
Understanding Sensitization, Cognitive and Neuropathic Associated Mechanisms behind Post-COVID Pain: A Network Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Sensory-Related Variables
2.3. Psychological Variables
2.4. Health-Related Quality of Life
2.5. Sleep Quality
2.6. Data Analysis
3. Results
4. Discussion
4.1. Importance of Neuropathic and Sensitization Mechanisms
4.2. Importance of Function
4.3. Importance of Gender
4.4. Clinical Applications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of Post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Int. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C. Long COVID: Current definition. Infection 2022, 50, 285–286. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Navarro-Santana, M.; Plaza-Manzano, G.; Palacios-Ceña Arendt-Nielsen, L. Time course prevalence of Post-COVID pain symptoms of musculoskeletal origin in patients who had survived to SARS-CoV-2 infection: A systematic review and meta-analysis. Pain 2021, 169, 1220–1231. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; de-la-Llave-Rincón, A.I.; Ortega-Santiago, R.; Ambite-Quesada, S.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Hernández-Barrera, V.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; et al. Prevalence and risk factors of musculoskeletal pain symptoms as long-term post-COVID sequelae in hospitalized COVID-19 survivors: A multicenter study. Pain 2021. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Montes, M.; Fernández-de-las-Peñas, C.; Ferrer-Pargada, D.; Tello-Mena, S.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Palacios-Ceña, D.; Parás-Bravo, P. Prevalence of neuropathic component in post-COVID pain symptoms in previously hospitalized COVID-19 survivors. Int. J. Clin. Pract. 2022, 2022, 3532917. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.S.C.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Gómez-Mayordomo, V.; de-la-Llave-Rincón, A.I.; Palacios-Ceña, M.; Rodríguez-Jiménez, J.; Florencio, L.L.; Velasco-Arribas, M.; Fuensalida-Novo, S.; Cigarán-Méndez, M.; Ambite-Quesada, S.; et al. Anxiety, depression and poor sleep quality as long-term post-COVID sequelae in previously hospitalized patients: A multicenter study. J. Infect. 2021, 83, 496–522. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Noppen, M.; Moens, M. Is central sensitisation the missing link of persisting symptoms after COVID-19 infection? J. Clin. Med. 2021, 10, 5594. [Google Scholar] [CrossRef] [PubMed]
- Schmittmann, V.D.; Cramer, A.O.J.; Waldorp, L.J.; Epskamp, S.; Kievit, R.A.; Borsboom, D. Deconstructing the construct: A network perspective on psychological phenomena. New Ideas Psychol. 2013, 31, 43–53. [Google Scholar] [CrossRef]
- Valente, T.W. Network Interventions. Science 2012, 337, 49. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, M.; Valera-Calero, J.A.; Cuadrado, M.L.; Guerrero-Peral, A.; Pareja, J.A.; Arendt-Nielsen, L.; Varol, U. Understanding the interaction between clinical, emotional and psychophysical outcomes underlying tension-type headache: A network analysis approach. J. Neurol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Liew, B.X.W.; De-la-Llave-Rincón, A.I.; Arias-Buría, J.L.; Ortega-Santiago, R.; Fernández-de-las-Peñas, C. Understanding the psychophysiological mechanisms related to widespread pressure pain hyperalgesia underpinning carpal tunnel syndrome: A Network Analysis Approach. Pain Med. 2021, 22, 2708–2717. [Google Scholar] [CrossRef]
- López-de-Uralde-Villanueva, I.; Gil-Martínez, A.; Candelas-Fernández, P.; de Andrés-Ares, J.; Beltrán-Alacreu, H.; La Touche, R. Validity and reliability of the Spanish-language version of the self-administered Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) pain scale. Neurologia 2018, 33, 505–514. [Google Scholar] [CrossRef]
- De Andrés, J.; Pérez-Cajaraville, J.; Lopez-Alarcón, M.D.; López-Millán, J.M.; Margarit, C.; Rodrigo-Royo, M.D.; Franco-Gay, M.L.; Abejón, D.; Ruiz, M.A.; López-Gomez, V.; et al. Cultural adaptation and validation of the painDETECT scale into Spanish. Clin. J. Pain. 2012, 28, 243–253. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.I.; Roldan-Jimenez, C.; Neblett, R.; Gatchel, R.J. Cross-cultural adaptation and validity of the Spanish central sensitization inventory. Springerplus 2016, 5, 1837. [Google Scholar] [CrossRef] [Green Version]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement properties of the central sensitization inventory: A systematic review. Pain Pract. 2018, 18, 544–554. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Grupo de Trabajo de la Guía de Práctica Clínica para el Manejo de Pacientes con Trastornos de Ansiedad en Atención Primaria 2008. Guías de Práctica Clínica en el SNS—UETS Nº 2006/10. Madrid: Plan Nacional para el SNS del MSC; Unidad de Evaluación de Tecnologías Sanitarias, Agencia Laín Entralgo, Comunidad de Madrid: Madrid, Spain, 2008. [Google Scholar]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Van Hout, B.; Janssen, M.F.; Feng, Y.J.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; KindM, P.; Pickard, S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Glasso: Graphical Lasso Estimation of Gaussian Graphical Models; R Package Version. 2014, Volume 1. Available online: https://cran.r-project.org/web/packages/glasso/index.html (accessed on 15 April 2022).
- Shraim, M.A.; Massé-Alarie, H.; Hodges, P.W. Methods to discriminate between mechanism-based categories of pain experienced in the musculoskeletal system: A systematic review. Pain 2021, 162, 1007–1037. [Google Scholar] [CrossRef]
- Nijs, J.; Huysmans, E. Clinimetrics: The Central Sensitisation Inventory: A useful screening tool for clinicians, but not the gold standard. J. Physiother. 2021, 21, S1836–S9553. [Google Scholar] [CrossRef]
- Moreton, B.J.; Tew, V.; das Nair, R.; Wheeler, M.; Walsh, D.A.; Lincoln, N.B. Pain phenotype in patients with knee osteoarthritis: Classification and measurement properties of painDETECT and self-report Leeds assessment of neuropathic symptoms and signs scale in a cross-sectional study. Arthritis Care Res. 2015, 67, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Cotchett, M.; Lennecke, A.; Medica, V.G.; Whittaker, G.A.; Bonanno, D.R. The association between pain catastrophising and kinesiophobia with pain and function in people with plantar heel pain. Foot 2017, 32, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Priore, L.B.; Azevedo, F.M.; Pazzinatto, M.F.; Ferreira, A.S.; Hart, H.F.; Barton, C.; de Oliveira Silva, D. Influence of kinesiophobia and pain catastrophism on objective function in women with patellofemoral pain. Phys. Ther. Sport. 2019, 35, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Kroska, E.B. A meta-analysis of fear-avoidance and pain intensity: The paradox of chronic pain. Scand. J. Pain 2016, 13, 43–58. [Google Scholar] [CrossRef] [PubMed]
- El Sayed, S.; Gomaa, S.; Shokry, D.; Kabil, A.; Eissa, A. Sleep in post-COVID-19 recovery period and its impact on different domains of quality of life. Egypt J. Neurol. Psychiatr. Neurosurg. 2021, 57, 172. [Google Scholar] [CrossRef]
- Maglietta, G.; Diodati, F.; Puntoni, M.; Lazzarelli, S.; Marcomini, B.; Patrizi, L.; Caminiti, C. Prognostic factors for Post-COVID-19 syndrome: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 1541. [Google Scholar] [CrossRef]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Cattadori, G.; Di Marco, S.; Baravelli, M.; Picozzi, A.; Ambrosio, G. Exercise Training in Post-COVID-19 Patients: The need for a multifactorial protocol for a multifactorial pathophysiology. J. Clin. Med. 2022, 11, 2228. [Google Scholar] [CrossRef]
- O’Leary, H.; Smart, K.M.; Moloney, N.A.; Doody, C.M. Nervous system sensitization as a predictor of outcome in the treatment of peripheral musculoskeletal conditions: A systematic review. Pain Pract. 2017, 17, 249–266. [Google Scholar] [CrossRef]
- Ferro Moura Franco, K.; Lenoir, D.; Dos Santos Franco, Y.R.; Jandre Reis, F.J.; Nunes Cabral, C.M.; Meeus, M. Prescription of exercises for the treatment of chronic pain along the continuum of nociplastic pain: A systematic review with meta-analysis. Eur. J. Pain 2021, 25, 51–70. [Google Scholar] [CrossRef]
- Dotan, A.; David, P.; Arnheim, D.; Shoenfeld, Y. The autonomic aspects of the post-COVID19 syndrome. Autoimmun Rev. 2022, 21, 103071. [Google Scholar] [CrossRef]




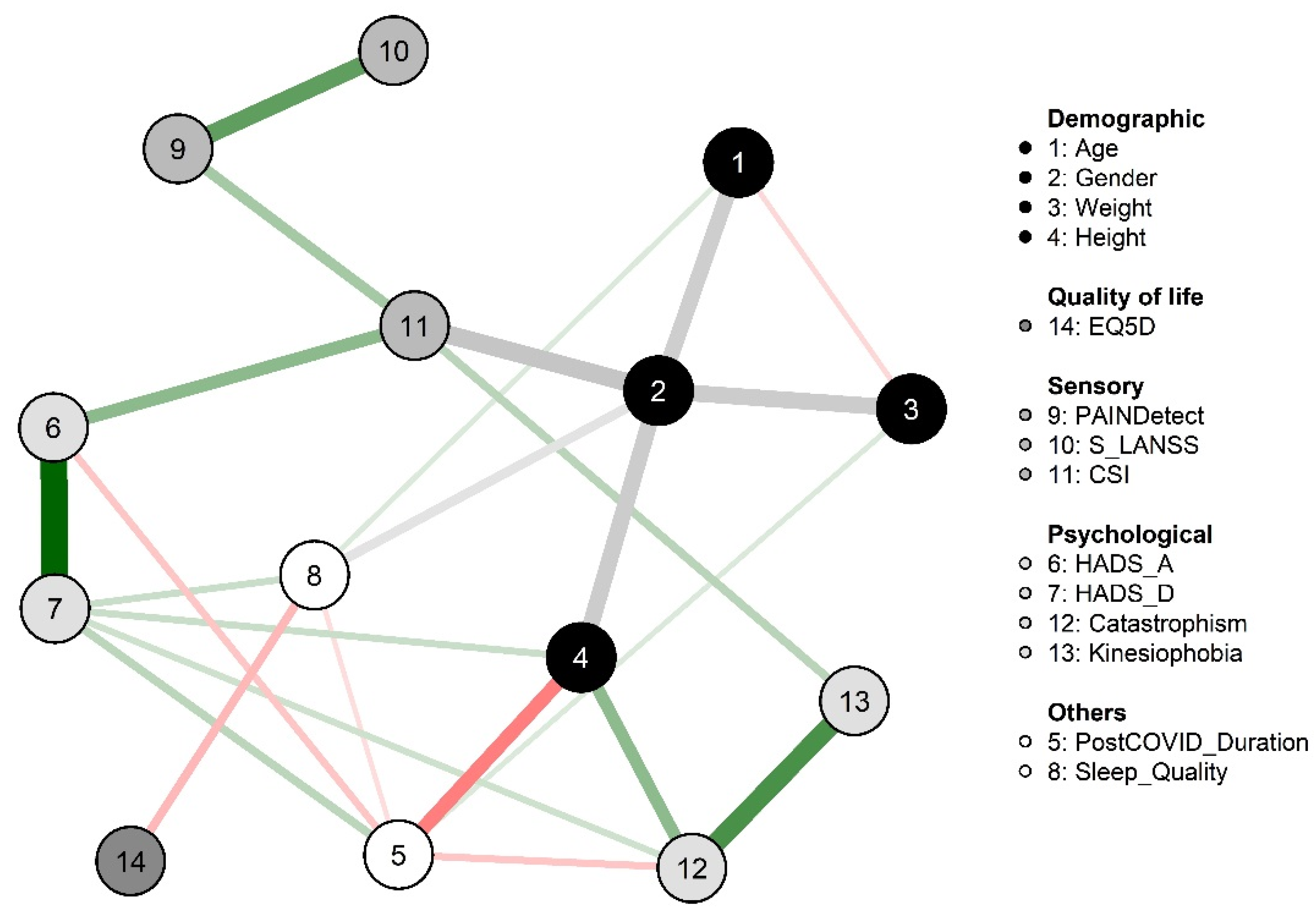{kind=link}
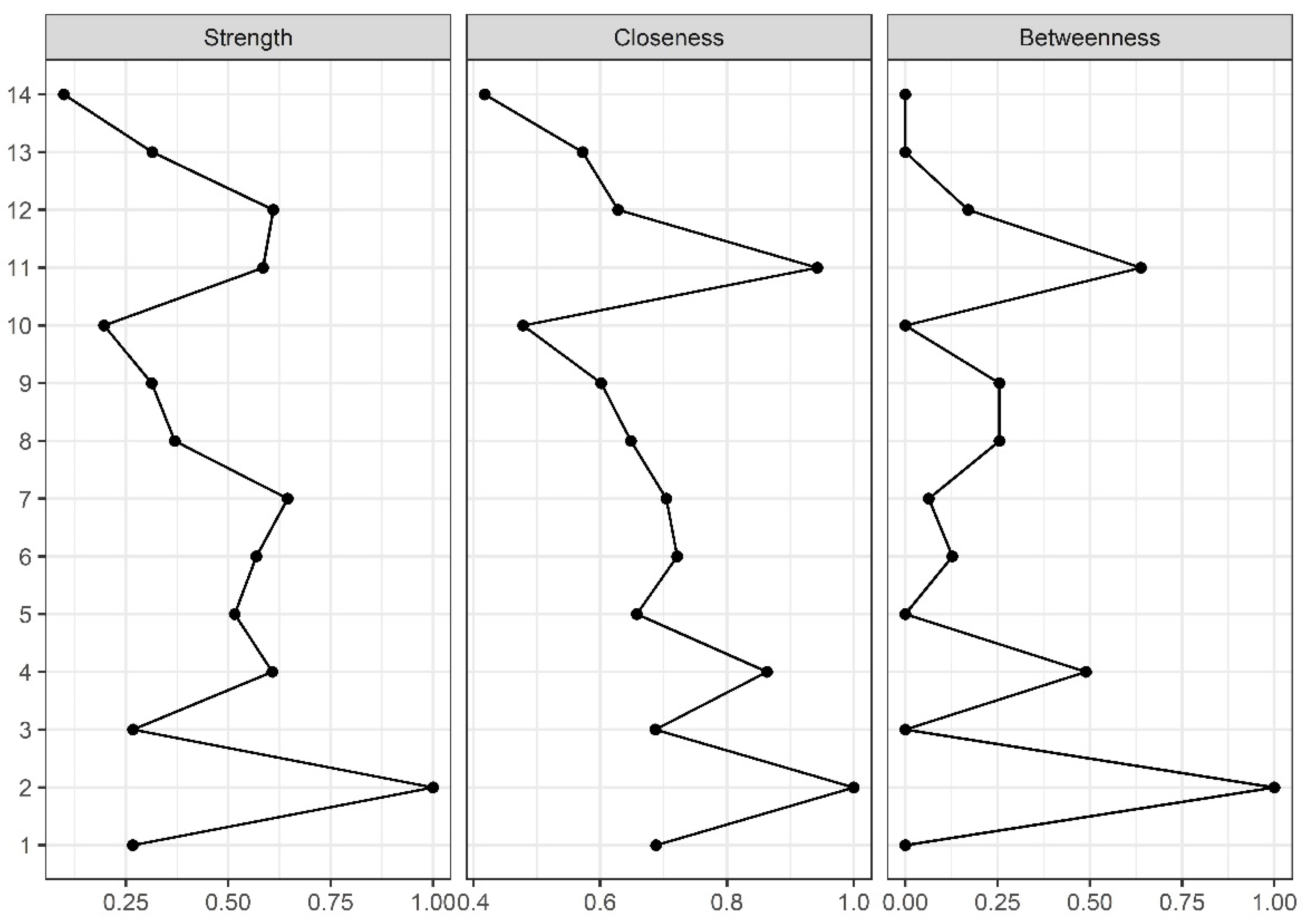{kind=link}
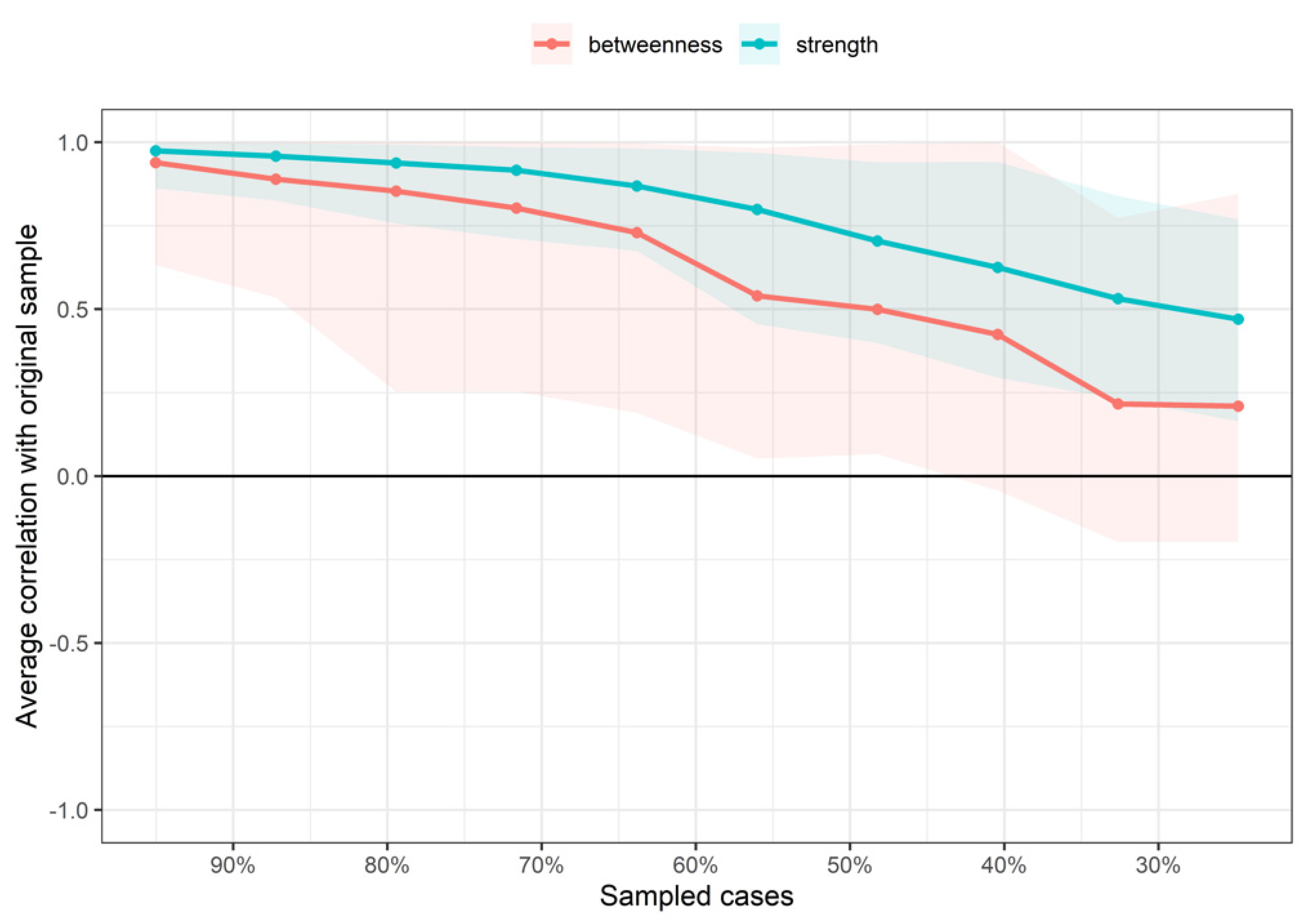{kind=link}
| Variable | |
|---|---|
| Age (years) | 57.3 ± 11.7 |
| Gender (male, n; %) | 66; 46.8 |
| Weight (kg) | 81.8 ± 17.0 |
| Height (cm) | 1.65 ± 0.10 |
| Post-COVID Duration (months) | 18.8 ± 1.8 |
| HADS-A (0–21) | 5.2 ± 4.2 |
| HADS-D (0–21) | 4.9 ± 4.3 |
| PSQI (0–21) | 8.0 ± 4.2 |
| PainDETECT (−1 to 38) | 7.0 ± 6.2 |
| S-LANSS (0–24) | 7.5 ± 8.5 |
| CSI (0–100) | 33.9 ± 17.2 |
| PCS (0–52) | 12.3 ± 12.0 |
| TSK-11 (0–44) | 24.0 ± 8.6 |
| EuroQol-5D-5L (0–1) | 0.8 ± 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-de-las-Peñas, C.; Herrero-Montes, M.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Parás-Bravo, P.; Varol, U.; del-Valle-Loarte, P.; Flox-Benítez, G.; Arendt-Nielsen, L.; Valera-Calero, J.A. Understanding Sensitization, Cognitive and Neuropathic Associated Mechanisms behind Post-COVID Pain: A Network Analysis. Diagnostics 2022, 12, 1538. https://doi.org/10.3390/diagnostics12071538
Fernández-de-las-Peñas C, Herrero-Montes M, Cancela-Cilleruelo I, Rodríguez-Jiménez J, Parás-Bravo P, Varol U, del-Valle-Loarte P, Flox-Benítez G, Arendt-Nielsen L, Valera-Calero JA. Understanding Sensitization, Cognitive and Neuropathic Associated Mechanisms behind Post-COVID Pain: A Network Analysis. Diagnostics. 2022; 12(7):1538. https://doi.org/10.3390/diagnostics12071538
Chicago/Turabian StyleFernández-de-las-Peñas, César, Manuel Herrero-Montes, Ignacio Cancela-Cilleruelo, Jorge Rodríguez-Jiménez, Paula Parás-Bravo, Umut Varol, Pablo del-Valle-Loarte, Gema Flox-Benítez, Lars Arendt-Nielsen, and Juan A. Valera-Calero. 2022. "Understanding Sensitization, Cognitive and Neuropathic Associated Mechanisms behind Post-COVID Pain: A Network Analysis" Diagnostics 12, no. 7: 1538. https://doi.org/10.3390/diagnostics12071538
APA StyleFernández-de-las-Peñas, C., Herrero-Montes, M., Cancela-Cilleruelo, I., Rodríguez-Jiménez, J., Parás-Bravo, P., Varol, U., del-Valle-Loarte, P., Flox-Benítez, G., Arendt-Nielsen, L., & Valera-Calero, J. A. (2022). Understanding Sensitization, Cognitive and Neuropathic Associated Mechanisms behind Post-COVID Pain: A Network Analysis. Diagnostics, 12(7), 1538. https://doi.org/10.3390/diagnostics12071538