
OCT Angiography Features in Diabetes Mellitus Type 1 and 2

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. OCT-A Imaging
2.3. Structural OCT Imaging
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. FAZ Area
3.3. Vessel Density
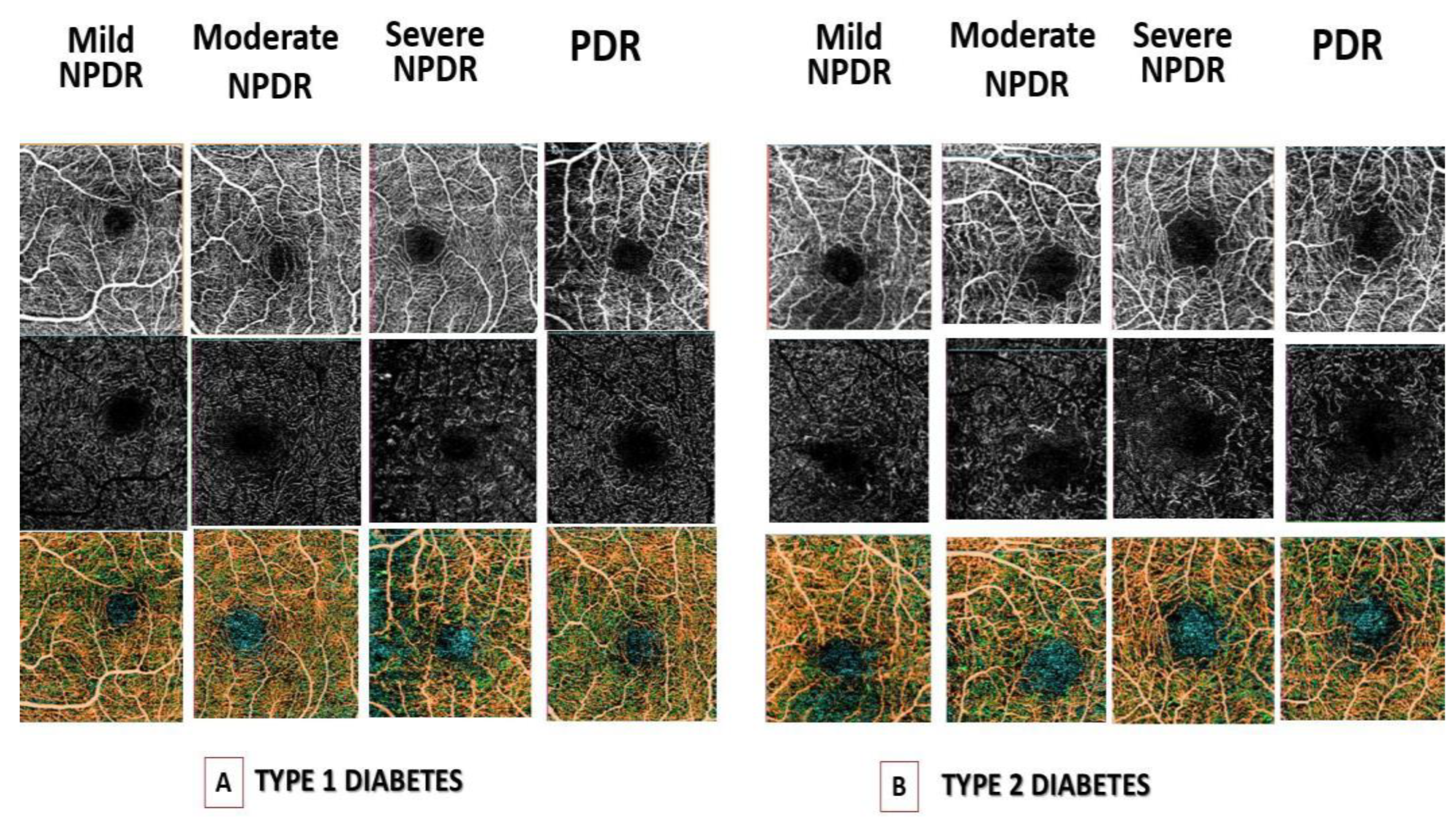
3.4. Qualitative Analysis
3.5. GCL+ and RNFL Layers
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tapp, R.J.; Shaw, J.E.; Harper, C.A.; de Courten, M.P.; Balkau, B.; McCarty, D.J.; Taylor, H.R.; Welborn, T.A.; Zimmet, P.Z.; on behalf of the AusDiab Study Group. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 2003, 26, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.; Klein, B.E.; Moss, S.E. The Wisconsin Epidemiologic Study of diabetic retinopathy. XIV. Ten-year incidence and progression of diabetic retinopathy. Arch. Ophthalmol. 1994, 112, 1217–1228. [Google Scholar] [CrossRef]
- Williams, R.; Airey, M.; Baxter, H.; Forrester, J.; Kennedy-Martin, T.; Girach, A. Epidemiology of diabetic retinopathy and macular oedema: A systematic review. Eye 2004, 18, 963–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Zuo, Y.; Wang, N.; Tong, B. Fundus fluorescence Angiography in diagnosing diabetic retinopathy. Pak. J. Med. Sci. 2017, 33, 1328–1332. [Google Scholar] [CrossRef]
- de Barros Garcia, J.M.B.; Isaac, D.L.C.; Avila, M. Diabetic retinopathy and OCT angiography: Clinical findings and future perspectives. Int. J. Retina Vitreous 2017, 3, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tey, K.Y.; Teo, K.; Tan, A.C.S.; Devarajan, K.; Tan, B.; Tan, J.; Schmetterer, L.; Ang, M. Optical coherence tomography angiography in diabetic retinopathy: A review of current applications. Eye Vis. 2019, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Khadamy, J.; Abri Aghdam, K.; Falavarjani, K.G. An Update on Optical Coherence Tomography Angiography in Diabetic Retinopathy. J. Ophthalmic Vis. Res. 2018, 13, 487–497. [Google Scholar]
- Sun, Z.; Tang, F.; Wong, R.; Lok, J.; Szeto, S.K.; Chan, J.C.; Chan, C.K.M.; Tham, C.C.; Ng, D.S.; Cheung, C.Y. OCT Angiography Metrics Predict Progression of Diabetic Retinopathy and Development of Diabetic Macular Edema: A Prospective Study. Ophthalmology 2019, 126, 1675–1684. [Google Scholar] [CrossRef]
- Ashraf, M.; Nesper, P.L.; Jampol, L.M.; Yu, F.; Fawzi, A.A. Statistical Model of Optical Coherence Tomography Angiography Parameters That Correlate with Severity of Diabetic Retinopathy. Investig. Opthalmol. Vis. Sci. 2018, 59, 4292–4298. [Google Scholar] [CrossRef] [Green Version]
- Bhanushali, D.; Anegondi, N.; Gadde, S.G.K.; Srinivasan, P.; Chidambara, L.; Yadav, N.K.; Roy, A.S. Linking retinal microvasculature features with severity of diabetic retinopathy using optical coherence tomography angiography. Investig. Opthalmol. Vis. Sci. 2016, 57, OCT519–OCT525. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, R.; Toto, L.; Mastropasqua, A.; Aloia, R.; De Nicola, C.; A Mattei, P.; Di Marzio, G.; Di Nicola, M.; Di Antonio, L. Foveal avascular zone area and parafoveal vessel density measurements in different stages of diabetic retinopathy by optical coherence tomography angiography. Int. J. Ophthalmol. 2017, 10, 1545–1551. [Google Scholar] [PubMed]
- Wu, L.; Fernandez-Loaiza, P.; Sauma, J.; Hernandez-Bogantes, E.; Masis, M. Classification of diabetic retinopathy and diabetic macular edema. World J. Diabetes 2013, 4, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Stanga, P.E.; Tsamis, E.; Papayannis, A.; Stringa, F.; Cole, T.; Jalil, A. Swept-Source Optical Coherence Tomography Angio™ (Topcon Corp, Japan): Technology Review. Dev. Ophthalmol. 2016, 56, 13–17. [Google Scholar]
- Fenner, B.J.; Tan, G.S.W.; Tan, A.C.S.; Yeo, I.Y.S.; Wong, T.Y.; Cheung, C.M.G. Identification of imaging features that determine quality and repeatability of retinal capillary plexus density measurements in OCT angiography. Br. J. Ophthalmol. 2018, 102, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Bin Lim, H.; Shin, Y.I.; Lee, M.W.; Park, G.S.; Kim, J.Y. Longitudinal changes in the peripapillary retinal nerve fiber layer thickness of patients with type 2 diabetes. JAMA Ophthalmol. 2019, 137, 1125–1132. [Google Scholar]
- Sohn, E.H.; van Dijk, H.W.; Jiao, C.; Kok, P.H.; Jeong, W.; Demirkaya, N.; Garmager, A.; Wit, F.; Kucukevcilioglu, M.; van Velthoven, M.E.J.; et al. Retinal neurodegeneration may precede microvascular changes characteristic of diabetic retinopathy in diabetes mellitus. Proc. Natl. Acad. Sci. USA 2016, 113, E2655–E2664. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.W.; Lee, J.W.; Lee, K.H.; Lee, Y.H.; Kim, J.Y. Peripapillary RNFL/vessel density ratio in patients with type2 diabetes without clinical diabetic retinopathy. Sci. Rep. 2022, 12, 9463. [Google Scholar] [CrossRef]
- Vujosevic, S.; Toma, C.; Villani, E.; Gatti, V.; Brambilla, M.; Muraca, A.; Ponziani, M.C.; Aimaretti, G.; Nuzzo, A.; Nucci, P.; et al. Early Detection of Microvascular Changes in Patients with Diabetes Mellitus without and with Diabetic Retinopathy: Comparison between Different Swept-Source OCT-A Instruments. J. Diabetes Res. 2019, 2019, 2547216. [Google Scholar] [CrossRef] [Green Version]
- Garrity, S.T.; Iafe, N.A.; Phasukkijwatana, N.; Chen, X.; Sarraf, D. Quantitative Analysis of Three Distinct Retinal Capillary Plexuses in Healthy Eyes Using Optical Coherence Tomography Angiography. Invest. Ophthalmol. Vis. Sci. 2017, 58, 5548–5555. [Google Scholar] [CrossRef] [Green Version]
- Munk, M.R.; Giannakaki-Zimmermann, H.; Berger, L.; Huf, W.; Ebneter, A.; Wolf, S.; Zinkernagel, M.S. OCT-angiography: A qualitative and quantitative comparison of 4 OCT-A devices. PLoS ONE 2017, 12, e0177059. [Google Scholar] [CrossRef]
- Ceravolo, I.; Oliverio, G.W.; Alibrandi, A.; Bhatti, A.; Trombetta, L.; Rejdak, R.; Toro, M.D.; Trombetta, C.J. The Application of Structural Retinal Biomarkers to Evaluate the Effect of Intravitreal Ranibizumab and Dexamethasone Intravitreal Implant on Treatment of Diabetic Macular Edema. Diagnostics 2020, 10, 413. [Google Scholar] [CrossRef] [PubMed]
- Meduri, A.; Oliverio, G.W.; Trombetta, L.; Giordano, M.; Inferrera, L.; Trombetta, C.J. Optical Coherence Tomography Predictors of Favorable Functional Response in Naïve Diabetic Macular Edema Eyes Treated with Dexamethasone Implants as a First-Line Agent. J. Ophthalmol. 2021, 2021, 6639418. [Google Scholar] [CrossRef]
- Takase, N.; Nozaki, M.; Kato, A.; Ozeki, H.; Yoshida, M.; Ogura, Y. Enlargement of foveal Avascular Zone in Diabetic Eyes Evaluated by En Face Optical Coherence Tomography Angiography. Retina 2015, 35, 2377–2383. [Google Scholar] [CrossRef] [PubMed]
- Talisa, E.; Chin, A.T.; Bonini Filho, M.A.; Adhi, M.; Branchini, L.; Salz, D.A.; Baumal, C.R.; Crawford, C.; Reichel, E.; Witkin, A.J.; et al. Detection of Microvascular Changes in Eyes of Patients with Diabetes but Not Clinical Diabetic Retinopathy Using Optical Coherence Tomography Angiography. Retina 2015, 35, 2364–2370. [Google Scholar]
- Oliverio, G.W.; Ceravolo, I.; Bhatti, A.; Trombetta, C.J. Foveal avascular zone analysis by optical coherence tomography angiography in patients with type 1 and 2 diabetes and without clinical signs of diabetic retinopathy. Int. Ophthalmol. 2021, 41, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Ting, D.S.W.; Tan, G.S.W.; Agrawal, R.; Yanagi, Y.; Sie, N.M.; Wong, C.W.; San Yeo, I.Y.; Lee, S.Y.; Cheung, C.M.G.; Wong, T.Y. Optical Coherence Tomographic Angiography in Type 2 Diabetes and Diabetic Retinopathy. JAMA Ophthalmol. 2017, 135, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Scarinci, F.; Nesper, P.L.; Fawzi, A.A. Deep retinal capillary nonperfusion is associated with photoreceptor disruption in diabetic macular ischemia. Am. J. Ophthalmol. 2016, 168, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Custo Greig, E.; Brigell, M.; Cao, F.; Levine, E.S.; Peters, K.; Moult, E.M.; Fujimoto, J.G.; Waheed, N.K. Macular and Peripapillary Optical Coherence Tomography Angiography Metrics Predict Progression in Diabetic Retinopathy: A Sub-analysis of TIME-2b Study Data. Am. J. Ophthalmol. 2020, 219, 66–76. [Google Scholar] [CrossRef]
- Matuszewski, W.; Stefanowicz-Rutkowska, M.M.; Szychlińska, M.; Bandurska-Stankiewicz, E. Differences in Risk Factors for Diabetic Retinopathy in Type 1 and Type 2 Diabetes Mellitus Patients in North-East Poland. Medicina 2020, 56, 177. [Google Scholar] [CrossRef] [Green Version]
- Coscas, F.; Sellam, A.; Glacet-Bernard, A.; Jung, C.; Goudot, M.; Miere, A.; Souied, E.H. Normative Data for Vascular Density in Superficial and Deep Capillary Plexuses of Healthy Adults Assessed by Optical Coherence Tomography Angiography. Invest. Ophthalmol. Vis. Sci. 2016, 57, OCT211–OCT223. [Google Scholar] [CrossRef]
- Pierro, L.; Iuliano, L.; Cicinelli, M.V.; Casalino, G.; Bandello, F. Retinal neurovascular changes appear earlier in type 2 diabetic patients. Eur. J. Ophthalmol. 2017, 27, 346–351. [Google Scholar] [CrossRef]
- Lee, M.W.; Lee, W.H.; Ryu, C.K.; Lee, Y.M.; Lee, Y.H.; Kim, J.Y. Peripapillary Retinal Nerve Fiber Layer and Microvasculature in Prolonged Type 2 Diabetes Patients Without Clinical Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2021, 62, 9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | DM1 | DM2 | Control Group 1 | Control Group 2 | p-Value |
|---|---|---|---|---|---|
| Age (years) | 55.3 ± 13.1 | 66.7 ± 7.3 | 55.6 ± 10.6 | 66.5 ± 13.4 | <0.001 |
| Gender (male/female) | 74/76 | 84/71 | 22/18 | 26/14 | 0.41 |
| Duration of diabetes (years) | 20.4 ± 8.1 | 17.5 ± 8.8 | - | - | <0.001 |
| HbA1c (%) | 7.9 ± 0.8 | 7.2 ± 0.7 | - | - | <0.001 |
| Glycaemia | 139.1 ± 23.8 | 140.2 ± 20.4 | - | - | 0.27 |
| Mild NPDR | 39 (26.0%) | 26 (16.8%) | - | - | 0.11 |
| Moderate NPDR | 36 (24.0%) | 47 (30.3%) | - | - | 0.19 |
| Severe NPDR | 40 (26.7%) | 42 (27.1%) | - | - | 0.69 |
| PDR | 35 (23.3%) | 40 (25.8%) | - | - | 0.38 |
| FAZ area SCP (mm2) | 0.550 ± 0.12 | 0.592 ± 0.18 | 0.271 ± 0.09 | 0.276 ± 0.11 | 0.62 |
| FAZ area DCP (mm2) | 0.690 ± 0.15 | 0.710 ± 0.15 | 0.320 ± 0.11 | 0.307 ± 0.12 | 0.50 |
| VD (%) | 15.1 ± 4.2 | 14.6 ± 5.2 | 22.3 ± 5.1 | 22.9 ± 5.1 | 0.51 |
| Superior VD (%) | 45.6 ± 3.0 | 45.2 ± 3.4 | 49.8 ± 5.2 | 48.1 ± 5.5 | 0.21 |
| Inferior VD (%) | 47.1 ± 3.2 | 46.3 ± 3.8 | 48.2 ± 3.9 | 46.5 ± 4.2 | 0.13 |
| Nasal VD (%) | 45.7 ± 3.7 | 44.9 ± 2.9 | 50.1 ± 5.6 | 50.4 ± 5.2 | 0.06 |
| Temporal VD (%) | 45.1 ± 2.7 | 45.5 ± 3.7 | 49.5 ± 4.6 | 48.7 ± 5.1 | 0.07 |
| Variables | DM1 | DM2 | p-Value * |
|---|---|---|---|
| FAZ SCP (mm2) | |||
| Mild NPDR | 0.408 ± 0.46 | 0.306 ± 0.52 | <0.001 |
| Moderate NPDR | 0.532 ± 0.34 | 0.479 ± 0.53.1 | <0.001 |
| Severe NPDR | 0.574 ± 0.60 | 0.551 ± 0.30 | 0.17 |
| PDR | 0.699 ± 0.72 | 0.707 ± 0.79 | 0.23 |
| p-value ** | <0.001 | <0.001 | |
| FAZ DCP (mm2) | |||
| Mild NPDR | 0.516 ± 60.3 | 0.522 ± 0.46 | 0.77 |
| Moderate NPDR | 0.647 ± 30.7 | 0.622 ± 0.46 | 0.12 |
| Severe NPDR | 0.729 ± 35.4 | 0.725 ± 0.58 | 0.79 |
| PDR | 0.885 ± 118.2 | 0.919 ± 0.88 | 0.14 |
| p-value ** | <0.001 | <0.001 | |
| VD (%) | |||
| Mild NPDR | 20.3 ± 3.9 | 23.3 ± 3.8 | <0.001 |
| Moderate NPDR | 14.9 ± 0.9 | 16.6 ± 1.1 | <0.001 |
| Severe NPDR | 13.7 ± 1.9 | 12.9 ± 1.3 | 0.91 |
| PDR | 10.9 ± 1.8 | 10.6 ± 1.4 | 0.76 |
| p-value ** | <0.001 | <0.001 | |
| Superior VD (%) | |||
| Mild NPDR | 44.8 ± 2.1 | 48.3 ± 2.4 | <0.001 |
| Moderate NPDR | 47.6 ± 1.8 | 43.4 ± 3.5 | 0.03 |
| Severe NPDR | 45.6 ± 3.9 | 43.9 ± 2.4 | 0.07 |
| PDR | 44.6 ± 2.8 | 46.6 ± 2.8 | 0.02 |
| p-value ** | 0.37 | 0.19 | |
| Inferior VD (%) | |||
| Mild NPDR | 46.2 ± 3.4 | 47.7 ± 4.1 | 0.83 |
| Moderate NPDR | 45.7 ± 3.2 | 45.7 ± 3.2 | 0.11 |
| Severe NPDR | 47.3 ± 2.5 | 47.9 ± 3.3 | 0.11 |
| PDR | 47.4 ± 3.5 | 44.5 ± 4.1 | 0.002 |
| p-value ** | 0.51 | 0.39 | |
| Nasal VD (%) | |||
| Mild NPDR | 45.4 ± 4.4 | 45.1 ± 3.0 | 0.62 |
| Moderate NPDR | 45.6 ± 3.7 | 44.2 ± 2.8 | 0.01 |
| Severe NPDR | 46.2 ± 3.6 | 44.8 ± 2.8 | 0.007 |
| PDR | 45.9 ± 3.4 | 45.8 ± 2.9 | 0.56 |
| p-value ** | 0.68 | 0.84 | |
| Temporal VD (%) | |||
| Mild NPDR | 44.6 ± 2.9 | 47.6 ± 2.8 | 0.11 |
| Moderate NPDR | 45.5 ± 1.5 | 44.9 ± 3.7 | 0.42 |
| Severe NPDR | 44.6 ± 2.4 | 45.1 ± 3.9 | 0.71 |
| PDR | 46.1 ± 3.4 | 45.5 ± 4.0 | 0.07 |
| p-value ** | 0.21 | 0.14 |
| DM1 | DM2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | FAZ SCP | FAZ DCP | VD | RNFL | GCL | FAZ SCP | FAZ DCP | VD | RNFL | GCL |
| Duration | 0.43 p = 0.03 | 0.38 p = 0.01 | −0.34 p < 0.001 | −0.28 p < 0.001 | −0.21 p < 0.001 | 0.64 p < 0.001 | 0.41 p = 0.02 | −0.39 p < 0.001 | −0.26 p < 0.001 | −0.23 p < 0.001 |
| HbA1C (%) | 0.07 p = 0.23 | 0.13 p = 0.19 | 0.11 p = 0.1 | 0.08 p = 0.2 | 0.16 p = 0.23 | 0.18 p = 0.32 | 0.15 p = 0.07 | 0.21 p = 0.11 | 0.19 p = 0.16 | 0.21 p = 0.14 |
| Variables | DM1 | DM2 | ||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| FAZ SCP | 0.003 | 0.004 | 0.004 | <0.001 |
| FAZ DCP | 0.004 | <0.001 | 0.001 | 0.03 |
| VD | −0.026 | 0.04 | −0.04 | 0.03 |
| DM1 | DM2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Mild NPDR | Moderate NPDR | Severe NPDR | PDR | Mild NPDR | Moderate NPDR | Severe NPDR | PDR |
| Irregular FAZ | 11 (28.2%) | 18 (50%) | 24 (60%) | 28 (80%) | 11 (42.3%) | 26 (55.3) | 25 (62.5%) | 33 (78.6%) |
| Capillary loss | 8 (20.5%) | 15 (41.7%) | 27 (67.5%) | 31 (88.6%) | 14 a (53.8%) | 24 (51.1%) | 30 (75%) | 36 (85.7%) |
| Capillary tortuosity | 12 (30.8%) | 18 (50%) | 31 (77.5%) | 33 (94.3%) | 11 (42.3%) | 28 (59.6%) | 31 (77.5%) | 38 (90.5%) |
| Crossing vessel | 2 (5.1%) | 2 (5.6%) | 4 (11.1%) | 8 (22.9%) | 2 (7.7%) | 3 (6.4%) | 5 (12.5%) | 9 (21.4%) |
| Variables | DM1 | DM2 | Control Group 1 | Control Group 2 | p-Value |
|---|---|---|---|---|---|
| GCL+ | |||||
| Total | 70.1 ± 1.1 | 69.7 ± 1.0 | 75.1 ± 1.2 | 74.9 ± 1.0 | 0.31 |
| Superior | 69.9 ± 1.0 | 69.5 ± 1.2 | 73.5 ± 1.1 | 73.2 ± 1.1 | 0.44 |
| Sup. Temporal | 70.8 ± 0.9 | 70.4 ± 0.8 | 74.2 ± 0.8 | 74.1 ± 1.0 | 0.73 |
| Sup. Nasal | 72.7 ± 0.7 | 72.6 ± 0.8 | 76.8 ± 1.1 | 76.5 ± 0.9 | 0.8 |
| Inferior | 67.4 ± 1.1 | 67.3 ± 1.0 | 70.1 ± 0.8 | 69.9 ± 0.9 | 0.85 |
| Inf. Temporal | 71.7 ± 0.9 | 71.9 ± 0.9 | 75.1 ± 0.9 | 74.9 ± 1.0 | 0.61 |
| Inf. Nasal | 71.9 ± 0.8 | 71.9 ± 0.9 | 75.4 ± 1.1 | 75.3 ± 0.9 | 0.89 |
| RNFL | |||||
| Total | 106.9 ± 1.5 | 106.5 ± 1.8 | 110.8 ± 1.4 | 110.4 ± 1.3 | 0.81 |
| Temporal | 76.3 ± 1.7 | 76.2 ± 1.5 | 79.4 ± 1.6 | 79.6 ± 1.5 | 0.84 |
| Sup. Temporal | 139.9 ± 2.8 | 139.5 ± 2.4 | 146.8 ± 2.1 | 146.5 ± 1.8 | 0.91 |
| Inf. Temporal | 144.3 ± 2.7 | 144.1 ± 2.8 | 150.4 ± 2.5 | 150.3 ± 2.7 | 0.92 |
| Nasal | 90.6 ± 2.2 | 90.5 ± 2.0 | 93.5 ± 1.7 | 93.2 ± 1.9 | 0.89 |
| Sup. Nasal | 120.7 ± 3.2 | 120.6 ± 3.6 | 121.7 ± 2.9 | 121.5 ± 3.1 | 0.79 |
| Inf. Nasal | 137.1 ± 3.4 | 136.8 ± 3.1 | 140.9 ± 3.3 | 140.7 ± 3.2 | 0.41 |
| Variables | DM1 | DM2 | p-Value * |
|---|---|---|---|
| GCL + Total (μm) | |||
| Mild NPDR | 70.4 ± 1.3 | 70.1 ± 1.5 | 0.37 |
| Moderate NPDR | 70.6 ± 1.5 | 70.2 ± 1.3 | 0.13 |
| Severe NPDR | 70.1 ± 1.3 | 70.4 ± 1.3 | 0.27 |
| PDR | 69.6 ± 1.3 | 68.9 ± 1.3 | 0.08 |
| p-value ** | 0.13 | 0.08 | |
| GCL + Superior (μm) | |||
| Mild NPDR | 70.7 ± 1.5 | 70.5 ± 1.2 | 0.22 |
| Moderate NPDR | 70.4 ± 1.6 | 70.4 ± 1.3 | 0.48 |
| Severe NPDR | 69.5 ± 1.7 | 69.8 ± 1.6 | 0.35 |
| PDR | 68.4 ± 1.5 | 68.5 ± 1.4 | 0.38 |
| p-value ** | 0.09 | 0.08 | |
| GCL + Sup. Temporal (μm) | |||
| Mild NPDR | 71.7 ± 1.2 | 71.5 ± 1.4 | 0.75 |
| Moderate NPDR | 70.9 ± 1.4 | 70.7 ± 1.4 | 0.62 |
| Severe NPDR | 70.2 ± 1.4 | 70.4 ± 1.5 | 0.59 |
| PDR | 69.7 ± 1.3 | 69.5 ± 1.4 | 0.49 |
| p-value ** | 0.13 | 0.12 | |
| GCL + Sup. Nasal (μm) | |||
| Mild NPDR | 74.5 ± 1.5 | 74.6 ± 1.6 | 0.72 |
| Moderate NPDR | 73.6 ± 1.4 | 73.3 ± 1.4 | 0.46 |
| Severe NPDR | 71.9 ± 1.5 | 72.1 ± 1.4 | 0.32 |
| PDR | 69.8 ± 1.5 | 69.9 ± 1.3 | 0.88 |
| p-value ** | 0.04 | 0.04 | |
| GCL + Inferior (μm) | |||
| Mild NPDR | 70.1 ± 1.2 | 70.3 ± 1.4 | 0.77 |
| Moderate NPDR | 69.6 ± 1.4 | 69.7 ± 1.3 | 0.83 |
| Severe NPDR | 68.1 ± 1.4 | 68.5 ± 1.5 | 0.79 |
| PDR | 65.4 ± 1.4 | 65.5 ± 1.4 | 0.88 |
| p-value ** | 0.03 | 0.02 | |
| GCL + Inf. Temporal (μm) | |||
| Mild NPDR | 72.6 ± 1.5 | 72.4 ± 1.6 | 0.55 |
| Moderate NPDR | 72.1 ± 1.5 | 72.2 ± 1.3 | 0.51 |
| Severe NPDR | 71.4 ± 1.3 | 71.5 ± 1.3 | 0.47 |
| PDR | 70.2 ± 1.4 | 70.4 ± 1.3 | 0.67 |
| p-value ** | 0.09 | 0.08 | |
| GCL + Inf. Nasal (μm) | |||
| Mild NPDR | 72.4 ± 1.4 | 72.4 ± 1.5 | 0.96 |
| Moderate NPDR | 71.3 ± 1.5 | 71.2 ± 1.3 | 0.83 |
| Severe NPDR | 70.4 ± 1.4 | 70.5 ± 1.3 | 0.79 |
| PDR | 70.1 ± 1.4 | 70.2 ± 1.4 | 0.88 |
| p-value ** | 0.13 | 0.11 | |
| RNFL Total (μm) | |||
| Mild NPDR | 107.6± 1.8 | 107.5± 1.6 | 0.89 |
| Moderate NPDR | 107.4± 1.5 | 107.7± 1.5 | 0.63 |
| Severe NPDR | 106.8± 1.9 | 106.9± 1.7 | 0.79 |
| PDR | 106.2± 1.8 | 106.6± 1.9 | 0.55 |
| p-value ** | 0.27 | 0.31 | |
| RNFL Temporal (μm) | |||
| Mild NPDR | 77.8 ± 1.6 | 77.6 ± 1.7 | 0.75 |
| Moderate NPDR | 77.2 ± 1.5 | 77.1 ± 1.6 | 0.82 |
| Severe NPDR | 76.5 ± 1.6 | 76.4 ± 1.6 | 0.79 |
| PDR | 75.1 ± 1.6 | 75.2 ± 1.7 | 0.83 |
| p-value ** | 0.14 | 0.15 | |
| RNFL Sup. Temporal (μm) | |||
| Mild NPDR | 142.5 ± 2.8 | 142.6 ± 2.6 | 0.91 |
| Moderate NPDR | 141.8 ± 2.7 | 141.7 ± 2.6 | 0.91 |
| Severe NPDR | 140.4 ± 2.7 | 140.5 ± 2.5 | 0.91 |
| PDR | 139.2 ± 2.5 | 139.3 ± 2.6 | 0.91 |
| p-value ** | 0.13 | 0.11 | |
| RNFL Inf. Temporal (μm) | |||
| Mild NPDR | 146.5 ± 2.6 | 146.4 ± 2.6 | 0.94 |
| Moderate NPDR | 145.4 ± 2.6 | 145.3 ± 2.6 | 0.88 |
| Severe NPDR | 144.6 ± 2.7 | 144.6 ± 2.7 | 0.92 |
| PDR | 143.2 ± 2.8 | 143.3 ± 2.6 | 0.90 |
| p-value ** | 0.07 | 0.08 | |
| RNFL Nasal (μm) | |||
| Mild NPDR | 92.3 ± 2.3 | 92.5 ± 2.2 | 0.76 |
| Moderate NPDR | 91.6 ± 2.3 | 91.7 ± 2.3 | 0.81 |
| Severe NPDR | 90.4 ± 2.2 | 90.6 ± 2.3 | 0.86 |
| PDR | 89.6 ± 2.3 | 89.5 ± 2.3 | 0.91 |
| p-value ** | 0.06 | 0.07 | |
| RNFL Sup. Nasal (μm) | |||
| Mild NPDR | 122.6 ± 3.3 | 122.7 ± 3.2 | 0.81 |
| Moderate NPDR | 121.5 ± 3.2 | 121.7 ± 3.4 | 0.72 |
| Severe NPDR | 120.8 ± 3.3 | 120.7 ± 3.3 | 0.77 |
| PDR | 119.4 ± 3.3 | 119.5 ± 3.4 | 0.79 |
| p-value ** | 0.09 | 0.08 | |
| RNFL Inf. Nasal (μm) | |||
| Mild NPDR | 139.6 ± 3.3 | 139.7 ± 3.3 | 0.52 |
| Moderate NPDR | 138.8 ± 3.4 | 138.7 ± 3.4 | 0.53 |
| Severe NPDR | 137.6 ± 3.5 | 137.8 ± 3.5 | 0.35 |
| PDR | 136.2 ± 3.4 | 136.4 ± 3.4 | 0.31 |
| p-value ** | 0.12 | 0.11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliverio, G.W.; Meduri, A.; De Salvo, G.; Trombetta, L.; Aragona, P. OCT Angiography Features in Diabetes Mellitus Type 1 and 2. Diagnostics 2022, 12, 2942. https://doi.org/10.3390/diagnostics12122942
Oliverio GW, Meduri A, De Salvo G, Trombetta L, Aragona P. OCT Angiography Features in Diabetes Mellitus Type 1 and 2. Diagnostics. 2022; 12(12):2942. https://doi.org/10.3390/diagnostics12122942
Chicago/Turabian StyleOliverio, Giovanni William, Alessandro Meduri, Gabriella De Salvo, Luigi Trombetta, and Pasquale Aragona. 2022. "OCT Angiography Features in Diabetes Mellitus Type 1 and 2" Diagnostics 12, no. 12: 2942. https://doi.org/10.3390/diagnostics12122942
APA StyleOliverio, G. W., Meduri, A., De Salvo, G., Trombetta, L., & Aragona, P. (2022). OCT Angiography Features in Diabetes Mellitus Type 1 and 2. Diagnostics, 12(12), 2942. https://doi.org/10.3390/diagnostics12122942