
Radiomics for the Prediction of Response to Antifibrotic Treatment in Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Disease Progression
2.3. Acquisition Protocol for HRCT
2.4. Semiquantitative Fibrosis Quantification (Fibrotic Score)
2.5. Whole-Lung CT Texture Analysis
2.6. Automated Quantification of Parenchymal Patterns
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Inter-Rater Reliability of the Fibrotic Score
3.3. Radiomic Feature Extraction and Selection
3.4. Automated Quantification of Parenchymal Patterns
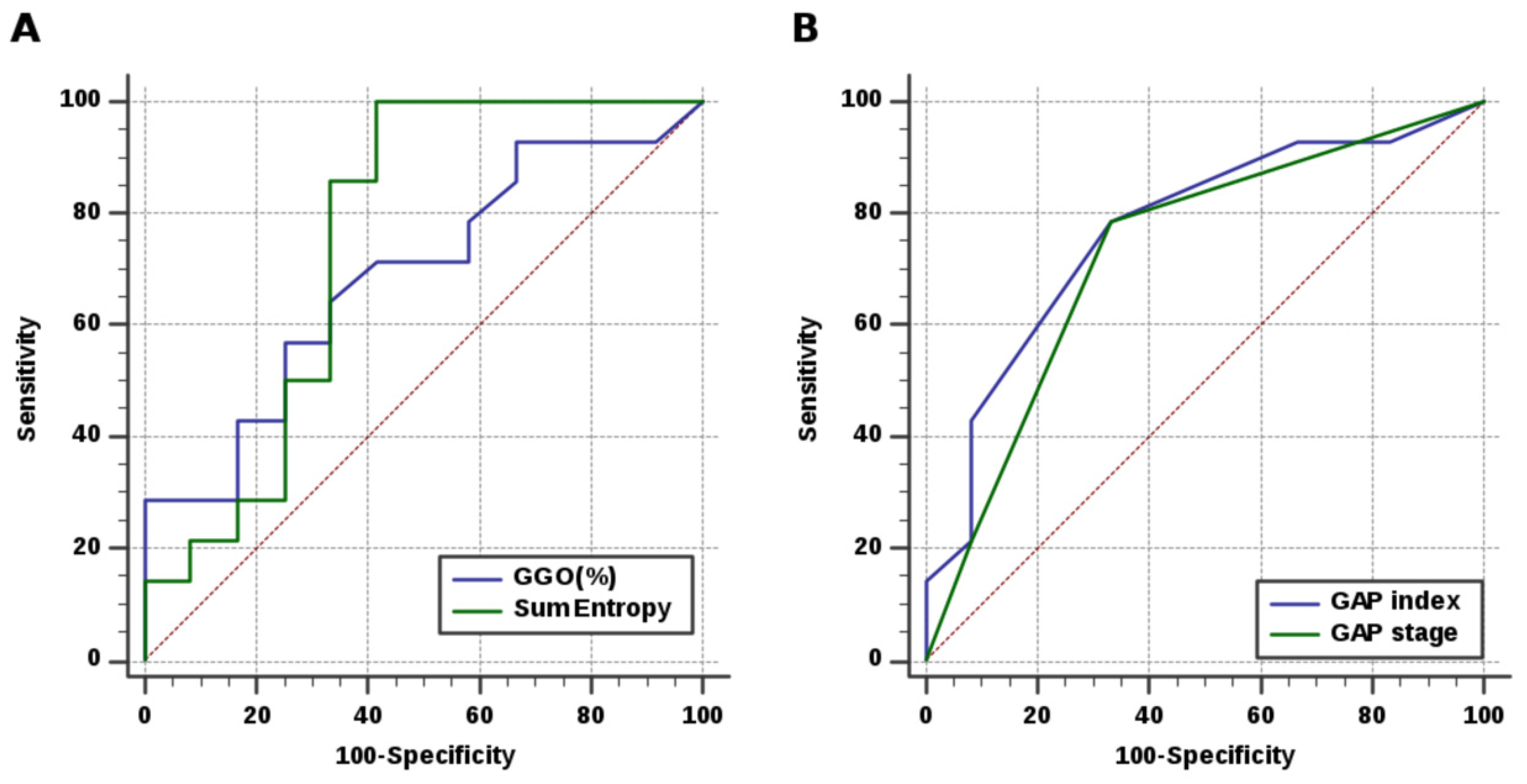
3.5. Development of Prediction Model with Performance Evaluation and Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lederer, D.J.; Martinez, F.J. Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2018, 378, 1811–1823. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, M.; Zaizen, Y.; Kataoka, K.; Kuroda, K.; Tabata, K.; Bychkov, A.; Sumikawa, H.; Johkoh, T.; Aoshima, M.; Kondoh, Y.; et al. Histologic factors associated with nintedanib efficacy in patients with idiopathic pulmonary fibrosis. PLoS ONE 2021, 16, e0245147. [Google Scholar] [CrossRef]
- Fernandez Fabrellas, E.; Peris Sanchez, R.; Sabater Abad, C.; Juan Samper, G. Prognosis and Follow-Up of Idiopathic Pulmonary Fibrosis. Med. Sci. 2018, 6, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [Green Version]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glassberg, M.K.; Kardatzke, D.; King, T.E., Jr.; Lancaster, L.; Sahn, S.A.; Szwarcberg, J.; et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): Two randomised trials. Lancet 2011, 377, 1760–1769. [Google Scholar] [CrossRef]
- Loveman, E.; Copley, V.R.; Scott, D.A.; Colquitt, J.L.; Clegg, A.J.; O’Reilly, K.M. Comparing new treatments for idiopathic pulmonary fibrosis--a network meta-analysis. BMC Pulm. Med. 2015, 15, 37. [Google Scholar] [CrossRef] [Green Version]
- Skandamis, A.; Kani, C.; Markantonis, S.L.; Souliotis, K. Systematic review and network meta-analysis of approved medicines for the treatment of idiopathic pulmonary fibrosis. J. Drug Assess. 2019, 8, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Behr, J.; Prasse, A.; Wirtz, H.; Koschel, D.; Pittrow, D.; Held, M.; Klotsche, J.; Andreas, S.; Claussen, M.; Grohe, C.; et al. Survival and course of lung function in the presence or absence of antifibrotic treatment in patients with idiopathic pulmonary fibrosis: Long-term results of the INSIGHTS-IPF registry. Eur. Respir. J. 2020, 56, 1902279. [Google Scholar] [CrossRef]
- Kang, J.; Han, M.; Song, J.W. Antifibrotic treatment improves clinical outcomes in patients with idiopathic pulmonary fibrosis: A propensity score matching analysis. Sci. Rep. 2020, 10, 15620. [Google Scholar] [CrossRef]
- Nathan, S.D.; Albera, C.; Bradford, W.Z.; Costabel, U.; du Bois, R.M.; Fagan, E.A.; Fishman, R.S.; Glaspole, I.; Glassberg, M.K.; Glasscock, K.F.; et al. Effect of continued treatment with pirfenidone following clinically meaningful declines in forced vital capacity: Analysis of data from three phase 3 trials in patients with idiopathic pulmonary fibrosis. Thorax 2016, 71, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterniti, M.O.; Bi, Y.; Rekic, D.; Wang, Y.; Karimi-Shah, B.A.; Chowdhury, B.A. Acute Exacerbation and Decline in Forced Vital Capacity Are Associated with Increased Mortality in Idiopathic Pulmonary Fibrosis. Ann. Am. Thorac. Soc. 2017, 14, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; du Bois, R.M.; Fagan, E.A.; Fishman, R.S.; Glaspole, I.; Glassberg, M.K.; Lancaster, L.; et al. Pirfenidone for idiopathic pulmonary fibrosis: Analysis of pooled data from three multinational phase 3 trials. Eur. Respir. J. 2016, 47, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Costabel, U.; Inoue, Y.; Richeldi, L.; Collard, H.R.; Tschoepe, I.; Stowasser, S.; Azuma, A. Efficacy of Nintedanib in Idiopathic Pulmonary Fibrosis across Prespecified Subgroups in INPULSIS. Am. J. Respir. Crit. Care Med. 2016, 193, 178–185. [Google Scholar] [CrossRef]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.H.; Tomassetti, S.; Lee, J.S.; Poletti, V.; Buccioli, M.; Elicker, B.M.; Jones, K.D.; et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern. Med. 2012, 156, 684–691. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Lang, D.; Akbari, K.; Walcherberger, S.; Hergan, B.; Horner, A.; Hepp, M.; Kaiser, B.; Pieringer, H.; Lamprecht, B. Computed tomography findings as determinants of pulmonary function tests in fibrotic interstitial lung diseases-Network-analyses and multivariate models. Chron. Respir. Dis. 2020, 17, 1479973120967025. [Google Scholar] [CrossRef]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Nair, A.; Karwoski, R.; Raghunath, S.M.; Walsh, S.L.; Wells, A.U.; Hansell, D.M. Automated Quantitative Computed Tomography Versus Visual Computed Tomography Scoring in Idiopathic Pulmonary Fibrosis: Validation Against Pulmonary Function. J. Thorac. Imaging 2016, 31, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Balestro, E.; Cocconcelli, E.; Giraudo, C.; Polverosi, R.; Biondini, D.; Lacedonia, D.; Bazzan, E.; Mazzai, L.; Rizzon, G.; Lococo, S.; et al. High-Resolution CT Change over Time in Patients with Idiopathic Pulmonary Fibrosis on Antifibrotic Treatment. J. Clin. Med. 2019, 8, 1469. [Google Scholar] [CrossRef] [Green Version]
- Sugino, K.; Shimizu, H.; Nakamura, Y.; Isshiki, T.; Matsumoto, K.; Homma, S. Clinico-radiological features and efficacy of anti-fibrotic agents in atypical idiopathic pulmonary fibrosis. J. Thorac. Dis. 2018, 10, 899–908. [Google Scholar] [CrossRef] [Green Version]
- Bartholmai, B.J.; Raghunath, S.; Karwoski, R.A.; Moua, T.; Rajagopalan, S.; Maldonado, F.; Decker, P.A.; Robb, R.A. Quantitative computed tomography imaging of interstitial lung diseases. J. Thorac. Imaging 2013, 28, 298–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, A.; Karwoski, R.A.; Gierada, D.S.; Bartholmai, B.J.; Koo, C.W. Quantitative CT Analysis of Diffuse Lung Disease. Radiographics 2020, 40, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Frix, A.N.; Cousin, F.; Refaee, T.; Bottari, F.; Vaidyanathan, A.; Desir, C.; Vos, W.; Walsh, S.; Occhipinti, M.; Lovinfosse, P.; et al. Radiomics in Lung Diseases Imaging: State-of-the-Art for Clinicians. J. Pers. Med. 2021, 11, 602. [Google Scholar] [CrossRef] [PubMed]
- Parekh, V.; Jacobs, M.A. Radiomics: A new application from established techniques. Expert Rev. Precis. Med. Drug Dev. 2016, 1, 207–226. [Google Scholar] [CrossRef] [Green Version]
- Stefano, A.; Gioe, M.; Russo, G.; Palmucci, S.; Torrisi, S.E.; Bignardi, S.; Basile, A.; Comelli, A.; Benfante, V.; Sambataro, G.; et al. Performance of Radiomics Features in the Quantification of Idiopathic Pulmonary Fibrosis from HRCT. Diagnostics 2020, 10, 306. [Google Scholar] [CrossRef]
- Kim, H.J.; Brown, M.S.; Chong, D.; Gjertson, D.W.; Lu, P.; Kim, H.J.; Coy, H.; Goldin, J.G. Comparison of the quantitative CT imaging biomarkers of idiopathic pulmonary fibrosis at baseline and early change with an interval of 7 months. Acad. Radiol. 2015, 22, 70–80. [Google Scholar] [CrossRef]
- Best, A.C.; Meng, J.; Lynch, A.M.; Bozic, C.M.; Miller, D.; Grunwald, G.K.; Lynch, D.A. Idiopathic pulmonary fibrosis: Physiologic tests, quantitative CT indexes, and CT visual scores as predictors of mortality. Radiology 2008, 246, 935–940. [Google Scholar] [CrossRef]
- Budzikowski, J.D.; Foy, J.J.; Rashid, A.A.; Chung, J.H.; Noth, I.; Armato, S.G., 3rd. Radiomics-based assessment of idiopathic pulmonary fibrosis is associated with genetic mutations and patient survival. J. Med. Imaging 2021, 8, 031903. [Google Scholar] [CrossRef]
- Reichmann, W.M.; Yu, Y.F.; Macaulay, D.; Wu, E.Q.; Nathan, S.D. Change in forced vital capacity and associated subsequent outcomes in patients with newly diagnosed idiopathic pulmonary fibrosis. BMC Pulm. Med. 2015, 15, 167. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.A.; Stewart, I.; Moss, S.; Fabbri, L.; Robinson, K.A.; Johnson, S.R.; Jenkins, R.G. Three-Month FVC Change: A Trial Endpoint for IPF Based on Individual Participant Data Meta-Analysis. Am. J. Respir. Crit. Care Med. 2022; ahead of print. [Google Scholar] [CrossRef]
- Fraser, E.; St Noble, V.; Hoyles, R.K.; Benamore, R.; Ho, L.P. Readily accessible CT scoring method to quantify fibrosis in IPF. BMJ Open Respir. Res. 2020, 7, e000584. [Google Scholar] [CrossRef] [PubMed]
- Choe, J.; Hwang, H.J.; Seo, J.B.; Lee, S.M.; Yun, J.; Kim, M.J.; Jeong, J.; Lee, Y.; Jin, K.; Park, R.; et al. Content-based Image Retrieval by Using Deep Learning for Interstitial Lung Disease Diagnosis with Chest CT. Radiology 2022, 302, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, C.H.; Liu, Y.C.; Wan, Y.L.; Yun, C.H.; Wu, W.J.; Lopez-Gonzalez, R.; Huang, W.M. Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images. Cancers 2021, 13, 5600. [Google Scholar] [CrossRef]
- Dercle, L.; Ammari, S.; Bateson, M.; Durand, P.B.; Haspinger, E.; Massard, C.; Jaudet, C.; Varga, A.; Deutsch, E.; Soria, J.C.; et al. Limits of radiomic-based entropy as a surrogate of tumor heterogeneity: ROI-area, acquisition protocol and tissue site exert substantial influence. Sci. Rep. 2017, 7, 7952. [Google Scholar] [CrossRef]
- Vancheri, C. Common pathways in idiopathic pulmonary fibrosis and cancer. Eur. Respir. Rev. 2013, 22, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, L.; Goldin, J.; Trampisch, M.; Kim, G.H.; Ilowite, J.; Homik, L.; Hotchkin, D.L.; Kaye, M.; Ryerson, C.J.; Mogulkoc, N.; et al. Effects of Nintedanib on Quantitative Lung Fibrosis Score in Idiopathic Pulmonary Fibrosis. Open Respir. Med. J. 2020, 14, 22–31. [Google Scholar] [CrossRef]
- Zhang, Y.; Jones, K.D.; Achtar-Zadeh, N.; Green, G.; Kukreja, J.; Xu, B.; Wolters, P.J. Histopathological and molecular analysis of idiopathic pulmonary fibrosis lungs from patients treated with pirfenidone or nintedanib. Histopathology 2019, 74, 341–349. [Google Scholar] [CrossRef]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; van Moorsel, C.H.M.; van Es, H.W.; van Beek, F.T.; Struik, M.H.L.; Kokosi, M.; Egashira, R.; Brun, A.L.; et al. Predicting Outcomes in Idiopathic Pulmonary Fibrosis Using Automated Computed Tomographic Analysis. Am. J. Respir. Crit. Care Med. 2018, 198, 767–776. [Google Scholar] [CrossRef]
- Wright, W.A.; Crowley, L.E.; Parekh, D.; Crawshaw, A.; Dosanjh, D.P.; Nightingale, P.; Thickett, D.R. Real-world retrospective observational study exploring the effectiveness and safety of antifibrotics in idiopathic pulmonary fibrosis. BMJ Open Respir. Res. 2021, 8, e000782. [Google Scholar] [CrossRef]
- Okamori, S.; Asakura, T.; Masuzawa, K.; Yasuda, H.; Kamata, H.; Ishii, M.; Betsuyaku, T. Suspected accelerated disease progression after discontinuation of nintedanib in patients with idiopathic pulmonary fibrosis: Two case reports. Medicine 2017, 96, e9081. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Set | Validation Set | ||||
|---|---|---|---|---|---|---|
| SD (n = 12) | PD (n = 14) | p-Value | SD (n = 7) | PD (n = 2) | p-Value | |
| Age | 72.58 ± 10.21 | 76.14 ± 7.88 | 0.326 | 76.71 ± 7.99 | 69.00 ± 0.00 | 0.018 * |
| Sex (M) | 7 (58%) | 12 (86%) | 0.139 | 6 (86%) | 0 | 0.043 * |
| Smoking | 5 (42%) | 7 (50%) | 0.686 | 4 (57%) | 0 | 0.030 * |
| PFTs | ||||||
| FVC (%) | 82.17 ± 19.69 | 82.09 ± 22.80 | 0.993 | 91.57 ± 26.61 | 65.00 | 0.386 |
| FEV1 (%) | 90.42 ± 20.37 | 79.90 ± 30.58 | 0.321 | 94.43 ± 20.35 | 73.00 | 0.363 |
| DLCO (%) | 69.36 ± 19.71 | 62.45 ± 17.27 | 0.392 | 63.33 ± 33.63 | 54.00 | 0.807 |
| TLC (%) | 75.50 ± 8.94 | 72.07 ± 12.03 | 0.425 | 89.29 ± 20.23 | 60.00 | 0.224 |
| GAP index | 3.00 ± 1.41 | 4.43 ± 1.60 | 0.025 * | 4.00 ± 1.26 | 4.50 ± 0.71 | 0.625 |
| GAP stage | 1.42 ± 0.67 | 2.00 ± 0.68 | 0.038 * | 2.00 ± 0.63 | 2.00 ± 0.00 | 1.000 |
| Treatment duration (weeks) | 48.95 ± 17.60 | 35.96 ±18.64 | 0.082 | 36.96 ± 14.48 | 16.50 ± 2.12 | 0.099 |
| Fibrotic score | 19.89 ± 10.59 | 25.50 ± 11.08 | 0.200 | 21.90 ± 9.06 | 26.72 ± 23.65 | 0.639 |
| Lung volume (mL) | 3242.25 ± 666.33 | 3057.29 ± 849.69 | 0.546 | 3308.96 ± 1362.99 | 3553.67 ± 49.14 | 0.816 |
| Metrics | Features | SD | PD | p-Value |
|---|---|---|---|---|
| First order | Energy | 2.21 × 1012 | 2.03 × 1012 | 0.385 |
| Entropy | 8.23 | 8.80 | 0.030 * | |
| Kurtosis | 21.28 | 15.77 | 0.028 * | |
| Skewness | 5.00 | 4.00 | 0.025 * | |
| Mean | −411.04 | −357.93 | 0.415 | |
| Standard deviation | 359.54 | 382.53 | 0.169 | |
| Median | −530.11 | −479.29 | 0.409 | |
| 10th percentile | −678.26 | −675.09 | 0.951 | |
| 90th percentile | 13.85 | 137.23 | 0.213 | |
| Second order (GLCM) | Autocorrelation | 444.15 | 556.28 | 0.075 |
| Cluster prominence | 627,504.74 | 590,318.29 | 0.651 | |
| Cluster shade | 10,774.07 | 10,488.91 | 0.820 | |
| Contrast | 50.01 | 58.24 | 0.101 | |
| Correlation | 1.45 | 1.44 | 0.788 | |
| Difference entropy | 6.19 | 6.55 | 0.038 * | |
| Difference variance | 30.55 | 33.30 | 0.247 | |
| Dissimilarity | 5.95 | 6.79 | 0.048 * | |
| Inverse difference | 0.91 | 0.83 | 0.035 * | |
| IMC1 | −0.28 | −0.28 | 0.837 | |
| IMC2 | 1.55 | 1.56 | 0.642 | |
| Maximum probability | 0.11 | 0.07 | 0.028 * | |
| Sum average | 54.13 | 61.10 | 0.059 | |
| Sum entropy | 9.87 | 10.45 | 0.036 * | |
| Sum of squares | 93.72 | 107.59 | 0.160 | |
| Sum variance | 324.86 | 372.13 | 0.190 |
| Characteristics | Univariate Regression Analysis | Multivariate Regression Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Entropy | 4.37 | 1.05–18.30 | 0.04 * | 3.42 × 1075 | 0.02–5.94 × 10153 | 0.06 |
| Difference entropy | 8.15 | 0.99–66.94 | 0.05 * | 1.67 × 1016 | 0.01–4.14 × 1040 | 0.19 |
| Sum entropy | 3.93 | 1.01–15.32 | 0.05 * | 0.01 | 0.01–0.22 | 0.04 * |
| Kurtosis | 0.85 | 0.73–1.01 | 0.04 * | 0.90 | 0.25–3.25 | 0.87 |
| Skewness | 0.40 | 0.16–0.95 | 0.04 * | 0.01 | 0.01–63.14 | 0.29 |
| Dissimilarity | 2.30 | 0.97–5.48 | 0.06 * | 0.01 | 0.01–525.21 | 0.16 |
| Inverse difference | 0.03 | 0.01–0.95 | 0.05 * | 1.40 × 1061 | 0.35–5.58 × 10122 | 0.05 |
| Maximum probability | 0.02 | 0.01–0.47 | 0.04 * | 0.01 | 0.01–2.21 × 1042 | 0.58 |
| GGO% | 1.04 | 0.97–1.09 | 0.09 * | 1.10 | 0.99–1.22 | 0.07 |
| Honeycombing% | 0.75 | 0.21–2.73 | 0.67 | |||
| Reticulation% | 1.06 | 0.84–1.34 | 0.62 | |||
| Emphysema% | 1.04 | 0.89–1.13 | 0.92 | |||
| Age | 1.08 | 0.98–1.19 | 0.13 | |||
| Sex | 4.29 | 0.65–28.26 | 0.13 | |||
| Smoking | 1.40 | 0.30–6.62 | 0.67 | |||
| Characteristics | Cut-Off | AUC | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|---|---|
| Entropy | >7.95 | 0.76 [0.55–0.90] | 100.0 | 58.33 | 80.77 |
| Difference entropy | >6.39 | 0.74 [0.54–0.89] | 78.57 | 75.00 | 76.92 |
| Sum entropy | >9.60 | 0.75 [0.54–0.89] | 100.00 | 58.33 | 80.77 |
| Kurtosis | ≤19.45 | 0.73 [0.52–0.88] | 85.71 | 66.67 | 76.92 |
| Skewness | ≤4.98 | 0.76 [0.56–0.91] | 92.86 | 66.67 | 80.77 |
| Dissimilarity | >5.62 | 0.76 [0.55–0.90] | 92.86 | 58.33 | 76.92 |
| Inverse difference | ≤0.90 | 0.77 [0.56–0.91] | 78.57 | 75.00 | 76.92 |
| Maximum probability | ≤0.09 | 0.74 [0.54–0.89] | 85.71 | 66.67 | 76.92 |
| GGO% | >16.00 | 0.69 [0.48–0.85] | 57.14 | 75.00 | 65.38 |
| Sum entropy + GGO% | 0.77 [0.56–0.91] | 100.00 | 75.00 | 88.46 | |
| GAP index | >3 | 0.77 [0.56–0.91] | 78.57 | 66.67 | 73.07 |
| GAP stage | >1 | 0.73 [0.52–0.88] | 78.57 | 66.67 | 73.07 |
| Characteristics | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|
| Entropy | 50.00 | 71.43 | 66.67 |
| Difference entropy | 50.00 | 85.71 | 77.78 |
| Sum entropy | 50.00 | 71.43 | 66.67 |
| Kurtosis | 50.00 | 42.86 | 44.44 |
| Skewness | 50.00 | 28.57 | 33.33 |
| Dissimilarity | 50.00 | 85.71 | 77.78 |
| Inverse difference | 50.00 | 71.43 | 66.67 |
| Maximum probability | 50.00 | 71.43 | 66.67 |
| GGO% | 50.00 | 50.00 | 50.00 |
| Sum entropy + GGO% | 50.00 | 74.43 | 66.67 |
| GAP index | 100.00 | 16.67 | 37.50 |
| GAP stage | 100.00 | 16.67 | 37.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.-C.; Chen, C.-Y.; Kuo, Y.-T.; Ko, C.-C.; Wu, W.-J.; Liang, C.-H.; Yun, C.-H.; Huang, W.-M. Radiomics for the Prediction of Response to Antifibrotic Treatment in Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study. Diagnostics 2022, 12, 1002. https://doi.org/10.3390/diagnostics12041002
Yang C-C, Chen C-Y, Kuo Y-T, Ko C-C, Wu W-J, Liang C-H, Yun C-H, Huang W-M. Radiomics for the Prediction of Response to Antifibrotic Treatment in Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study. Diagnostics. 2022; 12(4):1002. https://doi.org/10.3390/diagnostics12041002
Chicago/Turabian StyleYang, Cheng-Chun, Chin-Yu Chen, Yu-Ting Kuo, Ching-Chung Ko, Wen-Jui Wu, Chia-Hao Liang, Chun-Ho Yun, and Wei-Ming Huang. 2022. "Radiomics for the Prediction of Response to Antifibrotic Treatment in Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study" Diagnostics 12, no. 4: 1002. https://doi.org/10.3390/diagnostics12041002
APA StyleYang, C. -C., Chen, C. -Y., Kuo, Y. -T., Ko, C. -C., Wu, W. -J., Liang, C. -H., Yun, C. -H., & Huang, W. -M. (2022). Radiomics for the Prediction of Response to Antifibrotic Treatment in Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study. Diagnostics, 12(4), 1002. https://doi.org/10.3390/diagnostics12041002