
“A Head Start or a Pain in the Neck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
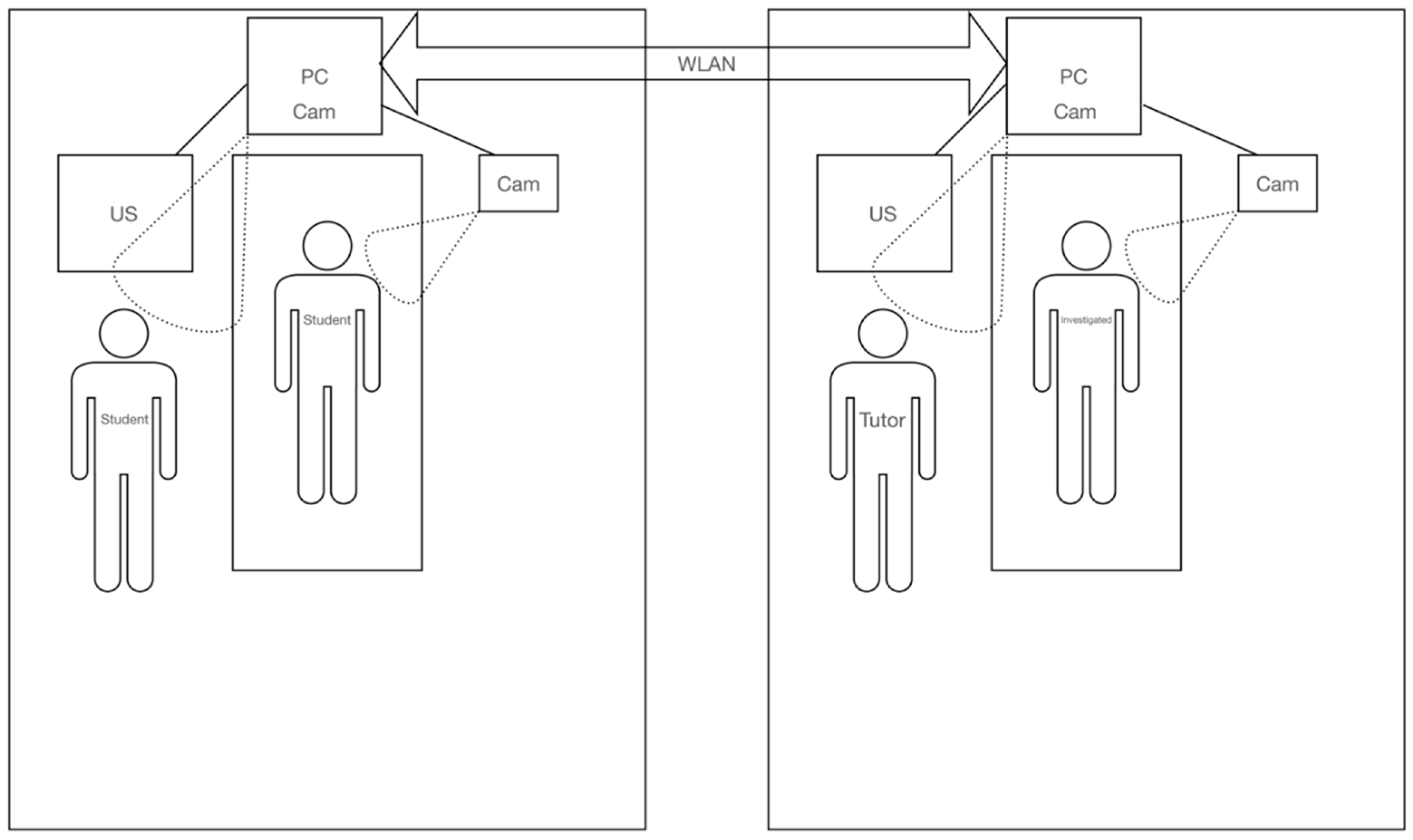
2.2. Technical Setup
2.2.1. In-Person Teaching
2.2.2. Video-Based Teaching
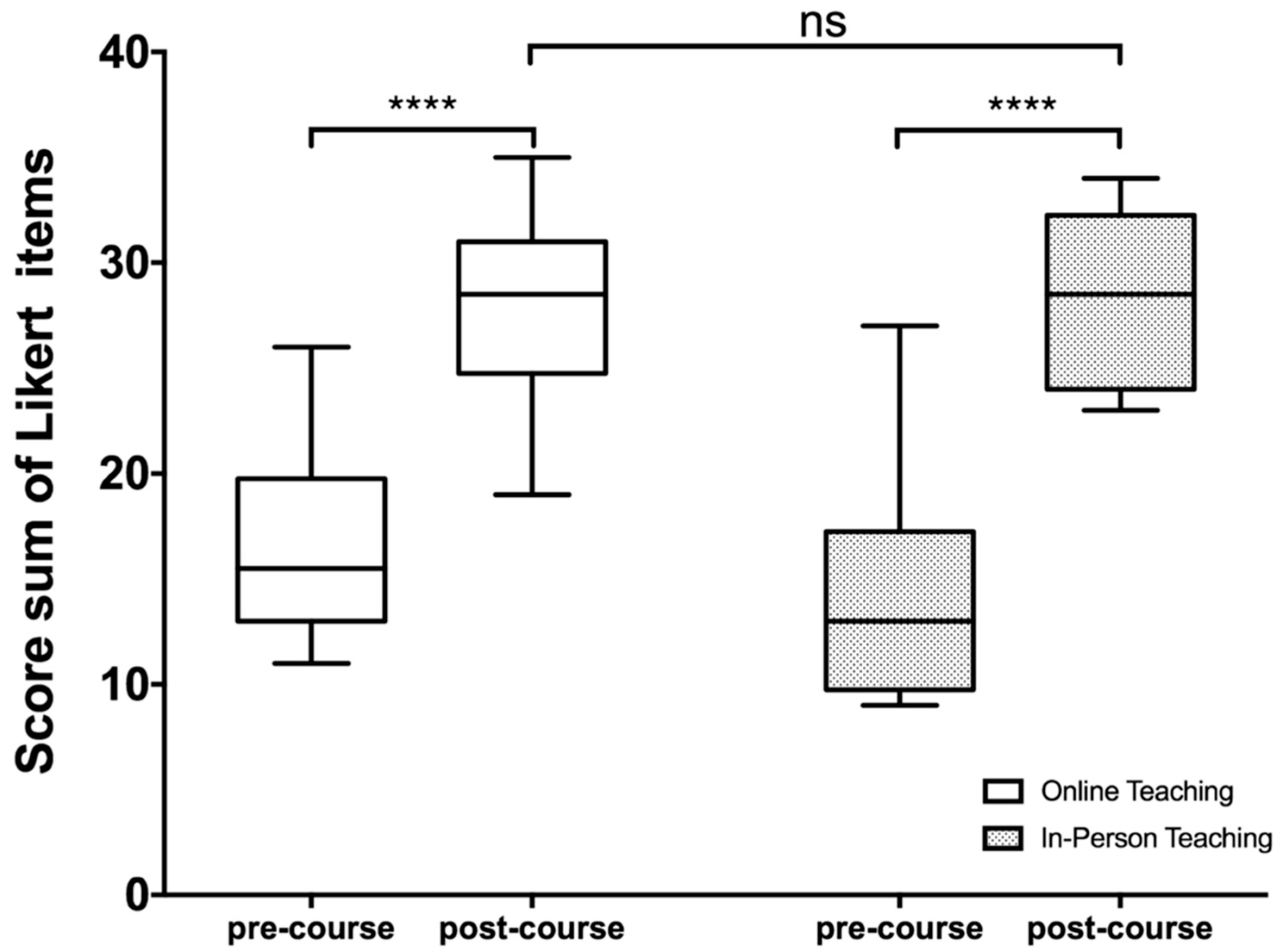
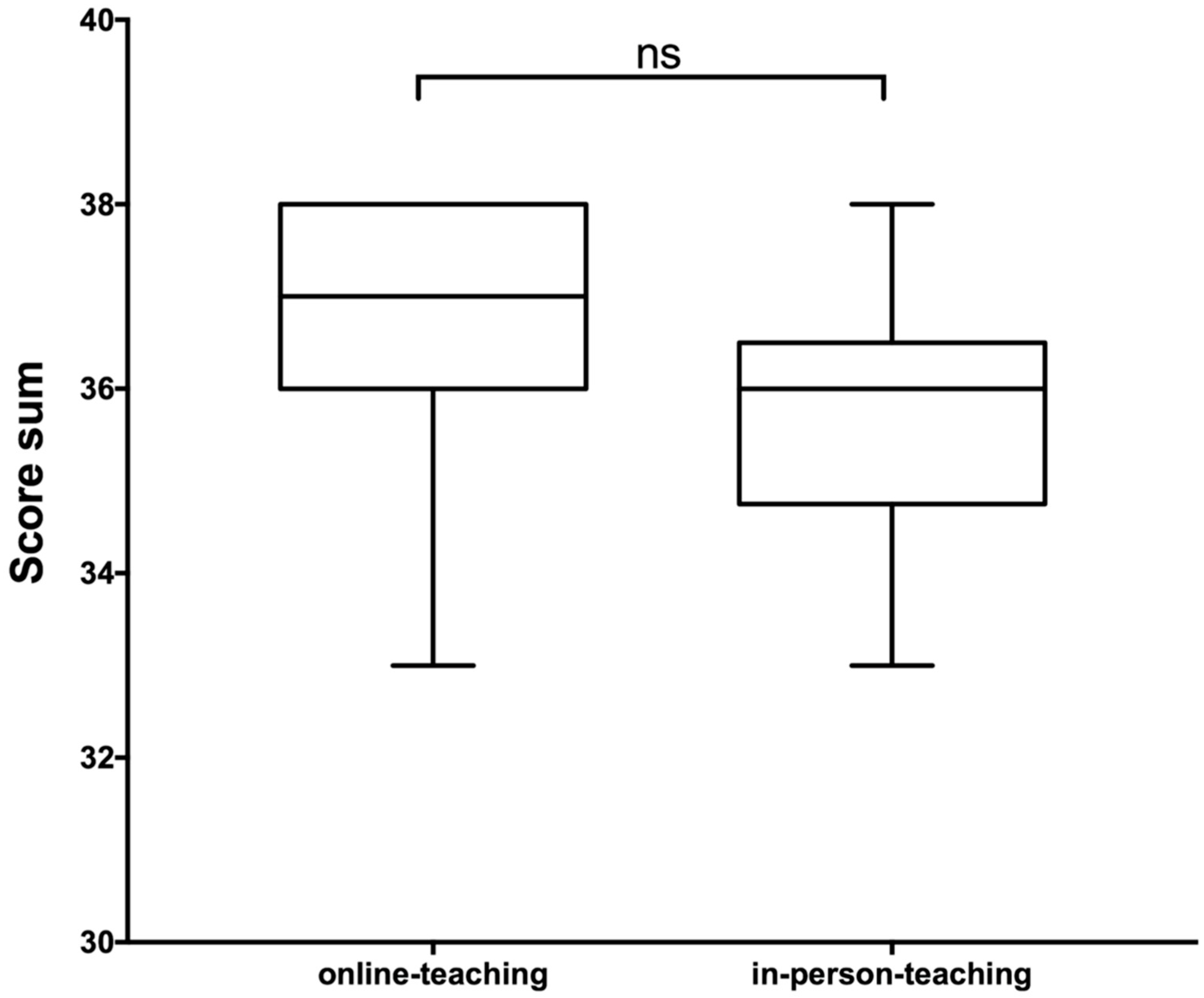
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camargo, C.P.; Tempski, P.Z.; Busnardo, F.F.; de Arruda Martins, M.; Gemperli, R.; Moraes, M.; De Almeida, R.P.; Da Silva, J.E.L.; Madi, M.R.; Carrara, D.; et al. Online learning and COVID-19: A meta-synthesis analysis. Clinics 2020, 75, e2286. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Shelden, D.; Kraftson, A.; Else, T.; Auchus, R.J. A virtual teaching clinic for virtual care during the COVID-19 pandemic. Clin. Diabetes Endocrinol. 2020, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Holtel, M.R. Emerging Technology in Head and Neck Ultrasonography. Otolaryngol. Clin. N. Am. 2010, 43, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Siegel-Richman, Y.; Kendall, J. Establishing an Ultrasound Curriculum in Undergraduate Medical Education: How Much Time Does It Take? J. Ultrasound Med. 2017, 37, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sniezek, J.C. Head and Neck Ultrasound: Why Now? Otolaryngol. Clin. N. Am. 2010, 43, 1143–1147. [Google Scholar] [CrossRef]
- Badran, K.; Jani, P.; Berman, L. Otolaryngologist-performed head and neck ultrasound: Outcomes and challenges in learning the technique. J. Laryngol. Otol. 2014, 128, 447–453. [Google Scholar] [CrossRef]
- Nourkami-Tutdibi, N.; Tutdibi, E.; Schmidt, S.; Zemlin, M.; Abdul-Khaliq, H.; Hofer, M. Long-Term Knowledge Retention after Peer-Assisted Abdominal Ultrasound Teaching: Is PAL a Successful Model for Achieving Knowledge Retention? Ultraschall Med.—Eur. J. Ultrasound 2020, 41, 36–43. [Google Scholar] [CrossRef]
- Nourkami-Tutdibi, N.; Hofer, M.; Zemlin, M.; Abdul-Khaliq, H.; Tutdibi, E. TEACHING MUST GO ON: Flexibility and advantages of peer assisted learning during the COVID-19 pandemic for undergraduate medical ultrasound education—Perspective from the “sonoBYstudents” ultrasound group. GMS J. Med. 2021, 38, 5. [Google Scholar] [CrossRef]
- McRoy, C.; Patel, L.; Gaddam, D.S.; Rothenberg, S.; Herring, A.; Hamm, J.; Chelala, L.; Weinstein, J.; Smith, E.; Awan, O. Radiology Education in the Time of COVID-19: A Novel Distance Learning Workstation Experience for Residents. Acad. Radiol. 2020, 27, 1467–1474. [Google Scholar] [CrossRef]
- Darras, K.E.; Spouge, R.J.; de Bruin, A.B.H.; Sedlic, A.; Hague, C.; Forster, B.B. Undergraduate Radiology Education During the COVID-19 Pandemic: A Review of Teaching and Learning Strategies. Can. Assoc. Radiol. J. 2021, 72, 194–200. [Google Scholar] [CrossRef]
- Biegler, N.; McBeth, P.B.; Tevez-Molina, M.C.; McMillan, J.; Crawford, I.; Hamilton, D.R.; Kirkpatrick, A.W. Just-in-Time Cost-Effective Off-the-Shelf Remote Telementoring of Paramedical Personnel in Bedside Lung Sonography—A Technical Case Study. Telemed. e-Health 2012, 18, 807–809. [Google Scholar] [CrossRef] [PubMed]
- Biegler, N.; McBeth, P.B.; Tiruta, C.; Hamilton, D.R.; Xiao, Z.; Crawford, I.; Tevez-Molina, M.; Miletic, N.; Ball, C.G.; Pian, L.; et al. The feasibility of nurse practitioner-performed, telementored lung telesonography with remote physician guidance—‘A remote virtual mentor’. Crit. Ultrasound J. 2013, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheehan, F.H.; Ricci, M.A.; Murtagh, C.; Clark, H.; Bolson, E.L. Expert visual guidance of ultrasound for telemedicine. J. Telemed. Telecare 2009, 16, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Douglas, T.M.; Levine, A.R.; Olivieri, P.; McCurdy, M.T.; Papali, A.; Zubrow, M.T.; Rodick, K.M.; Hurley, J.M.; Verceles, A.C. Brief training increases nurses’ comfort using tele-ultrasound: A feasibility study. Intensive Crit. Care Nurs. 2019, 51, 45–49. [Google Scholar] [CrossRef]
- Olivieri, P.; Verceles, A.C.; Hurley, J.M.; Zubrow, M.T.; Jeudy, J.; McCurdy, M.T. A Pilot Study of Ultrasonography-Naïve Operators’ Ability to Use Tele-Ultrasonography to Assess the Heart and Lung. J. Intensive Care Med. 2018, 35, 672–678. [Google Scholar] [CrossRef]
- Schroeder, A.N.; Hall, M.M.; Kruse, R.C. Sports Ultrasound Training During a Pandemic: Developing a “Hands-on” Skill Through Distance Learning. Am. J. Phys. Med. Rehabil. 2020, 99, 860–862. [Google Scholar] [CrossRef]
- Todsen, T.; Melchiors, J.; Charabi, B.; Henriksen, B.; Ringsted, C.; Konge, L.; Von Buchwald, C. Competency-based assessment in surgeon-performed head and neck ultrasonography: A validity study. Laryngoscope 2018, 128, 1346–1352. [Google Scholar] [CrossRef]
- Subhi, Y.; Todsen, T.; Konge, L. An integrable, web-based solution for easy assessment of video-recorded performances. Adv. Med. Educ. Pract. 2014, 5, 103–105. [Google Scholar] [CrossRef] [Green Version]
- Ernst, B.P.; Katzer, F.; Künzel, J.; Hodeib, M.; Strieth, S.; Eckrich, J.; Tattermusch, A.; Froelich, M.F.; Matthias, C.; Sommer, W.H.; et al. Impact of structured reporting on developing head and neck ultrasound skills. BMC Med. Educ. 2019, 19, 102. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.-T.; Kang, Y.-N.; Wang, T.-C.; Lin, C.-W.; Cheng, C.-Y.; Suk, F.-M.; Hsu, C.-W.; Huang, S.-K.; Huang, W.-C. Does ultrasound education improve anatomy learning? Effects of the Parallel Ultrasound Hands-on (PUSH) undergraduate medicine course. BMC Med. Educ. 2022, 22, 207. [Google Scholar] [CrossRef]
- Kloth, C.; Schmidt, S.A.; Graeter, T.; Nikolaou, K.; Kaufmann, S.; Beer, M.; Thaiss, W.M. Evaluation of an elective ultrasound course for medical students. Clin. Anat. 2022, 35, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Situ-LaCasse, E.; Acuña, J.; Huynh, D.; Amini, R.; Irving, S.; Samsel, K.; Patanwala, A.E.; Biffar, D.E.; Adhikari, S. Can ultrasound novices develop image acquisition skills after reviewing online ultrasound modules? BMC Med. Educ. 2021, 21, 175. [Google Scholar] [CrossRef] [PubMed]
- Meuwly, J.-Y.; Mandralis, K.; Tenisch, E.; Gullo, G.; Frossard, P.; Morend, L. Use of an Online Ultrasound Simulator to Teach Basic Psychomotor Skills to Medical Students During the Initial COVID-19 Lockdown: Quality Control Study. JMIR Med. Educ. 2021, 7, e31132. [Google Scholar] [CrossRef] [PubMed]
- Kollmann, C.; Santner, L. A prototype of a handheld augmented reality application to get familiar with ultrasound equipment knobology. Med. Ultrason. 2021, 23, 438. [Google Scholar] [CrossRef] [PubMed]
- DePhilip, R.M.; Quinn, M.M. Adaptation of an anatomy graduate course in ultrasound imaging from in-person to live, remote instruction during the COVID-19 pandemic. Anat. Sci. Educ. 2022, 15, 493–507. [Google Scholar] [CrossRef]
- Zavitz, J.; Sarwal, A.; Schoeneck, J.; Glass, C.; Hays, B.; Shen, E.; Bryant, C.; Gupta, K. Virtual multispecialty point-of-care ultrasound rotation for fourth-year medical students during COVID-19: Innovative teaching techniques improve ultrasound knowledge and image interpretation. AEM Educ. Train. 2021, 5, e10632. [Google Scholar] [CrossRef]
- Olivares-Perez, M.E.; Graglia, S.; Harmon, D.J.; Klein, B.A. Virtual anatomy and point-of-care ultrasonography integration pilot for medical students. Anat. Sci. Educ. 2022, 15, 464–475. [Google Scholar] [CrossRef]
- Weiskittel, T.M.; Lachman, N.; Bhagra, A.; Andersen, K.; Jeor, J.S.; Pawlina, W. Team-Based Ultrasound Objective Structured Practice Examination (OSPE) in the Anatomy Course. Anat. Sci. Educ. 2021, 14, 377–384. [Google Scholar] [CrossRef]
- Friedman, L.; Situ-LaCasse, E.; Acuna, J.; Amini, R.; Irving, S.C.; Stolz, L.A.; Sterling, R.; Jung, C.; Sanders, A.B.; Adhikari, S. Point-of-care Head and Neck Sonography for Clinical Problem-solving: Impact of One-day Training Sessions on Medical Student Education. Cureus 2018, 10, e3740. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Self-Assessment Questionnaire | |||||
|---|---|---|---|---|---|
| Age | |||||
| Sex | |||||
| Clinical semester | |||||
| pre-course ultrasound experience | Yes | No | |||
| If YES, pre-course knowledge gained through | Courses | Literature | Internships | ||
| Self-assessment | Locating and visualizing the organ | 1 = is not possible | 2 = is rather possible | 3 = Is possible | 4 = is confidently possible |
| Floor of mouth | |||||
| Larynx | |||||
| Trachea | |||||
| Thyroid gland | |||||
| Esophagus | |||||
| Salivary glands | |||||
| Vessels | |||||
| Lymph nodes | |||||
| Pathologies | |||||
| The time allocated for the course was sufficient | 0 | 1 | 2 | 3 | 4 |
| The teaching materials provided were sufficient | 0 | 1 | 2 | 3 | 4 |
| The comments of the tutors were helpful | 0 | 1 | 2 | 3 | 4 |
| The content of the course was sufficient | 0 | 1 | 2 | 3 | 4 |
| The tasks were clearly formulated | 0 | 1 | 2 | 3 | 4 |
| The teaching materials provided were clearly structured | 0 | 1 | 2 | 3 | 4 |
| The learning content did not overwhelm me | 0 | 1 | 2 | 3 | 4 |
| The group size was comfortable | 0 | 1 | 2 | 3 | 4 |
| The explanations of the tutors were well understandable | 0 | 1 | 2 | 3 | 4 |
| My questions were answered sufficiently | 0 | 1 | 2 | 3 | 4 |
| The feedback on my skills was sufficient | 0 | 1 | 2 | 3 | 4 |
| I consider the course format suitable for knowledge transfer | 0 | 1 | 2 | 3 | 4 |
| It would be useful to extend this course to other organ systems | 0 | 1 | 2 | 3 | 4 |
| Assessment Category | Score Points | |
|---|---|---|
| Manual skills | max. 8 points | |
| Situs orientation | 0–2 | Landmarks and guiding structures are recognized: 0 = no, 1 = partially, 2 = relevant structures can be named |
| Transducer positioning | 0–2 | 0 = no orientation, 1 = partial orientation, 2 = complete orientation |
| Adjusting the focus position | 0–2 | 0 = no focus, 1 = partial focus, 2 = focus is adjusted |
| Adjusting gain | 0–2 | 0 = no gain, 1 = partial gain, 2 = gain is adjusted |
| Interaction with the patient | max. 4 points | Score: 0 = There was no interaction between investigator and patient 1 = The investigator has informed the patient about the planned examination 1 = The investigator has encouraged the patient to cooperate 1 = The investigator explained the results to the patient 1 = The investigator has taken an introductory medical history |
| Patient positioning | 0–2 | 0 = no adjustment of patient position, 1 = partial adjustment of patient position, 2 = patient position is adjusted and properly optimized |
| Systematics of the examination | 0–2 | 0 = no systematics, 1 = partial systematics, 2 = good systematics |
| Visualization of the organs | max. 20 points | |
| Measuring | 0–4 | 0–4 Organs or structures are measured correctly |
| Demonstration | 0–16 | 0–16 Organs are displayed |
| Explanation of the anatomy shown | max. 18 points | |
| Normal findings | 0–14 | 0–16 Organs are examined |
| Pathologies | 0–4 | 0–4 Pathologies are assessed; if no pathology, then 4 points |
| Score total points | max. 50 points |
| Online Course | In-Person Course | |
|---|---|---|
| Age | 23 (21–29) | 22.5 (22–30) |
| Gender (female/male) | 6:6 | 7:3 |
| Semester | 8 (6–10) | 6 (6–8) |
| Ultrasound-knowledge/experience pre-course (courses, internships, literature) | 66.6% | 40% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillong, L.; Bozzato, A.; Hecker, D.; Bozzato, V.; Schick, B.; Kulas, P. “A Head Start or a Pain in the Neck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course. Diagnostics 2022, 12, 1239. https://doi.org/10.3390/diagnostics12051239
Pillong L, Bozzato A, Hecker D, Bozzato V, Schick B, Kulas P. “A Head Start or a Pain in the Neck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course. Diagnostics. 2022; 12(5):1239. https://doi.org/10.3390/diagnostics12051239
Chicago/Turabian StylePillong, Lukas, Alessandro Bozzato, Dietmar Hecker, Victoria Bozzato, Bernhard Schick, and Philipp Kulas. 2022. "“A Head Start or a Pain in the Neck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course" Diagnostics 12, no. 5: 1239. https://doi.org/10.3390/diagnostics12051239
APA StylePillong, L., Bozzato, A., Hecker, D., Bozzato, V., Schick, B., & Kulas, P. (2022). “A Head Start or a Pain in the Neck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course. Diagnostics, 12(5), 1239. https://doi.org/10.3390/diagnostics12051239