
LumiraDX SARS-CoV-2 Antigen Test for Diagnosing Acute SARS-CoV-2 Infection: Critical Literature Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Immunoassay Description
2.2. Search Strategy
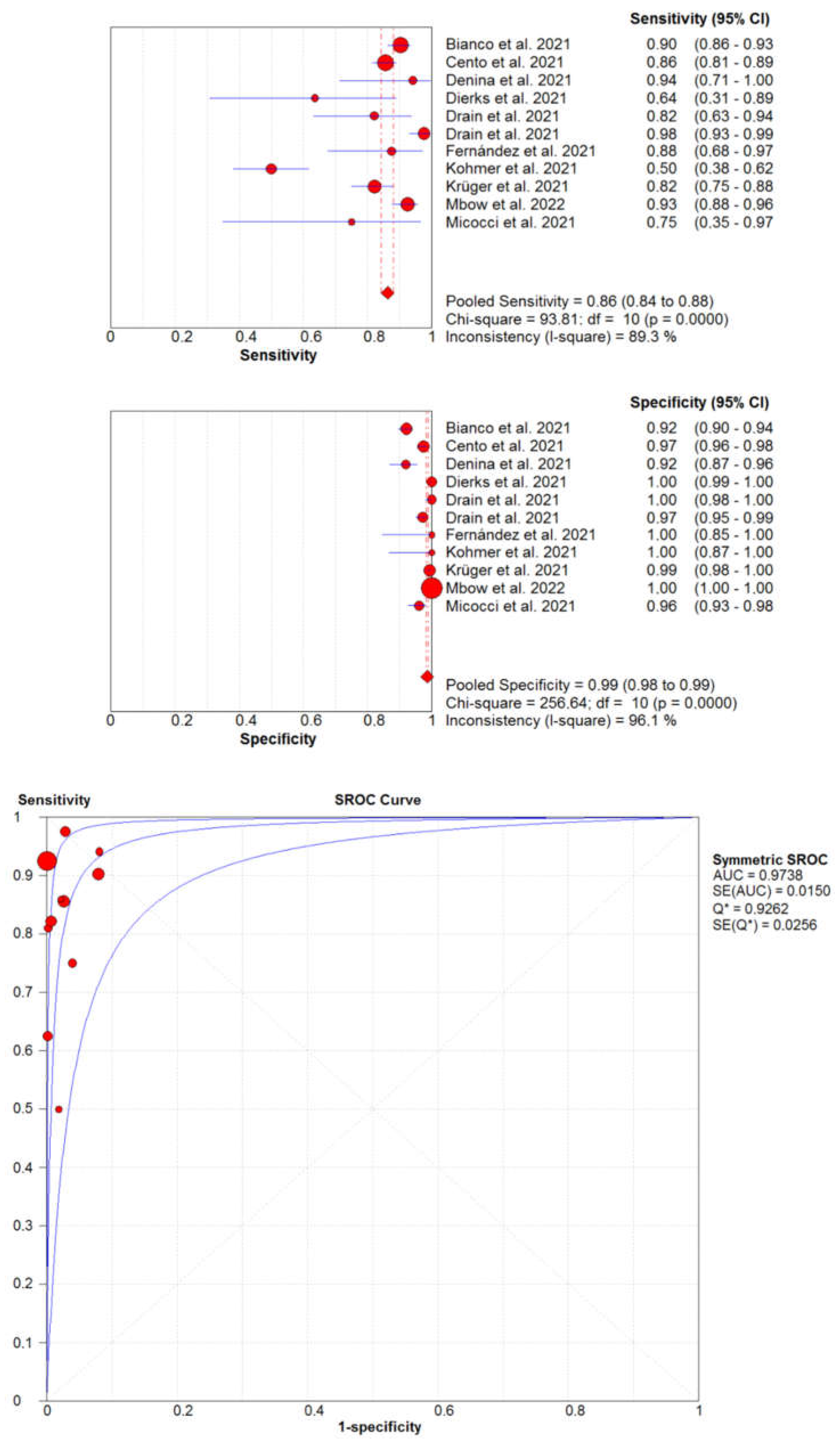
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. Coronavirus disease 2019 (COVID-19): The portrait of a perfect storm. Ann. Transl. Med. 2020, 8, 497. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C.; Henry, B.M. Updated picture of SARS-CoV-2 variants and mutations. Diagnosis 2021, 9, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.K.; Mancini, N.; Loh, T.P.; Wang, C.B.; Grimmler, M.; Gramegna, M.; Yuen, K.Y.; Mueller, R.; Koch, D.; Sethi, S. IFCC Interim Guidelines on Molecular Testing of SARS-CoV-2 Infection. Clin. Chem. Lab. Med. 2020, 58, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- FIND. SARS-CoV-2 Diagnostic Pipeline. Available online: https://www.finddx.org/covid-19/pipeline/ (accessed on 1 February 2022).
- Brümmer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, 1003735. [Google Scholar] [CrossRef]
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection—Interim Guidance. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 1 February 2022).
- Bohn, M.K.; Lippi, G.; Horvath, A.R.; Erasmus, R.; Grimmler, M.; Gramegna, M.; Mancini, N.; Mueller, R.; Rawlinson, W.D.; Menezes, M.E.; et al. IFCC interim guidelines on rapid point-of-care antigen testing for SARS-CoV-2 detection in asymptomatic and symptomatic individuals. Clin. Chem. Lab. Med. 2021, 59, 1507–1515. [Google Scholar] [CrossRef]
- Lippi, G.; Horvath, A.R.; Adeli, K. Editorial and Executive Summary: IFCC Interim Guidelines on Clinical Laboratory testing during the COVID-19 Pandemic. Clin. Chem. Lab. Med. 2020, 58, 1965–1969. [Google Scholar] [CrossRef]
- Schlattmann, P. Statistics in diagnostic medicine. Clin. Chem. Lab. Med. 2022, epub ahead of print. [Google Scholar] [CrossRef]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef]
- Bianco, G.; Boattini, M.; Barbui, A.M.; Scozzari, G.; Riccardini, F.; Coggiola, M.; Lupia, E.; Cavallo, R.; Costa, C. Evaluation of an antigen-based test for hospital point-of-care diagnosis of SARS-CoV-2 infection. J. Clin. Virol. 2021, 139, 104838. [Google Scholar] [CrossRef]
- Cento, V.; Renica, S.; Matarazzo, E.; Antonello, M.; Colagrossi, L.; Di Ruscio, F.; Pani, A.; Fanti, D.; Vismara, C.; Puoti, M.; et al. Frontline Screening for SARS-CoV-2 Infection at Emergency Department Admission by Third Generation Rapid Antigen Test: Can We Spare RT-qPCR? Viruses 2021, 13, 818. [Google Scholar] [CrossRef]
- Denina, M.; Giannone, V.; Curtoni, A.; Zanotto, E.; Garazzino, S.; Urbino, A.F.; Bondone, C. Can we trust in SARS-CoV-2 rapid antigen testing? Preliminary results from a paediatric cohort in the emergency department. Ir. J. Med. Sci. 2021; epub ahead of print. [Google Scholar] [CrossRef]
- Dierks, S.; Bader, O.; Schwanbeck, J.; Groß, U.; Weig, M.; Mese, K.; Lugert, R.; Bohne, W.; Hahn, A.; Feltgen, N.; et al. Diagnosing SARS-CoV-2 with Antigen Testing, Transcription-Mediated Amplification and Real-Time PCR. J. Clin. Med. 2021, 10, 2404. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.; Sulaiman, R.; Hoppers, M.; Lindner, N.M.; Lawson, V.; Ellis, J.E. Performance of the LumiraDx Microfluidic Immunofluorescence Point-of-Care SARS-CoV-2 Antigen Test in Asymptomatic Adults and Children. Am. J. Clin. Pathol. 2022, 157, 602–607. [Google Scholar] [CrossRef]
- Drain, P.K.; Ampajwala, M.; Chappel, C.; Gvozden, A.B.; Hoppers, M.; Wang, M.; Rosen, R.; Young, S.; Zissman, E.; Montano, M. A Rapid, High-Sensitivity SARS-CoV-2 Nucleocapsid Immunoassay to Aid Diagnosis of Acute COVID-19 at the Point of Care: A Clinical Performance Study. Infect. Dis. 2021, 10, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.D.; Estévez, A.S.; Alfonsín, F.L.; Bou, G. Utilidad del test de antígenos SARS-CoV-2 de LumiraDX™ en centros residenciales [Usefulness of the LumiraDX ™ SARS-CoV-2 antigen test in nursing home]. Enferm. Infecc. Microbiol. Clin. 2021; epub ahead of print. [Google Scholar] [CrossRef]
- Kohmer, N.; Toptan, T.; Pallas, C.; Karaca, O.; Pfeiffer, A.; Westhaus, S.; Widera, M.; Berger, A.; Hoehl, S.; Kammel, M.; et al. The Comparative Clinical Performance of Four SARS-CoV-2 Rapid Antigen Tests and Their Correlation to Infectivity In Vitro. J. Clin. Med. 2021, 17, 328. [Google Scholar] [CrossRef] [PubMed]
- Krüger, L.J.; Klein, J.A.F.; Tobian, F.; Gaeddert, M.; Lainati, F.; Klemm, S.; Schnitzler, P.; Bartenschlager, R.; Cerikan, B.; Neufeldt, C.J.; et al. Evaluation of accuracy, exclusivity, limit-of-detection and ease-of-use of LumiraDx™: An antigen-detecting point-of-care device for SARS-CoV-2. Infection 2022, 50, 395–406. [Google Scholar] [CrossRef]
- Mbow, M.; Diallo, I.; Diouf, M.; Cissé, M.; Mboup, M.G.A.; Leye, N.; Lo, G.; Dia, Y.A.; Padane, A.; Wade, D.; et al. Evaluation of the LumiraDx SARS-CoV-2 antigen assay for large-scale population testing in Senegal. Int. J. Clin. Virol. 2022, 6, 1–6. [Google Scholar]
- Micocci, M.; Buckle, P.; Hayward, G.; Allen, A.J.; Davies, K.; Kierkegaard, P.; Spilsbury, K.; Thompson, C.; Astle, A.; Heath, R.; et al. Point of care testing using rapid automated antigen testing for SARS-CoV-2 in care homes—An exploratory safety, usability and diagnostic agreement evaluation. J. Patient Saf. Risk Manag. 2021, 26, 243–250. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Burdino, E.; Cerutti, F.; Panero, F.; Allice, T.; Gregori, G.; Milia, M.G.; Cavalot, G.; Altavilla, A.; Aprà, F.; Ghisetti, V. SARS-CoV-2 microfluidic antigen point-of-care testing in Emergency Room patients during COVID-19 pandemic. J. Virol. Methods 2022, 299, 114337. [Google Scholar] [CrossRef] [PubMed]
- Gresh, J.; Kisner, H.; DuChateau, B. Urgent care study of the LumiraDx SARS-CoV-2 Ag Test for rapid diagnosis of COVID-19. Diagn. Progn. Res. 2021, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Greub, G.; Caruana, G.; Schweitzer, M.; Imperiali, M.; Muigg, V.; Risch, M.; Croxatto, A.; Opota, O.; Heller, S.; Albertos Torres, D.; et al. Multicenter Technical Validation of 30 Rapid Antigen Tests for the Detection of SARS-CoV-2 (VALIDATE). Microorganisms 2021, 9, 2589. [Google Scholar] [CrossRef]
- Karon, B.S.; Donato, L.J.; Bridgeman, A.R.; Blommel, J.H.; Kipp, B.; Maus, A.; Renuse, S.; Kemp, J.; Madugundu, A.K.; Vanderboom, P.M.; et al. Analytical Sensitivity and Specificity of Four Point of Care Rapid Antigen Diagnostic Tests for SARS-CoV-2 Using Real-Time Quantitative PCR, Quantitative Droplet Digital PCR, and a Mass Spectrometric Antigen Assay as Comparator Methods. Clin. Chem. 2021, 67, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Scheiblauer, H.; Filomena, A.; Nitsche, A.; Puyskens, A.; Corman, V.M.; Drosten, C.; Zwirglmaier, K.; Lange, C.; Emmerich, P.; Müller, M.; et al. Comparative sensitivity evaluation for 122 CE-marked rapid diagnostic tests for SARS-CoV-2 antigen, Germany, September 2020 to April 2021. Euro Surveill. 2021, 26, 21004416. [Google Scholar] [CrossRef] [PubMed]
- Scheiblauer, H.; Filomena, A.; Nitsche, A.; Puyskens, A.; Corman, V.M.; Drosten, C.; Zwirglmaier, K.; Lange, C.; Emmerich, P.; Müller, M. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Henry, B.M. Neutralizing potency of COVID-19 vaccines against the SARS-CoV-2 Omicron (B.1.1.529) variant. J. Med. Virol. 2022, 94, 1799–1802. [Google Scholar] [CrossRef]
- American Association of Clinical Chemistry. Coronavirus Testing Survey. Available online: https://www.aacc.org/science-and-research/covid-19-resources/aacc-covid-19-testing-survey (accessed on 1 February 2022).
- Thakur, V.; Ratho, R.K. OMICRON (B.1.1.529): A new SARS-CoV-2 variant of concern mounting worldwide fear. J. Med. Virol. 2022, 94, 1821–1824. [Google Scholar] [CrossRef]
- Khalid, M.F.; Selvam, K.; Jeffry, A.J.N.; Salmi, M.F.; Najib, M.A.; Norhayati, M.N.; Aziah, I. Performance of Rapid Antigen Tests for COVID-19 Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 110. [Google Scholar] [CrossRef]
- Fujita-Rohwerder, N.; Beckmann, L.; Zens, Y.; Verma, A. Diagnostic accuracy of rapid point-of-care tests for diagnosis of current SARS-CoV-2 infections in children: A systematic review and meta-analysis. BMJ Evid. Based Med. 2022, epub ahead of print. [Google Scholar] [CrossRef]
- Chen, C.C.; Lu, S.C.; Bai, C.H.; Wang, P.Y.; Lee, K.Y.; Wang, Y.H. Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11451. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Gianfilippi, G.; Fiorio, G.; Pighi, L.; De Nitto, S.; Henry, B.M.; Lippi, G. Clinical Assessment of the DiaSorin LIAISON SARS-CoV-2 Ag Chemiluminescence Immunoassay. EJIFCC 2021, 32, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Adeli, K. Diagnostic performance of the fully automated Roche Elecsys SARS-CoV-2 antigen electrochemiluminescence immunoassay: A pooled analysis. Clin. Chem. Lab. Med. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Levett, P.N.; Cheung, B.; Kustra, J.; Pidduck, T.; Mak, A.; Tsang, F.; Petric, M.; Krajden, M. Evaluation of a high volume antigen test for detection of SARS-CoV-2. J. Clin. Virol. 2021, 142, 104938. [Google Scholar] [CrossRef] [PubMed]
- Caputo, V.; Bax, C.; Colantoni, L.; Peconi, C.; Termine, A.; Fabrizio, C.; Calvino, G.; Luzzi, L.; Panunzi, G.G.; Fusco, C.; et al. Comparative analysis of antigen and molecular tests for the detection of SARS-CoV-2 and related variants: A study on 4266 samples. Int. J. Infect. Dis. 2021, 108, 187–189. [Google Scholar] [CrossRef]
- Lau, M.S.; Grenfell, B.; Thomas, M.; Bryan, M.; Nelson, K.; Lopman, B. Characterizing superspreading events and age-specific infectiousness of SARS-CoV-2 transmission in Georgia, USA. Proc. Natl. Acad. Sci. USA 2020, 117, 22430–22435. [Google Scholar] [CrossRef]


{kind=link}
| Items | Specification |
|---|---|
| Date of Search | 1 February 2022 |
| Databases and other sources searched | Scopus, Medline (PubMed interface) |
| Search terms used | “LumiraDX” AND “COVID-19” or “SARS-CoV-2” |
| Timeframe | Up to 1 February 2022 |
| Inclusion and exclusion criteria | No date or language restrictions, clinical studies where the rates of true positive (TP), true negative (TN), false positive (FP) and false negative (FN) cases compared to reference SARS-CoV-2 molecular biology techniques were available for constructing a 2 × 2 table |
| Selection process | Conducted by G.L., verified by B.M.H. |
| Study | Country | Sample Matrix | Sample Size (n) | Population | Molecular Assay (Gene Targets) |
|---|---|---|---|---|---|
| Bianco et al. 2021 [11] | Italy | NS and NPS | 907 | Median age 48 (range, 0.2–94) years; 56% females | Cepheid Xpert Xpress SARS-CoV-2 PCR |
| Cento et al. 2021 [12] | Italy | NPS | 959 | Median age 66 (IQR, 45–79) years; 42.2% females | In-house |
| Denina et al. 2021 [13] | Italy | NPS | 191 | Median age 5.8 (IQR, 1.1–10.8) years, 46% females | Diasorin Simplexa COVID-19 Direct kit |
| Dierks et al. 2021 [14] | Germany | NPS | 444 | N/A | Primerdesign Genesig Real-Time PCR Coronavirus (COVID-19) assay, Cepheid Xpert Xpress SARS-CoV-2 PCR and Roche Cobas 6800 SARS-CoV-2 Test |
| Drain et al. 2021 [15] | USA | NS | 222 | Mean age, 39 ± 17 years; 63% females | Roche Cobas 6800 SARS-CoV-2 Test and Thermo Fisher TruGenX |
| Drain et al. 2021 [16] | USA | NS and NPS | 512 | Mean age, 34 ± 19 years; 56% females | Roche Cobas 6800 SARS-CoV-2 Test |
| Fernández et al. 2021 [17] | Spain | NS and NPS | 46 | N/A | Seegene Allplex SARS-CoV-2 assay |
| Kohmer et al. 2021 [18] | Germany | NPS | 100 | N/A | Roche Cobas 6800 SARS-CoV-2 Test |
| Krüger et al. 2021 [19] | Germany | NPS | 761 | Median, 35 (IQR, 27–42) years; 52% females | Seegene Allplex SARS-CoV-2 assay and Roche Cobas 6800 SARS-CoV-2 Test |
| Mbow et al. 2022 [20] | Senegal | OPS and NPS | 4146 | Age range, 2–96 years; 47% females | Seegene Allplex SARS-CoV-2 assay |
| Micocci et al. 2021 [21] | Italy | NS | 239 | N/A | N/A |
| Study | Country | Sample Matrix | Sample Size | Sensitivity | Specificity | Accuracy |
|---|---|---|---|---|---|---|
| Burdino et al. 2021 [23] | Italy | NS and NPS | 1232 | 0.90 (95%CI, 0.86–0.93) | 0.99 (95%CI, 0.99–1.00) | Concordance: 96.9% |
| Gresh et al. 2021 [24] | USA | NS | 2241 | N/A | 1.00 (95%CI, 0.99–1.00) | Agreement: 96.3% |
| Greub et al. 2021 [25] | Switzerland | NPS | 200 | 0.99 (95%CI, 0.93–1.00) | 0.99 (95%CI, 0.99–1.00) | N/A |
| Karon et al. 2021 [26] | USA | NPS | 350 | 0.83 (95%CI, 0.77–0.88) | 1.00 (95%CI, 0.98–1.00) | N/A |
| Scheiblauer et al. 2021 [27] | Germany | OPS and NPS | 50 | 0.60 (95%CI, N/A) | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippi, G.; Henry, B.M.; Plebani, M. LumiraDX SARS-CoV-2 Antigen Test for Diagnosing Acute SARS-CoV-2 Infection: Critical Literature Review and Meta-Analysis. Diagnostics 2022, 12, 947. https://doi.org/10.3390/diagnostics12040947
Lippi G, Henry BM, Plebani M. LumiraDX SARS-CoV-2 Antigen Test for Diagnosing Acute SARS-CoV-2 Infection: Critical Literature Review and Meta-Analysis. Diagnostics. 2022; 12(4):947. https://doi.org/10.3390/diagnostics12040947
Chicago/Turabian StyleLippi, Giuseppe, Brandon M. Henry, and Mario Plebani. 2022. "LumiraDX SARS-CoV-2 Antigen Test for Diagnosing Acute SARS-CoV-2 Infection: Critical Literature Review and Meta-Analysis" Diagnostics 12, no. 4: 947. https://doi.org/10.3390/diagnostics12040947
APA StyleLippi, G., Henry, B. M., & Plebani, M. (2022). LumiraDX SARS-CoV-2 Antigen Test for Diagnosing Acute SARS-CoV-2 Infection: Critical Literature Review and Meta-Analysis. Diagnostics, 12(4), 947. https://doi.org/10.3390/diagnostics12040947