
Refractive Outcomes after Cataract Surgery

 ,
,  ,
, 
Abstract
:1. Introduction
2. Refractive Outcomes Prior to the Advent of Modern Optical Biometry
3. Pre-, Intra-, and Post-Operative Factors That Affect Refractive Outcomes
3.1. Pre-Operative Factors
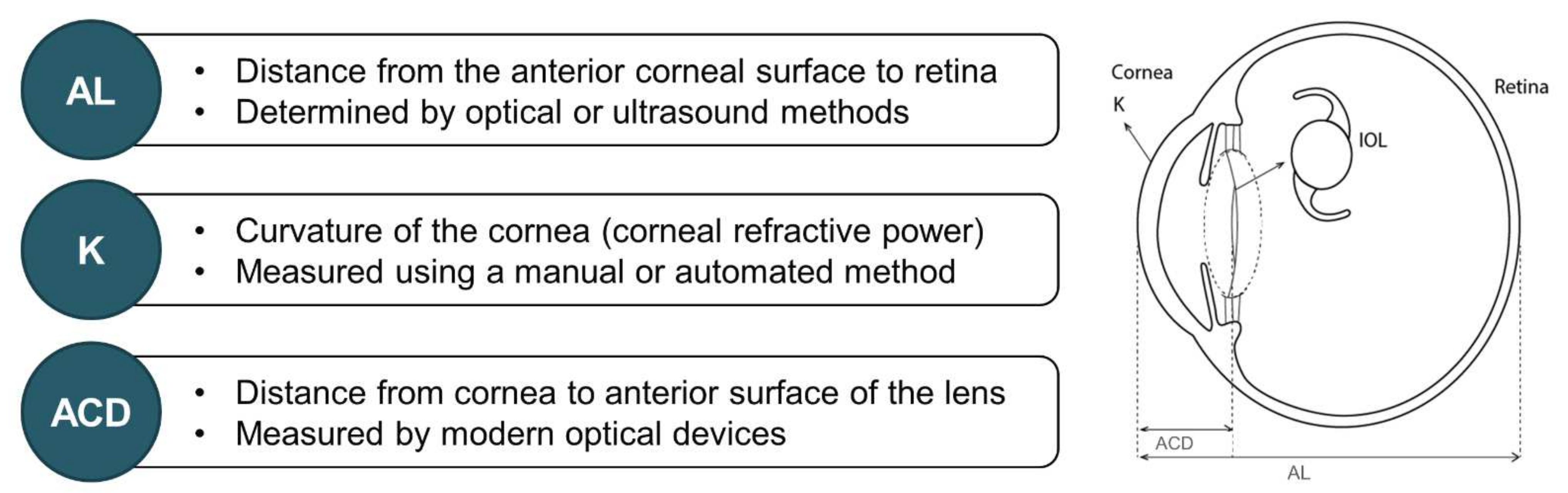
3.1.1. Axial Length
3.1.2. Corneal Power
3.1.3. Pre-Operative Corneal Astigmatism
3.1.4. Anterior Chamber Depth
3.1.5. IOL Power Calculations
3.1.6. Other Pre-Operative Considerations
3.2. Intra-Operative Factors
3.3. Post-Operative Factors
4. How Modern-Day Biometry Has Changed Refractive Outcomes
5. The Impact of Residual Refractive Error on Visual Outcomes
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abdelghany, A.A.; Alio, J.L. Surgical options for correction of refractive error following cataract surgery. Eye Vis. 2014, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Aristodemou, P.; Cartwright, N.E.; Sparrow, J.M.; Johnston, R.L. Improving refractive outcomes in cataract surgery: A global perspective. World J. Ophthalmol. 2014, 4, 140–146. [Google Scholar] [CrossRef]
- Ladi, J.S. Prevention and correction of residual refractive errors after cataract surgery. J. Clin. Ophthalmol. Res. 2017, 5, 45. [Google Scholar] [CrossRef]
- Coleman, D.J.; Carlin, B. A new system for visual axis measurements in the human eye using ultrasound. Arch. Ophthalmol. 1967, 77, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Ademola-Popoola, D.S.; Nzeh, D.A.; Saka, S.E.; Olokoba, L.B.; Obajolowo, T.S. Comparison of ocular biometry measurements by applanation and immersion A-scan techniques. J. Curr. Ophthalmol. 2015, 27, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, P.; Hütz, W.; Eckhardt, H.; Heuring, A. Intraocular lens calculation and ultrasound biometry: Immersion and contact proceduresn. Klin. Mon. Augenheilkd. 1998, 213, 161–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giers, U.; Epple, C. Comparison of A-scan device accuracy. J. Cataract. Refract. Surg. 1990, 16, 235–242. [Google Scholar] [CrossRef]
- Rajan, M.S.; Keilhorn, I.; Bell, J.A. Partial coherence laser interferometry vs conventional ultrasound biometry in intraocular lens power calculations. Eye 2002, 16, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, S.W.; Lim, S.H.; Lee, H.Y. Accuracy of biometry for intraocular lens implantation using the new partial coherence interferometer, AL-scan. Korean J. Ophthalmol. 2014, 28, 444–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, C.; Tuft, S.J.; Minassian, D.C. Refractive error and visual outcome after cataract extraction. J. Cataract. Refract. Surg. 2002, 28, 62–66. [Google Scholar] [CrossRef]
- Kugelberg, M.; Lundström, M. Factors related to the degree of success in achieving target refraction in cataract surgery: Swedish National Cataract Register study. J. Cataract. Refract. Surg. 2008, 34, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Drexler, W.; Findl, O.; Menapace, R.; Rainer, G.; Vass, C.; Hitzenberger, C.; Fercher, A.F. Partial coherence interferometry: A novel approach to biometry in cataract surgery. Am. J. Ophthalmol. 1998, 126, 524–534. [Google Scholar] [CrossRef]
- Sahin, A.; Hamrah, P. Clinically relevant biometry. Curr. Opin. Ophthalmol. 2012, 23, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hitzenberger, C.K.; Drexler, W.; Leitgeb, R.A.; Findl, O.; Fercher, A.F. Key developments for partial coherence biometry and optical coherence tomography in the human eye made in Vienna. Investig. Opthalmology Vis. Sci. 2016, 57, 460–474. [Google Scholar] [CrossRef] [Green Version]
- Roy, A.; Das, S.; Sahu, S.K.; Rath, S. Ultrasound biometry vs. IOL Master. Ophthalmology 2012, 119, 1937–1937.e2. [Google Scholar] [CrossRef] [PubMed]
- Landers, J.; Goggin, M. Comparison of refractive outcomes using immersion ultrasound biometry and IOLMaster biometry. Clin. Exp. Ophthalmol. 2009, 37, 566–569. [Google Scholar] [CrossRef]
- Nakhli, F.R. Comparison of optical biometry and applanation ultrasound measurements of the axial length of the eye. Saudi J. Ophthalmol. 2014, 28, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.W. Ultrasound vs. Optical Biometry. Available online: https://www.ophthalmologyweb.com/Tech-Spotlights/26583-Ultrasound-Vs-Optical-Biometry/ (accessed on 10 December 2021).
- Hill, W. Biometry Methods Explained. Available online: https://www.doctor-hill.com/iol-main/biometry_explained.html (accessed on 10 December 2021).
- Gale, R.P.; Saldana, M.; Johnston, R.L.; Zuberbuhler, B.; McKibbin, M. Benchmark standards for refractive outcomes after NHS cataract surgery. Eye 2009, 23, 149–152. [Google Scholar] [CrossRef]
- Lundström, M.; Stenevi, U.; Thorburn, W. The Swedish National Cataract Register: A 9-year review. Acta Ophthalmol. Scand. 2002, 80, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Behndig, A.; Montan, P.; Stenevi, U.; Kugelberg, M.; Zetterström, C.; Lundström, M. Aiming for emmetropia after cataract surgery: Swedish National Cataract Register study. J. Cataract. Refract. Surg. 2012, 38, 1181–1186. [Google Scholar] [CrossRef]
- Hahn, U.; Krummenauer, F.; Kölbl, B.; Neuhann, T.; Schayan-Araghi, K.; Schmickler, S.; von Wolff, K.; Weindler, J.; Will, T.; Neuhann, I. Determination of valid benchmarks for outcome indicators in cataract surgery: A multicenter, prospective cohort trial. Ophthalmology 2011, 118, 2105–2112. [Google Scholar] [CrossRef]
- Lundström, M.; Dickman, M.; Henry, Y.; Manning, S.; Rosen, P.; Tassignon, M.-J.; Young, D.; Behndig, A.; Stenevi, U. Changing practice patterns in European cataract surgery as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery 2008 to 2017. J. Cataract Refract. Surg. 2021, 47, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Aristodemou, P.; Cartwright, N.E.K.; Sparrow, J.M.; Johnston, R.L. First eye prediction error improves second eye refractive outcome. Opthalmology 2011, 118, 1701–1709. [Google Scholar] [CrossRef]
- Jivrajka, R.V.; Shammas, M.C.; Shammas, H.J. Improving the second-eye refractive error in patients undergoing bilateral sequential cataract surgery. Ophthalmology 2012, 119, 1097–1101. [Google Scholar] [CrossRef] [PubMed]
- Tamaoki, A.; Kojima, T.; Hasegawa, A.; Yamamoto, M.; Kaga, T.; Tanaka, K.; Ichikawa, K. Clinical evaluation of a new swept-source optical coherence biometer that uses individual refractive indices to measure axial length in cataract patients. Ophthalmic Res. 2019, 62, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Shammas, J.H.; Ortiz, S.; Shammas, M.C.; Kim, S.H.; Chong, C. Biometry measurements using a new large-coherence–length swept-source optical coherence tomographer. J. Cataract Refract. Surg. 2016, 42, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Goto, S.; Maeda, N.; Noda, T.; Ohnuma, K.; Koh, S.; Iehisa, I.; Nishida, K. Comparison of composite and segmental methods for acquiring optical axial length with swept-source optical coherence tomography. Sci. Rep. 2020, 10, 4474. [Google Scholar] [CrossRef]
- Hirnschall, N.; Varsits, R.; Doeller, B.; Findl, O. enhanced penetration for axial length measurement of eyes with dense cataracts using swept source optical coherence tomography: A consecutive observational study. Ophthalmol. Ther. 2018, 7, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.C.; Qazi, M.A.; Pepose, J.S. Biometry and intraocular lens power calculation. Curr. Opin. Ophthalmol. 2008, 19, 13–17. [Google Scholar] [CrossRef]
- Kaswin, G.; Rousseau, A.; Mgarrech, M.; Barreau, E.; Labetoulle, M. Biometry and intraocular lens power calculation results with a new optical biometry device: Comparison with the gold standard. J. Cataract. Refract. Surg. 2014, 40, 593–600. [Google Scholar] [CrossRef]
- Olsen, T. Calculation of intraocular lens power: A review. Acta Ophthalmol. Scand. 2007, 85, 472–485. [Google Scholar] [CrossRef]
- Millán, M.S.; Alba-Bueno, F.; Vega, F. New trends in intraocular lens imaging. In Proceedings of the 22nd Congress of the International Commission for Optics: Light for the Development of the World, Puebla, Mexico, 15–19 August 2011; Volume 8011, p. 80119. [Google Scholar]
- American Academy of Ophthalmology. Biometry for Intra-Ocular Lens (IOL) Power Calculation. Available online: https://eyewiki.aao.org/Biometry_for_Intra-Ocular_Lens_(IOL)_Power_Calculation (accessed on 10 December 2020).
- Tamaoki, A.; Kojima, T.; Hasegawa, A.; Yamamoto, M.; Kaga, T.; Tanaka, K.; Ichikawa, K. Evaluation of axial length measurement using enhanced retina visualization mode of the swept-source optical coherence tomography biometer in dense cataract. Ophthalmic Res. 2021, 64, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Kanclerz, P.; Khoramnia, R.; Wang, X. Current developments in corneal topography and tomography. Diagnostics 2021, 11, 1466. [Google Scholar] [CrossRef] [PubMed]
- Day, A.C.; Dhariwal, M.; Keith, M.S.; Ender, F.; Vives, C.P.; Miglio, C.; Zou, L.; Anderson, D.F. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br. J. Ophthalmol. 2018, 103, 993–1000. [Google Scholar] [CrossRef] [Green Version]
- Koch, D.D. The posterior cornea: Hiding in plain sight. Ophthalmology 2015, 122, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Łabuz, G.; Varadi, D.; Khoramnia, R.; Auffarth, G.U. Central and mid-peripheral corneal astigmatism in an elderly population: A retrospective analysis of Scheimpflug topography results. Sci. Rep. 2021, 11, 7968. [Google Scholar] [CrossRef]
- Łabuz, G.; Varadi, D.; Khoramnia, R.; Auffarth, G.U. Progressive-toric IOL design reduces residual astigmatism with increasing pupil size: A ray-tracing simulation based on corneal topography data. Biomed. Opt. Express 2021, 12, 1568–1576. [Google Scholar] [CrossRef]
- Ho, J.-D.; Tsai, C.-Y.; Liou, S.-W. Accuracy of corneal astigmatism estimation by neglecting the posterior corneal surface measurement. Am. J. Ophthalmol. 2009, 147, 788–795.e2. [Google Scholar] [CrossRef] [PubMed]
- Koch, D.D.; Ali, S.F.; Weikert, M.; Shirayama, M.; Jenkins, R.; Wang, L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J. Cataract Refract. Surg. 2012, 38, 2080–2087. [Google Scholar] [CrossRef]
- Koch, D.D.; Jenkins, R.B.; Weikert, M.P.; Yeu, E.; Wang, L. Correcting astigmatism with toric intraocular lenses: Effect of posterior corneal astigmatism. J. Cataract Refract. Surg. 2013, 39, 1803–1809. [Google Scholar] [CrossRef] [PubMed]
- Norrby, S. Sources of error in intraocular lens power calculation. J. Cataract Refract. Surg. 2008, 34, 368–376. [Google Scholar] [CrossRef]
- Rabsilber, T.M.; Khoramnia, R.; Auffarth, G. Anterior chamber measurements using Pentacam rotating Scheimpflug camera. J. Cataract. Refract. Surg. 2006, 32, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Schröder, S.; Leydolt, C.; Menapace, R.; Eppig, T.; Langenbucher, A. Determination of personalized IOL-constants for the Haigis formula under consideration of measurement precision. PLoS ONE 2016, 11, e0158988. [Google Scholar] [CrossRef]
- Sheard, R. Optimising biometry for best outcomes in cataract surgery. Eye 2014, 28, 118–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.H.; Karp, C.L.; Yoo, S.H.; Amescua, G.; Galor, A. Cataract surgery after refractive surgery. Int. Ophthalmol. Clin. 2016, 56, 169–180. [Google Scholar] [CrossRef] [Green Version]
- Khoramnia, R.; Auffarth, G.; Rabsilber, T.M.; Holzer, M.P. Implantation of a multifocal toric intraocular lens with a surface-embedded near segment after repeated LASIK treatments. J. Cataract. Refract. Surg. 2012, 38, 2049–2052. [Google Scholar] [CrossRef] [PubMed]
- Turczynowska, M.; Koźlik-Nowakowska, K.; Gaca-Wysocka, M.; Grzybowski, A. Effective ocular biometry and intraocular lens power calculation. Eur. Ophthalmic Rev. 2016, 10, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Vale, C.; Menezes, C.; Firmino-Machado, J.; Rodrigues, P.; Lume, M.; Tenedório, P.; Menéres, P.; Brochado, M.D.C. Astigmatism management in cataract surgery with Precizon® toric intraocular lens: A prospective study. Clin. Ophthalmol. 2016, 10, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.H.; Kim, K.-H.; Lee, J.Y.; Nam, D.H. Surgically induced astigmatism after 3.0 mm temporal and nasal clear corneal incisions in bilateral cataract surgery. Indian J. Ophthalmol. 2013, 61, 645–648. [Google Scholar] [CrossRef]
- Yang, J.; Wang, X.; Zhang, H.; Pang, Y.; Wei, R.-H. Clinical evaluation of surgery-induced astigmatism in cataract surgery using 2.2 mm or 1.8 mm clear corneal micro-incisions. Int. J. Ophthalmol. 2017, 10, 68–71. [Google Scholar] [CrossRef]
- Liu, J.; Wolfe, P.; Hernandez, V.; Kohnen, T. Comparative assessment of the corneal incision enlargement of 4 preloaded IOL delivery systems. J. Cataract. Refract. Surg. 2020, 46, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.S.; Subash, M.; Sandhu, A.; Wilkins, M. Intraocular lens delivery characteristics of the preloaded AcrySof IQ SN60WS/AcrySert Injectable Lens System. Am. J. Ophthalmol. 2013, 156, 77–81.e2. [Google Scholar] [CrossRef]
- Yildirim, T.M.; Łabuz, G.; Baur, I.D.; Poompokawat, P.; Knorz, M.C.; Auffarth, G.U.; Khoramnia, R. Corneal incision enlargement in two preloaded intraocular lens injectors: An intraindividual in vivo study. J. Refract. Surg. 2021, 37, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Khoramnia, R.; Yildirim, T.M.; Weindler, J.; Naujokaitis, T.; Dzhambazova, M.; Auffarth, G.U. Preloaded injectors used in a clinical study: Videographic assessment and laboratory analysis of injector nozzle damage. J. Cataract. Refract. Surg. 2021, 47, 1338–1344. [Google Scholar] [CrossRef]
- American Academy of Ophthalmology. Toric IOLs. Available online: http://eyewiki.aao.org/Toric_IOLs (accessed on 24 May 2021).
- American Academy of Ophthalmology. Toric IOLs: Four Options for Addressing Residual Astigmatism. Available online: https://www.aao.org/eyenet/article/toric-iols-four-options-addressing-residual-astigm (accessed on 24 May 2021).
- Gatinel, D.; Debellemanière, G.; Saad, A.; Dubois, M.; Rampat, R. Determining the theoretical effective lens position of thick intraocular lenses for machine learning–based IOL power calculation and simulation. Transl. Vis. Sci. Technol. 2021, 10, 27. [Google Scholar] [CrossRef]
- Erickson, P. Effects of intraocular lens position errors on postoperative refractive error. J. Cataract. Refract. Surg. 1990, 16, 305–311. [Google Scholar] [CrossRef]
- Shajari, M.; Sonntag, R.; Niermann, T.; Holland, D.; Kohnen, T.; Priglinger, S.; Mayer, W.J. Determining and comparing the effective lens position and refractive outcome of a novel rhexis-fixated lens to established lens designs. Am. J. Ophthalmol. 2020, 213, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Łabuz, G.; Auffarth, G.; Yan, W.; Yildirim, T.; Khoramnia, R. Simulations of decentration and tilt of a supplementary sulcus-fixated intraocular lens in a polypseudophakic combination using ray-tracing software. Photonics 2021, 8, 309. [Google Scholar] [CrossRef]
- Ashena, Z.; Maqsood, S.; Ahmed, S.N.; Nanavaty, M.A. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision 2020, 4, 41. [Google Scholar] [CrossRef]
- Tandogan, T.; Son, H.S.; Choi, C.Y.; Knorz, M.C.; Auffarth, G.U.; Khoramnia, R. Laboratory evaluation of the influence of decentration and pupil size on the optical performance of a monofocal, bifocal, and trifocal intraocular lens. J. Refract. Surg. 2017, 33, 808–812. [Google Scholar] [CrossRef] [Green Version]
- Auffarth, G.U.; Friedmann, E.; Breyer, D.; Kaymak, H.; Holland, D.; Dick, B.; Petzold, A.; Shah, S.; Ladaria, L.S.; Garcia, S.A.; et al. Stability and visual outcomes of the capsulotomy-fixated FEMTIS-IOL after automated femtosecond laser–assisted anterior capsulotomy. Am. J. Ophthalmol. 2021, 225, 27–37. [Google Scholar] [CrossRef]
- Goss, D.A.; Grosvenor, T. Reliability of refraction--a literature review. J. Am. Optom. Assoc. 1996, 67, 619–630. [Google Scholar]
- Zadnik, K.; Mutti, D.O.; Adams, A.J. The repeatability of measurement of the ocular components. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2325–2333. [Google Scholar]
- Bullimore, M.A.; Fusaro, R.E.; Adams, C.W. The repeatability of automated and clinician refraction. Optom. Vis. Sci. 1998, 75, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Sheedy, J.; Schanz, P.; Bullimore, M. Evaluation of an automated subjective refractor. Optom. Vis. Sci. 2004, 81, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Smith, G. Refraction and visual acuity measurements: What are their measurement uncertainties? Clin. Exp. Optom. 2006, 89, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, A.M.; Barrett, G.D. Using the first-eye prediction error in cataract surgery to refine the refractive outcome of the second eye. J. Cataract. Refract. Surg. 2019, 45, 1239–1245. [Google Scholar] [CrossRef]
- Leffler, C.T.; Wilkes, M.; Reeves, J.; Mahmood, M.A. Postoperative refraction in the second eye having cataract surgery. ISRN Ophthalmol. 2011, 2011, 273923. [Google Scholar] [CrossRef] [Green Version]
- Higashiyama, T.; Mori, H.; Nakajima, F.; Ohji, M. Comparison of a new biometer using swept-source optical coherence tomography and a conventional biometer using partial coherence interferometry. PLoS ONE 2018, 13, e0196401. [Google Scholar] [CrossRef]
- Huang, J.; Chen, H.; Li, Y.; Chen, Z.; Gao, R.; Yu, J.; Zhao, Y.; Lu, W.; McAlinden, C.; Wang, Q. Comprehensive comparison of axial length measurement with three swept-source OCT-Based biometers and partial coherence interferometry. J. Refract. Surg. 2019, 35, 115–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatino, F.; Matarazzo, F.; Findl, O.; Maurino, V. Comparative analysis of 2 swept-source optical coherence tomography biometers. J. Cataract Refract. Surg. 2019, 45, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.M.; Lim, D.H.; Kim, H.J.; Chung, T.-Y. Comparison of two swept-source optical coherence tomography biometers and a partial coherence interferometer. PLoS ONE 2019, 14, e0223114. [Google Scholar] [CrossRef]
- Whang, W.-J.; Yoo, Y.-S.; Kang, M.-J.; Joo, C.-K. Predictive accuracy of partial coherence interferometry and swept-source optical coherence tomography for intraocular lens power calculation. Sci. Rep. 2018, 8, 13732. [Google Scholar] [CrossRef]
- Connell, B.J.; Kane, J. Comparison of the Kane formula with existing formulas for intraocular lens power selection. BMJ Open Ophthalmol. 2019, 4, e000251. [Google Scholar] [CrossRef]
- Omoto, M.K.; Torii, H.; Masui, S.; Ayaki, M.; Tsubota, K.; Negishi, K. Ocular biometry and refractive outcomes using two swept-source optical coherence tomography-based biometers with segmental or equivalent refractive indices. Sci. Rep. 2019, 9, 6557. [Google Scholar] [CrossRef] [PubMed]
- Shammas, H.J.; Shammas, M.C.; Jivrajka, R.V.; Cooke, D.L.; Potvin, R. Effects on IOL power calculation and expected clinical outcomes of axial length measurements based on multiple vs single refractive indices. Clin. Ophthalmol. 2020, 14, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, G.R. Spectacle independence after cataract surgery: A prospective study with a multifocal intraocular lens. Med. Hypothesis Discov. Innov. Ophthalmol. 2020, 9, 38–46. [Google Scholar] [PubMed]
- Hovanesian, J.A.; Lane, S.S.; Allen, Q.B.; Jones, M. Patient-reported outcomes/satisfaction and spectacle independence with blended or bilateral multifocal intraocular lenses in cataract surgery. Clin. Ophthalmol. 2019, 13, 2591–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Kouhen, N.; Mnasri, H.; Mouna, A.; Agapie, A.; Ferte, A.; Ameloot, F.; Perone, J.-M. Refractive outcome and patient satisfaction after cataract surgery with mutifocal intraocular lens implantation. Investig. Ophthalmol. Vis. Sci. 2013, 54, 2999. [Google Scholar]
- Visser, N.; Nuijts, R.M.; de Vries, N.E.; Bauer, N.J. Visual outcomes and patient satisfaction after cataract surgery with toric multifocal intraocular lens implantation. J. Cataract. Refract. Surg. 2011, 37, 2034–2042. [Google Scholar] [CrossRef]
- Lavanya, R.; Wong, T.Y.; Aung, T.; Tan, D.T.H.; Saw, S.-M.; Tay, W.T.; Wang, J.J.; For the SiMES Team. Prevalence of cataract surgery and post-surgical visual outcomes in an urban Asian population: The Singapore Malay Eye Study. Br. J. Ophthalmol. 2009, 93, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Kanthan, G.L.; Mitchell, P.; Burlutsky, G.; Wang, J.J. Intermediate- and longer-term visual outcomes after cataract surgery: The Blue Mountains Eye Study. Clin. Exp. Ophthalmol. 2010, 39, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Keel, S.; Xie, J.; Foreman, J.; Taylor, H.R.; Dirani, M. Population-based assessment of visual acuity outcomes following cataract surgery in Australia: The National Eye Health Survey. Br. J. Ophthalmol. 2018, 102, 1419–1424. [Google Scholar] [CrossRef]
- Park, C.Y.; Chuck, R.S. Residual refractive error and visual outcome after cataract surgery using spherical versus aspheric IOLs. Ophthalmic Surg. Lasers Imaging Retin. 2011, 42, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Vega, L.; Alfonso, J.F.; Montés-Micó, R.; Amhaz, H. Visual acuity tolerance to residual refractive errors in patients with an apodized diffractive intraocular lens. J. Cataract. Refract. Surg. 2008, 34, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.K.; Schlichtenbrede, F.C.; Harder, B.C.; Beutelspacher, S.C.; Jonas, J.B. Target refraction for best uncorrected distance and near vision in cataract surgery. Eur. J. Ophthalmol. 2014, 24, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Son, H.-S.; Kim, S.H.; Auffarth, G.U.; Choi, C.Y. Prospective comparative study of tolerance to refractive errors after implantation of extended depth of focus and monofocal intraocular lenses with identical aspheric platform in Korean population. BMC Ophthalmol. 2019, 19, 187. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.E.; Webers, C.A.; Touwslager, W.R.; Bauer, N.J.; de Brabander, J.; Berendschot, T.T.; Nuijts, R.M. Dissatisfaction after implantation of multifocal intraocular lenses. J. Cataract Refract. Surg. 2011, 37, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Sales, C.; Manche, E.E. Managing residual refractive error after cataract surgery. J. Cataract. Refract. Surg. 2015, 41, 1289–1299. [Google Scholar] [CrossRef] [PubMed]
- von Mohrenfels, C.W.; Salgado, J.; Khoramnia, R.; Maier, M.; Lohmann, C.P. Clinical results with the light adjustable intraocular lens after cataract surgery. J. Refract. Surg. 2010, 26, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Jobson Medical Information LLC. Answering Your Top 10 IOL-Formula Questions. Review of Ophthalmology Annual IOL Edition. Reviewofophthalmology.com. 2018. Available online: https://www.reviewofophthalmology.com/CMSDocuments/2018/01/rp0118i.pdf (accessed on 25 August 2021).
- Baur, I.D.; Auffarth, G.U.; Yildirim, T.M.; Mayer, C.S.; Khoramnia, R. Reversibility of the duet procedure: Bilateral exchange of a supplementary trifocal sulcus-fixated intraocular lens for correction of a postoperative refractive error. Am. J. Ophthalmol. Case Rep. 2020, 20, 100957. [Google Scholar] [CrossRef] [PubMed]
- Łabuz, G.; Auffarth, G.U.; Knorz, M.C.; Son, H.-S.; Yildirim, T.M.; Khoramnia, R. Trifocality achieved through polypseudophakia: Optical quality and light loss compared with a single trifocal intraocular lens. J. Refract. Surg. 2020, 36, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Khoramnia, R.; Yildirim, T.M.; Son, H.-S.; Łabuz, G.; Mayer, C.S.; Auffarth, G.U. Reversible Trifokalität durch das Duett-Verfahren. Ophthalmologe 2020, 117, 999–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoramnia, R.; Yildirim, T.M.; Baur, I.; Auffarth, G.U. Duet procedure to achieve reversible trifocality in a young patient with hereditary hyperferritinemia-cataract syndrome. Am. J. Ophthalmol. Case Rep. 2021, 21, 101026. [Google Scholar] [CrossRef] [PubMed]
- Ang, R.E. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with small aperture, trifocal, or monofocal intraocular lenses. Clin. Ophthalmol. 2019, 13, 905–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carones, F. Residual astigmatism threshold and patient satisfaction with bifocal, trifocal and extended range of vision intraocular lenses (IOLs). Open J. Ophthalmol. 2017, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Pesala, V.; Garg, P.; Bharadwaj, S.R. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom. Vis. Sci. 2013, 90, 378–384. [Google Scholar] [CrossRef]
- Kohnen, T.; Herzog, M.; Hemkeppler, E.; Schönbrunn, S.; De Lorenzo, N.; Petermann, K.; Böhm, M. Visual performance of a quadrifocal (trifocal) intraocular lens following removal of the crystalline lens. Am. J. Ophthalmol. 2017, 184, 52–62. [Google Scholar] [CrossRef]
- Ribeiro, F.; Ferreira, T.B. Comparison of clinical outcomes of 3 trifocal IOLs. J. Cataract. Refract. Surg. 2020, 46, 1247–1252. [Google Scholar] [CrossRef]
- Böhm, M.; Petermann, K.; Hemkeppler, E.; Kohnen, T. Defocus curves of 4 presbyopia-correcting IOL designs: Diffractive panfocal, diffractive trifocal, segmental refractive, and extended-depth-of-focus. J. Cataract Refract. Surg. 2019, 45, 1625–1636. [Google Scholar] [CrossRef]
- Tran, D.B.; Owyang, A.; Hwang, J.; Potvin, R. Visual acuity, quality of vision, and patient-reported outcomes after bilateral implantation with a trifocal or extended depth of focus intraocular lens. Clin. Ophthalmol. 2021, 15, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Shamir, R.R.; Friedman, Y.G.; Joskowicz, L.; Mimouni, M.; Blumenthal, E.Z. The influence of varying the number of characters per row on the accuracy and reproducibility of the ETDRS visual acuity chart. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.B. The good (logMAR), the bad (Snellen) and the ugly (BCVA, number of letters read) of visual acuity measurement. Ophthalmic Physiol. Opt. 2016, 36, 355–358. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Surgical Period | Data Source | N | Follow-Up Time | PE (%) | |||
|---|---|---|---|---|---|---|---|---|
| ≤±0.5 D | ≤±1.0 D | >1.0 D | ||||||
| Studies published prior to 2010 | Lundstrӧm et al., 2002 [21] | 1992–2000 | Swedish National Cataract Register | 405,149 1 | - | - | 79.2 | 13–28% |
| Murphy et al., 2002 [10] | 1996–1999 | Teaching hospital, England | 1676 2 | 3 weeks 3 | 44.6 | 72.3 | ||
| Kugelberg and Lundstrӧm, 2008 [11] | 2000–2005 | Swedish National Cataract Register | 23,244 4 | - | 58.4 | 83.8 | ||
| Gale et al., 2009 [20] | 2003–2006 | Single NHS center, England | 4806 5 | ~4 weeks | - | 79.7–87.0 | ||
| Studies published after 2010 | Hahn et al., 2011 [23] | 2007–2008 | Seven private practices, Germany | 1553 1 | 3 months | 80.3 | 97.3 | 3–10% |
| Jivrajka et al., 2012 [26] | 2010 | Single center, USA | 250 2,4 | 6–8 weeks | 61.2 | 89.6 | ||
| Aristodemou et al., 2011 [25] | 2005–2010 | Single NHS center, England | 1867 4 | ≥4 weeks | 74.5 | 95.9 | ||
| Behndig et al., 2012 [22] | 2008–2010 | Swedish National Cataract Register | 17,056 2 | 1–2 months | 71.4 | 92.7 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoramnia, R.; Auffarth, G.; Łabuz, G.; Pettit, G.; Suryakumar, R. Refractive Outcomes after Cataract Surgery. Diagnostics 2022, 12, 243. https://doi.org/10.3390/diagnostics12020243
Khoramnia R, Auffarth G, Łabuz G, Pettit G, Suryakumar R. Refractive Outcomes after Cataract Surgery. Diagnostics. 2022; 12(2):243. https://doi.org/10.3390/diagnostics12020243
Chicago/Turabian StyleKhoramnia, Ramin, Gerd Auffarth, Grzegorz Łabuz, George Pettit, and Rajaraman Suryakumar. 2022. "Refractive Outcomes after Cataract Surgery" Diagnostics 12, no. 2: 243. https://doi.org/10.3390/diagnostics12020243
APA StyleKhoramnia, R., Auffarth, G., Łabuz, G., Pettit, G., & Suryakumar, R. (2022). Refractive Outcomes after Cataract Surgery. Diagnostics, 12(2), 243. https://doi.org/10.3390/diagnostics12020243