
Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality

 ,
,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility
2.2. Statistical Methods and Ethics
3. Results
3.1. Descriptive Data
3.2. Histochemical Comparison Analisys between the Two Groups
3.3. Radiological Comparison Analisys between the Two Groups
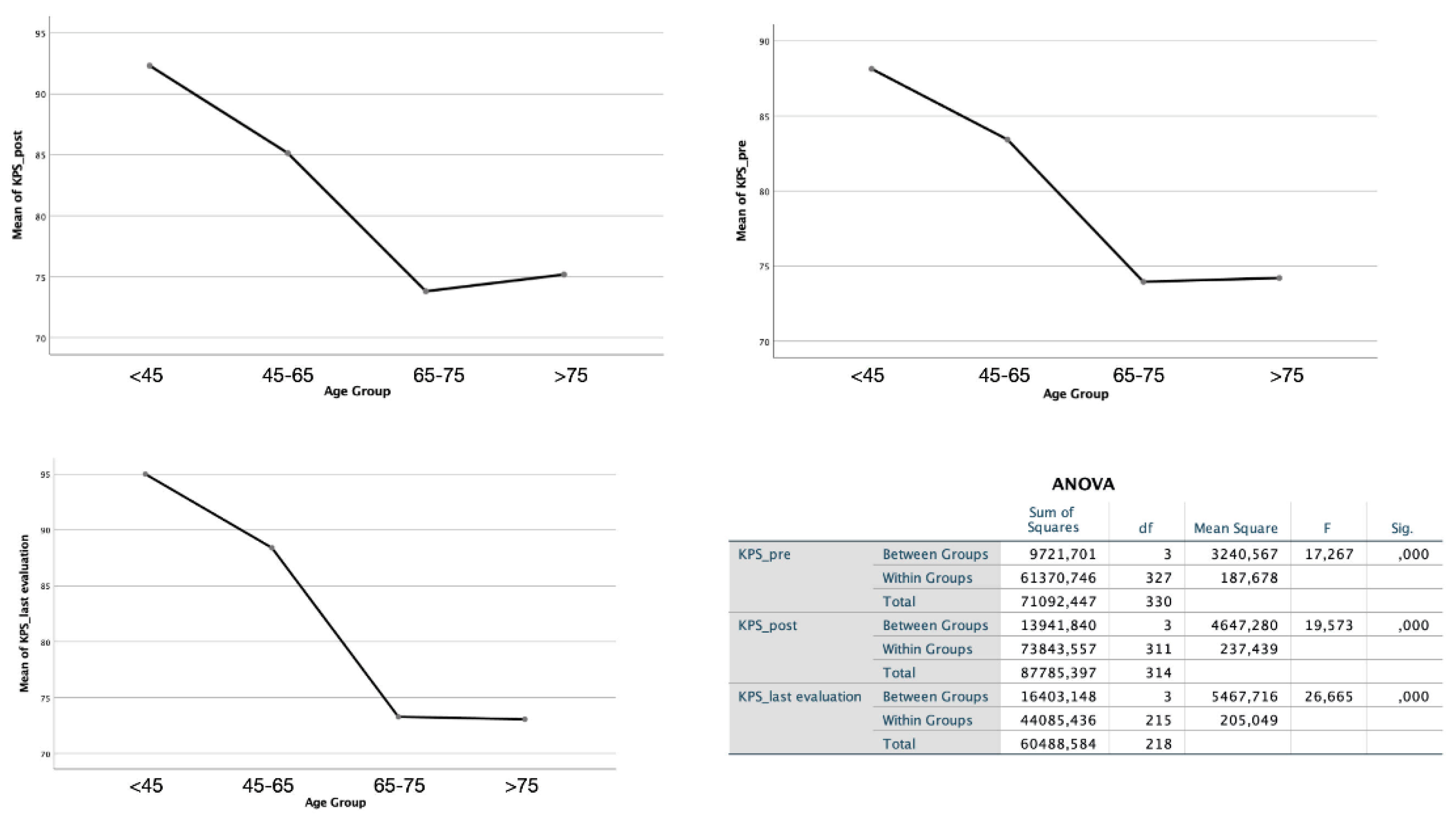
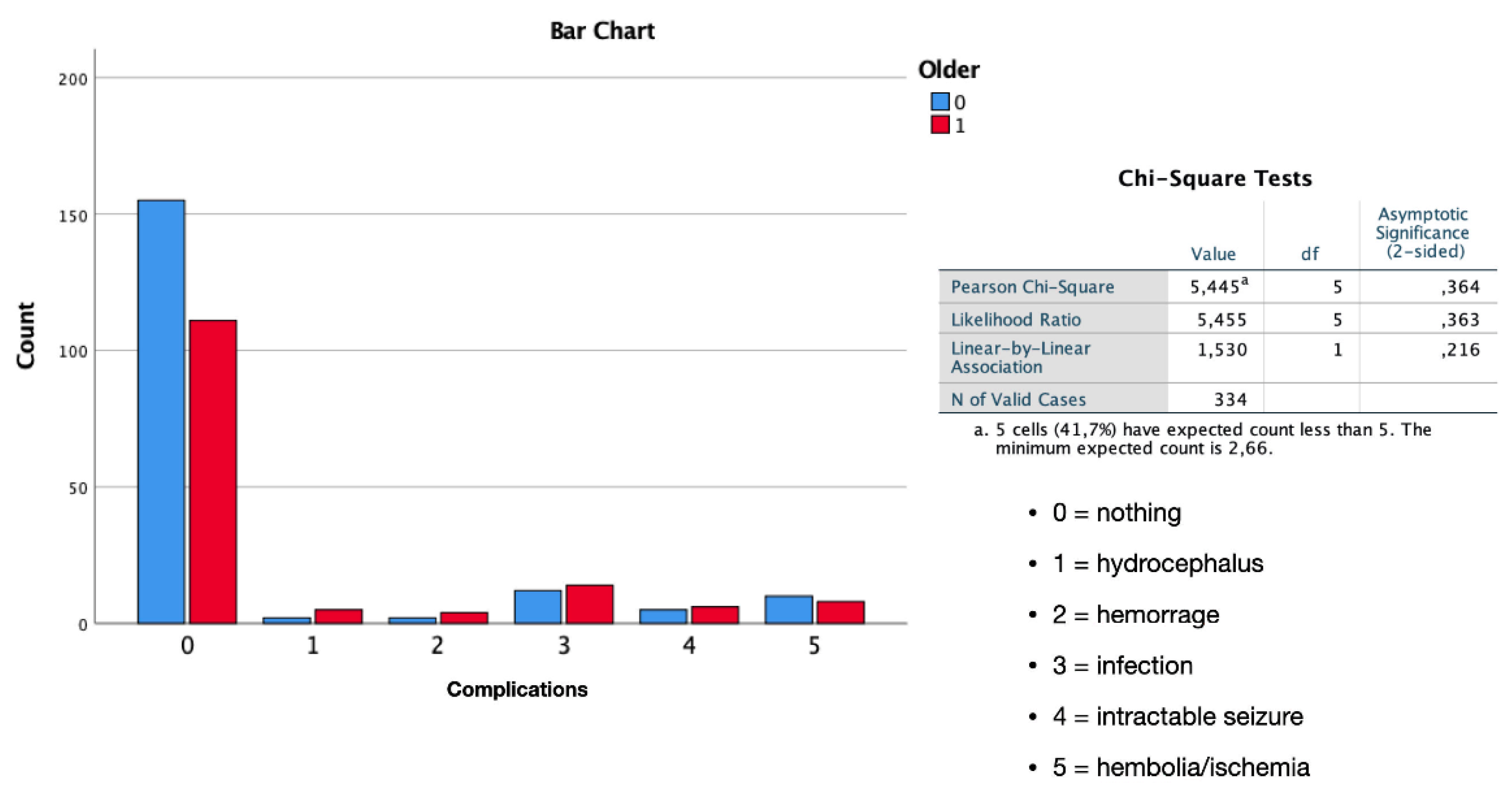
3.4. Outcome Data and Main Results
4. Discussion
Strengths, Limitations and Further Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eseonu, C.; Vivas-Buitrago, T.; Quiñones-Hinojosa, A. Meningiomas in the elderly. Handb. Clin. Neurol. 2020, 169, 261–271. [Google Scholar] [CrossRef]
- Claus, E.B.; Bondy, M.L.; Schildkraut, J.M.; Wiemels, J.L.; Wrensch, M.; Black, P.M. Epidemiology of Intracranial Meningioma. Neurosurgery 2005, 57, 1088–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmer, M.; Seibl-Leven, M.; Wittenstein, K.; Grau, S.; Stavrinou, P.; Röhn, G.; Krischek, B.; Goldbrunner, R. Long-Term Outcome and Health-Related Quality of Life of Elderly Patients After Meningioma Surgery. World Neurosurg. 2019, 125, e697–e710. [Google Scholar] [CrossRef]
- Awad, I.A.; Kalfas, I.; Hahn, J.F.; Little, J.R. Intracranial meningiomas in the aged: Surgical outcome in the era of computed tomography. Neurosurgery 1989, 24, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.Y.; Zheng, C.H.; Tang Li Su, X.Y.; Lu, G.H.; Zhang, C.Y.; Xiao, S.W.; Tan, Y.F. Intracranial meningioma surgery in the elderly (over 65 years): Prognostic factors and outcome. Acta Neurochir. 2015, 157, 1549–1557, Discussion 1557. [Google Scholar] [CrossRef]
- Soyalp, C.; Yuzkat, N.; Kilic, M.; Akyol, M.E.; Demir, C.Y.; Gulhas, N. Operative and prognostic parameters associated with elective versus emergency surgery in a retrospective cohort of elderly patients. Aging Clin. Exp. Res. 2019, 31, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Konglund, A.; Rogne, S.G.; Lund-Johansen, M.; Scheie, D.; Helseth, E.; Meling, T.R. Outcome following surgery for intracranial meningiomas in the aging. Acta Neurol. Scand. 2013, 127, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Bateman, B.T.; Pile-Spellman, J.; Gutin, P.H.; Berman, M.F. Meningioma resection in the elderly: Nationwide inpatient sample, 1998–2002. Neurosurgery 2005, 57, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Ekşi, M.Ş.; Canbolat, Ç.; Akbaş, A.; Özmen, B.B.; Akpınar, E.; Usseli, M.İ.; Güngör, A.; Güdük, M.; Hacıhanefioğlu, M.; Erşen Danyeli, A.; et al. Elderly Patients with Intracranial Meningioma: Surgical Considerations in 228 Patients with a Comprehensive Analysis of the Literature. World Neurosurg. 2019, 132, e350–e365. [Google Scholar] [CrossRef]
- World Health Organisation. 10 Facts on Ageing and the Life Course. 2012. Available online: http://www.who.int/features/factfiles/ageing/ageing_facts/en/index.html (accessed on 2 February 2014).
- Knuf, K.M.; Maani, C.V.; Cummings, A.K. Clinical agreement in the American Society of Anesthesiologists physical status classification. Perioper. Med. 2018, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Bir, S.C.; Konar, S.; Maiti, T.K.; Guthikonda, B.; Nanda, A. Surgical Outcomes and Predictors of Recurrence in Elderly Patients with Meningiomas. World Neurosurg. 2016, 90, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Schul, D.B.; Wolf, S.; Krammer, M.J.; Landscheidt, J.F.; Tomasino, A.; Lumenta, C.B. Meningioma surgery in the elderly: Outcome and validation of 2 proposed grading score systems. Neurosurgery 2012, 70, 555–565. [Google Scholar] [CrossRef]
- Cornu, P.; Chatellier, G.; Dagreou, F.; Clemenceau, S.; Foncin, J.-F.; Rivierez, M.; Philippon, J. Intracranial meningiomas in elderly patients. Acta Neurochir. 1990, 102, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Slot, K.M.; Peters, J.V.M.; Vandertop, W.P.; Verbaan, D.; Peerdeman, S.M. Meningioma surgery in younger and older adults: Patient profile and surgical outcomes. Eur. Geriatr. Med. 2017, 9, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Packer, R.J. The 2021 WHO Classification of Tumors of the Central Nervous System: Clinical implications. Neuro-Oncology 2021, 23, 1215–1217. [Google Scholar] [CrossRef]
- Armocida, D.; Frati, A.; Salvati, M.; Santoro, A.; Pesce, A. Is Ki-67 index overexpression in IDH wild type glioblastoma a predictor of shorter Progression Free survival? A clinical and Molecular analytic investigation. Clin. Neurol. Neurosurg. 2020, 198, 106126. [Google Scholar] [CrossRef]
- Armocida, D.; Pesce, A.; Frati, A.; Santoro, A.; Salvati, M. EGFR amplification is a real independent prognostic impact factor between young adults and adults over 45yo with wild-type glioblastoma? J. Neuro-Oncol. 2019, 146, 275–284. [Google Scholar] [CrossRef]
- Mandel, M.; Li, Y.; Figueiredo, E.G.; Teixeira, M.J.; Steinberg, G.K. Presurgical Planning with Open-Source Horos Software for Superficial Brain Arteriovenous Malformations. World Neurosurg. 2021, 157, 3–12. [Google Scholar] [CrossRef]
- Armocida, D.; Pesce, A.; Frati, A.; Miscusi, M.; Paglia, F.; Raco, A. Pneumoventricle of Unknown Origin: A Personal Experience and Literature Review of a Clinical Enigma. World Neurosurg. 2019, 122, 661–664. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Italy Collaborators. Italy’s health performance, 1990–2017: Findings from the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e645–e657. [Google Scholar] [CrossRef]
- Black, P.; Kathiresan, S.; Chung, W. Meningioma surgery in the elderly: A case-control study assessing morbidity and mortality. Acta Neurochir. 1998, 140, 1013–1016, Discussion 1016–1017. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, R.; Katiyar, V.; Garg, K.; Kasliwal, M.; Chandra, P.S.; Kale, S.S. Comparison of outcomes of surgery for intracranial meningioma in elderly and young patients—A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2021, 207, 106772. [Google Scholar] [CrossRef]
- Ahmeti, H.; Borzikowsky, C.; Hollander, D.; Röcken, C.; Jansen, O.; Synowitz, M.; Mehdorn, M.H. Risks and neurological benefits of meningioma surgery in elderly patients compared to young patients. J. Neuro-Oncol. 2021, 154, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Amano, T.; Nakamizo, A.; Michiwaki, Y.; Matsuo, S.; Fujioka, Y.; Nagata, S. Surgical outcome in elderly patients with intracranial meningioma. J. Clin. Neurosci. 2018, 56, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Brokinkel, B.; Holling, M.; Spille, D.C.; Hess, K.; Sauerland, C.; Bleimüller, C.; Paulus, W.; Wölfer, J.; Stummer, W. Surgery for meningioma in the elderly and long-term survival: Comparison with an age- and sex-matched general population and with younger patients. J. Neurosurg. 2017, 126, 1201–1211. [Google Scholar] [CrossRef] [Green Version]
- Poon, M.; Fung, L.H.-K.; Pu, J.K.-S.; Leung, G.K.-K. Outcome of elderly patients undergoing intracranial meningioma resection—A systematic review and meta-analysis. Br. J. Neurosurg. 2013, 28, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, J.; Takahashi, M.; Idei, M.; Nakano, Y.; Soejima, Y.; Akiba, D.; Kitagawa, T.; Ueta, K.; Miyaoka, R.; Nishizawa, S. Clinical features and surgical management of intracranial meningiomas in the elderly. Oncol. Lett. 2017, 14, 909–917. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, G.; Roperto, R.; Caroli, E.; Crispo, F.; Ferrante, L. Thirty-seven cases of intracranial meningiomas in the ninth decade of life: Our experience and review of the literature. Neurosurgery 2005, 56, 956–961. [Google Scholar]
- Roser, F.; Ebner, F.; Ritz, R.; Samii, M.; Tatagiba, M.; Nakamura, M. Management of skull based meningiomas in the elderly patient. J. Clin. Neurosci. 2007, 14, 224–228. [Google Scholar] [CrossRef]
- Guo, S.; Gerganov, V.; Giordano, M.; Samii, A.; Samii, M. Elderly Patients with Frontobasal and Suprasellar Meningiomas: Safety and Efficacy of Tumor Removal via Frontolateral Approach. World Neurosurg. 2020, 135, e452–e458. [Google Scholar] [CrossRef]
- Zhao, X.; Zhao, D.; Wu, Y.; Gao, W.; Cui, H.; Wang, Y.; Nakaji, P.; Bao, Y. Meningioma in the elderly: Characteristics, prognostic factors, and surgical strategy. J. Clin. Neurosci. 2018, 56, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Armocida, D.; Marzetti, F.; Pesce, A.; Caporlingua, A.; D’Angelo, L.; Santoro, A. Purely Meningeal Intracranial Relapse of Melanoma Brain Metastases After Surgical Resection and Immunotherapy as a Unique Disease Progression Pattern: Our Experience and Review of the Literature. World Neurosurg. 2019, 134, 150–154. [Google Scholar] [CrossRef]
- Kolakshyapati, M.; Ikawa, F.; Abiko, M.; Mitsuhara, T.; Kinoshita, Y.; Takeda, M.; Kurisu, K.; Alumni Association Group of the Department of Neurosurgery at Hiroshima University. Multivariate risk factor analysis and literature review of postoperative deterioration in Karnofsky Performance Scale score in elderly patients with skull base meningioma. Neurosurg. Focus 2018, 44, E14. [Google Scholar] [CrossRef] [PubMed]
- Karhade, A.V.; Fandino, L.; Gupta, S.; Cote, D.J.; Iorgulescu, J.B.; Broekman, M.L.; Aglio, L.S.; Dunn, I.F.; Smith, T.R. Impact of operative length on post-operative complications in meningioma surgery: A NSQIP analysis. J. Neuro-Oncol. 2016, 131, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Caroli, M.; Locatelli, M.; Prada, F.; Beretta, F.; Martinelli-Boneschi, F.; Campanella, R.; Arienta, C. Surgery for intracranial menin- giomas in the elderly: A clinical-radiological grading system as a predictor of outcome. J. Neurosurg. 2005, 102, 290–294. [Google Scholar] [CrossRef]
- Czernicki, T. Surgical Management of Intracranial Meningiomas in the Elderly: Early and Long-term Outcomes. Clin. Interv. Aging 2020, 15, 2439–2451. [Google Scholar] [CrossRef]
- Ikawa, F.; Kinoshita, Y.; Takeda, M.; Saito, T.; Yamaguchi, S.; Yamasaki, F.; Iida, K.; Sugiyama, K.; Arita, K.; Kurisu, K. Review of Current Evidence Regarding Surgery in Elderly Patients with Meningioma. Neurol. Med.-Chir. 2017, 57, 521–533. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Populations (340) | Group <65 (188) | Group Elderly (152) | p-Value | |
|---|---|---|---|---|
| Sex | F = 142 | F = 96 | 0.09 | |
| Clinical | Hospitalization | 15.79 | 20.26 | 0.19 |
| Follow-up | 46.76 DS = 14.83 | 48.89 SD = 14.77 | 0.639 | |
| Cardiopathy | 29/140 = 20.71% | 79/116 = 68.1% | <0.01 | |
| Smoke habit | 52/152 | 46/115 | 0.199 | |
| Localization | 0.856 | |||
| Radiological | Multiple | 8/188 | 5/145 | 0.434 |
| Diameter means | 4.42 | 4.34 | 0.693 | |
| Volume means | 36.55 | 35.91 | 0.893 | |
| Edema V means | 27.99 | 28.78 | 0.902 | |
| Ki67 means | 5.03 SD= 6.34 | 6.58 SD = 6.43 | 0.847 | |
| Biological | Mitotic index 10 HPF | 1.26 SD = 2 | 1.67 SD = 2.12 | 0.372 |
| PR + | 27/175 = 15.42% | 11/133 = 8.3% | 0.079–0.041 | |
| High grading (III-IV) | 4/188 = 2.13% | 4/152 = 2.63% | 1 | |
| Recurrence | 10.5% | 12.77% | 0.598 | |
| Simpson Grading | 0.611 | |||
| Outcome | Simpson Grade I | 0.138 | ||
| Progression Malignant | 3/188 | 2/145 | 0.599 | |
| KPS pre | 11 | 42 | <0.01 | |
| KPS post | 14 | 41 | <0.01 | |
| KPS last | 7 | 24 | <0.01 | |
| Complications post-operative | 0.217 | |||
| Ischemia post | 10/186 = 5.4% | 8/148 = 5.4% | 1 | |
| Infections post | 12/186 = 6.45% | 14/148 = 9.45% | 0.314 | |
| Hemorrhage post | 2/186 = 1.1% | 4/148 = 2.7% | 0.41 | |
| Seizure post | 22/186 | 19/145 | 0.364 | |
| Complications Rate | 31/187 = 16.6% | 37/148 = 25% | 0.075–0.039 | |
| Mortality | 5/188 = 2.6% | 25/152 = 16.44% | <0.01 |
| Populations | Group 1 (<45) 44 pts | Group 2 (45–65) 143 pts | Group 3 (65–75) 94 pts | Group 4 (>75) 58 pts | p-Value |
|---|---|---|---|---|---|
| Diameter mean | 4.39 SD = 1.75 | 4.43 SD = 1.88 | 4.31 SD = 1.73 | 4.38 SD = 1.44 | 0.971 |
| Volume mean | 35.70 SD = 29.58 | 36.80 SD = 41.22 | 37.87 SD = 37.46 | 32.96 SD = 28 | 0.919 |
| Edema vol mean | 23.63 SD = 35.78 | 29.25 SD = 47.97 | 24.75 SD = 43.85 | 35.23 SD = 53.94 | 0.701 |
| Complicances | 0.209 | ||||
| Mortality rate | 0 | 5 = 3.5% | 13 = 13.8% | 12 = 20.7% | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armocida, D.; Arcidiacono, U.A.; Palmieri, M.; Pesce, A.; Cofano, F.; Picotti, V.; Salvati, M.; D’Andrea, G.; Garbossa, D.; Santoro, A.; et al. Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality. Diagnostics 2022, 12, 351. https://doi.org/10.3390/diagnostics12020351
Armocida D, Arcidiacono UA, Palmieri M, Pesce A, Cofano F, Picotti V, Salvati M, D’Andrea G, Garbossa D, Santoro A, et al. Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality. Diagnostics. 2022; 12(2):351. https://doi.org/10.3390/diagnostics12020351
Chicago/Turabian StyleArmocida, Daniele, Umberto Aldo Arcidiacono, Mauro Palmieri, Alessandro Pesce, Fabio Cofano, Veronica Picotti, Maurizio Salvati, Giancarlo D’Andrea, Diego Garbossa, Antonio Santoro, and et al. 2022. "Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality" Diagnostics 12, no. 2: 351. https://doi.org/10.3390/diagnostics12020351
APA StyleArmocida, D., Arcidiacono, U. A., Palmieri, M., Pesce, A., Cofano, F., Picotti, V., Salvati, M., D’Andrea, G., Garbossa, D., Santoro, A., & Frati, A. (2022). Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality. Diagnostics, 12(2), 351. https://doi.org/10.3390/diagnostics12020351