
Pathological Evaluation of Rectal Cancer Specimens Using Micro-Computed Tomography


 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Materials
2.2. Whole-Slide Imaging Analysis
2.3. Whole-Block Imaging Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
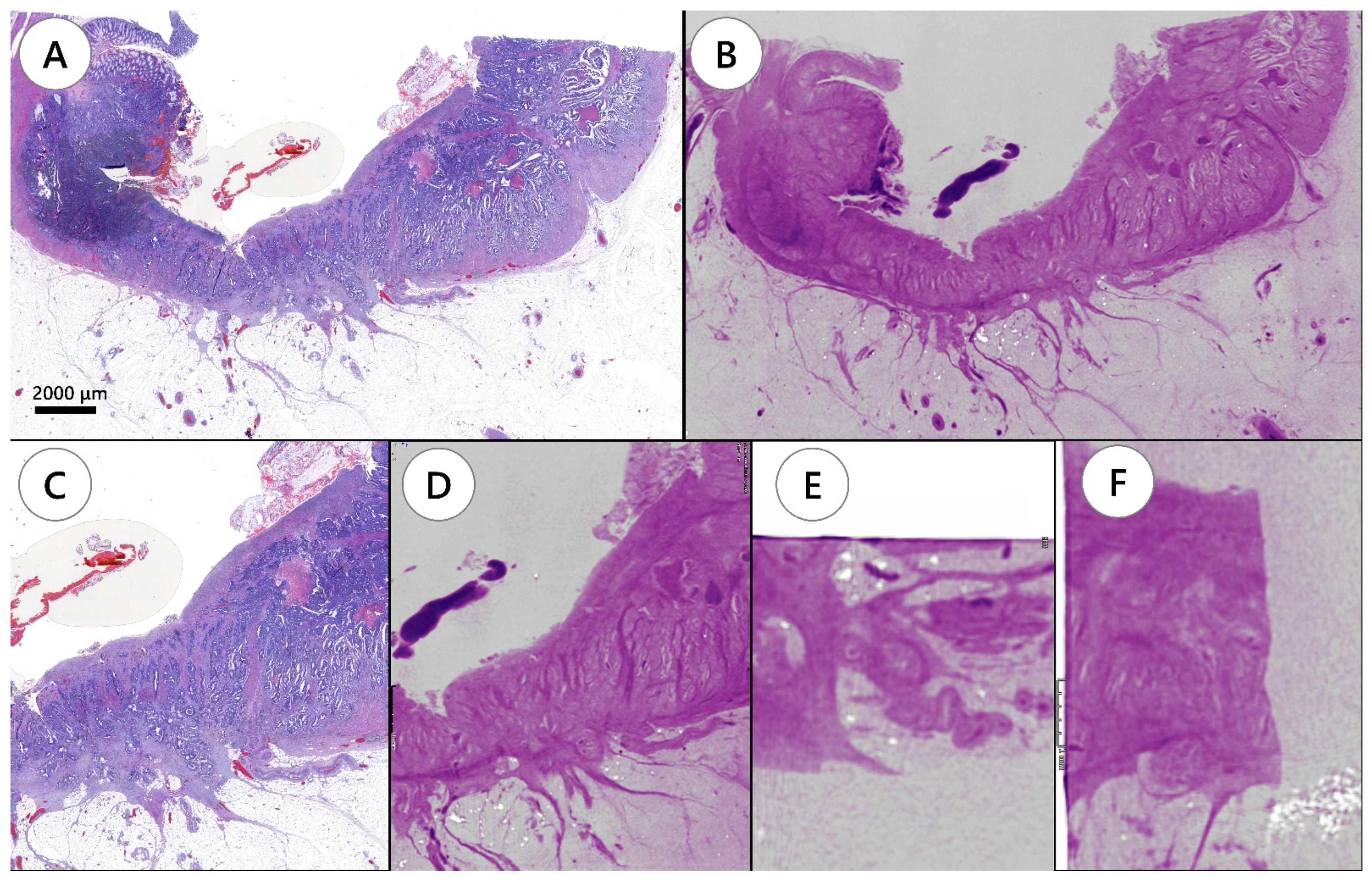
3.2. Pathological Tumor Staging
3.3. Circumferential Resection Margin
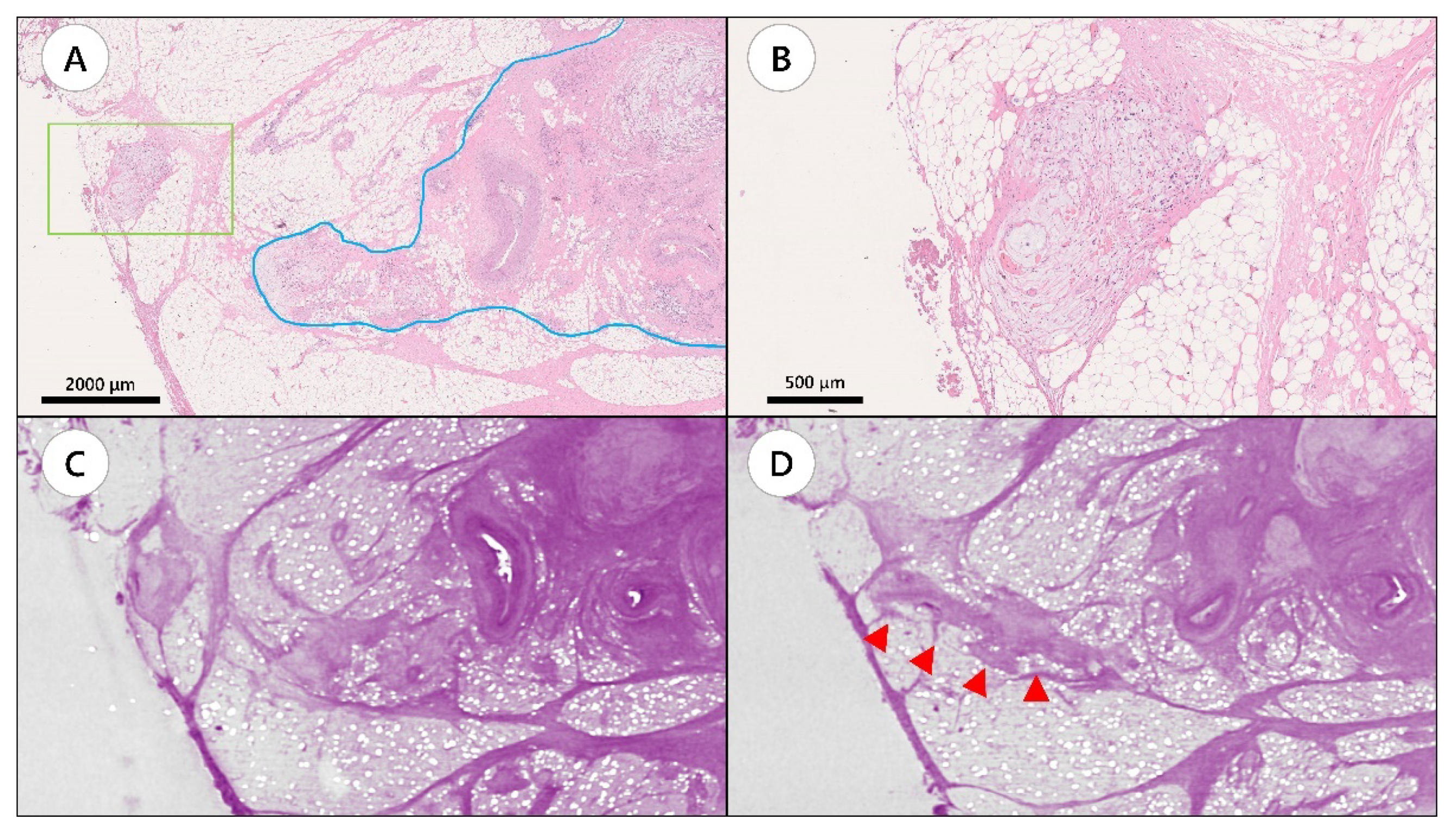
3.4. Tumor Deposits, Lymphovascular Invasion, and Perineural Invasion
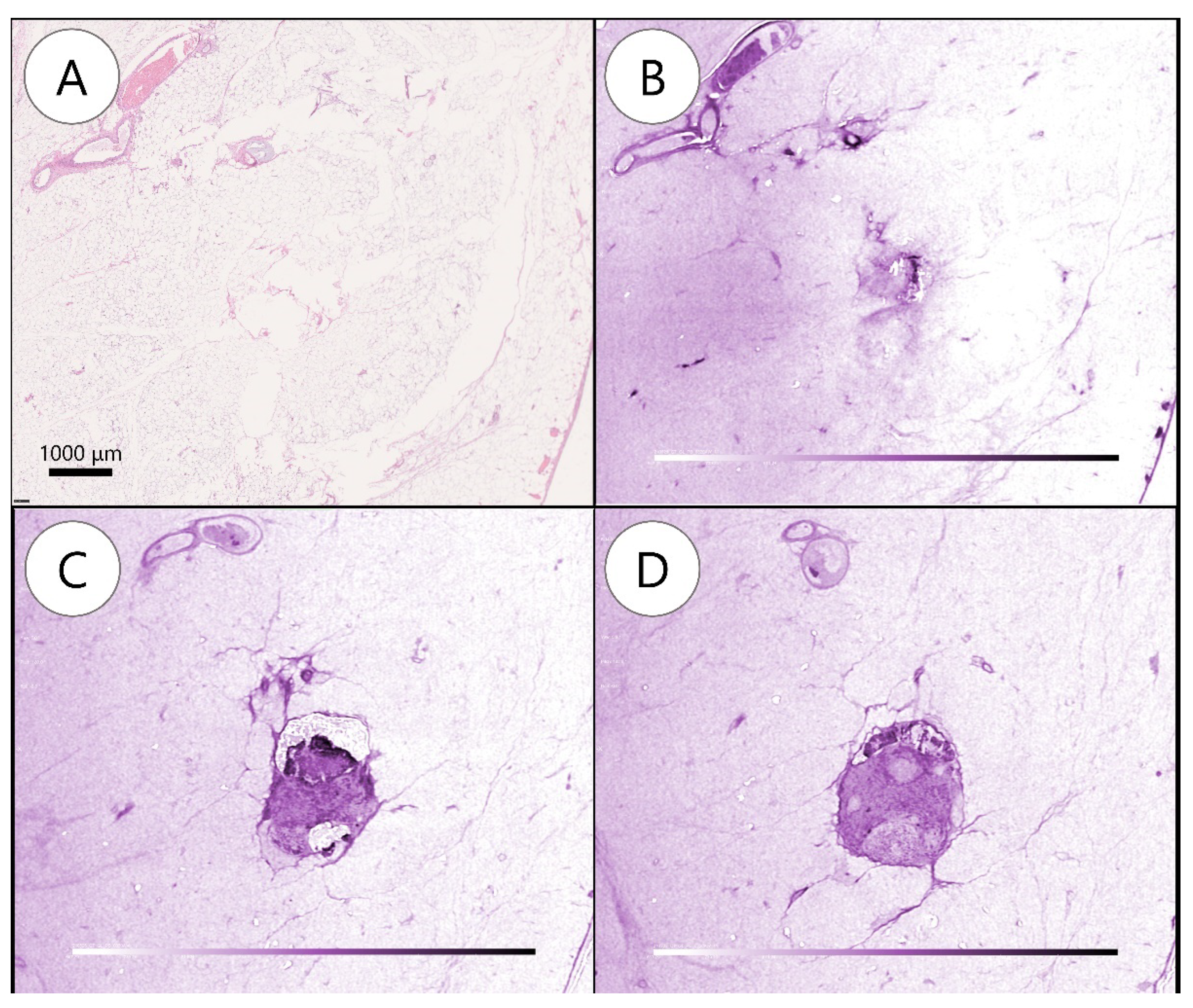
3.5. Lymph Node Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal Cancer Statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrick, J.L.; Barber, L.E.; Warren Andersen, S.; Florio, A.A.; Palmer, J.R.; Rosenberg, L. Racial Disparities and Sex Differences in Early- and Late-Onset Colorectal Cancer Incidence, 2001–2018. Front. Oncol. 2021, 11, 734998. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wang, W. Serum hsa-miR-30e as a Potential Biomarker to Predict the Effect of Neoadjuvant Chemoradiation Therapy in Locally Advanced Rectal Cancer. Genet. Test. Mol. Biomark. 2021, 25, 696–706. [Google Scholar] [CrossRef]
- Weiser, M.R.; Quah, H.M.; Shia, J.; Guillem, J.G.; Paty, P.B.; Temple, L.K.; Goodman, K.A.; Minsky, B.D.; Wong, W.D. Sphincter Preservation in Low Rectal Cancer Is Facilitated by Preoperative Chemoradiation and Intersphincteric Dissection. Ann. Surg. 2009, 249, 236–242. [Google Scholar] [CrossRef]
- Leibold, T.; Shia, J.; Ruo, L.; Minsky, B.D.; Akhurst, T.; Gollub, M.J.; Ginsberg, M.S.; Larson, S.; Riedel, E.; Wong, W.D.; et al. Prognostic Implications of the Distribution of Lymph Node Metastases in Rectal Cancer After Neoadjuvant Chemoradiotherapy. J. Clin. Oncol. 2008, 26, 2106–2111. [Google Scholar] [CrossRef]
- Quah, H.M.; Chou, J.F.; Gonen, M.; Shia, J.; Schrag, D.; Saltz, L.B.; Goodman, K.A.; Minsky, B.D.; Wong, W.D.; Weiser, M.R. Pathologic Stage Is Most Prognostic of Disease-Free Survival in Locally Advanced Rectal Cancer Patients After Preoperative Chemoradiation. Cancer 2008, 113, 57–64. [Google Scholar] [CrossRef]
- Trakarnsanga, A.; Gonen, M.; Shia, J.; Goodman, K.A.; Nash, G.M.; Temple, L.K.; Guillem, J.G.; Paty, P.B.; Garcia-Aguilar, J.; Weiser, M.R. What Is the Significance of the Circumferential Margin in Locally Advanced Rectal Cancer After Neoadjuvant Chemoradiotherapy? Ann. Surg. Oncol. 2013, 20, 1179–1184. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.V.; Roxburgh, C.S.; Vakiani, E.; Shia, J.; Smith, J.J.; Temple, L.K.; Paty, P.; Garcia-Aguilar, J.; Nash, G.; Guillem, J.; et al. Distance to the Anal Verge Is Associated With Pathologic Complete Response to Neoadjuvant Therapy in Locally Advanced Rectal Cancer. J. Surg. Oncol. 2016, 114, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.D.B.; Mazaheri, Y.; Lobaugh, S.; Golia Pernicka, J.S.; Paroder, V.; Shia, J.; Zheng, J.; Capanu, M.; Petkovska, I.; Gollub, M.J. Evaluation of Diffusion Kurtosis and Diffusivity From Baseline Staging MRI as Predictive Biomarkers for Response to Neoadjuvant Chemoradiation in Locally Advanced Rectal Cancer. Abdom. Radiol. 2019, 44, 3701–3708. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R.; Chou, J.F.; Keshinro, A.; Chapman, W.C.; Bauer, P.S.; Mutch, M.G.; Parikh, P.J.; Cercek, A.; Saltz, L.B.; Gollub, M.J.; et al. Development and Assessment of a Clinical Calculator for Estimating the Likelihood of Recurrence and Survival Among Patients With Locally Advanced Rectal Cancer Treated With Chemotherapy, Radiotherapy, and Surgery. JAMA Network Open 2021, 4, e2133457. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl Compr. Canc. Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, T.D.; Fakih, M.G.; Yang, G.Y. Management of stage II/III Rectal Cancer. J. Gastrointest. Oncol. 2010, 1, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Mezhir, J.J.; Shia, J.; Riedel, E.; Temple, L.K.; Nash, G.M.; Weiser, M.R.; Paty, P.B.; Wong, W.D.; Guillem, J.G. Whole-Mount Pathologic Analysis of Rectal Cancer Following Neoadjuvant Therapy: Implications of Margin Status on Long-Term Oncologic Outcome. Ann. Surg. 2012, 256, 274–279. [Google Scholar] [CrossRef]
- Guillem, J.G.; Chessin, D.B.; Shia, J.; Suriawinata, A.; Riedel, E.; Moore, H.G.; Minsky, B.D.; Wong, W.D. A Prospective Pathologic Analysis Using Whole-Mount Sections of Rectal Cancer Following Preoperative Combined Modality Therapy: Implications for Sphincter Preservation. Ann. Surg. 2007, 245, 88–93. [Google Scholar] [CrossRef]
- Ohnishi, T.; Teplov, A.; Kawata, N.; Ibrahim, K.; Ntiamoah, P.; Firat, C.; Haneishi, H.; Hameed, M.; Shia, J.; Yagi, Y. Three-Dimensional Vessel Segmentation in Whole-Tissue and Whole-Block Imaging Using a Deep Neural Network: Proof-of-Concept Study. Am. J. Pathol. 2021, 191, 463–474. [Google Scholar] [CrossRef]
- DiCorpo, D.; Tiwari, A.; Tang, R.; Griffin, M.; Aftreth, O.; Bautista, P.; Hughes, K.; Gershenfeld, N.; Michaelson, J. The Role of Micro-CT in Imaging Breast Cancer Specimens. Breast Cancer Res. Treat. 2020, 180, 343–357. [Google Scholar] [CrossRef]
- Sarraj, W.M.; Tang, R.; Najjar, A.L.; Griffin, M.; Bui, A.H.; Zambeli-Ljepovic, A.; Senter-Zapata, M.; Lewin-Berlin, M.; Fernandez, L.; Buckley, J.; et al. Prediction of Primary Breast Cancer Size and T-Stage Using Micro-Computed Tomography in Lumpectomy Specimens. J. Pathol. Inform. 2015, 6, 60. [Google Scholar] [CrossRef]
- Xu, B.; Teplov, A.; Ibrahim, K.; Inoue, T.; Stueben, B.; Katabi, N.; Hameed, M.; Yagi, Y.; Ghossein, R. Detection and Assessment of Capsular Invasion, Vascular Invasion and Lymph Node Metastasis Volume in Thyroid Carcinoma Using microCT Scanning of Paraffin Tissue Blocks (3D Whole Block Imaging): A Proof of Concept. Mod. Pathol. 2020, 33, 2449–2457. [Google Scholar] [CrossRef]
- Troschel, F.M.; Gottumukkala, R.V.; DiCorpo, D.; Mario, J.; Ott, H.C.; Wright, C.D.; Muniappan, A.; Lanuti, M.; Yang, K.; Shepard, J.O.; et al. Feasibility of Perioperative Micro-Computed Tomography of Human Lung Cancer Specimens: A Pilot Study. Arch. Pathol. Lab. Med. 2019, 143, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Yagi, Y.; Aly, R.G.; Tabata, K.; Barlas, A.; Rekhtman, N.; Eguchi, T.; Montecalvo, J.; Hameed, M.; Manova-Todorova, K.; Adusumilli, P.S.; et al. Three-Dimensional Histologic, Immunohistochemical, and Multiplex Immunofluorescence Analyses of Dynamic Vessel Co-Option of Spread Through Air Spaces in Lung Adenocarcinoma. J. Thorac. Oncol. 2020, 15, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Boyce, B.F. An Update on the Validation of Whole Slide Imaging Systems Following FDA Approval of a System for a Routine Pathology Diagnostic Service in the United States. Biotech. Histochem. 2017, 92, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.G.; Reuter, V.E.; Hameed, M.R.; Tan, L.K.; Chiang, S.; Sigel, C.; Hollmann, T.; Giri, D.; Samboy, J.; Moradel, C.; et al. Whole Slide Imaging Equivalency and Efficiency Study: Experience at a Large Academic Center. Mod. Pathol. 2019, 32, 916–928. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R.; AJCC. AJCC 8th Edition: Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 1454–1455. [Google Scholar] [CrossRef] [Green Version]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Mehrkhani, F.; Nasiri, S.; Donboli, K.; Meysamie, A.; Hedayat, A. Prognostic Factors in Survival of Colorectal Cancer Patients After Surgery. Colorectal Dis. 2009, 11, 157–161. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-Based to a More “Personalized” Approach to Cancer Staging 8th edition. CA Cancer J. Clin. Mar. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Quirke, P.; Durdey, P.; Dixon, M.F.; Williams, N.S. Local Recurrence of Rectal Adenocarcinoma Due to Inadequate Surgical Resection. Histopathological Study of Lateral Tumour Spread and Surgical Excision. Lancet 1986, 2, 996–999. [Google Scholar] [CrossRef]
- Shia, J.; McManus, M.; Guillem, J.G.; Leibold, T.; Zhou, Q.; Tang, L.H.; Riedel, E.R.; Weiser, M.R.; Paty, P.B.; Temple, L.K.; et al. Significance of Acellular Mucin Pools in Rectal Carcinoma After Neoadjuvant Chemoradiotherapy. Am. J. Surg. Pathol. 2011, 35, 127–134. [Google Scholar] [CrossRef]
- Zheng, K.; Zheng, N.; Xin, C.; Zhou, L.; Sun, G.; Wen, R.; Zhang, H.; Yu, G.; Bai, C.; Zhang, W. The Prognostic Significance of Tumor Deposit Count for Colorectal Cancer Patients After Radical Surgery. Gastroenterol. Res. Pract. 2020, 2020, 2052561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for Management of Patients with Colon and Rectal Cancer. A Personalized Approach to Clinical Decision Making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef] [PubMed]
- Beaufrère, A.; Guedj, N.; Maggiori, L.; Patroni, A.; Bedossa, P.; Panis, Y. Circumferential Margin Involvement After Total Mesorectal Excision for Mid or Low Rectal Cancer: Are All R1 Resections Equal? Colorectal Dis. 2017, 19, O377–O385. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Luo, D.; Cai, S.; Li, Q.; Li, X. Circumferential Resection Margin as a Prognostic Factor After Rectal Cancer Surgery: A Large Population-Based Retrospective Study. Cancer Med. 2018, 7, 3673–3681. [Google Scholar] [CrossRef] [Green Version]
- Santos, C.; López-Doriga, A.; Navarro, M.; Mateo, J.; Biondo, S.; Martínez Villacampa, M.; Soler, G.; Sanjuan, X.; Paules, M.J.; Laquente, B.; et al. Clinicopathological Risk Factors of Stage II Colon Cancer: Results of a Prospective Study. Colorectal Dis. 2013, 15, 414–422. [Google Scholar] [CrossRef]
- Lim, S.B.; Yu, C.S.; Jang, S.J.; Kim, T.W.; Kim, J.H.; Kim, J.C. Prognostic Significance of Lymphovascular Invasion in Sporadic Colorectal Cancer. Dis. Colon Rectum. 2010, 53, 377–384. [Google Scholar] [CrossRef]
- Betge, J.; Pollheimer, M.J.; Lindtner, R.A.; Kornprat, P.; Schlemmer, A.; Rehak, P.; Vieth, M.; Hoefler, G.; Langner, C. Intramural and Extramural Vascular Invasion in Colorectal Cancer: Prognostic Significance and Quality of Pathology Reporting. Cancer 2012, 118, 628–638. [Google Scholar] [CrossRef]
- Sun, Q.; Liu, T.; Liu, P.; Luo, J.; Zhang, N.; Lu, K.; Ju, H.; Zhu, Y.; Wu, W.; Zhang, L.; et al. Perineural and Lymphovascular Invasion Predicts for Poor Prognosis in Locally Advanced Rectal Cancer After Neoadjuvant Chemoradiotherapy and Surgery. J. Cancer 2019, 10, 2243–2249. [Google Scholar] [CrossRef] [Green Version]
- Compton, C.C.; Greene, F.L. The Staging of Colorectal Cancer: 2004 and Beyond. CA Cancer J. Clin. 2004, 54, 295–308. [Google Scholar] [CrossRef]
- Burroughs, S.H.; Williams, G.T. ACP Best Practice No 159. Examination of Large Intestine Resection Specimens. J. Clin. Pathol. 2000, 53, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Katti, S.V.; Paulose, R.R.; Malipatil, B.; Verma, N.S. Grossing and Reporting of Colorectal Cancer Resection Specimens: An Evidence-Based Approach. Indian J. Cancer 2020, 57, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Görög, D.; Nagy, P.; Péter, A.; Perner, F. Influence of Obesity on Lymph Node Recovery From Rectal Resection Specimens. Pathol. Oncol. Res. 2003, 9, 180–183. [Google Scholar] [CrossRef] [Green Version]
- Wijesuriya, R.E.; Deen, K.I.; Hewavisenthi, J.; Balawardana, J.; Perera, M. Neoadjuvant Therapy for Rectal Cancer Down-Stages the Tumor but Reduces Lymph Node Harvest Significantly. Surg. Today 2005, 35, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Li Destri, G.; Di Carlo, I.; Scilletta, R.; Scilletta, B.; Puleo, S. Colorectal Cancer and Lymph Nodes: The Obsession With the Number 12. World J. Gastroenterol. 2014, 20, 1951–1960. [Google Scholar] [CrossRef]
- Flynn, S.M.; Burchette, R.J.; Ghassemi, M.; Ratner, O.; Mandel, D.; Tomassi, M.J.; Klaristenfeld, D.D. Carnoy’s Solution Fixation With Compression Significantly Increases the Number of Lymph Nodes Yielded From Colorectal Cancer Specimens. J. Surg. Oncol. 2019, 119, 766–770. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 13 |
|---|---|
| Mean patient age, years | 58.8 ± 17.9 |
| Sex, n (%) | |
| Male | 9 (69.2) |
| Female | 4 (30.8) |
| Pretreatment histology, n (%) | |
| Well-differentiated | 2 (15.4) |
| Moderately differentiated | 8 (61.5) |
| Poorly differentiated | 1 (7.7) |
| Mucinous | 2 (15.4) |
| Clinical tumor stage †, n (%) | |
| cT2 | 3 (23.1) |
| cT3 | 9 (69.2) |
| cT4 | 1 (7.7) |
| Lymph node metastasis, yes, n (%) | 6 (46.2) |
| Neoadjuvant chemoradiotherapy, yes, n (%) | 8 (61.5) |
| Mean radiation dose ‡, Gy | 48.4 ± 2.8 |
| Resection, n (%) | |
| LAR | 8 (61.5) |
| APR | 5 (38.5) |
| WSI | WSI + WBI | p-Value | |
|---|---|---|---|
| Tumor deposit, yes, n (%) | 3 (23.1) | 3 (23.1) | 1.00 |
| Lymphovascular invasion, yes, n (%) | 7 (53.8) | 7 (53.8) | 1.00 |
| Perineural invasion, yes, n (%) | 4 (30.8) | 2 (15.4) | 0.35 |
| Lymph node metastasis, yes, n (%) | 4 (30.8) | 4 (30.8) | 1.00 |
| Total number of BLN † | 80 | 108 | NA |
| Total number of MLN † | 29 | 35 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, M.; Cesmecioglu, E.; Firat, C.; Sakamoto, H.; Teplov, A.; Kawata, N.; Ntiamoah, P.; Ohnishi, T.; Ibrahim, K.; Vakiani, E.; et al. Pathological Evaluation of Rectal Cancer Specimens Using Micro-Computed Tomography. Diagnostics 2022, 12, 984. https://doi.org/10.3390/diagnostics12040984
Yoshida M, Cesmecioglu E, Firat C, Sakamoto H, Teplov A, Kawata N, Ntiamoah P, Ohnishi T, Ibrahim K, Vakiani E, et al. Pathological Evaluation of Rectal Cancer Specimens Using Micro-Computed Tomography. Diagnostics. 2022; 12(4):984. https://doi.org/10.3390/diagnostics12040984
Chicago/Turabian StyleYoshida, Masao, Emine Cesmecioglu, Canan Firat, Hirotsugu Sakamoto, Alexei Teplov, Noboru Kawata, Peter Ntiamoah, Takashi Ohnishi, Kareem Ibrahim, Efsevia Vakiani, and et al. 2022. "Pathological Evaluation of Rectal Cancer Specimens Using Micro-Computed Tomography" Diagnostics 12, no. 4: 984. https://doi.org/10.3390/diagnostics12040984
APA StyleYoshida, M., Cesmecioglu, E., Firat, C., Sakamoto, H., Teplov, A., Kawata, N., Ntiamoah, P., Ohnishi, T., Ibrahim, K., Vakiani, E., Garcia-Aguilar, J., Hameed, M., Shia, J., & Yagi, Y. (2022). Pathological Evaluation of Rectal Cancer Specimens Using Micro-Computed Tomography. Diagnostics, 12(4), 984. https://doi.org/10.3390/diagnostics12040984