Sci. 2013, 28, 1241–1247. [Google Scholar] [CrossRef]
- Maftei, G.-A.; Martu, M.-A.; Martu, M.-C.; Popescu, D.; Surlin, P.; Tatarciuc, D.; Popa, C.; Foia, L.-G. Correlations between Salivary Immuno-Biochemical Markers and HbA1c in Type 2 Diabetes Subjects before and after Dental Extraction. Antioxidants 2021, 10, 1741. [Google Scholar] [CrossRef]
- Martu, M.-A.; Surlin, P.; Lazar, L.; Maftei, G.A.; Luchian, I.; Gheorghe, D.-N.; Rezus, E.; Toma, V.; Foia, L.-G. Evaluation of Oxidative Stress before and after Using Laser and Photoactivation Therapy as Adjuvant of Non-Surgical Periodontal Treatment in Patients with Rheumatoid Arthritis. Antioxidants 2021, 10, 226. [Google Scholar] [CrossRef]
- Nicolae, V.; Chiscop, I.; Cioranu, V.S.I.; Martu, M.A.; Luchian, A.I.; Martu, S.; Solomon, S.M. The use of photoactivated blue-o toluidine for periimplantitis treatment in patients with periodontal disease. Rev. Chim. (Buchar.) 2015, 66, 2121–2123. [Google Scholar]
- Cerea, M.; Dolcini, G.A. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants: A Retrospective Clinical Study on 70 Patients. BioMed Res. Int. 2018, 2018, 5420391. [Google Scholar] [CrossRef] [Green Version]
- Maftei, G.A.; Martu, C.M.; Popa, C.; Geletu, G.; Danila, V.; Jelihovschi, I.; Foia, L. The biomechanical properties of suture materials and their relationship to bacterial adherence. Mater. Plast. 2019, 56, 980–985. [Google Scholar] [CrossRef]
- Martu, M.A.; Maftei, G.A.; Sufaru, I.G.; Jelihovschi, I.; Luchian, I.; Hurjui, L.; Martu, I.; Pasarin, L. COVID-19 and Periodontal Disease-Ethiopathogenic and Clinical Implications. Rom. J. Oral Rehab. 2020, 12, 116–124. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Age | Localization/Type of Edentulism | Fit and Implant Stability | Duration of Intervention (Minutes) | Implant Survival |
|---|---|---|---|---|---|---|
| 1 | Male | 68 | Maxillary/full arch | 5 | 53 | yes |
| 2 | Female | 57 | Maxillary/full arch | 5 | 51 | yes |
| 3 | Male | 68 | Maxillary/partial arch | 2 | 112 | no |
| 4 | Female | 67 | Maxillary/full arch | 4 | 67 | yes |
| 5 | Male | 67 | Maxillary/full arch | 3 | 102 | yes |
| 6 | Male | 56 | Maxillary/full arch | 4 | 105 | yes |
| 7 | Male | 59 | Maxillary/full arch | 3 | 118 | yes |
| 8 | Female | 55 | Maxillary/full arch | 4 | 97 | yes |
| 9 | Male | 61 | Maxillary/full arch | 5 | 89 | yes |
| 10 | Male | 62 | Maxillary/full arch | 4 | 91 | yes |
| 11 | Female | 55 | Maxillary/full arch | 3 | 108 | yes |
| 12 | Male | 63 | Mandible/partial arch | 4 | 95 | yes |
| 13 | Female | 56 | Mandible/full arch | 5 | 67 | yes |
| 14 | Female | 61 | Mandible/full arch | 4 | 78 | yes |
| 15 | Male | 56 | Mandible/full arch | 4 | 98 | yes |
| 16 | Female | 69 | Mandible/full arch | 5 | 48 | yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nemtoi, A.; Covrig, V.; Nemtoi, A.; Stoica, G.; Vatavu, R.; Haba, D.; Zetu, I. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients—A Pilot Study. Diagnostics 2022, 12, 2531. https://doi.org/10.3390/diagnostics12102531
Nemtoi A, Covrig V, Nemtoi A, Stoica G, Vatavu R, Haba D, Zetu I. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients—A Pilot Study. Diagnostics. 2022; 12(10):2531. https://doi.org/10.3390/diagnostics12102531
Chicago/Turabian StyleNemtoi, Alexandru, Vlad Covrig, Ana Nemtoi, George Stoica, Ruxandra Vatavu, Danisia Haba, and Irina Zetu. 2022. "Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients—A Pilot Study" Diagnostics 12, no. 10: 2531. https://doi.org/10.3390/diagnostics12102531
APA StyleNemtoi, A., Covrig, V., Nemtoi, A., Stoica, G., Vatavu, R., Haba, D., & Zetu, I. (2022). Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants in Oral and Maxillofacial Surgery for Severe Bone-Deficient Patients—A Pilot Study. Diagnostics, 12(10), 2531. https://doi.org/10.3390/diagnostics12102531