
Needle Tip Detection Using Ultrasound Probe for Vertical Punctures: A Simulation and Experimental Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Statement
2.2. Detection of the Needle Tip in the Phantom and Animal Experiments
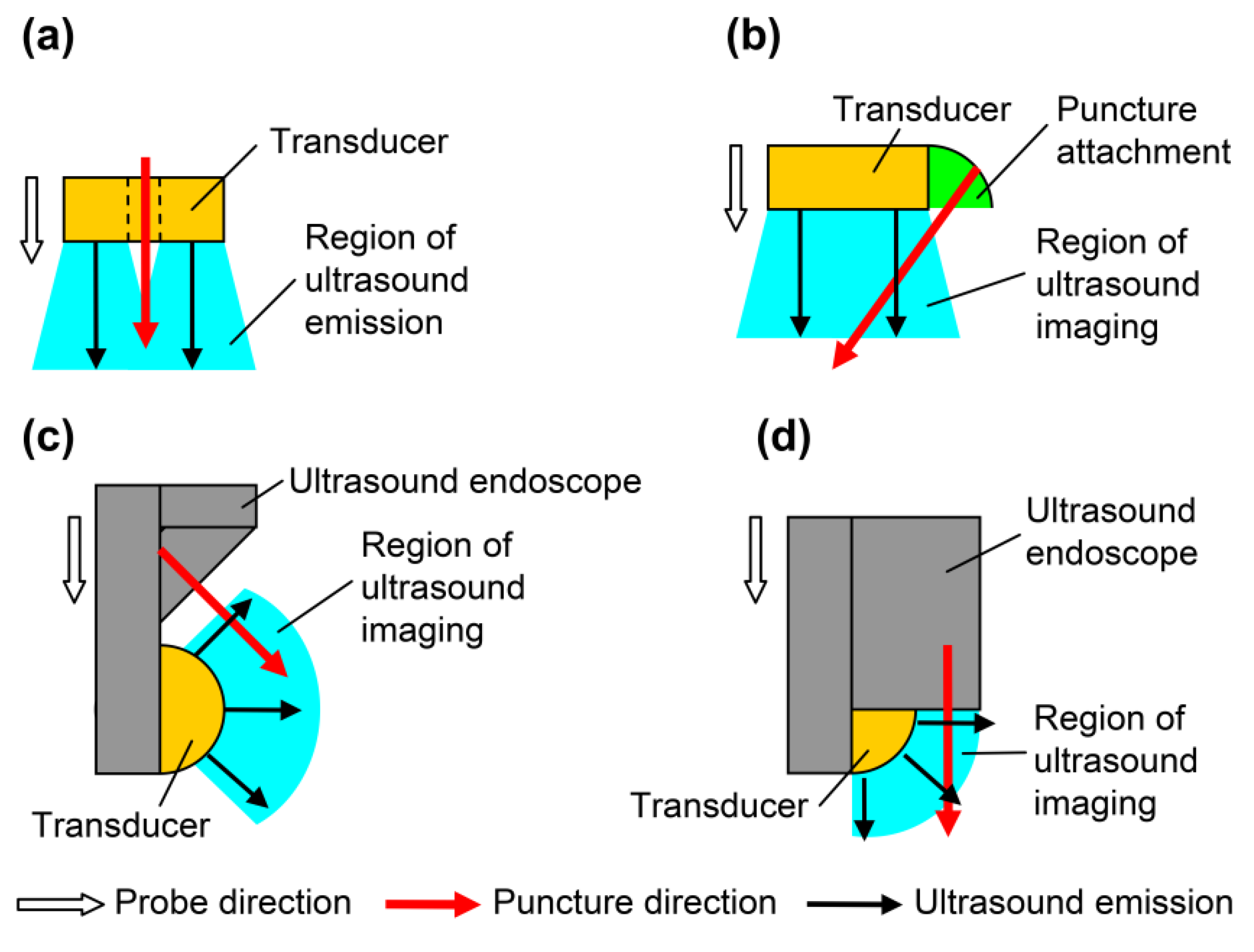
2.2.1. Ultrasound Probes for Vertical Puncture
2.2.2. Needle Tip Detection in Porcine Liver
2.2.3. Needle Tip Detection in Canine Femoral Artery
2.3. Principle of Needle Tip Detection
2.3.1. Basic Model Simulation
2.3.2. Angle of Needle Tip Detection Sensitivity
2.3.3. Needle Tip Width and Length Modification Model
3. Results
3.1. Needle Tip Detection at the Phantom and Animal Experiments
3.1.1. Needle Tip Detection in Porcine Liver
3.1.2. Needle Tip Detection in the Canine Femoral Artery
3.2. Experiments of Needle Tip Detection
3.2.1. Simulation of the Basic Model
3.2.2. Angle of Needle Tip Detection Sensitivity
3.2.3. Needle Tip Width and Length Modification Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berlyne, G.M. Ultrasonics in renal biopsy. Lancet 1961, 1, 750–751. [Google Scholar] [CrossRef]
- Holm, H.H. Interventional ultrasound in Europe. Ultrasound Med. Biol. 1998, 24, 779–791. [Google Scholar] [CrossRef]
- Goldberg, B.B.; Pollack, H.M. Ultrasonic aspiration transducer. Radiology 1972, 102, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Holm, H.H.; Kristensen, J.K.; Rasmussen, S.N.; Northeved, A.; Barlebo, H. Ultrasound as a guide in percutaneous puncture technique. Ultrasonics 1972, 10, 83–86. [Google Scholar] [CrossRef]
- Itoh, K.; Yamanaka, T.; Kasahara, K.; Koike, M.; Nakamura, A.; Hayaski, A.; Kimura, K.; Morioka, Y.; Kawai, T. Definitive diagnosis of pancreatic carcinoma with percutaneous fine needle aspiration biopsy under ultrasonic guidance. Am. J. Gastroenterol. 1979, 71, 469–472. [Google Scholar] [PubMed]
- Rasmussen, S.N.; Holm, H.H.; Kristensen, J.K.; Barlebo, H. Ultrasonically guided liver biopsy. Br. Med. J. 1972, 2, 500–502. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, J.K.; Holm, H.H.; Rasmussen, S.N.; Barlebo, H. Ultrasonically guided percutaneous puncture of renal masses. Scand. J. Urol. Nephrol. 1972, 6, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, J.F. Percutaneous puncture guided by ultrasonic multitransducer scanning. J. Clin. Ultrasound 1977, 5, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, M.; Watanabe, H.; Ohe, H.; Tanaka, S.; Itakura, S.; Date, S. Ultrasonic realtime guidance for percutaneous puncture. J. Clin. Ultrasound 1979, 7, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, B.B.; Beuglet, C.C.; Kurtz, A.B.; Rubin, C.S. Real-time aspiration-biopsy transducer. J. Clin. Ultrasound 1980, 8, 107–112. [Google Scholar] [CrossRef]
- Ohto, M.; Karasawa, E.; Tsuchiya, Y.; Kimura, K.; Saisho, H.; Ono, T.; Okuda, K. Ultrasonically guided percutaneous contrast medium injection and aspiration biopsy using a real-time puncture transducer. Radiology 1980, 136, 171–176. [Google Scholar] [CrossRef] [PubMed]
- McGahan, J.P. The history of interventional ultrasound. J. Ultrasound Med. 2004, 23, 727–741. [Google Scholar] [CrossRef]
- Kida, M.; Araki, M.; Tokunaga, S.; Yamauchi, H.; Okuwaki, K.; Miyazawa, S.; Iwai, T.; Takezawa, M.; Kikuchi, H.; Watanabe, M.; et al. Role of a forward-viewing echoendoscope in fine-needle aspiration. Gastrointest. Interv. 2013, 2, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, I.; Miyahara, R.; Hirooka, Y.; Funasaka, K.; Ohno, E.; Nakamura, M.; Kawashima, H.; Nukaga, A.; Shimoyama, Y.; Goto, H. Forward-viewing versus oblique-viewing echoendoscopes in the diagnosis of upper GI subepithelial lesions with EUS-guided FNA: A prospective, randomized, crossover study. Gastrointest. Endosc. 2015, 82, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Ceroni, L.; Caletti, G. Forward-view endoscopic ultrasound: A systematic review of diagnostic and therapeutic applications. Endosc. Ultrasound 2013, 2, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Fujita, A.; Ryozawa, S.; Tanisaka, Y.; Ogawa, T.; Suzuki, M.; Noguchi, T.; Katsuda, H.; Mizuide, M. Current status of needles in the optimization of endoscopic ultrasound-guided procedures. Diagnostics 2020, 10, 463. [Google Scholar] [CrossRef] [PubMed]
- Gálvez, J.A.; Lin, E.E.; Schwartz, A.J.; Simpao, A.F. Ultrasound-guided vascular access: Visualizing the tip of the needle. Anesthesiology 2016, 125, 396. [Google Scholar] [CrossRef]
- Forgia, D.L.; Fausto, A.; Gatta, G.; Grezia, G.D.; Faggian, A.; Fanizzi, A.; Cutrignelli, D.; Cutrignelli, D.; Dentamaro, R.; Didonna, V.; et al. Elite VABB 13G: A new ultrasound-guided wireless biopsy system for breast lesions. technical characteristics and comparison with respect to traditional core-biopsy 14-16G systems. Diagnostics 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Tanaka, Y.; Shiomi, H.; Kurumi, Y.; Tani, T. Basic properties of ultrasonic probe with a through hole for medical application. Procedia Eng. 2012, 47, 366–369. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Tanaka, K.; Sugiyama, S.; Shiomi, H.; Kurumi, Y.; Tani, T.; Takahashi, O. Basic properties of an ultrasonic probe with a through hole for puncture and detection principle of a puncture needle. Electr. Commun. Jpn. 2014, 97, 67–73. [Google Scholar] [CrossRef]
- Tanaka, Y.; Ohira, K.; Ogura, Y.; Tanaka, K.; Shiomi, H.; Kurumi, Y.; Tani, T. Ultrasonic imaging of medical puncture using array probe. Jpn. J. Appl. Phys. 2014, 53, 07KF26. [Google Scholar] [CrossRef]
- Tanaka, Y.; Ohira, K.; Ogura, Y.; Tanaka, K.; Shiomi, H.; Kurumi, Y.; Tani, T. Ultrasonic imaging of puncturing using linear array probe. IEICE Tech. Rep. 2014, 114, 13–17. [Google Scholar]
- Tanaka, Y.; Ohira, K.; Ogura, Y. Ultrasonic Visualisation Pulse and Continuous Waves. Available online: https://www3.e-kenkyu.com/asj_library/manuscripts/2016/year (accessed on 3 February 2022).
- National Research Council of the National Academies. Guide for the Care and Use of Laboratory Animals, 8th ed.; The National Academies Press: Washington, DC, USA, 2011. Available online: https://grants.nih.gov/grants/olaw/guide-for-the-care-and-use-of-laboratory-animals.pdf (accessed on 14 December 2020).
- Scholten, H.J.; Pourtaherian, A.; Mihajlovic, N.; Korsten, H.H.M.; Bouwman, R.A. Improving needle tip identification during ultrasound-guided procedures in anaesthetic practice. Anaesthesia 2017, 72, 889–904. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, B.B.; Ziskin, M.C. Echo Patterns with an aspiration ultrasonic transducer. Investig. Radiol. 1973, 8, 78–83. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application | Evidence | References |
|---|---|---|
| Amniotic fluid puncture | Kratochwil | [2] |
| Aspiration of body fluids | Goldberg | [3] |
| Puncture of the liver and the pancreas | Holm | [4] |
| Puncture of the pancreas | Itoh | [5] |
| Puncture of the liver | Rasmussen | [6] |
| Biopsy of the kidney | Kristensen | [7] |
| Obtaining fluid or biopsy at amniocentesis, renal cyst aspiration, paracentesis, thoracentesis, kidney, liver masses, pancreas, and breast | Goldberg | [10] |
| Epidural puncture | Our idea | |
| Central venous catheter insertion | Our idea |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, Y.; Tanaka, K.; Shiomi, H.; Kurumi, Y.; Tani, T.; Ogura, Y. Needle Tip Detection Using Ultrasound Probe for Vertical Punctures: A Simulation and Experimental Study. Diagnostics 2022, 12, 527. https://doi.org/10.3390/diagnostics12020527
Tanaka Y, Tanaka K, Shiomi H, Kurumi Y, Tani T, Ogura Y. Needle Tip Detection Using Ultrasound Probe for Vertical Punctures: A Simulation and Experimental Study. Diagnostics. 2022; 12(2):527. https://doi.org/10.3390/diagnostics12020527
Chicago/Turabian StyleTanaka, Yuusuke, Katsuhiko Tanaka, Hisanori Shiomi, Yoshimasa Kurumi, Tohru Tani, and Yukio Ogura. 2022. "Needle Tip Detection Using Ultrasound Probe for Vertical Punctures: A Simulation and Experimental Study" Diagnostics 12, no. 2: 527. https://doi.org/10.3390/diagnostics12020527
APA StyleTanaka, Y., Tanaka, K., Shiomi, H., Kurumi, Y., Tani, T., & Ogura, Y. (2022). Needle Tip Detection Using Ultrasound Probe for Vertical Punctures: A Simulation and Experimental Study. Diagnostics, 12(2), 527. https://doi.org/10.3390/diagnostics12020527