
Prognostic Value of Pathologically Positive Nodal Number in p16-Negative Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma with pN3b Status

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables and Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
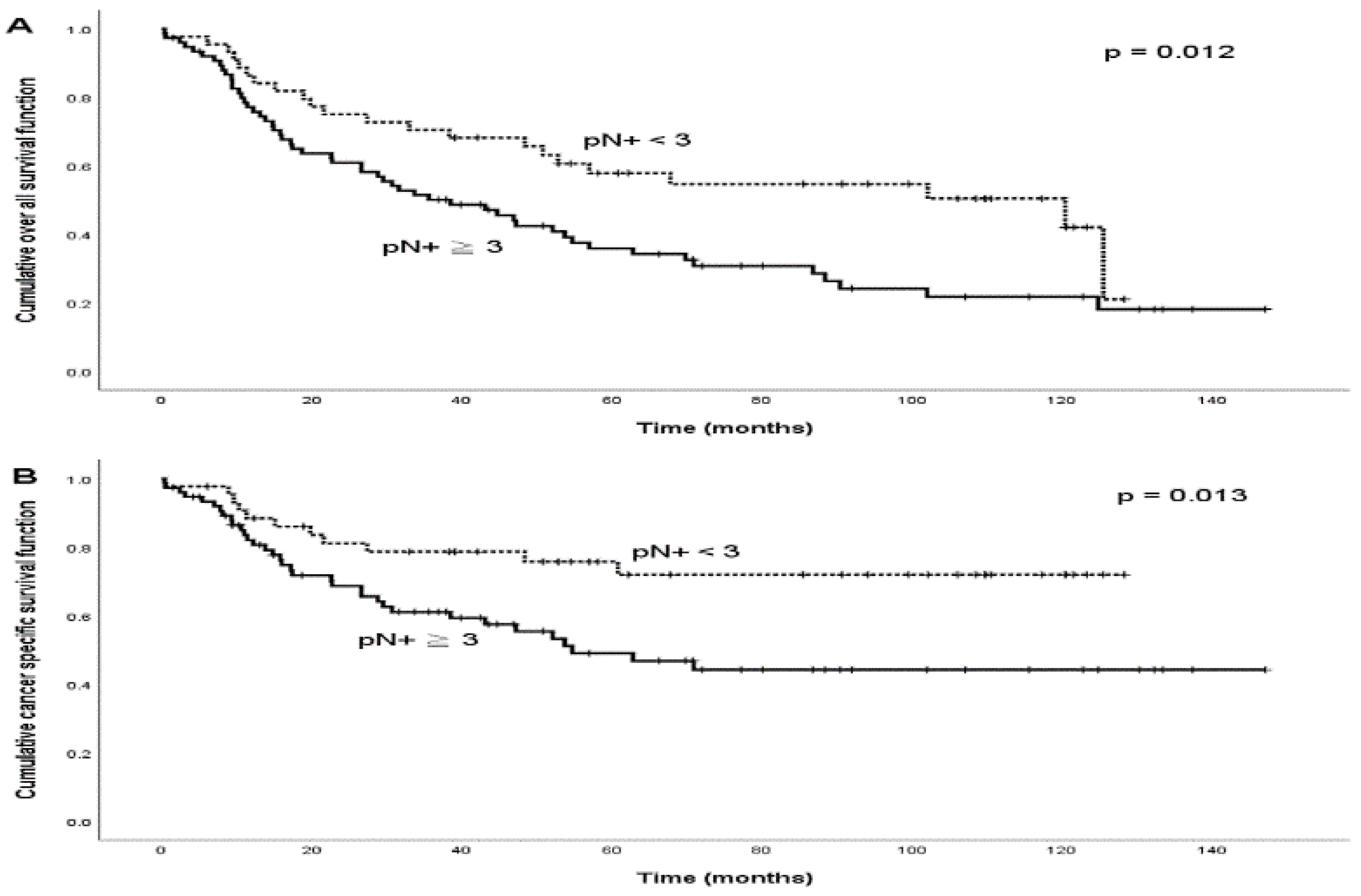
3.2. Number of pN+ and Survival Outcome
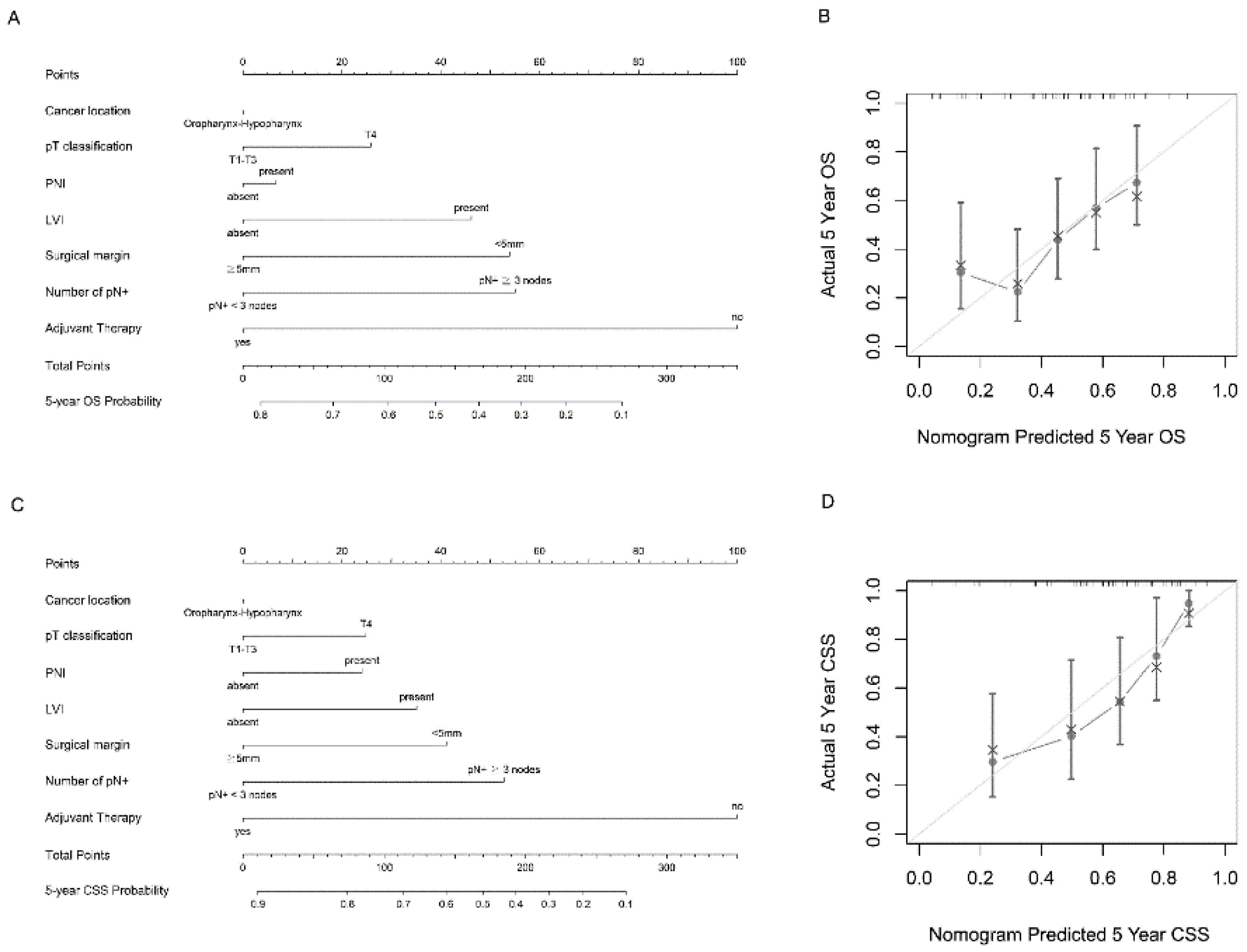
3.3. Predictive Nomograms of Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liao, C.T.; Hsueh, C.; Lee, L.Y.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Huang, S.F.; Chen, I.H.; Kang, C.J.; Ng, S.H.; et al. Neck dissection field and lymph node density predict prognosis in patients with oral cavity cancer and pathological node metastases treated with adjuvant therapy. Oral Oncol. 2012, 48, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.N.; Greenberg, J.S.; Mo, V.; Roberts, D. Extracapsular spread. A significant predictor of treatment failure in patients with squamous cell carcinoma of the tongue. Cancer 2001, 92, 3030–3036. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.J.; Colevas, A.D.; Hara, W.; Holsinger, F.C.; Oakley-Girvan, I.; Divi, V. Number of positive nodes is superior to the lymph node ratio and American Joint Committee on Cancer N staging for the prognosis of surgically treated head and neck squamous cell carcinomas. Cancer 2016, 122, 1388–1397. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.H.; Hu, Q.Y.; Piao, Y.F.; Tang, Q.; Fu, Z.F. Effect of number and ratio of positive lymph nodes in hypopharyngeal cancer. Head Neck 2015, 37, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Hu, Q.; Tang, Q.; Piao, Y.; Fu, Z. Prognostic significance of the number of positive lymph nodes, number of involved regions and metastatic lymph node ratio in hypopharyngeal cancer. Zhonghua Zhong Liu Za Zhi 2014, 36, 783–787. [Google Scholar] [PubMed]
- Subramaniam, N.; Balasubramanian, D.; Kumar, N.; Murthy, S.; Vijayan, S.N.; Nambiar, A.; Vidhyadharan, S.; Thankappan, K.; Iyer, S. Lymph node staging systems in oral squamous cell carcinoma: A comparative analysis. Oral Oncol. 2019, 97, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Puri, S.K.; Fan, C.Y.; Hanna, E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr. Opin. Otolaryngol. Head Neck Surg. 2003, 11, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Joo, Y.H.; Yoo Ie, R.; Cho, K.J.; Park, J.O.; Nam, I.C.; Kim, M.S. Extracapsular spread in hypopharyngeal squamous cell carcinoma: Diagnostic value of FDG PET/CT. Head Neck 2013, 35, 1771–1776. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.S.; Kim, S.; Tighiouart, M.; Gudino, C.; Mita, A.; Scher, K.S.; Laury, A.; Prasad, R.; Shiao, S.L.; Van Eyk, J.E.; et al. Metastatic Lymph Node Burden and Survival in Oral Cavity Cancer. J. Clin. Oncol. 2017, 35, 3601–3609. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Lee, L.Y.; Hsueh, C.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Hsieh, C.H.; Ng, S.H.; Lin, C.H.; Tsao, C.K.; et al. Pathological risk factors stratification in pN3b oral cavity squamous cell carcinoma: Focus on the number of positive nodes and extranodal extension. Oral Oncol. 2018, 86, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.S.; Kim, S.; Tighiouart, M.; Gudino, C.; Mita, A.; Scher, K.S.; Laury, A.; Prasad, R.; Shiao, S.L.; Ali, N.; et al. Association of Quantitative Metastatic Lymph Node Burden With Survival in Hypopharyngeal and Laryngeal Cancer. JAMA Oncol. 2018, 4, 985–989. [Google Scholar] [CrossRef] [PubMed]
- Devaraja, K.; Pujary, K.; Ramaswamy, B.; Nayak, D.R.; Kumar, N.; Nayak, D. Lymph node yield in treatment naive cases of head and neck squamous cell carcinoma: En bloc lymphadenectomy versus level-by-level dissection. J. Laryngol. Otol. 2021, 135, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Clark, J.R.; Amit, M.; Yen, T.C.; Liao, C.T.; Kowalski, L.P.; Kreppel, M.; Cernea, C.R.; Bachar, G.; Villaret, A.B.; et al. Minimum nodal yield in oral squamous cell carcinoma: Defining the standard of care in a multicenter international pooled validation study. Ann. Surg. Oncol. 2014, 21, 3049–3055. [Google Scholar] [CrossRef] [PubMed]
- Pou, J.D.; Barton, B.M.; Lawlor, C.M.; Frederick, C.H.; Moore, B.A.; Hasney, C.P. Minimum lymph node yield in elective level I-III neck dissection. Laryngoscope 2017, 127, 2070–2073. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Zhang, W.J.; Gao, K.; Clark, J.R. Nodal yield and survival in oral squamous cancer: Defining the standard of care. Cancer 2011, 117, 2917–2925. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; van Glabbeke, M.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.K.; et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005, 27, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Eldeeb, H.; Macmillan, C.; Elwell, C.; Hammod, A. The effect of the surgical margins on the outcome of patients with head and neck squamous cell carcinoma: Single institution experience. Cancer Biol. Med. 2012, 9, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.H.; Chuang, H.C.; Lin, Y.T.; Huang, T.L.; Fang, F.M.; Lu, H.; Chien, C.Y. Survival Outcomes and Predictors for Patients who Failed Chemoradiotherapy/Radiotherapy and Underwent Salvage Total Laryngectomy. Int. J. Environ. Res. Public Health 2021, 18, 371. [Google Scholar] [CrossRef] [PubMed]
- Bobdey, S.; Mair, M.; Nair, S.; Nair, D.; Balasubramaniam, G.; Chaturvedi, P. A Nomogram based prognostic score that is superior to conventional TNM staging in predicting outcome of surgically treated T4 buccal mucosa cancer: Time to think beyond TNM. Oral Oncol. 2018, 81, 10–15. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | % |
|---|---|---|
| Age, median range (years) | 53 (35–78) | |
| Sex (male/female) | 116/4 | 96.7/3.3 |
| Smoking habit (yes) | 113 | 94.2 |
| Betel nut chewing habit (yes) | 103 | 85.8 |
| Alcohol drinking habit (yes) | 110 | 91.7 |
| Cancer location (oropharynx/hypopharynx) | 56/64 | 46.7/53.3 |
| pT classification (T1–2/T3–4) | 52/68 | 43.3/56.7 |
| Histologic grade (WDSCC/MDSCC/PDSCC) | 24/89/7 | 20.0/74.2/5.8 |
| Perineural invasion (yes) | 62 | 51.7 |
| Lymphovascular invasion (yes) | 73 | 60.8 |
| Lymph node yields ≥ 18 | 105 | 87.5 |
| Maximal size of pN+ (≤3 cm/3–6 cm/>6 cm) | 70/47/3 | 58.3/39.2/2.5 |
| Margin (≥5 mm/<5 mm) | 75/45 | 62.5/37.5 |
| Neck dissection (ipsilateral/bilateral) | 67/53 | 55.8/44.2 |
| Bilateral nodal disease (yes) | 37 | 30.8 |
| Adjuvant therapy (CCRT/RT alone/none) | 98/10/12 | 81.7/8.3/10.0 |
| Variable | pN+ < 3 | pN+ ≥ 33 | p Value |
|---|---|---|---|
| Sex (male/female) | 42/2 | 74/2 | 0.623 |
| Age (<53 years/≥53 years) | 22/22 | 37/39 | 0.889 |
| Cancer location (oropharynx/hypopharynx) | 23/21 | 33/43 | 0.349 |
| pT classification (T1–2/T3–4) | 27/17 | 25/51 | 0.002 |
| Histologic grade (WDSCC/MDSCC/PDSCC) | 10/31/3 | 14/58/4 | 0.742 |
| Perineural invasion (no/yes) | 26/18 | 32/44 | 0.117 |
| Lymphovascular invasion (no/yes) | 24/20 | 23/53 | 0.012 |
| Margin (≥5 mm/<5 mm) | 15/29 | 30/46 | 0.557 |
| Bilateral nodal disease (no/yes) | 38/6 | 45/31 | 0.002 |
| Lymph node yields (<18/≥18) | 7/37 | 8/68 | 0.39 |
| Maximal size of pN+ (≤3 cm/3–6 cm/>6 cm) | 20/23/1 | 50/24/2 | 0.061 |
| Adjuvant therapy (no/yes) | 5/39 | 7/69 | 0.757 |
| Variable | 5-Year OS (%) | p-Value | 5-Year CSS (%) | p-Value |
|---|---|---|---|---|
| Sex (male/female) | 43.8/50.0 | 0.560 | 59.6/50.0 | 0.721 |
| Age (<53 years/≥53 years) | 46.5/41.5 | 0.853 | 55.6/62.3 | 0.468 |
| Cancer location (oropharynx/hypopharynx) | 37.5/49.7 | 0.492 | 51.9/65.6 | 0.144 |
| pT classification (T1–2/T3–4) | 53.2/37.3 | 0.046 | 71.6/50.1 | 0.041 |
| Histologic grade (WDSCC/MDSCC/PDSCC) | 40.9/43.3/71.4 | 0.944 | 57.2/59.1/71.4 | 0.950 |
| Perineural invasion (no/yes) | 48.2/38.3 | 0.399 | 65.8/51.2 | 0.121 |
| Lymphovascular invasion (no/yes) | 51.3/38.4 | 0.093 | 67.6/52.7 | 0.199 |
| Margin (≥5 mm/<5 mm) | 48.0/41.8 | 0.035 | 63.5/56.8 | 0.09 |
| Bilateral nodal disease (no/yes) | 47.0/37.7 | 0.118 | 61.5/55.2 | 0.298 |
| Lymph node yields (<18/≥18) | 33.3/45.8 | 0.223 | 54.5/60.2 | 0.933 |
| Maximal size of pN+ (≤3 cm/3–6 cm/>6 cm) | 39.1/50.7/66.7 | 0.220 | 54.8/65.1/66.7 | 0.447 |
| Number of pN+ (<3/≥3) | 57.9/35.9 | 0.012 | 75.7/49.0 | 0.013 |
| Adjuvant therapy (no/yes) | 41.7/44.2 | 0.031 | 50.0/60.3 | 0.047 |
| 5-Year OS | 5-Year CSS | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Variable | ||||
| pT classification: T3–4 (ref: T1–2) | 1.4 (0.9–2.4) | 0.152 | N/A | N/A |
| Surgical margin: <5 mm (ref: ≥5 mm) | 1.8(1.1–3.0) | 0.017 | N/A | N/A |
| pN+: ≥3 (ref: <3) | 1.9 (1.1–3.2) | 0.021 | 2.3 (1.2–4.6) | 0.015 |
| Adjuvant therapy: yes (ref: no) | 0.6 (0.3–1.1) | 0.088 | 0.4 (0.2–0.9) | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-H.; Lin, Y.-T.; Chuang, H.-C.; Huang, T.-L.; Lu, H.; Chien, C.-Y.; Fang, F.-M. Prognostic Value of Pathologically Positive Nodal Number in p16-Negative Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma with pN3b Status. Diagnostics 2022, 12, 1443. https://doi.org/10.3390/diagnostics12061443
Tsai M-H, Lin Y-T, Chuang H-C, Huang T-L, Lu H, Chien C-Y, Fang F-M. Prognostic Value of Pathologically Positive Nodal Number in p16-Negative Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma with pN3b Status. Diagnostics. 2022; 12(6):1443. https://doi.org/10.3390/diagnostics12061443
Chicago/Turabian StyleTsai, Ming-Hsien, Yu-Tsai Lin, Hui-Ching Chuang, Tai-Ling Huang, Hui Lu, Chih-Yen Chien, and Fu-Min Fang. 2022. "Prognostic Value of Pathologically Positive Nodal Number in p16-Negative Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma with pN3b Status" Diagnostics 12, no. 6: 1443. https://doi.org/10.3390/diagnostics12061443
APA StyleTsai, M. -H., Lin, Y. -T., Chuang, H. -C., Huang, T. -L., Lu, H., Chien, C. -Y., & Fang, F. -M. (2022). Prognostic Value of Pathologically Positive Nodal Number in p16-Negative Oropharyngeal and Hypopharyngeal Squamous Cell Carcinoma with pN3b Status. Diagnostics, 12(6), 1443. https://doi.org/10.3390/diagnostics12061443