
The Impact of Age on In-Hospital Mortality in Critically Ill COVID-19 Patients: A Retrospective and Multicenter Study

 , ,
on behalf of the CREMS Network (Clinical Research in Emergency Medicine and Sepsis)
, ,
on behalf of the CREMS Network (Clinical Research in Emergency Medicine and Sepsis)
Abstract
:1. Introduction
2. Methods
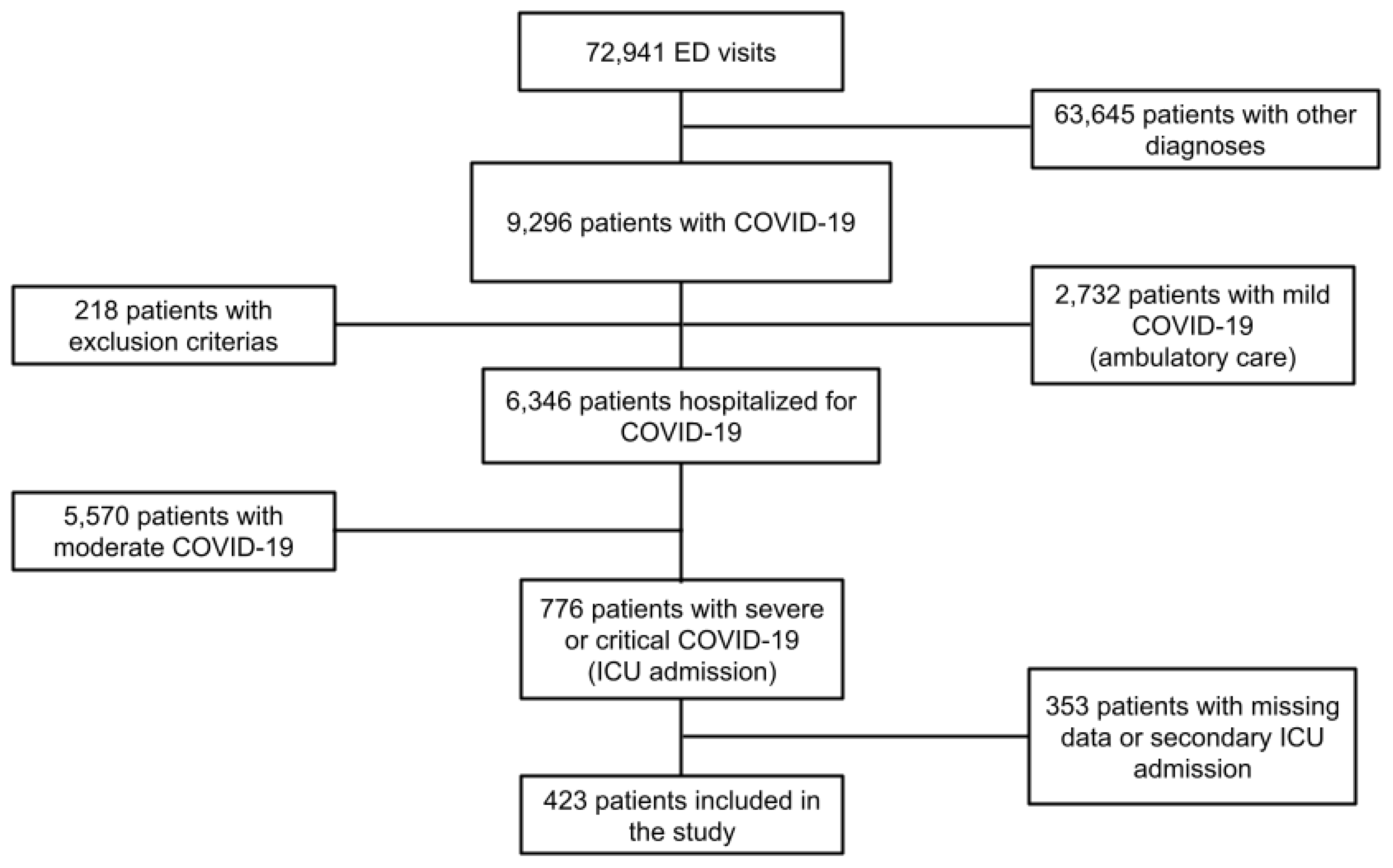
2.1. Study Population and Settings
2.2. Data Collection
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
3.2. Comparison and Correlation between Survivors and Non-Survivors
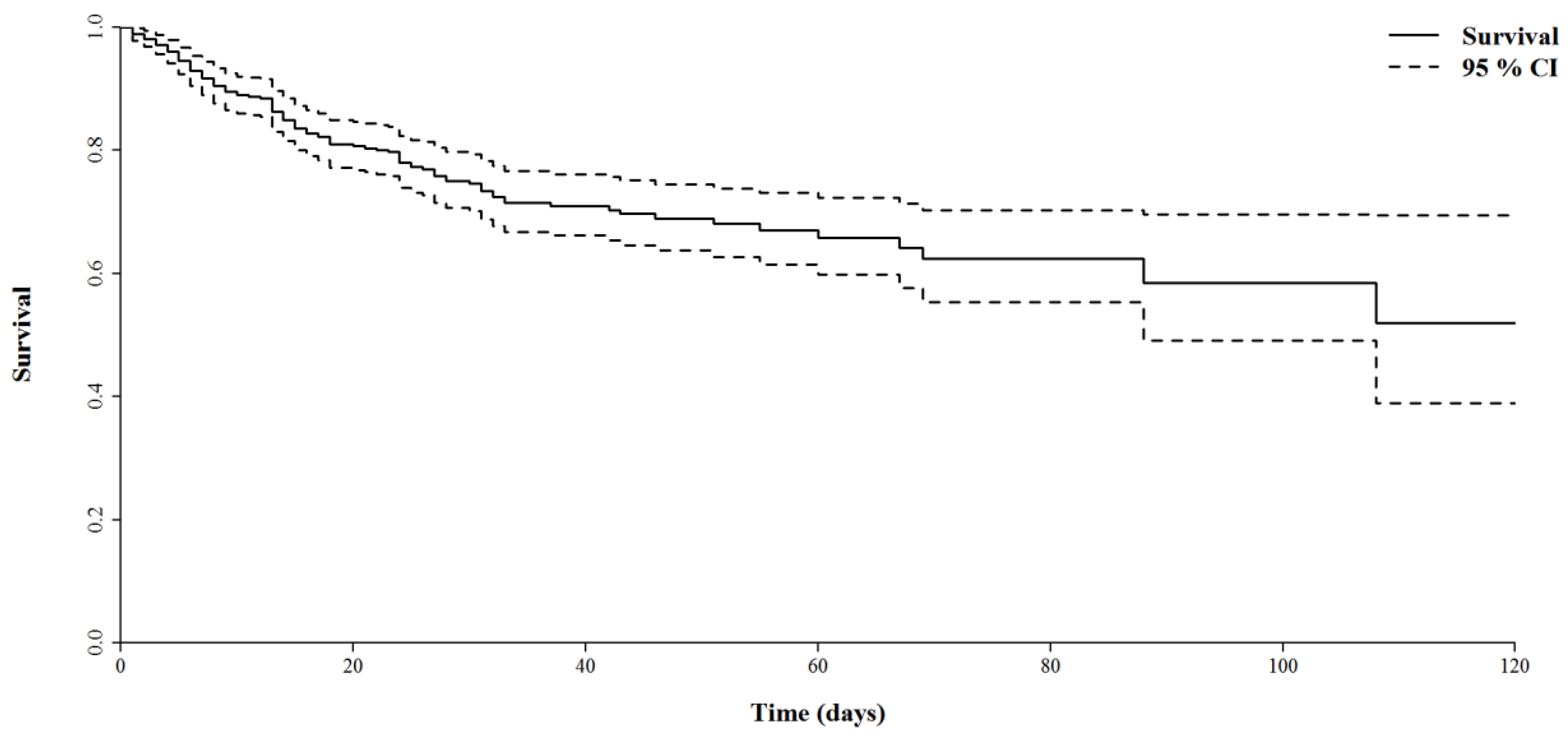
3.3. Overall Survival
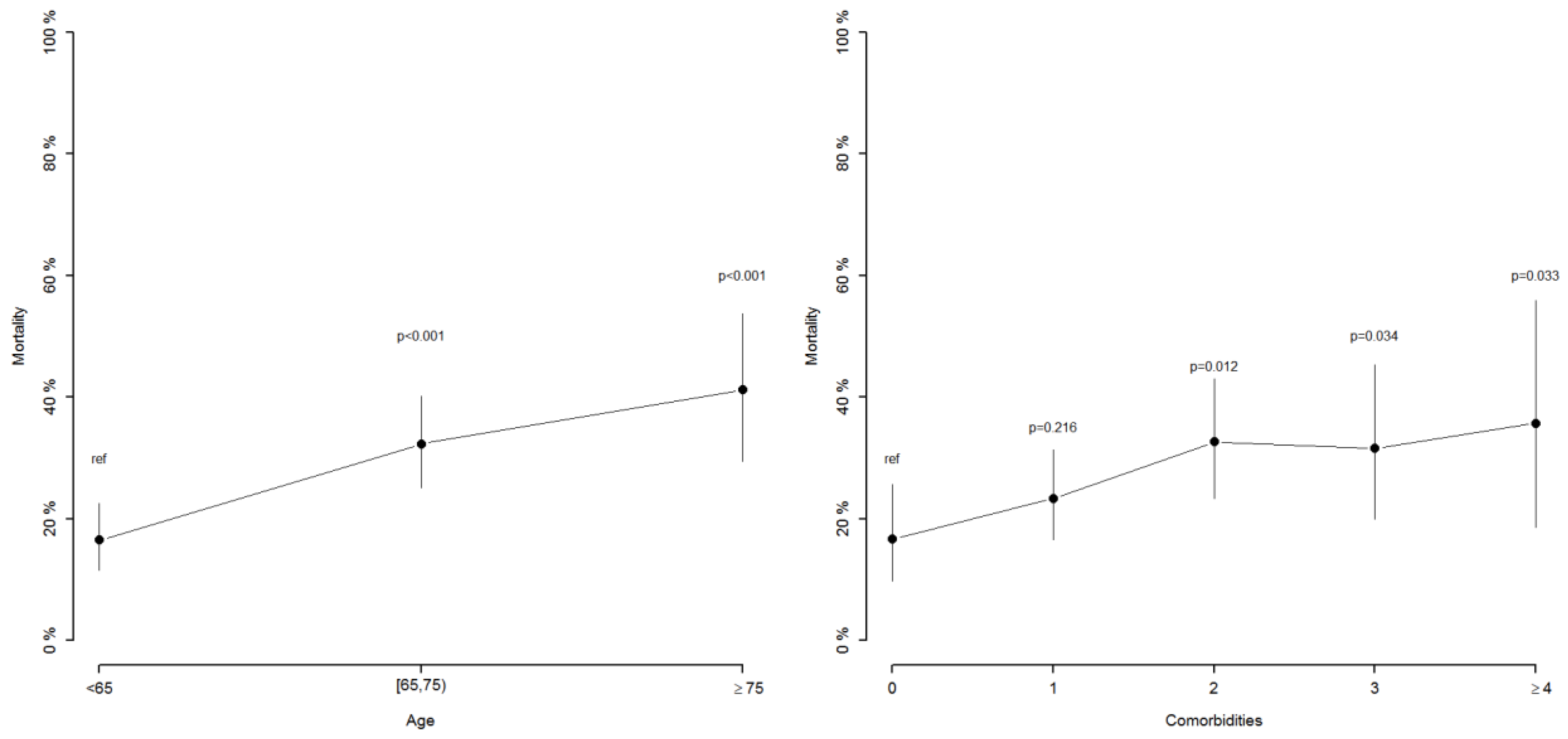
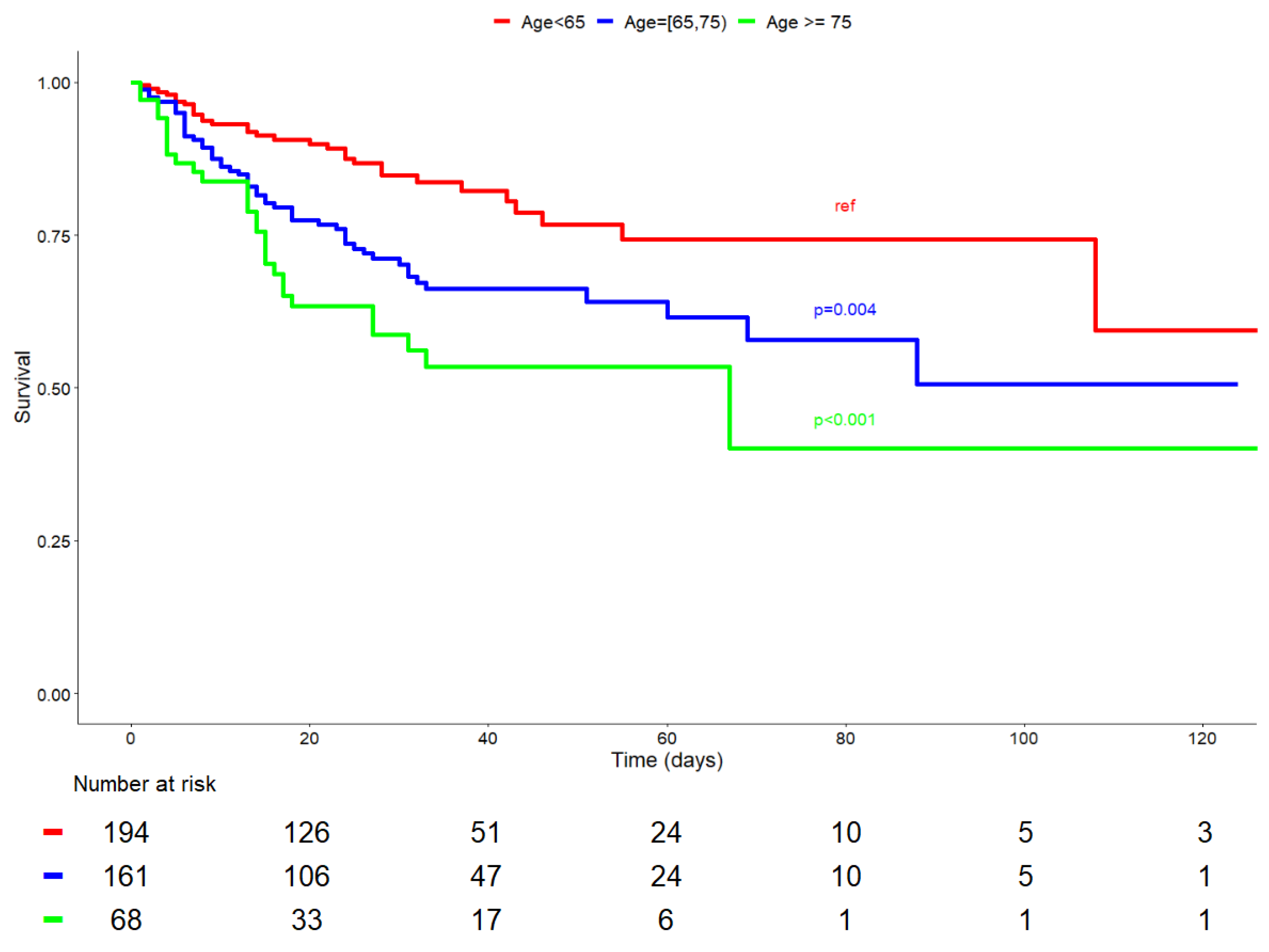
3.4. The Impact of Age on In-Hospital Mortality
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Hayek, S.S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated with Death in Critically Ill Patients with Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020, 180, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA—J. Am. Med. Assoc. 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [Green Version]
- Smorenberg, A.; Peters, E.J.; van Daele, P.L.; Nossent, E.J.; Muller, M. How does SARS-CoV-2 targets the elderly patients? A review on potential mechanisms increasing disease severity. Eur. J. Intern. Med. 2021, 83, 1–5. [Google Scholar] [CrossRef]
- Bravata, D.M.; Perkins, A.J.; Myers, L.J.; Arling, G.; Zhang, Y.; Zillich, A.J.; Reese, L.; Dysangco, A.; Agarwal, R.; Myers, J.; et al. Association of Intensive Care Unit Patient Load and Demand with Mortality Rates in US Department of Veterans Affairs Hospitals During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2034266. [Google Scholar] [CrossRef]
- Zangrillo, A.; Gattinoni, L. Learning from mistakes during the pandemic: The Lombardy lesson. Intensiv. Care Med. 2020, 46, 1622–1623. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE—Acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis with 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; De Lange, D.; Artigas, A.; Bin, D.; Moreno, R.; Christensen, S.; Joynt, G.; Bagshaw, S.M.; Sprung, C.L.; Benoit, D.; et al. The status of intensive care medicine research and a future agenda for very old patients in the ICU. Intensiv. Care Med. 2017, 43, 1319–1328. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Muscedere, J.; Waters, B.; Varambally, A.; Bagshaw, S.M.; Boyd, J.G.; Maslove, D.; Sibley, S.; Rockwood, K. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensiv. Care Med. 2017, 43, 1105–1122. [Google Scholar] [CrossRef] [Green Version]
- Vallet, H.; Schwarz, G.L.; Flaatten, H.; De Lange, D.W.; Guidet, B.; Dechartres, A. Mortality of Older Patients Admitted to an ICU: A Systematic Review. Crit. Care Med. 2020, 49, 324–334. [Google Scholar] [CrossRef]
- Guidet, B.; Vallet, H.; Boddaert, J.; De Lange, D.W.; Morandi, A.; Leblanc, G.; Artigas, A.; Flaatten, H. Caring for the critically ill patients over 80: A narrative review. Ann. Intensiv. Care 2018, 8, 114. [Google Scholar] [CrossRef]
- Nguyen, Y.-L.; Angus, D.C.; Boumendil, A.; Guidet, B. The challenge of admitting the very elderly to intensive care. Ann. Intensiv. Care 2011, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Anesi, G.L.; Kerlin, M.P. The impact of resource limitations on care delivery and outcomes: Routine variation, the coronavirus disease 2019 pandemic, and persistent shortage. Curr. Opin. Crit. Care 2021, 27, 513–519. [Google Scholar] [CrossRef]
- Lewis, E.G.; Breckons, M.; Lee, R.P.; Dotchin, C.; Walker, R. Rationing care by frailty during the COVID-19 pandemic. Age Ageing 2020, 50, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, G.; Boumendil, A.; Guidet, B. Ten things to know about critically ill elderly patients. Intensiv. Care Med. 2016, 43, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; Van Heerden, V.; Jung, C.; Beil, M.; Leaver, S.; Rhodes, A.; Guidet, B.; Delange, D.W. The good, the bad and the ugly: Pandemic priority decisions and triage. J. Med. Ethics 2020, 47, e75. [Google Scholar] [CrossRef]
- Capuzzo, M.; Volta, C.A.; Tassinati, T.; Moreno, R.P.; Valentin, A.; Guidet, B.; Iapichino, G.; Martin, C.; Perneger, T.; Combescure, C.; et al. Hospital mortality of adults admitted to Intensive Care Units in hospitals with and without Intermediate Care Units: A multicentre European cohort study. Crit. Care 2014, 18, 551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín, S.; Pérez, A.; Aldecoa, C. Sepsis and Immunosenescence in the Elderly Patient: A Review. Front. Med. 2017, 4, 20. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, F.; Corbi, G.; Mazzeo, G.; Boccia, M.; Aronne, L.; D’Agnano, V.; Komici, K.; Mazzarella, G.; Parrella, R.; Bianco, A. COVID-19 and the elderly: Insights into pathogenesis and clinical decision-making. Aging Clin. Exp. Res. 2020, 32, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Pang, S.-C.; Yang, Y. A potential association between immunosenescence and high COVID-19 related mortality among elderly patients with cardiovascular diseases. Immun. Ageing 2021, 18, 25. [Google Scholar] [CrossRef]
- Crooke, S.N.; Ovsyannikova, I.G.; Poland, G.A.; Kennedy, R.B. Immunosenescence and human vaccine immune responses. Immun. Ageing 2019, 16, 25. [Google Scholar] [CrossRef] [Green Version]
- Jung, C.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; Beil, M.; et al. Differences in mortality in critically ill elderly patients during the second COVID-19 surge in Europe. Crit. Care 2021, 25, 344. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Characteristics | All Patients n = 423 | Survivors n = 311 | Non-Survivors n = 112 | p Value |
|---|---|---|---|---|
| Age (years) | 66 [58–72] | 64.0 [56–71] | 69 [64–74.3] | <0.001 * |
| Age <65 years | 194 (45.9) | 162 (52.1) | 32 (28.6) | ref |
| Age 65–74 years | 161 (38.1) | 109 (35.1) | 52 (46.4) | <0.0001 * |
| Age >75 years | 68 (16.1) | 40 (12.9) | 28 (25.0) | <0.0001 * |
| Male n (%) | 311 (73.5) | 222 (71.4) | 89 (79.5) | 0.096 |
| Comorbidities n (%) | ||||
| Hypertension | 235 (55.6) | 164 (52.7) | 71 (63.4) | 0.052 |
| Overweight (BMI > 25 & <30) | 125 (30.3) | 93 (30.5) | 32 (29.6) | 0.867 |
| Obesity (BMI > 30) | 174 (42.1) | 131 (43.0) | 43 (39.8) | 0.571 |
| Cardiovascular diseases | 135 (31.9) | 89 (28.6) | 46 (41.1) | 0.015 * |
| Diabetes mellitus | 118 (27.9) | 82 (26.4) | 36 (32.1) | 0.243 |
| Chronic kidney disease | 69 (16.5) | 45 (14.6) | 24 (22.0) | 0.071 |
| Malignancies or ID | 52 (12.3) | 35 (11.3) | 17 (15.2) | 0.278 |
| Respiratory diseases | 95 (22.5) | 69 (22.2) | 26 (23.2) | 0.823 |
| Total autonomy | 386 (91.7) | 288 (92.6) | 98 (89.1) | 0.251 |
| ED parameters | ||||
| Respiratory rate (/min) | 30.0 [24–35] | 29 [24–35] | 30 [24.5–35.5] | 0.218 |
| First oxygen saturation (%) | 90 [84–94] | 91.0 [85–95.0] | 88 [82–92.9] | 0.005 * |
| Oxygen need (L/min) | 15 [6–15] | 15 [6–15] | 15 [9–15] | 0.085 |
| Systolic blood pressure (mmHg) | 130 [115–142] | 130 [115.8–142] | 129 [113–145] | 0.364 |
| Laboratory findings | ||||
| Creatinine (μmol/L) | 84 [67–105] | 80 [66–101.9] | 93.0 [72–119] | 0.001 * |
| Lymphocytes (/μL) | 780 [580–1110] | 790 [600–1128] | 725 [500–1063] | 0.144 |
| CRP (mg/L) | 148.2 [83–223] | 147.2 [85–222] | 153 [79–223] | 0.766 |
| pH | 7.46 [7.42–7.49] | 7.46 [7.42–7.49] | 7.46 [7.41–7.49] | 0.456 |
| PaO2 (mmHg) | 67 [55–80.7] | 67.8 [58–82.5] | 63.5 [52.6–77.8] | 0.037 * |
| PaCO2 (mmHg) | 33.9 [30–38] | 34 [30.1–38] | 33 [28–37] | 0.116 |
| Lactate (mmol/L) | 1.4 [1.1–2] | 1.4 [1–1.9] | 1.6 [1.2–2.4] | 0.002 * |
| Radiological findings n (%) | ||||
| Typical CT-scan | 223 (53.5) | 170 (55.6) | 53 (47.8) | 0.158 |
| Extension > 50% ICU stay and outcome | 140 (45.9) | 107 (46.1) | 33 (45.2) | 0.891 |
| SAPS II | 42 [32–54] | 40 [30.5–51] | 47 [39–58] | <0.001 * |
| Mechanical ventilation (days) | 14 [7–24] | 15 [8–25] | 12 [5–19.5] | 0.014 * |
| ARDS | 372 (91.0) | 268 (89.0) | 104 (96.3) | 0.024 * |
| Prone position | 263 (62.5) | 183 (59.2) | 80 (71.4) | 0.022 * |
| ECMO | 16 (3.8) | 11 (3.5) | 5 (4.5) | 0.847 |
| Dialysis | 59 (14.0) | 31 (10.0) | 28 (25.0) | <0.001 * |
| Pulmonary embolism | 50 (11.9) | 31 (10.0) | 19 (17.1) | 0.047 * |
| ICU LOS (days) | 17 [8–30] | 19 [10–31] | 13 [6–24] | <0.001 * |
| In-hospital LOS (days) | 26 [13–43] | 30.0 [19–48] | 13.5 [6–24.3] | <0.001 * |
| General Characteristics | Odds Ratio | 95%CI | p Value |
|---|---|---|---|
| Age < 65 years | 1 | ref | |
| Age 65–74 years | 2.962 | [1.231–7.132] | 0.015 * |
| Age ≥ 75 years | 3.084 | [0.952–9.992] | 0.060 |
| Gender (male) | 2.753 | [0.936–8.100] | 0.066 |
| SAPS II | 1.027 | [1.000–1.055] | 0.052 |
| Comorbidities | |||
| Knaus score < 6 | 0.739 | [0.160–3.400] | 0.697 |
| Hypertension | 0.880 | [0.355–2.181] | 0.782 |
| Obesity (BMI > 30) | 1.045 | [0.411–2.657] | 0.926 |
| Overweight (BMI > 25 and <30) | 1.273 | [0.494–3.284] | 0.617 |
| Cardiovascular diseases | 1. 248 | [0.503–3.100] | 0.633 |
| Diabetes mellitus | 0.944 | [0.367–2.427] | 0.905 |
| Respiratory diseases | 0.990 | [0.328–2.991] | 0.986 |
| Asthma | 0.739 | [0.249–2.193] | 0.586 |
| COPD | 0.586 | [0.216–1.589] | 0.294 |
| Liver diseases | 0.610 | [0.070–5.319] | 0.655 |
| Chronic kidney disease | 0.853 | [0.285–2.551] | 0.776 |
| Malignancies | 0.842 | [0.229–3.098] | 0.796 |
| Immunodeficiency | 4.207 | [1.006–17.586] | 0.049 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Borgne, P.; Dellenbach, Q.; Alame, K.; Noizet, M.; Gottwalles, Y.; Chouihed, T.; Abensur Vuillaume, L.; Lavoignet, C.-E.; Bérard, L.; Molter, L.; et al. The Impact of Age on In-Hospital Mortality in Critically Ill COVID-19 Patients: A Retrospective and Multicenter Study. Diagnostics 2022, 12, 666. https://doi.org/10.3390/diagnostics12030666
Le Borgne P, Dellenbach Q, Alame K, Noizet M, Gottwalles Y, Chouihed T, Abensur Vuillaume L, Lavoignet C-E, Bérard L, Molter L, et al. The Impact of Age on In-Hospital Mortality in Critically Ill COVID-19 Patients: A Retrospective and Multicenter Study. Diagnostics. 2022; 12(3):666. https://doi.org/10.3390/diagnostics12030666
Chicago/Turabian StyleLe Borgne, Pierrick, Quentin Dellenbach, Karine Alame, Marc Noizet, Yannick Gottwalles, Tahar Chouihed, Laure Abensur Vuillaume, Charles-Eric Lavoignet, Lise Bérard, Lise Molter, and et al. 2022. "The Impact of Age on In-Hospital Mortality in Critically Ill COVID-19 Patients: A Retrospective and Multicenter Study" Diagnostics 12, no. 3: 666. https://doi.org/10.3390/diagnostics12030666
APA StyleLe Borgne, P., Dellenbach, Q., Alame, K., Noizet, M., Gottwalles, Y., Chouihed, T., Abensur Vuillaume, L., Lavoignet, C. -E., Bérard, L., Molter, L., Gennai, S., Kepka, S., Lefebvre, F., & Bilbault, P., on behalf of the CREMS Network (Clinical Research in Emergency Medicine and Sepsis). (2022). The Impact of Age on In-Hospital Mortality in Critically Ill COVID-19 Patients: A Retrospective and Multicenter Study. Diagnostics, 12(3), 666. https://doi.org/10.3390/diagnostics12030666