
Extraskeletal Mesenchymal Chondrosarcoma of the Uterus


Abstract
:Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertoni, F.; Picci, P.; Bacchini, P.; Capanna, R.; Innao, V.; Bacci, G.; Campanacci, M. Mesenchymal chondrosarcoma of bone and soft tissues. Cancer 1983, 52, 533–541. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, Y.; Unni, K.K.; Shives, T.C.; Swee, R.G.; Dahlin, D.C. Mesenchymal chondrosarcoma of bone and soft tissue. A review of 111 cases. Cancer 1986, 57, 2444–2453. [Google Scholar] [CrossRef]
- Frezza, A.M.; Cesari, M.; Baumhoer, D.; Biau, D.; Bielack, S.; Campanacci, D.A.; Casanova, J.; Esler, C.; Ferrari, S.; Funovics, P.T.; et al. Mesenchymal chondrosarcoma: Prognostic factors and outcome in 113 patients. A European Musculoskeletal Oncology Society study. Eur. J. Cancer 2015, 51, 374–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Li, D.; Xie, L.; Tang, S.; Guo, W. Mesenchymal chondrosarcoma of bone and soft tissue: A systematic review of 107 patients in the past 20 years. PLoS ONE 2015, 10, e0122216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhabra, R.; Tripathi, M.; Patra, D.P.; Kumar, N.; Radotra, B.; Mukherjee, K.K. Primary intracranial extraskeletal mesenchymal chondrosarcoma: Clinical mimicry as glomus jugulare. Ann. Neurosci. 2017, 24, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Shakked, R.J.; Geller, D.S.; Gorlick, R.; Dorfman, H.D. Mesenchymal chondrosarcoma: Clinicopathologic study of 20 cases. Arch. Pathol. Lab. Med. 2012, 136, 61–75. [Google Scholar] [CrossRef] [Green Version]
- Arora, K.; Riddle, N.D. Extraskeletal mesenchymal chondrosarcoma. Arch. Pathol. Lab. Med. 2018, 142, 1421–1424. [Google Scholar] [CrossRef]
- Yamagishi, A.; Ichiyanagi, O.; Naito, S.; Ito, H.; Kabasawa, T.; Yamakawa, M.; Tsuchiya, N. Primary mesenchymal chondrosarcoma of the kidney without HEY1-NCOA2 and IRF2BP2-CDX1 fusion: A case report and review. Oncol. Lett. 2020, 19, 885–891. [Google Scholar] [CrossRef] [Green Version]
- Dobin, S.M.; Donner, L.R.; Speights, V.O., Jr. Mesenchymal chondrosarcoma A cytogenetic, immunohistochemical and ultrastructural study. Cancer Genet. Cytogenet. 1995, 83, 56–60. [Google Scholar] [CrossRef]
- Suzuki, Y.; Todo, Y.; Okamoto, K.; Kato, H.; Yamashiro, K.; Hasegawa, T. Mesenchymal chondrosarcoma of the uterus. Pathol. Int. 2014, 64, 45–47. [Google Scholar] [CrossRef]
- Jung, H.; Bae, G.E.; Kim, H.M.; Kim, H.S. Clinicopathological and molecular differences between gastric-type mucinous carcinoma and usual-type endocervical adenocarcinoma of the uterine cervix. Cancer Genom. Proteom. 2020, 17, 627–641. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Choi, S.; Do, S.I.; Lee, S.H.; Yoon, N.; Kim, H.S. Clinicopathological characteristics of pleomorphic high-grade squamous intraepithelial lesion of the uterine cervix: A single-institutional series of 31 cases. Diagnostics 2020, 10, 595. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yoon, N.; Woo, H.Y.; Lee, E.J.; Do, S.I.; Na, K.; Kim, H.S. Atypical mesonephric hyperplasia of the uterus harbors pathogenic mutation of Kirsten rat sarcoma 2 viral oncogene homolog (KRAS) and gain of chromosome 1q. Cancer Genom. Proteom. 2020, 17, 813–826. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, H.S. Primary retroperitoneal mucinous carcinoma with carcinosarcomatous mural nodules: A case report with emphasis on its histological features and immunophenotype. Diagnostics 2020, 10, 580. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Kim, H.; Bae, G.E.; Lee, S.H.; Woo, H.Y.; Kim, H.S. Mesonephric-like differentiation of ovarian endometrioid and high-grade serous carcinomas: Clinicopathological and molecular characteristics distinct from those of mesonephric-like adenocarcinoma. Anticancer Res. 2021, 41, 4587–4601. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Na, K.; Kim, S.W.; Kim, H.S. Dedifferentiated mesonephric-like adenocarcinoma of the uterine corpus. Anticancer Res. 2021, 41, 2719–2726. [Google Scholar] [CrossRef]
- Koh, H.H.; Jung, Y.Y.; Kim, H.S. Clinicopathological characteristics of gastric-type endocervical adenocarcinoma misdiagnosed as an endometrial, ovarian or extragenital malignancy, or mistyped as usual-type endocervical adenocarcinoma. In Vivo 2021, 35, 2261–2273. [Google Scholar] [CrossRef]
- Lee, J.; Park, S.; Woo, H.Y.; Kim, H.S. Clinicopathological characteristics of microscopic tubal intraepithelial metastases from adenocarcinoma and small cell neuroendocrine carcinoma of the uterine cervix. In Vivo 2021, 35, 2469–2481. [Google Scholar] [CrossRef]
- Park, S.; Bae, G.E.; Kim, J.; Kim, H.S. Mesonephric-like differentiation of endometrial endometrioid carcinoma: Clinicopathological and molecular characteristics distinct from those of uterine mesonephric-like adenocarcinoma. Diagnostics 2021, 11, 1450. [Google Scholar] [CrossRef]
- Kim, S.W.; Do, S.I.; Na, K. External validation of ALK and ROS1 fusions detected using an Oncomine Comprehensive Assay. Anticancer Res. 2021, 41, 4609–4617. [Google Scholar] [CrossRef]
- Hisaoka, M.; Matsuyama, A.; Shimajiri, S.; Akiba, J.; Kusano, H.; Hiraoka, K.; Shoda, T.; Hashimoto, H. Ossifying synovial sarcoma. Pathol. Res. Pract. 2009, 205, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Krane, J.F.; Bertoni, F.; Fletcher, C.D. Myxoid synovial sarcoma: An underappreciated morphologic subset. Mod. Pathol. 1999, 12, 456–462. [Google Scholar] [PubMed]
- Thway, K.; Fisher, C. Synovial sarcoma: Defining features and diagnostic evolution. Ann. Diagn. Pathol. 2014, 18, 369–380. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Antibody | Clone | Company | Dilution |
|---|---|---|---|
| Bcl-2 | 124 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:200 |
| CD10 | 56C6 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:100 |
| CD34 | QBEnd-10 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:400 |
| CD99 | PCB1 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:50 |
| Pan-CK | AE1/AE3 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:500 |
| Cyclin D1 | P2D11F11 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:50 |
| Desmin | D33 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:200 |
| ER | 6F11 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:300 |
| PR | MIB1 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:1200 |
| Ki-67 | DO7 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:200 |
| p53 | 16 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:800 |
| S100 | Polyclonal | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:5000 |
| STAT6 | EP325 | Cell Marque (Rocklin, CA, USA) | 1:100 |
| Case | 1 | 2 |
|---|---|---|
| Author (year published) | Suzuki et al. (2014) [10] | Lee et al. (2022) (present case) |
| Age of patient | 69 years | 33 years |
| Presenting symptom | Lower abdominal distention | Uterine mass on imaging |
| Previous medical or gynecological history | Absent | Absent |
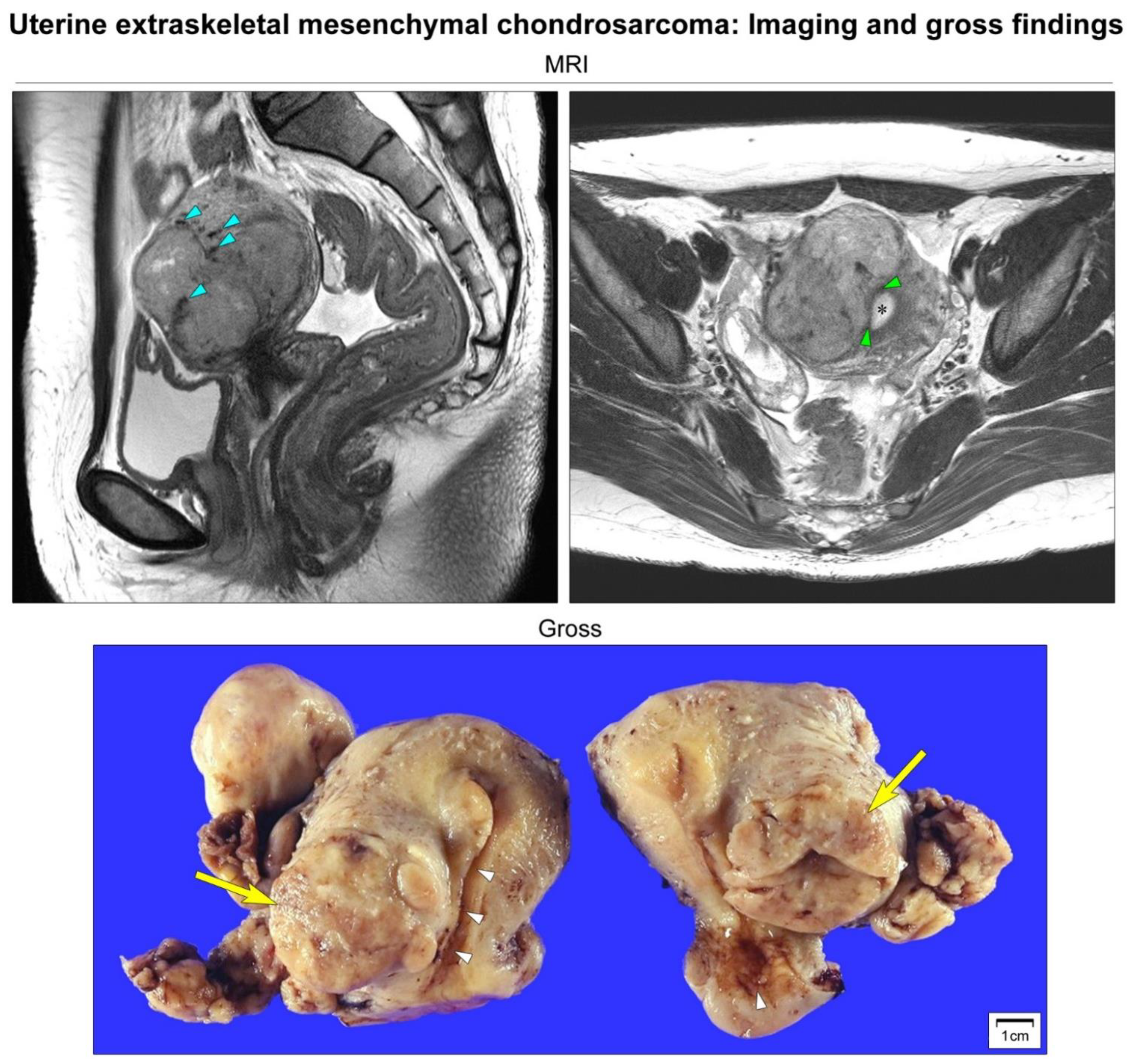
| Imaging finding | 12 cm well-defined intramural mass | 6 cm well-defined intramural mass |
| Hyaline cartilages | Present | Present |
| Undifferentiated mesenchymal cells (UMCs) | Present | Present |
| Hemangiopericytoma-like vascular pattern | Present | Present |
| Epithelial component | Absent | Absent |
| Myxoid component | Absent | Absent |
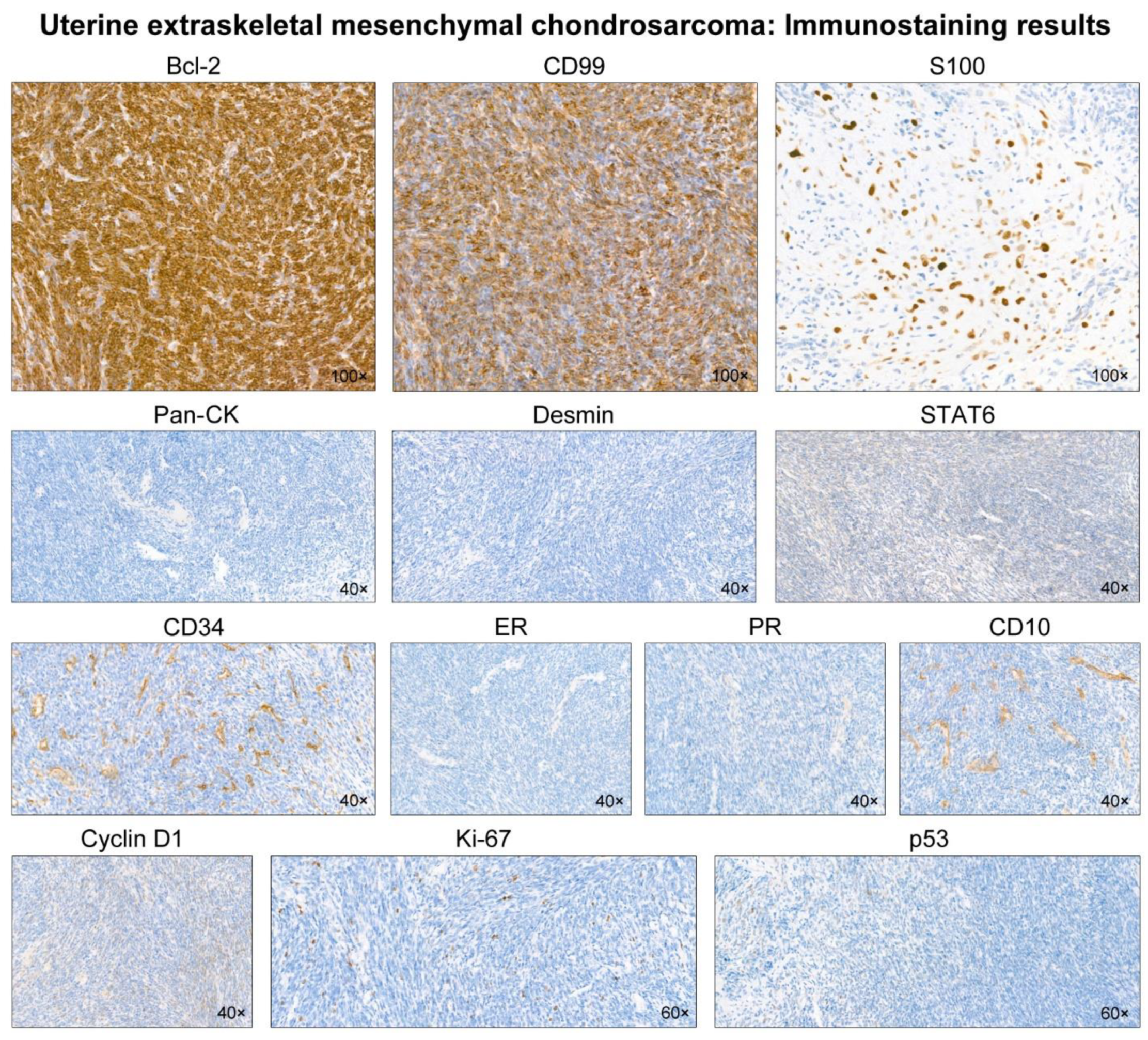
| Bcl-2 | Not applicable | Positive (in UMCs) |
| CD10 | Not applicable | Negative |
| CD34 | Negative | Negative |
| CD99 | Negative | Positive (in UMCs) |
| Pan-cytokeratin | Focal positive | Negative |
| Cyclin D1 | Not applicable | Negative |
| Desmin | Negative | Negative |
| ER | Not applicable | Negative |
| PR | Not applicable | Negative |
| Ki-67 | Not applicable | Low (<10%) |
| p53 | Not applicable | Wild-type |
| S100 | Not applicable | Positive (in cartilages) |
| SOX9 | Positive (in UMCs) | NA |
| HEY1-NCOA2 fusion | Detected | Detected |
| SS18-SSX fusion | Not applicable | Not detected |
| EWS-FLI1 fusion | Not applicable | Not detected |
| EWS-ERG fusion | Not applicable | Not detected |
| Primary treatment | Total hysterectomy | Total hysterectomy |
| Post-operative treatment | None | Whole-pelvic radiation therapy |
| Recurrence (location) | Present (bone metastasis) | Absent |
| Disease-free survival | 52 months | 3 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Choi, S.; Kim, H.-S. Extraskeletal Mesenchymal Chondrosarcoma of the Uterus. Diagnostics 2022, 12, 643. https://doi.org/10.3390/diagnostics12030643
Lee Y, Choi S, Kim H-S. Extraskeletal Mesenchymal Chondrosarcoma of the Uterus. Diagnostics. 2022; 12(3):643. https://doi.org/10.3390/diagnostics12030643
Chicago/Turabian StyleLee, Yurimi, Sangjoon Choi, and Hyun-Soo Kim. 2022. "Extraskeletal Mesenchymal Chondrosarcoma of the Uterus" Diagnostics 12, no. 3: 643. https://doi.org/10.3390/diagnostics12030643
APA StyleLee, Y., Choi, S., & Kim, H. -S. (2022). Extraskeletal Mesenchymal Chondrosarcoma of the Uterus. Diagnostics, 12(3), 643. https://doi.org/10.3390/diagnostics12030643