
Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics and Study Design
2.2. Liver Fat Content
2.2.1. MRS
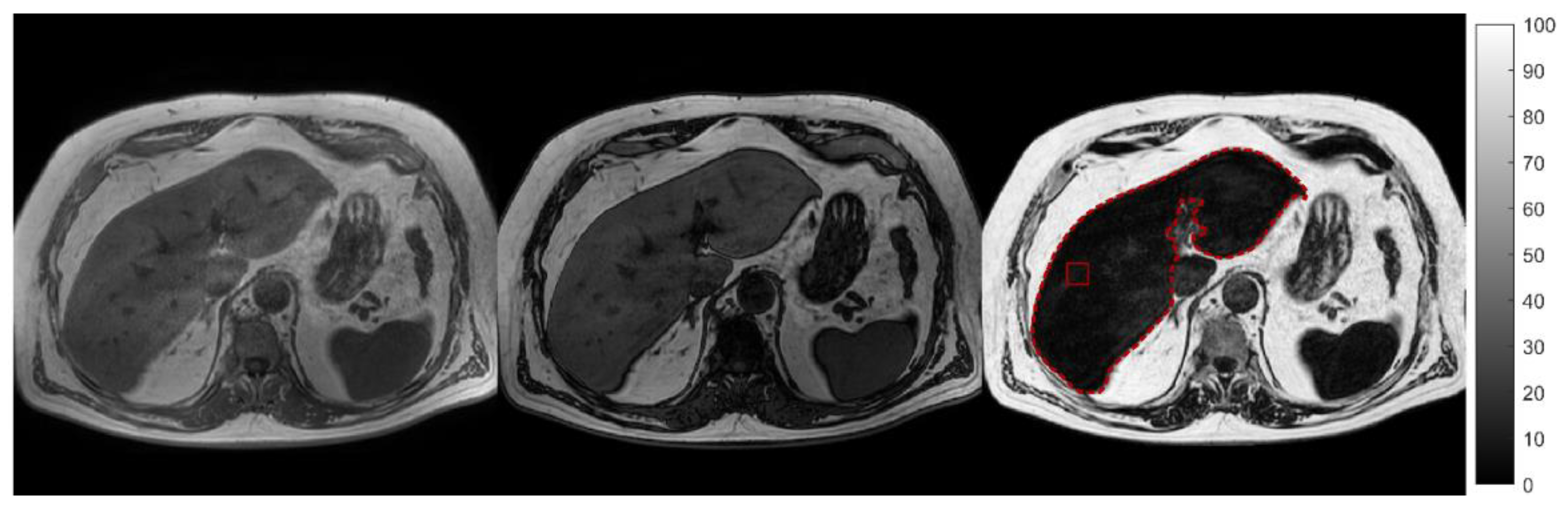
2.2.2. MRI
2.3. Statistical Analysis
2.3.1. Standard Analysis of Liver Fat
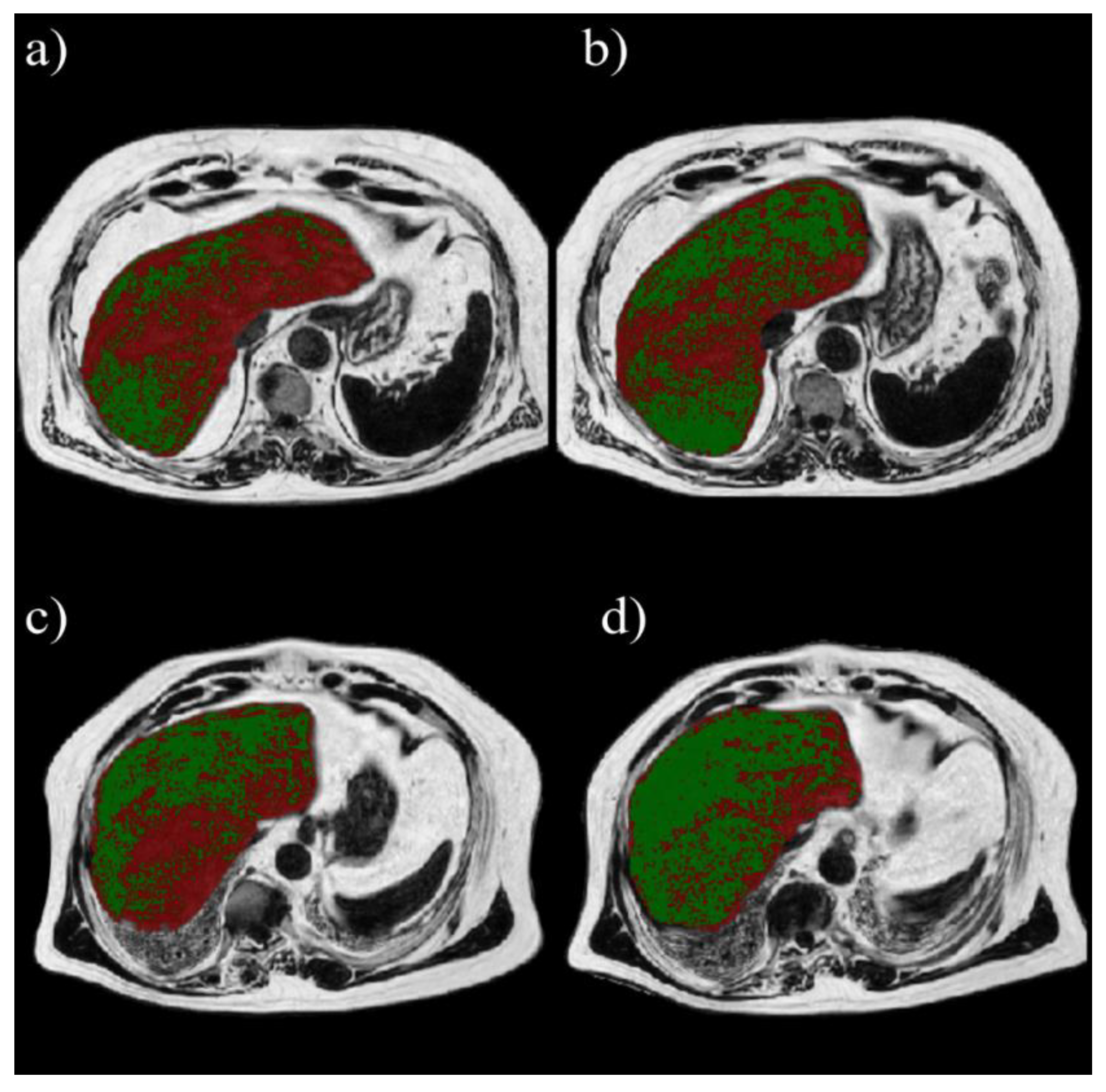
2.3.2. Volumetric Analysis of Liver Fat
3. Results
3.1. Anthropometrics and Metabolic Parameters
3.2. Correlation and Agreement of Liver Fat Content Measurements by MRI and MRS
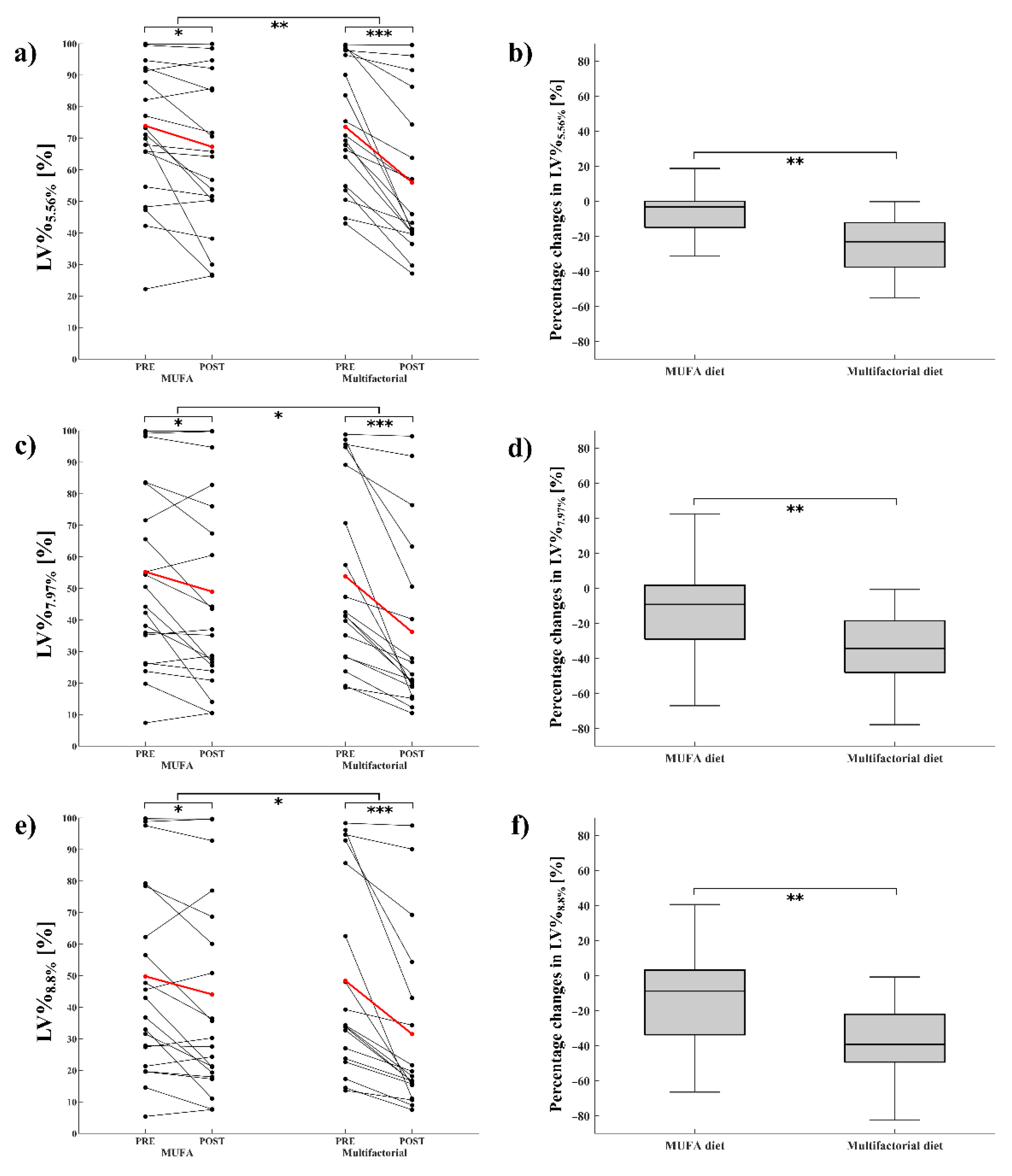
3.3. Standard Analysis of Liver Fat
3.4. Volumetric Analysis of Liver Fat
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anstee, Q.M.; McPherson, S.; Day, C.P. How Big a Problem Is Non-Alcoholic Fatty Liver Disease? BMJ 2011, 343, d3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazlehurst, J.M.; Woods, C.; Marjot, T.; Cobbold, J.F.; Tomlinson, J.W. Non-Alcoholic Fatty Liver Disease and Diabetes. Metabolism 2016, 65, 1096–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, D.; Thava, V.R.; Scott, B.B. Diagnosis of Fatty Liver Disease: Is Biopsy Necessary? Eur. J. Gastroenterol. Hepatol. 2003, 15, 539–543. [Google Scholar] [CrossRef] [PubMed]
- El-Badry, A.M.; Breitenstein, S.; Jochum, W.; Washington, K.; Paradis, V.; Rubbia-Brandt, L.; Puhan, M.A.; Slankamenac, K.; Graf, R.; Clavien, P.-A. Assessment of Hepatic Steatosis by Expert Pathologists: The End of a Gold Standard. Ann. Surg. 2009, 250, 691–697. [Google Scholar] [CrossRef]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Ultrasound Q. 2016, 32, 94–107. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- Reeder, S.B.; Hu, H.H.; Sirlin, C.B. Proton Density Fat-Fraction: A Standardized Mr-Based Biomarker of Tissue Fat Concentration. J. Magn. Reson. Imaging 2012, 36, 1011–1014. [Google Scholar] [CrossRef]
- Lee, S.S. Radiologic Evaluation of Nonalcoholic Fatty Liver Disease. WJG 2014, 20, 7392. [Google Scholar] [CrossRef]
- Kang, B.; Kim, M.; Song, S.; Jun, D.W.; Jang, K. Feasibility of Modified Dixon MRI Techniques for Hepatic Fat Quantification in Hepatic Disorders: Validation with MRS and Histology. BJR 2017, 20170378. [Google Scholar] [CrossRef]
- Kim, H.; Taksali, S.E.; Dufour, S.; Befroy, D.; Goodman, T.R.; Petersen, K.F.; Shulman, G.I.; Caprio, S.; Constable, R.T. Comparative MR Study of Hepatic Fat Quantification Using Single-Voxel Proton Spectroscopy, Two-Point Dixon and Three-Point IDEAL. Magn. Reson. Med. 2008, 59, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Dixon, W.T. Simple Proton Spectroscopic Imaging. Radiology 1984, 153, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Glover, G.H. Multipoint Dixon Technique for Water and Fat Proton and Susceptibility Imaging. J. Magn. Reson. Imaging 1991, 1, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Glover, G.H.; Schneider, E. Three-Point Dixon Technique for True Water/Fat Decomposition WithB0 Inhomogeneity Correction. Magn. Reson. Med. 1991, 18, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Reeder, S.B.; Pineda, A.R.; Wen, Z.; Shimakawa, A.; Yu, H.; Brittain, J.H.; Gold, G.E.; Beaulieu, C.H.; Pelc, N.J. Iterative Decomposition of Water and Fat with Echo Asymmetry and Least-Squares Estimation (IDEAL): Application with Fast Spin-Echo Imaging. Magn. Reson. Med. 2005, 54, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Reeder, S.B.; Wen, Z.; Yu, H.; Pineda, A.R.; Gold, G.E.; Markl, M.; Pelc, N.J. Multicoil Dixon Chemical Species Separation with an Iterative Least-Squares Estimation Method. Magn. Reson. Med. 2004, 51, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Chartampilas, E. Imaging of Nonalcoholic Fatty Liver Disease and Its Clinical Utility. Hormones 2018, 17, 69–81. [Google Scholar] [CrossRef] [Green Version]
- Berglund, J.; Ahlström, H.; Johansson, L.; Kullberg, J. Two-Point Dixon Method with Flexible Echo Times: Unconstrained Two-Point Dixon. Magn. Reson. Med. 2011, 65, 994–1004. [Google Scholar] [CrossRef]
- Satkunasingham, J.; Nik, H.H.; Fischer, S.; Menezes, R.; Selzner, N.; Cattral, M.; Grant, D.; Jhaveri, K. Can Negligible Hepatic Steatosis Determined by Magnetic Resonance Imaging-Proton Density Fat Fraction Obviate the Need for Liver Biopsy in Potential Liver Donors? Satkunasingham et Al. Liver Transpl. 2018, 24, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Van Werven, J.R.; Marsman, H.A.; Nederveen, A.J.; Smits, N.J.; Ten Kate, F.J.; Van Gulik, T.M.; Stoker, J. Assessment of Hepatic Steatosis in Patients Undergoing Liver Resection: Comparison of US, CT, T1-Weighted Dual-Echo MR Imaging, and Point-Resolved 1 H MR Spectroscopy. Radiology 2010, 256, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.-Z.; Gan, Y.-G.; Zhou, J.-L.; Liu, J.-Q.; Cao, W.-G.; Cheng, S.-M.; Bai, D.-M.; Wang, M.-Z.; Gao, F.-Q.; Zhou, S.-M. Accuracy of Multi-Echo Dixon Sequence in Quantification of Hepatic Steatosis in Chinese Children and Adolescents. WJG 2019, 25, 1513–1523. [Google Scholar] [CrossRef]
- Hayashi, T.; Saitoh, S.; Takahashi, J.; Tsuji, Y.; Ikeda, K.; Kobayashi, M.; Kawamura, Y.; Fujii, T.; Inoue, M.; Miyati, T.; et al. Hepatic Fat Quantification Using the Two-Point Dixon Method and Fat Color Maps Based on Non-Alcoholic Fatty Liver Disease Activity Score: Hepatic Fat Quantification Using MRI. Hepatol. Res. 2017, 47, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Yurdaisik, I.; Nurili, F. Accuracy of Multi-Echo Dixon Sequence in Quantification of Hepatic Steatosis. Cureus 2020, 12, e7103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bril, F.; Cusi, K. Management of Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Call to Action. Diabetes Care 2017, 40, 419–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzetto, L.; Prinster, A.; Annuzzi, G.; Costagliola, L.; Mangione, A.; Vitelli, A.; Mazzarella, R.; Longobardo, M.; Mancini, M.; Vigorito, C.; et al. Liver Fat Is Reduced by an Isoenergetic MUFA Diet in a Controlled Randomized Study in Type 2 Diabetic Patients. Diabetes Care 2012, 35, 1429–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Pepa, G.; Vetrani, C.; Brancato, V.; Vitale, M.; Monti, S.; Annuzzi, G.; Lombardi, G.; Izzo, A.; Tommasone, M.; Cipriano, P.; et al. Effects of a Multifactorial Ecosustainable Isocaloric Diet on Liver Fat in Patients with Type 2 Diabetes: Randomized Clinical Trial. BMJ Open Diab. Res. Care 2020, 8, e001342. [Google Scholar] [CrossRef]
- Provencher, S.W. Automatic Quantitation of Localizedin Vivo1H Spectra with LCModel. NMR Biomed. 2001, 14, 260–264. [Google Scholar] [CrossRef]
- Weis, J.; Kullberg, J.; Ahlström, H. Multiple Breath-Hold Proton Spectroscopy of Human Liver at 3T: Relaxation Times and Concentrations of Glycogen, Choline, and Lipids. J. Magn. Reson. Imaging 2018, 47, 410–417. [Google Scholar] [CrossRef]
- Szczepaniak, L.S.; Nurenberg, P.; Leonard, D.; Browning, J.D.; Reingold, J.S.; Grundy, S.; Hobbs, H.H.; Dobbins, R.L. Magnetic Resonance Spectroscopy to Measure Hepatic Triglyceride Content: Prevalence of Hepatic Steatosis in the General Population. Am. J. Physiol. Endocrinol. Metab. 2005, 288, E462–E468. [Google Scholar] [CrossRef] [Green Version]
- Idilman, I.S.; Keskin, O.; Celik, A.; Savas, B.; Halil Elhan, A.; Idilman, R.; Karcaaltincaba, M. A Comparison of Liver Fat Content as Determined by Magnetic Resonance Imaging-Proton Density Fat Fraction and MRS versus Liver Histology in Non-Alcoholic Fatty Liver Disease. Acta Radiol. 2016, 57, 271–278. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Middleton, M.S.; Behling, C.; Newton, K.P.; Awai, H.I.; Paiz, M.N.; Lam, J.; Hooker, J.C.; Hamilton, G.; Fontanesi, J.; et al. Magnetic Resonance Imaging and Liver Histology as Biomarkers of Hepatic Steatosis in Children with Nonalcoholic Fatty Liver Disease: Clinical observations in hepatology. Hepatology 2015, 61, 1887–1895. [Google Scholar] [CrossRef]
- Bhat, V. Quantification of Liver Fat with MDIXON Magnetic Resonance Imaging, Comparison with the Computed Tomography and the Biopsy. JCDR 2017, 11, TC06–TC10. [Google Scholar] [CrossRef]
- Korpraphong, P.; Somsap, K.; Saiviroonporn, P.; Pongpaibul, A.; Charatcharoenwitthaya, P. Semi-Quantification of Hepatic Steatosis in Patients with Chronic Liver Disease Using the Multiecho Two-Point Dixon Technique with Histopathology as the Reference Standard. Hong Kong J. Radiol. 2015, 18, 4–10. [Google Scholar] [CrossRef]
- Hui, S.C.N.; So, H.; Chan, D.F.Y.; Wong, S.K.H.; Yeung, D.K.W.; Ng, E.K.W.; Chu, W.C.W. Validation of Water-Fat MRI and Proton MRS in Assessment of Hepatic Fat and the Heterogeneous Distribution of Hepatic Fat and Iron in Subjects with Non-Alcoholic Fatty Liver Disease. Eur. J. Radiol. 2018, 107, 7–13. [Google Scholar] [CrossRef]
- Meisamy, S.; Hines, C.D.G.; Hamilton, G.; Sirlin, C.B.; McKenzie, C.A.; Yu, H.; Brittain, J.H.; Reeder, S.B. Quantification of Hepatic Steatosis with T1-Independent, T2*-Corrected MR Imaging with Spectral Modeling of Fat: Blinded Comparison with MR Spectroscopy. Radiology 2011, 258, 767–775. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Ye, J.; Cao, Y.-H.; Zhang, R.; Han, X.-F.; Zou, L.-L.; Kuang, L.; Zhang, J.; Lian, H.; Xia, J.-X.; et al. Association of [1H]-MRS Quantified Liver Fat Content with Glucose Metabolism Status. Diabetol. Metab. Syndr. 2020, 12, 51. [Google Scholar] [CrossRef]
- Middleton, M.S.; Heba, E.R.; Hooker, C.A.; Bashir, M.R.; Fowler, K.J.; Sandrasegaran, K.; Brunt, E.M.; Kleiner, D.E.; Doo, E.; Van Natta, M.L.; et al. Agreement Between Magnetic Resonance Imaging Proton Density Fat Fraction Measurements and Pathologist-Assigned Steatosis Grades of Liver Biopsies From Adults With Nonalcoholic Steatohepatitis. Gastroenterology 2017, 153, 753–761. [Google Scholar] [CrossRef] [Green Version]
- Tanpowpong, N.; Panichyawat, S. Diagnostic Radiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand Comparison of Sonographic Hepatorenal Ratio and the Degree of Hepatic Steatosis in Magnetic Resonance Imaging-Proton Density Fat Fraction. J. Ultrason 2020, 20, 169–175. [Google Scholar] [CrossRef]
- Marušić, M.; Paić, M.; Knobloch, M.; Liberati Pršo, A.-M. NAFLD, Insulin Resistance, and Diabetes Mellitus Type 2. Can. J. Gastroenterol. Hepatol. 2021, 2021, 6613827. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MUFA-Diet (n = 21) | Multifactorial-Diet (n = 18) | |
|---|---|---|
| Sex | ||
| Male | 12 (57%) | 10 (56%) |
| Female | 9 (43%) | 8 (44%) |
| Age (years) | 64 (5) | 64 (6) |
| BMI (kg/m2) | 31 (3) | 32 (4) |
| HbA1c (%) | 6.5 (0.6) | 6.5 (0.4) |
| Diabetes therapy: | ||
| Diet | 5 (24%) | 5 (28%) |
| Glucose lowering drugs | 16 (76%) | 13 (72%) |
| Other drugs: | ||
| Statin | 13 (62%) | 9 (50%) |
| Anti-hypertensive | 19 (90%) | 16 (89%) |
| Anti-platelet | 5 (24%) | 6 (34%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brancato, V.; Della Pepa, G.; Bozzetto, L.; Vitale, M.; Annuzzi, G.; Basso, L.; Cavaliere, C.; Salvatore, M.; Rivellese, A.A.; Monti, S. Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets. Diagnostics 2022, 12, 514. https://doi.org/10.3390/diagnostics12020514
Brancato V, Della Pepa G, Bozzetto L, Vitale M, Annuzzi G, Basso L, Cavaliere C, Salvatore M, Rivellese AA, Monti S. Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets. Diagnostics. 2022; 12(2):514. https://doi.org/10.3390/diagnostics12020514
Chicago/Turabian StyleBrancato, Valentina, Giuseppe Della Pepa, Lutgarda Bozzetto, Marilena Vitale, Giovanni Annuzzi, Luca Basso, Carlo Cavaliere, Marco Salvatore, Angela Albarosa Rivellese, and Serena Monti. 2022. "Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets" Diagnostics 12, no. 2: 514. https://doi.org/10.3390/diagnostics12020514
APA StyleBrancato, V., Della Pepa, G., Bozzetto, L., Vitale, M., Annuzzi, G., Basso, L., Cavaliere, C., Salvatore, M., Rivellese, A. A., & Monti, S. (2022). Evaluation of a Whole-Liver Dixon-Based MRI Approach for Quantification of Liver Fat in Patients with Type 2 Diabetes Treated with Two Isocaloric Different Diets. Diagnostics, 12(2), 514. https://doi.org/10.3390/diagnostics12020514