
Performance of a Deep Learning System for Automatic Diagnosis of Protruding Lesions in Colon Capsule Endoscopy

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
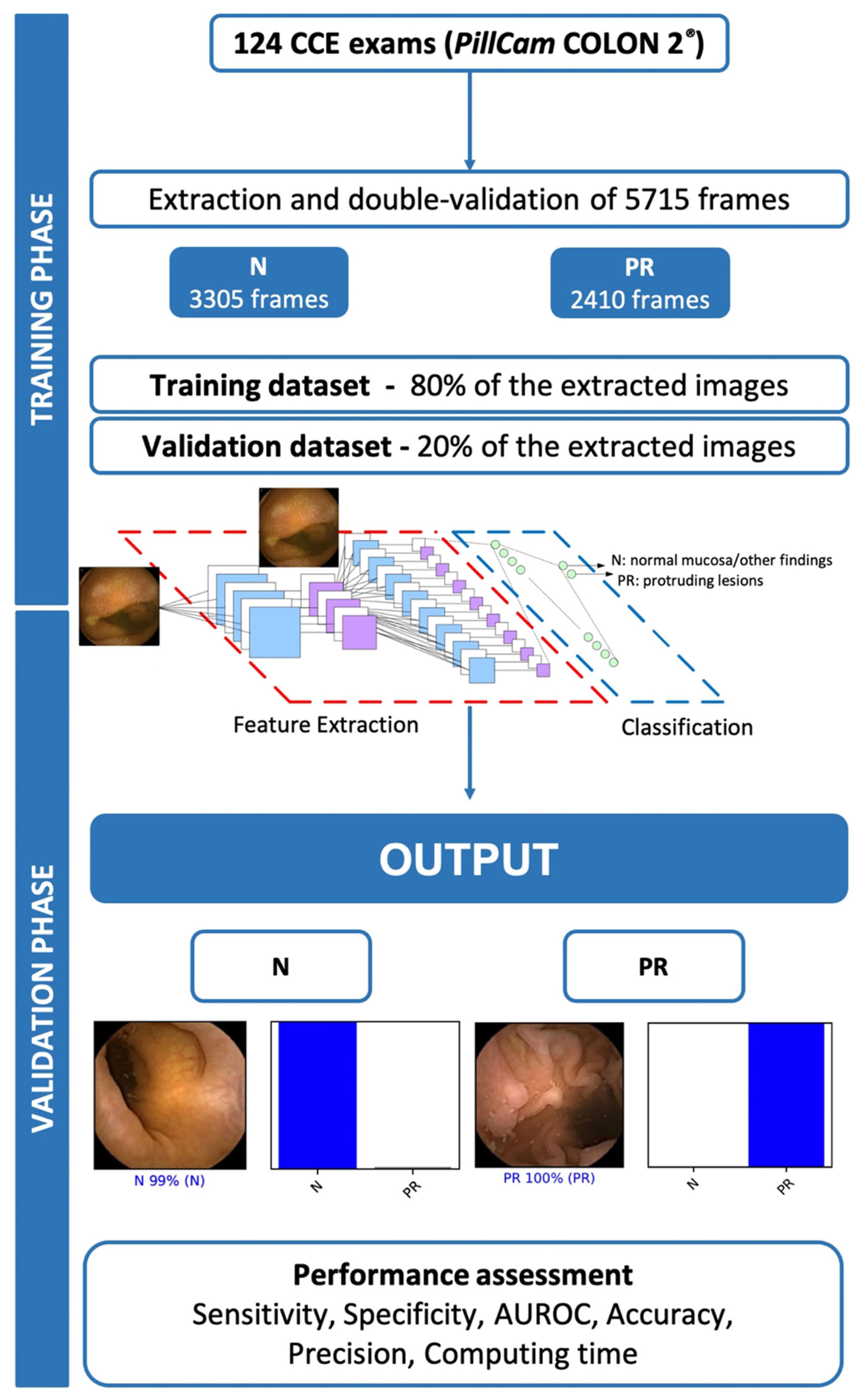
2.1. Study Design
2.1.1. Colon Capsule Endoscopy Procedure
2.1.2. Development of the Convolutional Neural Network
2.1.3. Model Performance and Statistical Analysis
3. Results
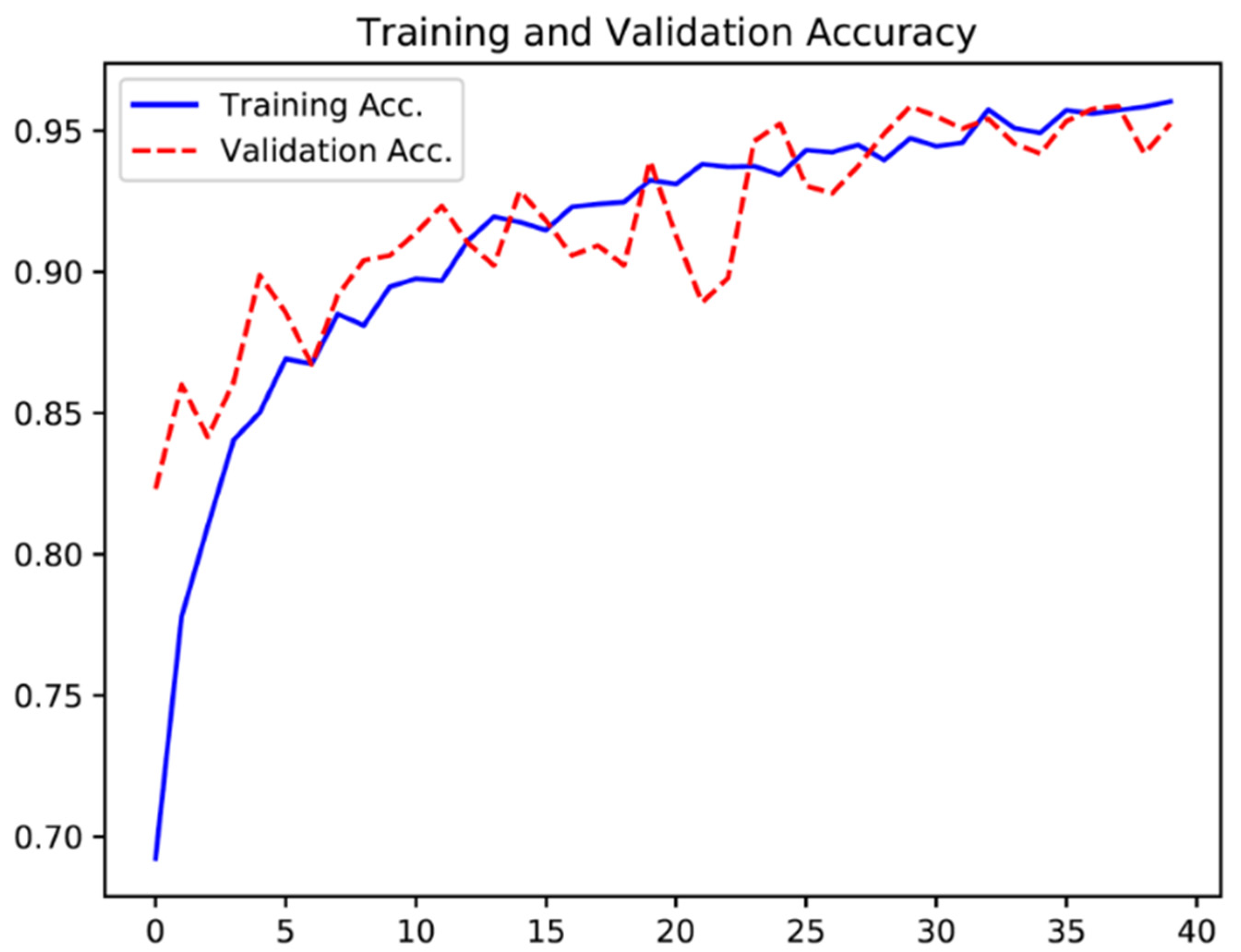
3.1. Construction of the Network
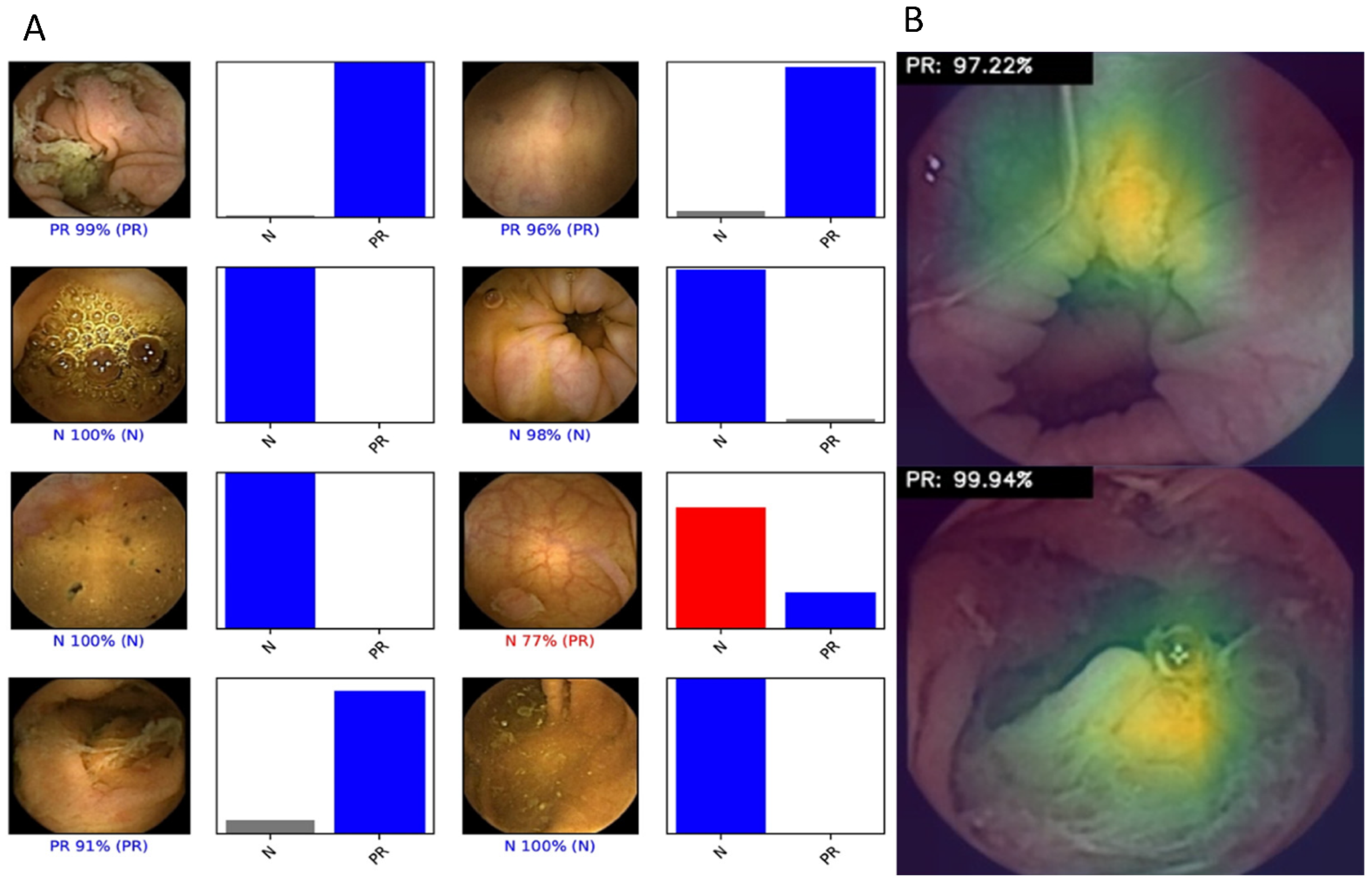
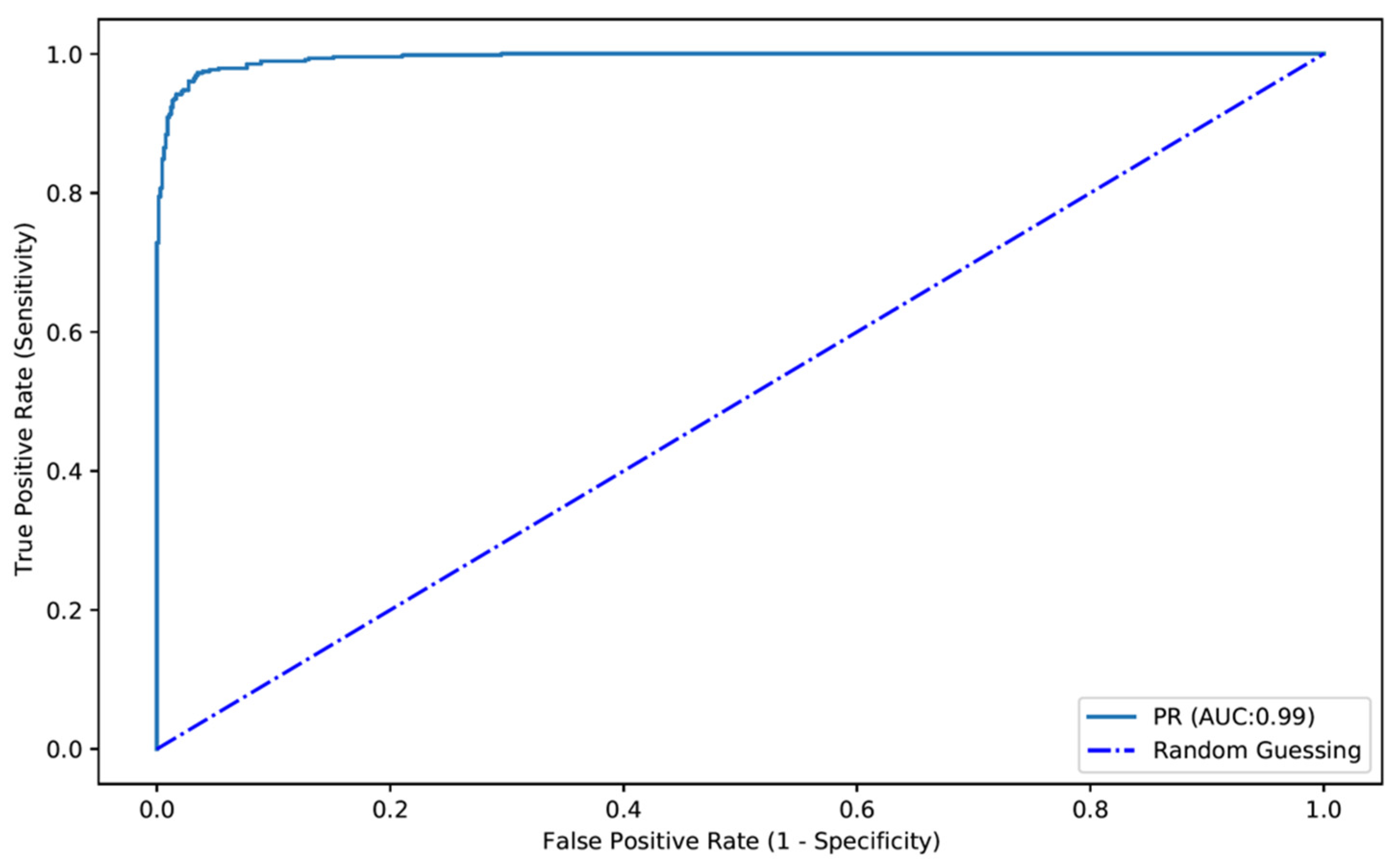
3.2. Overall Performance of the Network
3.3. Computational Performance of the CNN
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Eliakim, R.; Fireman, Z.; Gralnek, I.M.; Yassin, K.; Waterman, M.; Kopelman, Y.; Lachter, J.; Koslowsky, B.; Adler, S.N. Evaluation of the PillCam Colon capsule in the detection of colonic pathology: Results of the first multicenter, prospective, comparative study. Endoscopy 2006, 38, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, R.; Yassin, K.; Niv, Y.; Metzger, Y.; Lachter, J.; Gal, E.; Sapoznikov, B.; Konikoff, F.; Leichtmann, G.; Fireman, Z.; et al. Prospective multicenter performance evaluation of the second-generation colon capsule compared with colonoscopy. Endoscopy 2009, 41, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Niikura, R.; Yasunaga, H.; Yamada, A.; Matsui, H.; Fushimi, K.; Hirata, Y.; Koike, K. Factors predicting adverse events associated with therapeutic colonoscopy for colorectal neoplasia: A retrospective nationwide study in Japan. Gastrointest. Endosc. 2016, 84, 971–982.e976. [Google Scholar] [CrossRef] [PubMed]
- Spada, C.; Hassan, C.; Bellini, D.; Burling, D.; Cappello, G.; Carretero, C.; Dekker, E.; Eliakim, R.; de Haan, M.; Kaminski, M.F.; et al. Imaging alternatives to colonoscopy: CT colonography and colon capsule. European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastrointestinal and Abdominal Radiology (ESGAR) Guideline—Update 2020. Endoscopy 2020, 52, 1127–1141. [Google Scholar] [CrossRef]
- Milluzzo, S.M.; Bizzotto, A.; Cesaro, P.; Spada, C. Colon capsule endoscopy and its effectiveness in the diagnosis and management of colorectal neoplastic lesions. Exp. Rev. Anticancer Ther. 2019, 19, 71–80. [Google Scholar] [CrossRef]
- Vuik, F.E.R.; Nieuwenburg, S.A.V.; Moen, S.; Spada, C.; Senore, C.; Hassan, C.; Pennazio, M.; Rondonotti, E.; Pecere, S.; Kuipers, E.J.; et al. Colon capsule endoscopy in colorectal cancer screening: A systematic review. Endoscopy 2021, 53, 815–824. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Abe, O.; Kiryu, S. Deep Learning with Convolutional Neural Network for Differentiation of Liver Masses at Dynamic Contrast-enhanced CT: A Preliminary Study. Radiology 2018, 286, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Gargeya, R.; Leng, T. Automated Identification of Diabetic Retinopathy Using Deep Learning. Ophthalmology 2017, 124, 962–969. [Google Scholar] [CrossRef]
- Aoki, T.; Yamada, A.; Aoyama, K.; Saito, H.; Tsuboi, A.; Nakada, A.; Niikura, R.; Fujishiro, M.; Oka, S.; Ishihara, S.; et al. Automatic detection of erosions and ulcerations in wireless capsule endoscopy images based on a deep convolutional neural network. Gastrointest. Endosc. 2019, 89, 357–363.e352. [Google Scholar] [CrossRef]
- Aoki, T.; Yamada, A.; Kato, Y.; Saito, H.; Tsuboi, A.; Nakada, A.; Niikura, R.; Fujishiro, M.; Oka, S.; Ishihara, S.; et al. Automatic detection of blood content in capsule endoscopy images based on a deep convolutional neural network. J. Gastroenterol. Hepatol. 2020, 35, 1196–1200. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Shi, H.; Zhang, H.; Meng, L.; Fan, M.; Han, C.; Zhang, K.; Ming, F.; Xie, X.; Liu, H.; et al. Gastroenterologist-Level Identification of Small-Bowel Diseases and Normal Variants by Capsule Endoscopy Using a Deep-Learning Model. Gastroenterology 2019, 157, 1044–1054.e1045. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, A.; Oka, S.; Aoyama, K.; Saito, H.; Aoki, T.; Yamada, A.; Matsuda, T.; Fujishiro, M.; Ishihara, S.; Nakahori, M.; et al. Artificial intelligence using a convolutional neural network for automatic detection of small-bowel angioectasia in capsule endoscopy images. Dig. Endosc. 2020, 32, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Badalamenti, M.; Maselli, R.; Correale, L.; Radaelli, F.; Rondonotti, E.; Ferrara, E.; Spadaccini, M.; Alkandari, A.; Fugazza, A.; et al. Efficacy of Real-Time Computer-Aided Detection of Colorectal Neoplasia in a Randomized Trial. Gastroenterology 2020, 159, 512–520.e517. [Google Scholar] [CrossRef]
- Spada, C.; Hassan, C.; Galmiche, J.P.; Neuhaus, H.; Dumonceau, J.M.; Adler, S.; Epstein, O.; Gay, G.; Pennazio, M.; Rex, D.K.; et al. Colon capsule endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2012, 44, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Bisschops, R.; East, J.E.; Hassan, C.; Hazewinkel, Y.; Kamiński, M.F.; Neumann, H.; Pellisé, M.; Antonelli, G.; Bustamante Balen, M.; Coron, E.; et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 1155–1179. [Google Scholar] [CrossRef] [Green Version]
- Hassan, C.; Spadaccini, M.; Iannone, A.; Maselli, R.; Jovani, M.; Chandrasekar, V.T.; Antonelli, G.; Yu, H.; Areia, M.; Dinis-Ribeiro, M.; et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: A systematic review and meta-analysis. Gastrointest. Endosc. 2021, 93, 77–85.e76. [Google Scholar] [CrossRef]
- Bjørsum-Meyer, T.; Koulaouzidis, A.; Baatrup, G. Comment on “Artificial intelligence in gastroenterology: A state-of-the-art review”. World J. Gastroenterol. 2022, 28, 1722–1724. [Google Scholar] [CrossRef]
- Nakazawa, K.; Nouda, S.; Kakimoto, K.; Kinoshita, N.; Tanaka, Y.; Tawa, H.; Koshiba, R.; Naka, Y.; Hirata, Y.; Ota, K.; et al. The Differential Diagnosis of Colorectal Polyps Using Colon Capsule Endoscopy. Intern. Med. 2021, 60, 1805–1812. [Google Scholar] [CrossRef]
- Yamada, K.; Nakamura, M.; Yamamura, T.; Maeda, K.; Sawada, T.; Mizutani, Y.; Ishikawa, E.; Ishikawa, T.; Kakushima, N.; Furukawa, K.; et al. Diagnostic yield of colon capsule endoscopy for Crohn’s disease lesions in the whole gastrointestinal tract. BMC Gastroenterol. 2021, 21, 75. [Google Scholar] [CrossRef]
- Spada, C.; Barbaro, F.; Andrisani, G.; Minelli Grazioli, L.; Hassan, C.; Costamagna, I.; Campanale, M.; Costamagna, G. Colon capsule endoscopy: What we know and what we would like to know. World J. Gastroenterol. 2014, 20, 16948–16955. [Google Scholar] [CrossRef] [PubMed]
- Cash, B.D.; Fleisher, M.R.; Fern, S.; Rajan, E.; Haithcock, R.; Kastenberg, D.M.; Pound, D.; Papageorgiou, N.P.; Fernández-Urién, I.; Schmelkin, I.J.; et al. Multicentre, prospective, randomised study comparing the diagnostic yield of colon capsule endoscopy versus CT colonography in a screening population (the TOPAZ study). Gut 2020, 70, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Holleran, G.; Leen, R.; O’Morain, C.; McNamara, D. Colon capsule endoscopy as possible filter test for colonoscopy selection in a screening population with positive fecal immunology. Endoscopy 2014, 46, 473–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groth, S.; Krause, H.; Behrendt, R.; Hill, H.; Börner, M.; Bastürk, M.; Plathner, N.; Schütte, F.; Gauger, U.; Riemann, J.F.; et al. Capsule colonoscopy increases uptake of colorectal cancer screening. BMC Gastroenterol. 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Bjoersum-Meyer, T.; Spada, C.; Watson, A.; Eliakim, R.; Baatrup, G.; Toth, E.; Koulaouzidis, A. What holds back colon capsule endoscopy from being the main diagnostic test for the large bowel in cancer screening? Gastrointest. Endosc. 2021, 95, 168–170. [Google Scholar] [CrossRef]
- Hassan, C.; Zullo, A.; Winn, S.; Morini, S. Cost-effectiveness of capsule endoscopy in screening for colorectal cancer. Endoscopy 2008, 40, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Yamada, A.; Niikura, R.; Otani, K.; Aoki, T.; Koike, K. Automatic detection of colorectal neoplasia in wireless colon capsule endoscopic images using a deep convolutional neural network. Endoscopy 2020, 53, 832–836. [Google Scholar] [CrossRef]
- Saito, H.; Aoki, T.; Aoyama, K.; Kato, Y.; Tsuboi, A.; Yamada, A.; Fujishiro, M.; Oka, S.; Ishihara, S.; Matsuda, T.; et al. Automatic detection and classification of protruding lesions in wireless capsule endoscopy images based on a deep convolutional neural network. Gastrointest. Endosc. 2020, 92, 144–151.e141. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Expert Classification | |||
|---|---|---|---|
| Protruding Lesion | Normal Mucosa | ||
| CNN classification | Protruding lesion | 434 | 6 |
| Normal mucosa | 48 | 655 | |
| Sensitivity | 90.0% | ||
| Specificity | 99.1% | ||
| PPV | 98.6% | ||
| NPV | 93.2% | ||
| Accuracy | 95.3% | ||
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | AUC | |
|---|---|---|---|---|---|---|
| Fold 1 | 82.8 | 97.5 | 62.6 | 99.1 | 96.9 | 0.980 |
| Fold 2 | 87.4 | 95.9 | 57.1 | 99.2 | 95.4 | 0.970 |
| Fold 3 | 92.1 | 94.7 | 48.4 | 99.6 | 94.6 | 0.980 |
| Overall, mean (±SD) | 87.4 ± 4.6 | 96.1 ± 1.4 | 56.0 ± 7.1 | 99.3 ± 0.2 | 95.6 ± 1.1 | 0.976 ± 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mascarenhas, M.; Afonso, J.; Ribeiro, T.; Cardoso, H.; Andrade, P.; Ferreira, J.P.S.; Saraiva, M.M.; Macedo, G. Performance of a Deep Learning System for Automatic Diagnosis of Protruding Lesions in Colon Capsule Endoscopy. Diagnostics 2022, 12, 1445. https://doi.org/10.3390/diagnostics12061445
Mascarenhas M, Afonso J, Ribeiro T, Cardoso H, Andrade P, Ferreira JPS, Saraiva MM, Macedo G. Performance of a Deep Learning System for Automatic Diagnosis of Protruding Lesions in Colon Capsule Endoscopy. Diagnostics. 2022; 12(6):1445. https://doi.org/10.3390/diagnostics12061445
Chicago/Turabian StyleMascarenhas, Miguel, João Afonso, Tiago Ribeiro, Hélder Cardoso, Patrícia Andrade, João P. S. Ferreira, Miguel Mascarenhas Saraiva, and Guilherme Macedo. 2022. "Performance of a Deep Learning System for Automatic Diagnosis of Protruding Lesions in Colon Capsule Endoscopy" Diagnostics 12, no. 6: 1445. https://doi.org/10.3390/diagnostics12061445
APA StyleMascarenhas, M., Afonso, J., Ribeiro, T., Cardoso, H., Andrade, P., Ferreira, J. P. S., Saraiva, M. M., & Macedo, G. (2022). Performance of a Deep Learning System for Automatic Diagnosis of Protruding Lesions in Colon Capsule Endoscopy. Diagnostics, 12(6), 1445. https://doi.org/10.3390/diagnostics12061445