
Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome

 , , , , , ,
, , , , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
2.3. Ethics
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sari, D.M.; Wijaya, L.C.G. Cardiac rehabilitation via telerehabilitation in COVID-19 pandemic situation. Egypt. Heart J. 2021, 73, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Flowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef] [PubMed]
- Besnier, F.; Gayda, M.; Nigam, A.; Juneau, M.; Bherer, L. Cardiac Rehabilitation During Quarantine in COVID-19 Pandemic: Challenges for Center-Based Programs. Arch. Phys. Med. Rehabilitation 2020, 101, 1835–1838. [Google Scholar] [CrossRef] [PubMed]
- Yasu, T. Comprehensive cardiac rehabilitation program for peripheral arterial diseases. J. Cardiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- ESC Guidelines on Peripheral Arterial Diseases (Diagnosis and Treatment Of). Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Peripheral-Artery-Diseases-Diagnosis-and-Treatment-of (accessed on 30 May 2022).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.E.; Levin, A. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- American Diabetes Association. Glycemic targets: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43, S66–S76. [Google Scholar] [CrossRef]
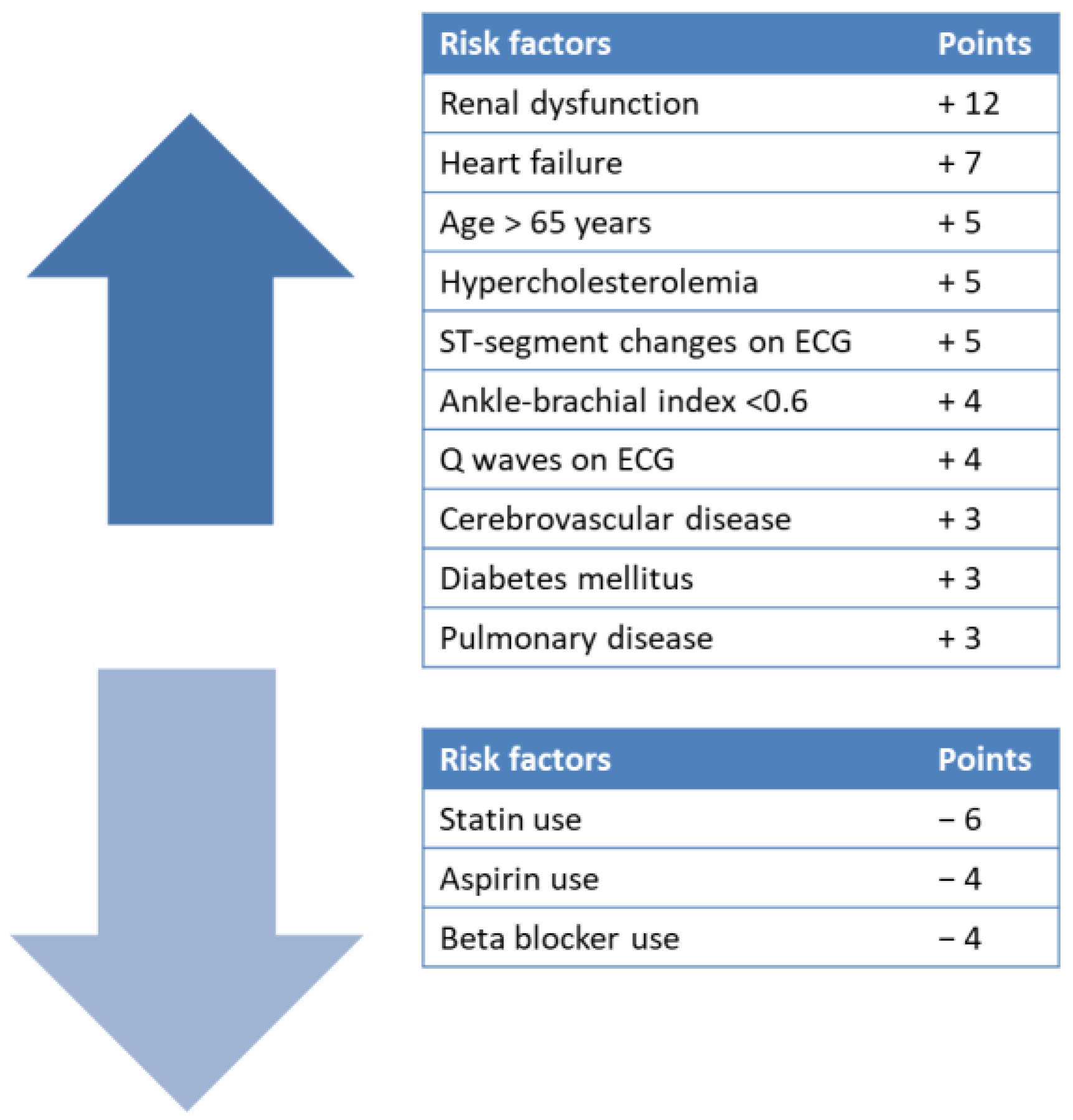
- Feringa, H.H.H. A Prognostic Risk Index for Long-term Mortality in Patients with Peripheral Arterial Disease. Arch. Intern. Med. 2007, 167, 2482–2489. [Google Scholar] [CrossRef] [Green Version]
- de Donato, G.; Pasqui, E.; Alba, G.; Abu Leil, M.; Palasciano, G. The Limitations of Social Behaviour Imposed by COVID-19 Impacted the Perception and the Evolution of Peripheral Arterial Disease Negatively. Ann. Vasc. Surg. 2021, 73, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Sharp, G.; Norton, R.; Zawada, J.; Dalal, H.; Dean, S.; Jolly, K.; Cowie, A.; Taylor, R. Home-based versus Centre-based Cardiac Rehabilitation. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Calabrese, M.; Garofano, M.; Palumbo, R.; Di Pietro, P.; Izzo, C.; Damato, A.; Venturini, E.; Iesu, S.; Virtuoso, N.; Strianese, A.; et al. Exercise Training and Cardiac Rehabilitation in COVID-19 Patients with Cardiovascular Complications: State of Art. Life 2021, 11, 259. [Google Scholar] [CrossRef]
- Selvin, E.; Erlinger, T.P. Prevalence of and Risk Factors for Peripheral Arterial Disease in the United States: Results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation 2004, 110, 738–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, N.; Sang, Y.; Chen, J.; Ballew, S.H.; Kalbaugh, C.A.; Salameh, M.J.; Blaha, M.J.; Allison, M.; Heiss, G.; Selvin, E.; et al. Cigarette Smoking, Smoking Cessation, and Long-Term Risk of 3 Major Atherosclerotic Diseases. J. Am. Coll. Cardiol. 2019, 74, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Lu, Y.; Ballew, S.H.; Tanaka, H.; Szklo, M.; Heiss, G.; Coresh, J.; Matsushita, K. 2017 ACC/AHA blood pressure classification and incident peripheral artery disease: The Atherosclerosis Risk in Communities (ARIC) Study. Eur. J. Prev. Cardiol. 2019, 27, 51–59. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Hammill, B.G.; Curtis, L.H.; Schulman, K.A.; Whellan, D.J. Relationship Between Cardiac Rehabilitation and Long-Term Risks of Death and Myocardial Infarction among Elderly Medicare Beneficiaries. Circulation 2010, 121, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Geiss, L.S.; Li, Y.; Hora, I.; Albright, A.; Rolka, D.; Gregg, E.W. Resurgence of Diabetes-Related Nontraumatic Lower-Extremity Amputation in the Young and Middle-Aged Adult, U.S. Population. Diabetes Care 2018, 42, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, M.G.; Klarin, D.; Assimes, T.L.; Freiberg, M.S.; Ingelsson, E.; Lynch, J.; Natarajan, P.; O’Donnell, C.; Rader, D.J.; Tsao, P.S.; et al. Genetics of Smoking and Risk of Atherosclerotic Cardiovascular Diseases: A Mendelian Randomization Study. JAMA Netw. Open 2021, 4, e2034461. [Google Scholar] [CrossRef] [PubMed]
- Dratva, J.; Probst-Hensch, N.; Schmidt-Trucksäss, A.; Caviezel, S.; de Groot, E.; Bettschart, R.; Saleh, L.; Gapoz, J.-M.; Rothe, T.; Schindler, C.; et al. Atherogenesis in youth–Early consequence of adolescent smoking. Atherosclerosis 2013, 230, 304–309. [Google Scholar] [CrossRef]
- Banerjee, A.; Fowkes, F.G.; Rothwell, P.M. Associations Between Peripheral Artery Disease and Ischemic Stroke: Implications for Primary and Secondary Prevention. Stroke 2010, 41, 2102–2107. [Google Scholar] [CrossRef]
- Farag, S.; Elbalkimy, M.; Elbassiouny, A.; George, J.; Fathy, M. Prevalence of peripheral arterial diseases in patients with large artery ischemic stroke and its prognostic value. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 1–6. [Google Scholar] [CrossRef]
- Tam, M.C.; Longenecker, C.T.; Chow, C.; Vest, M.; Sukeena, R.; Madan Mohan, S.K.; Carman, T.; Parikh, S.A.; Josephson, R.A. Occult peripheral artery disease is common and limits the benefit achieved in cardiac rehabilitation. Vasc. Med. 2016, 21, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Siercke, M.; Jørgensen, L.P.; Missel, M.; Thygesen, L.C.; Møller, S.P.; Sillesen, H.; Berg, S.K. Cardiovascular Rehabilitation Increases Walking Distance in Patients with Intermittent Claudication. Results of the CIPIC Rehab Study: A Randomised Controlled Trial. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 768–776. [Google Scholar] [CrossRef]
- Nishimura, H.; Miura, T.; Minamisawa, M.; Ueki, Y.; Abe, N.; Hashizume, N.; Mochidome, T.; Harada, M.; Shimizu, K.; Shoin, W.; et al. Prognostic value of ankle brachial index for future incident heart failure in patients without previous heart failure: Data from the impressive predictive value of ankle brachial index for clinical long term outcome in patients with cardiovascular disease examined by ABI study. Heart Vessel. 2016, 32, 295–302. [Google Scholar] [CrossRef]
- Gupta, D.K.; Skali, H.; Claggett, B.; Kasabov, R.; Cheng, S.; Shah, A.M.; Loehr, L.; Heiss, G.; Nambi, V.; Aguilar, D.; et al. Heart Failure Risk Across the Spectrum of Ankle-Brachial Index. JACC Heart Fail. 2014, 2, 447–454. [Google Scholar] [CrossRef]
- Prasada, S.; Shah, S.J.; Michos, E.D.; Polak, J.F.; Greenland, P. Ankle–brachial index and incident heart failure with reduced versus preserved ejection fraction: The Multi-Ethnic Study of Atherosclerosis. Vasc. Med. 2019, 24, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.; Murray, G.; Butcher, I.; Heald, C.L.; Lee, R.J.; Chambless, L.E.; Folsom, A.R.; Hirsch, A.T.; Dramaix, M.; Debacker, G.; et al. Ankle Brachial Index Combined with Framingham Risk Score to Predict Cardiovascular Events and Mortality: A meta-analysis. JAMA 2008, 300, 197–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rantner, B.; Kollerits, B.; Pohlhammer, J.; Stadler, M.; Lamina, C.; Peric, S.; Klein-Weigel, P.; Mühlthaler, H.; Fraedrich, G.; Kronenberg, F. The fate of patients with intermittent claudication in the 21st century revisited–results from the CAVASIC Study. Sci. Rep. 2017, 7, 45833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, M.M.; Guralnik, J.M.; Tian, L.; Liu, K.; Ferrucci, L.; Liao, Y.; Sharma, L.; Criqui, M.H. Associations of Borderline and Low Normal Ankle-Brachial Index Values with Functional Decline at 5-Year Follow-Up. J. Am. Coll. Cardiol. 2009, 53, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Heart Protection Study Collaborative Group. Randomized trial of the effects of cholesterol-lowering with simvastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. J. Vasc. Surg. 2007, 45, 645–654.e1. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.-Y.; Chen, Y.-T.; Su, Y.-W.; Chang, C.-C.; Huang, P.-H.; Lin, S.-J. Statin Therapy Reduces Future Risk of Lower-Limb Amputation in Patients with Diabetes and Peripheral Artery Disease. J. Clin. Endocrinol. Metab. 2017, 102, 2373–2381. [Google Scholar] [CrossRef]
- Kavanagh, T.; Hamm, L.F.; Beyene, J.; Mertens, D.J.; Kennedy, J.; Campbell, R.; Fallah, S.; Shephard, R.J. Usefulness of Improvement in Walking Distance Versus Peak Oxygen Uptake in Predicting Prognosis After Myocardial Infarction and/or Coronary Artery Bypass Grafting in Men. Am. J. Cardiol. 2008, 101, 1423–1427. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Vanhees, L.; Stevens, A.; Schepers, D.; DeFoor, J.; Rademakers, F.; Fagard, R. Determinants of the effects of physical training and of the complications requiring resuscitation during exercise in patients with cardiovascular disease. Eur. J. Cardiovasc. Prev. Rehabilitation 2004, 11, 304–312. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Before CR (n = 97) | Low & Low-Intermediate Risk Group (n = 45) | High-Intermediate & High Risk Group (n = 52) | p Value | ||
|---|---|---|---|---|---|---|
| Before CR | After CR | Before CR | After CR | |||
| Demographics | ||||||
| Males | 65 (67.0%) | - | - | - | ||
| Age, y | 69.66 ± 8.60 | 63.62 ± 10.32 | - | 70.81 ± 9.42 | - | - |
| Height, cm | 171.44 ± 8.77 | 170.51 ± 8.94 | - | 172.75 ± 8.18 | - | - |
| Weight, kg | 83.72 ± 15.49 | 74.08 ± 13.81 | 69.34 ± 10.98 | 72.14 ± 13.52 | 64.07 ± 12.93 | 0.034 |
| Body mass index, kg/m2 | 27.74 ± 3.65 | 28.85 ± 4.01 | 25.06 ± 2.93 | 26.57 ± 3.43 | 23.32 ± 2.96 | 0.005 |
| Resting hemodynamics | ||||||
| Heart rate, bpm | 72.71 ± 12.28 | 73.31 ± 14.03 | 68.83 ± 12.68 | 71.12 ± 10.53 | 64.49 ± 9.13 | 0.054 |
| Systolic BP, mmHg | 140.79 ± 21.56 | 144.63 ± 20.88 | 129.75 ± 21.27 | 141.34 ±19.98 | 139.06 ± 19.24 | 0.026 |
| Diastolic BP, mmHg | 80.15 ± 14.97 | 81.04 ± 14.68 | 75.98 ± 14.47 | 81.81 ± 14.65 | 78.38 ± 14.46 | 0.418 |
| Sedentary lifestyle | 69 (71.1%) | 29 (64.44%) | 22 (48.8%) | 40 (76.92%) | 29 (55.76%) | 0.030 |
| Smoking | ||||||
| Active/in the past | 63 (64.9%) | 21 (46.66%) | 9 (20.0%) | 42 (80.76%) | 20 (38.5%) | 0.048 |
| Alcohol | 16 (16.5%) | 5 (11.11%) | 2 (4.4%) | 11 (21.15%) | 7 (13.5%) | 0.130 |
| Obesity | 69 (71.1%) | 36 (80.0%) | 33 (73.3%) | 33 (63.5%) | 28 (53.8%) | 0.048 |
| Clinical signs | ||||||
| Paresthesia | 75 (77.3%) | 35 (77.8%) | 14 (31.1%) | 40 (76.9%) | 29 (55.8%) | 0.015 |
| Feeling of cold feet | 68 (70.1%) | 27 (60.0%) | 17 (37.8%) | 41 (78.8%) | 33 (63.5%) | 0.011 |
| Pale skin | 61 (62.9%) | 25 (55.6%) | 11 (24.4%) | 36 (69.2%) | 24 (46.2%) | 0.026 |
| Cold skin | 47 (48.5%) | 22 (48.9%) | 10 (22.2%) | 25 (48.1%) | 23 (44.2%) | 0.022 |
| Reduced pilosity | 36 (37.1%) | 18 (40%) | 17 (37.8%) | 18 (34.61%) | 15 (28.8%) | 0.351 |
| Subcutaneous atrophy | 22 (22.68%) | 9 (21.42%) | 9 (20.0%) | 13 (25%) | 12 (23.1%) | 0.714 |
| Thickened nails | 22 (22.7%) | 10 (23.8%) | 10 (22.2%) | 12 (23.07%) | 12 (23.1%) | 0.920 |
| Petechiae | 32 (33.0%) | 17 (37.8%) | 8 (17.8%) | 15 (28.8%) | 13 (25.0%) | 0.389 |
| Arterial ulcers | 5 (5.2%) | 2 (4.4%) | 1 (2.2%) | 3 (5.8%) | 4 (7.7%) | 0.450 |
| Dermatitis | 14 (14.4%) | 8 (17.8%) | 5 (11.1%) | 6 (11.5%) | 7 (13.5%) | 0.726 |
| Risk Factors | Low & Low-Intermediate Risk Group (n = 45) | High-Intermediate & High Risk Group (n = 52) | p Value |
|---|---|---|---|
| Renal dysfunction | 4 (8.9%) | 49 (94.2%) | <0.001 |
| Heart failure | 36 (80.0%) | 34 (65.4%) | 0.111 |
| Age > 65 years | 20 (44.4%) | 28 (53.8%) | 0.361 |
| Hypercholesterolemia | 18 (40.0%) | 39 (75.0%) | <0.001 |
| ST-segment changes | 31 (68.9%) | 25 (48.1%) | 0.039 |
| ABI <0.6 | 17 (37.8%) | 23 (44.2%) | 0.525 |
| Q-waves | 22 (48.9%) | 20 (38.5%) | 0.306 |
| Cerebrovascular disease | 14 (31.1%) | 23 (44.2%) | 0.188 |
| Diabetes mellitus | 13 (28.9%) | 43 (82.7%) | <0.001 |
| Pulmonary disease | 3 (6.7%) | 11 (21.2%) | 0.043 |
| Therapeutic Agents | Low & Low-Intermediate Risk Group (n = 45) | High-Intermediate & High Risk Group (n = 52) |
|---|---|---|
| Beta-blockers | 42 (93.3%) | 50 (96.15%) |
| Renin-angiotensin system blockers | 38 (84.44%) | 50 (96.15%) |
| Oral antidiabetics | 45 (100%) | 47 (88.47%) |
| Insulin | 0 (0%) | 5 (11.53%) |
| Statins | 45 (100%) | 52 (100%) |
| Aspirin | 45 (100%) | 52 (100%) |
| Parameter | Before CR (n = 97) | Low & Low-Intermediate Risk Group (n = 45) | High-Intermediate & High Risk Group (n = 52) |
|---|---|---|---|
| Blood biochemistry | |||
| Total cholesterol, mg/dL | 206.95 ± 75.90 | 217.72 ± 74.32 | 198.03 ± 78.85 |
| LDL-cholesterol, mg/dL | 135.40 ± 67.79 | 140.44 ± 64.44 | 131.05 ± 71.14 |
| HDL-cholesterol, mg/dL | 42.84 ± 16.92 | 43.63 ± 16.87 | 42.17 ± 17.11 |
| Triglycerides, mg/dL | 185.27 ± 122.13 | 186.57 ± 93.75 | 184.15 ± 143.16 |
| CRP, mg/dL | 5.33 ± 14.30 | 3.55 ± 4.19 | 6.87 ± 19.10 |
| HbA1C, g% | 7.96 ± 2.23 | 6.23 ± 0.87 | 9.92 ± 1.60 |
| Fasting glucose, mg/dL | 153.94 ± 63.54 | 128.55 ± 29.17 | 166.30 ± 77.72 |
| Exercise stress test | |||
| VO2peak mL/kg/min | 12.34 ± 4.74 | 12.06 ± 4.27 | 12.59 ± 5.14 |
| Peak HR, bpm | 118.61 ± 18.81 | 119.49 ± 18.66 | 116.73 ± 19.13 |
| Peak systolic BP, mmHg | 171.52 ± 27.03 | 174.47 ± 26.31 | 170.58 ± 27.91 |
| Peak diastolic BP, mmHg | 90.54 ± 13.31 | 89.36 ± 14.14 | 91.58 ± 12.61 |
| RER | 1.07 ± 0.10 | 1.07 ± 0.11 | 1.08 ± 0.10 |
| Borg scale | 15.45 ± 1.58 | 15.16 ± 1.48 | 15.02 ± 1.87 |
| ABI | 0.65 ± 0.21 | 0.74 ± 0.21 | 0.70 ± 0.23 |
| Pain free walking distance, m | 246.43 ± 185.49 | 220.44 ± 159.09 | 165.19 ± 124.88 |
| Walking time, min | 24.75 ± 9.15 | 29.50 ± 8.41 | 20.63 ± 7.72 |
| Walking distance, m | 253.27 ± 161.77 | 285.81 ± 153.67 | 225.12 ± 124.88 |
| Echocardiography | |||
| LVEF, % | 46.41 ± 9.74 | 47.60 ± 9.45 | 45.13 ± 10.82 |
| Parameter | 6 Months Follow-Up (n = 97) | Low & Low-Intermediate Risk Group (n = 45) | High-Intermediate & High Risk Group (n = 52) | p Value |
|---|---|---|---|---|
| Blood biochemistry | ° | ° | ° | ° |
| Total cholesterol, mg/dL | 172.92 ± 63.12 | 165.96 ± 65.85 | 180.98 ± 59.53 | 0.245 |
| LDL-cholesterol, mg/dL | 121.86 ± 61.01 | 101.96 ± 41.73 | 130.97 ± 48.90 | 0.002 |
| HDL-cholesterol, mg/dL | 44.56 ± 17.60 | 45.37 ± 17.54 | 43.86 ± 17.79 | 0.675 |
| Triglycerides, mg/dL | 161.18 ± 106.26 | 132.19 ± 63.12 | 180.29 ± 126.53 | 0.032 |
| CRP, mg/dL | 3.42 ± 5.07 | 2.40 ± 2.78 | 4.32 ± 6.33 | 0.063 |
| HbA1C, g% | 7.53 ± 1.93 | 7.08 ± 1.85 | 7.92 ± 1.94 | 0.003 |
| Fasting glucose, mg/dL | 140.67 ± 52.73 | 126.09 ± 31.59 | 153.30 ± 63.44 | 0.011 |
| Exercise stress test | ||||
| VO2peak mL/kg/min | 14.31 ± 4.74 | 15.96 ± 6.07 | 12.88 ± 4.52 | 0.005 |
| Peak HR, bpm | 131.66 ± 20.88 | 134.14 ± 18.16 | 128.59 ± 21.62 | 0.178 |
| Peak systolic BP, mmHg | 157.17 ± 19.78 | 152.28 ± 19.08 | 161.83 ± 19.83 | 0.018 |
| Peak diastolic BP, mmHg | 88.73 ± 13.04 | 87.57 ± 13.85 | 86.75 ± 12.36 | 0.415 |
| RER | 1.09 ± 0.10 | 1.09 ± 0.12 | 1.10 ± 0.11 | 0.695 |
| Borg scale | 13.31 ± 1.14 | 13.64 ± 1.03 | 13.02 ± 1.16 | 0.006 |
| ABI | 0.81 ± 0.25 | 0.87 ± 0.25 | 0.76 ± 0.26 | 0.034 |
| Pain free walking distance, m | 274.96 ± 175.52 | 323 ± 170.36 | 233.30 ± 170.87 | 0.011 |
| Walking time, min | 28.46 ± 10.53 | 33.93 ± 9.67 | 23.72 ± 8.88 | <0.001 |
| Walking distance, m | 300.58 ± 187.48 | 361.64 ± 180.55 | 247.75 ± 178.61 | 0.002 |
| Echocardiography | ||||
| LVEF, % | 49.37 ± 10.43 | 51.47 ± 11.25 | 47.35 ± 9.71 | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anghel, R.; Adam, C.A.; Mitu, O.; Marcu, D.T.M.; Onofrei, V.; Roca, M.; Costache, A.D.; Miftode, R.S.; Tinica, G.; Mitu, F. Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome. Diagnostics 2022, 12, 1500. https://doi.org/10.3390/diagnostics12061500
Anghel R, Adam CA, Mitu O, Marcu DTM, Onofrei V, Roca M, Costache AD, Miftode RS, Tinica G, Mitu F. Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome. Diagnostics. 2022; 12(6):1500. https://doi.org/10.3390/diagnostics12061500
Chicago/Turabian StyleAnghel, Razvan, Cristina Andreea Adam, Ovidiu Mitu, Dragos Traian Marius Marcu, Viviana Onofrei, Mihai Roca, Alexandru Dan Costache, Radu Stefan Miftode, Grigore Tinica, and Florin Mitu. 2022. "Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome" Diagnostics 12, no. 6: 1500. https://doi.org/10.3390/diagnostics12061500
APA StyleAnghel, R., Adam, C. A., Mitu, O., Marcu, D. T. M., Onofrei, V., Roca, M., Costache, A. D., Miftode, R. S., Tinica, G., & Mitu, F. (2022). Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome. Diagnostics, 12(6), 1500. https://doi.org/10.3390/diagnostics12061500