
The Effects of 810 nm Diode Laser and Indocyanine Green on Periodontal Parameters and HbA1c in Patients with Periodontitis and Type II Diabetes Mellitus: A Randomized Controlled Study

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
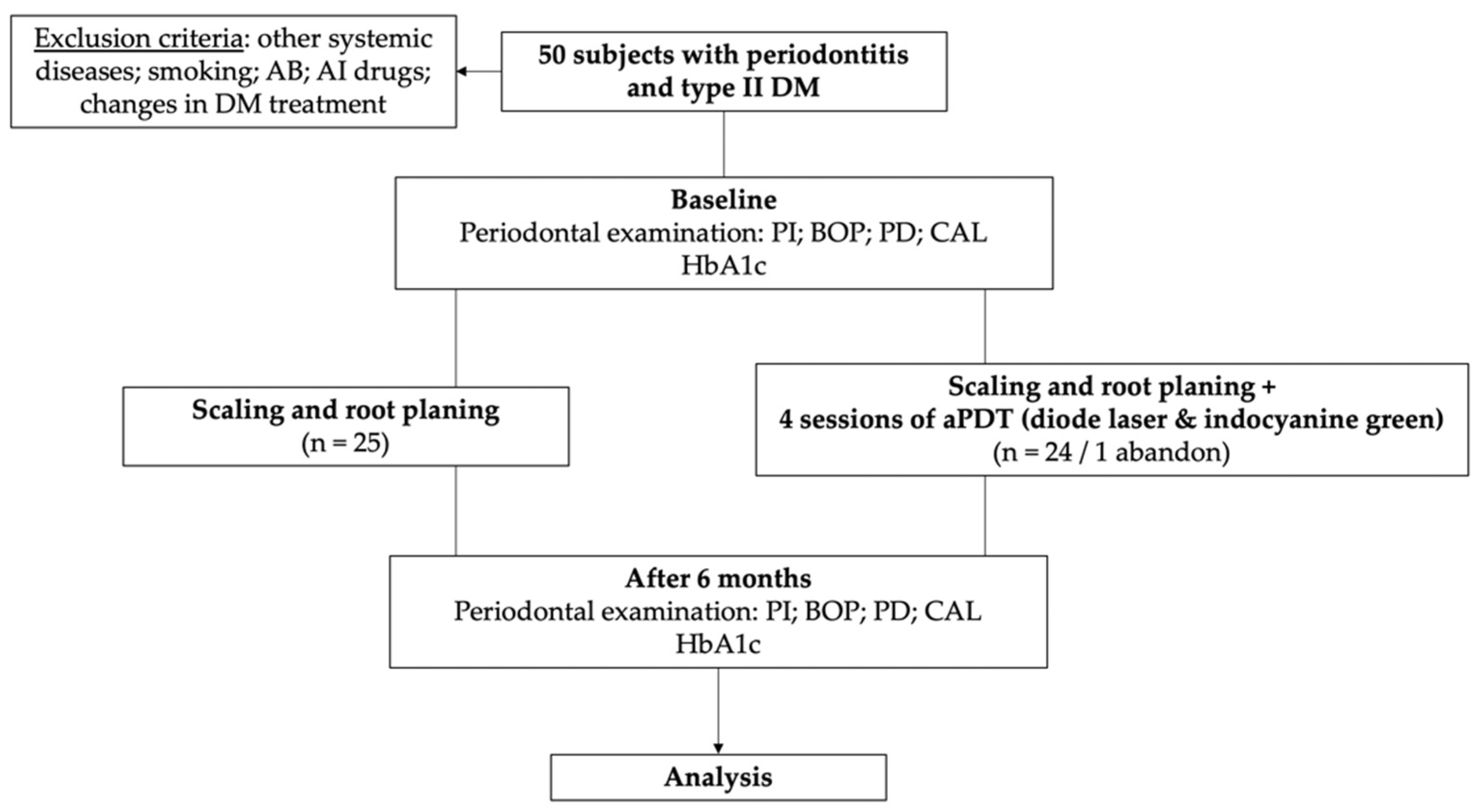
2. Materials and Methods
2.1. Patient Selection
2.2. Sample Size Calculation and Randomization
2.3. Clinical Investigations
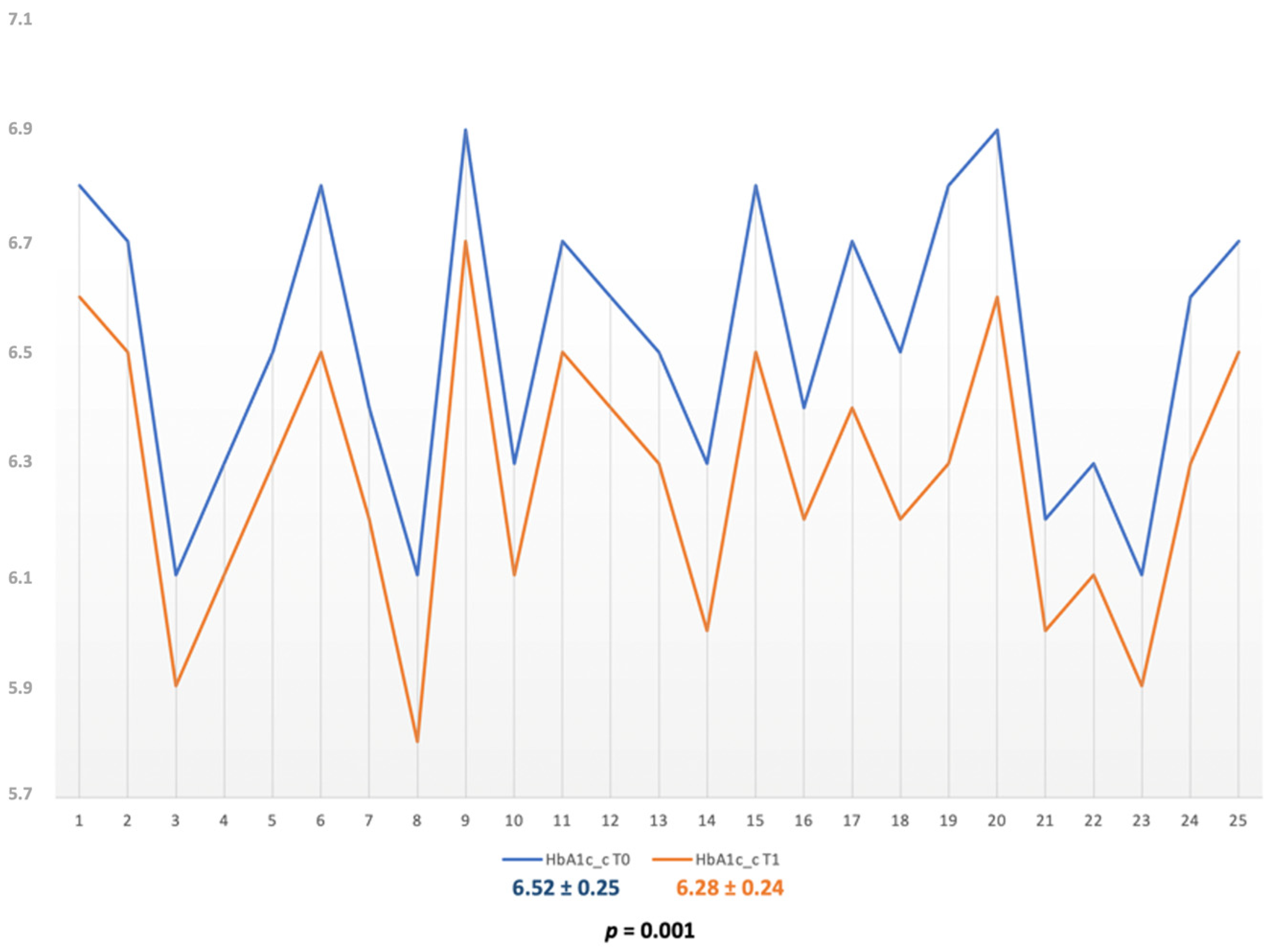
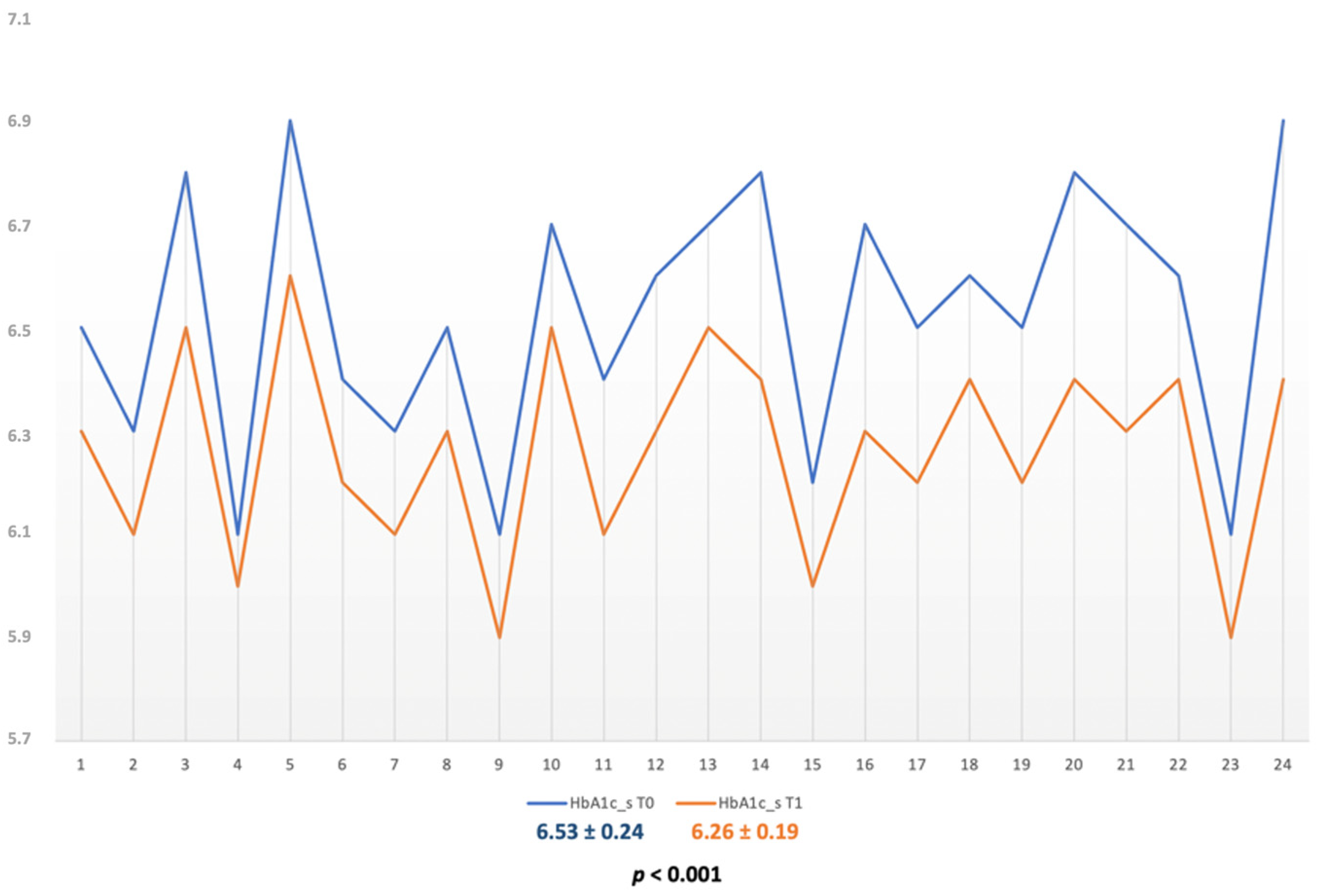
2.4. Evaluation of HbA1c
2.5. Treatment Methods
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Dyke, T.E.; Bartold, P.M.; Reynolds, E.C. The nexus between periodontal inflammation and dysbiosis. Front. Immunol. 2020, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Gibertoni, F.; Sommer, M.E.L.; Esquisatto, M.A.M.; Amaral, M.E.C.D.; Oliveira, C.A.; Andrade, T.A.M.; Mendonça, F.A.S.; Santamaria, M., Jr.; Felonato, M. Evolution of periodontal disease: Immune response and RANK/RANKL/OPG system. Braz. Dent. J. 2017, 28, 679–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.; Wu, M.Z.; Yu, S.Y.; Pelekos, G.; Yiu, K.H.; Jin, L. Periodontitis links to concurrent systemic comorbidities among ‘self-perceived health’ individuals. J. Periodontal Res. 2022, 57, 632–643. [Google Scholar] [CrossRef]
- Namayandeh, S.M.; Karimi, A.; Fallahzadeh, H.; Rahmanian, M.; Sadr Bafghi, S.M.; Soltani, M.; Hadiani, L. The incidence rate of diabetes mellitus (type II) and its related risk factors: A 10-year longitudinal study of Yazd Healthy Heart Cohort (YHHC). Iran. Diabetes Metab. Syndr. 2019, 13, 1437–1441. [Google Scholar] [CrossRef]
- Eschwège, E. Epidémiologie du diabète de type 2, diagnostic, prévalence, facteurs de risque, complications [Epidemiology of type II diabetes, diagnosis, prevalence, risk factors, complications]. Arch. Mal. Coeur Vaiss 2000, 4, 13–17. [Google Scholar]
- Löe, H. Periodontal disease. The sixth complication of diabetes mellitus. Diabetes Care 1993, 16, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Stevens, D.L.; Herman, W.H.; Funnell, M.M.; Standiford, C.J. Screening, prevention, counseling, and treatment for the complications of type II diabetes mellitus. Putting evidence into practice. J. Gen. Intern. Med. 1997, 12, 567–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astolfi, V.; Ríos-Carrasco, B.; Gil-Mur, F.J.; Ríos-Santos, J.V.; Bullón, B.; Herrero-Climent, M.; Bullón, P. Incidence of peri-implantitis and relationship with different conditions: A retrospective study. Int J. Environ. Res. Public Health 2022, 19, 4147. [Google Scholar] [CrossRef]
- Elkerbout, T.A.; Slot, D.E.; Rijnen, M.E.; van der Weijden, G.A.F. Change in oral hygiene behaviour after non-surgical periodontal therapy-A retrospective analyses. Int. J. Dent. Hyg. 2022, 0, 1–13. [Google Scholar] [CrossRef]
- Koromantzos, P.A.; Makrilakis, K.; Dereka, X.; Katsilambros, N.; Vrotsos, I.A.; Madianos, P.N. A randomized, controlled trial on the effect of non-surgical periodontal therapy in patients with type 2 diabetes. Part I: Effect on periodontal status and glycaemic control. J. Clin. Periodontol. 2011, 38, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.-L.; Chen, L.-L.; Zhang, S.-Z.; Wu, Y.-M.; Ren, Y.-Z.; Qin, G.-M. Inflammatory cytokines, adiponectin, insulin resistance and metabolic control after periodontal intervention in patients with type 2 diabetes and chronic periodontitis. Intern. Med. 2011, 50, 1569–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.; Gupta, J.; Bansal, D.; Sood, S.; Gupta, S.; Jain, A. Effect of scaling and root planing as monotherapy on glycemic control in patients of Type 2 diabetes with chronic periodontitis: A systematic review and meta-analysis. J. Indian Soc. Periodontol. 2019, 23, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Madianos, P.N.; Koromantzos, P.A. An update of the evidence on the potential impact of periodontal therapy on diabetes outcomes. J. Clin. Periodontol. 2018, 45, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; Stein, J.M.; Schumacher, A.; Kupietz, D.; Yekta-Michael, S.S.; Schittenhelm, F.; Conrads, G.; Schaller, H.G.; Reichert, S. Nonsurgical Periodontal Treatment Options and Their Impact on Subgingival Microbiota. J. Clin. Med. 2022, 11, 1187. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, K.; Jepsen, S. Antibiotics/antimicrobials: Systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontology 2000 2016, 71, 82–112. [Google Scholar] [CrossRef]
- Golub, L.M.; Lee, H.M. Periodontal therapeutics: Current host-modulation agents and future directions. Periodontology 2000 2020, 82, 186–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobotta, L.; Skupin-Mrugalska, P.; Piskorz, J.; Mielcarek, J. Non-porphyrinoid photosensitizers mediated photodynamic inactivation against bacteria. Dye. Pigment. 2019, 163, 337–355. [Google Scholar] [CrossRef]
- Sales, L.S.; Miranda, M.L.; de Oliveira, A.B.; Ferrisse, T.M.; Fontana, C.R.; Milward, M.; Brighenti, F.L. Effect of the technique of photodynamic therapy against the main microorganisms responsible for periodontitis: A systematic review of in-vitro studies. Arch. Oral Biol. 2022, 138, 105425. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Zhang, H.; Wang, X.; Lv, J.; Liu, D.; Shen, W.; Li, Y.; Du, J.; Yang, Q. Development of a NIR fluorescent probe for highly selective and sensitive detection of cysteine in living cells and in vivo. Talanta 2021, 234, 122685. [Google Scholar] [CrossRef] [PubMed]
- Porcu, E.P.; Salis, A.; Gavini, E.; Rassu, G.; Maestri, M.; Giunchedi, P. Indocyanine green delivery systems for tumour detection and treatments. Biotechnol. Adv. 2016, 34, 768–789. [Google Scholar] [CrossRef] [PubMed]
- Houthoofd, S.; Vuylsteke, M.; Mordon, S.; Fourneau, I. Photodynamic therapy for atherosclerosis. The potential of indocyanine green. Photodiagnosis Photodyn. Ther. 2020, 29, 101568. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, C.; Shang, S.; Luo, Z. Scaling and root planing with enhanced root planing on healthcare for type 2 diabetes mellitus: A randomized controlled clinical trial. J. Dent. Sci 2013, 8, 272–280. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Anton, D.-M.; Martu, M.-A.; Maris, M.; Maftei, G.-A.; Sufaru, I.-G.; Tatarciuc, D.; Luchian, I.; Ioanid, N.; Martu, S. Study on the Effects of Melatonin on Glycemic Control and Periodontal Parameters in Patients with Type II Diabetes Mellitus and Periodontal Disease. Medicina 2021, 57, 140. [Google Scholar] [CrossRef]
- Zaharescu, A.; Martu, I.; Luchian, A.; Martu, M.; Sufaru, I.; Martu, C.; Solomon, S. Role of adjunctive therapy with subantimicrobial doses of doxycycline in glycemic control (HbA1c) in patients with diabetes and endo-periodontal lesions to prevent sinus complications. Exp. Ther. Med. 2021, 21, 277. [Google Scholar] [CrossRef]
- Hamwi, A.; Schweiger, C.R.; Veitl, M.; Schmid, R. Quantitative measurement of HbA1c by an immunoturbidimetric assay compared to a standard HPLC method. Am. J. Clin. Pathol 1995, 104, 89–95. [Google Scholar] [CrossRef]
- Raut, C.P.; Sethi, K.S.; Kohale, B.R.; Mamajiwala, A.; Warang, A. Indocyanine green-mediated photothermal therapy in treatment of chronic periodontitis: A clinico-microbiological study. J. Indian Soc. Periodontol. 2018, 22, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Sethi, K.S.; Raut, C.P. Antimicrobial photodynamic therapy using indocyanine green as a photosensitizer in treatment of chronic periodontitis: A clinico-microbial study. Indian J. Dent. Res. 2019, 30, 870. [Google Scholar]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Graziani, F.; Gatto, R.; Monaco, A. Adjunctive photodynamic therapy to non-surgical treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, 514–526. [Google Scholar] [CrossRef]
- Bashir, N.Z.; Singh, H.A.; Virdee, S.S. Indocyanine green–mediated antimicrobial photodynamic therapy as an adjunct to periodontal therapy: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 5699–5710. [Google Scholar] [CrossRef]
- Nagahara, A.; Mitani, A.; Fukuda, M.; Yamamoto, H.; Tahara, K.; Morita, I.; Ting, C.C.; Watanabe, T.; Fujimura, T.; Osawa, K.; et al. Antimicrobial photodynamic therapy using a diode laser with a potential new photosensitizer, indocyanine green-loaded nanospheres, may be effective for the clearance of Porphyromonas gingivalis. J. Periodontal Res. 2013, 48, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Al-Zahrani, M.S.; Bamshmous, S.O.; Alhassani, A.A.; Al-Sherbini, M.M. Short-term effects of photodynamic therapy on periodontal status and glycemic control of patients with diabetes. J. Periodontol. 2009, 80, 1568–1573. [Google Scholar] [CrossRef]
- Macedo, G.D.; Novaes, A.B.; Souza, S.L.; Taba, M.; Palioto, D.B.; Grisi, M.F. Additional effects of aPDT on nonsurgical periodontal treatment with doxycycline in type II diabetes: A randomized, controlled clinical trial. Lasers Med. Sci. 2014, 29, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Ramos, U.D.; Ayub, L.G.; Reino, D.M.; Grisi, M.F.; Taba, M.; Souza, S.L.; Palioto, D.B.; Novaes, A.B. Antimicrobial photodynamic therapy as an alternative to systemic antibiotics: Results from a double-blind, randomized, placebo-controlled, clinical study on type 2 diabetics. J. Clin. Periodontol. 2015, 43, 147–155. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, N.C.; Andere, N.M.; Araujo, C.F.; de Marco, A.C.; dos Santos, L.M.; Jardini, M.A.; Santamaria, M.P. Local adjunct effect of antimicrobial photodynamic therapy for the treatment of chronic periodontitis in type 2 diabetics: Split-mouth double-blind randomized controlled clinical trial. Lasers Med. Sci. 2016, 22, 1–8. [Google Scholar]
- Monzavi, A.; Chinipardaz, Z.; Mousavi, M.; Fekrazad, R.; Moslemi, N.; Azaripour, A.; Bagherpasand, O.; Chiniforush, N. Antimicrobial photodynamic therapy using diode laser activated indocyanine green as an adjunct in the treatment of chronic periodontitis: A randomized clinical trial. Photodiagn. Photodyn. Ther. 2016, 14, 93–97. [Google Scholar] [CrossRef]
- Sukumar, K.; Tadepalli, A.; Parthasarathy, H.; Ponnaiyan, D. Evaluation of combined efficacy of photodynamic therapy using indocyanine green photosensitizer and non-surgical periodontal therapy on clinical and microbial parameters in the management of chronic periodontitis subjects: A randomized split-mouth design. Photodiagn. Photodyn. Ther. 2020, 31, 101949. [Google Scholar] [CrossRef]
- Boehm, T.K.; Ciancio, S.G. Diode laser activated indocyanine green selectively kills bacteria. J. Int. Acad. Periodontol. 2011, 13, 58–63. [Google Scholar]
- Srikanth, K.; Chandra, R.V.; Reddy, A.A.; Reddy, B.H.; Reddy, C.; Naveen, A. Effect of a single session of antimicrobial photodynamic therapy using indocyanine green in the treatment of chronic periodontitis: A randomized controlled pilot trial. Quintessence Int. 2015, 46, 391–400. [Google Scholar]
- You, Q.; Sun, Q.; Wang, J.; Tan, X.; Pang, X.; Liu, L.; Yu, M.; Tan, F.; Li, N. A single-light triggered and dual-imaging guided multifunctional platform for combined photothermal and photodynamic therapy based on TD-controlled and ICG-loaded CuS@mSiO2. Nanoscale 2017, 9, 3784–3796. [Google Scholar] [CrossRef]
- Vangipuram, P.; Ravishankar, P.L.; Saravanan, A.V.; Vaidya, J.; Visithiriyan, G.; Gurupasath, P. Indocyanine green-mediated photodynamic therapy as adjuvant to non-surgical periodontal treatment in chronic periodontitis patients: A clinical and microbiological study. Ann. RSCB 2021, 25, 363–371. [Google Scholar]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Jervøe-Storm, P.M.; Jepsen, S.; Worthington, H.V.; Needleman, I.; Eberhard, J. Adjunctive antimicrobial photodynamic therapy for treating periodontal and peri-implant diseases. Cochrane Database Syst. Rev. 2015, 6, CD011778. [Google Scholar] [CrossRef]
- Al-Momani, M.M. Indocyanine-mediated antimicrobial photodynamic therapy promotes superior clinical effects in stage III and grade C chronic periodontitis among controlled and uncontrolled diabetes mellitus: A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2021, 35, 102379. [Google Scholar] [CrossRef] [PubMed]
- Hill, G.; Dehn, C.; Hinze, A.V.; Frentzen, M.; Meister, J. Indocyanine green-based adjunctive antimicrobial photodynamic therapy for treating chronic periodontitis: A randomized clinical trial. Photodiagn. Photodyn. Ther. 2019, 26, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Shingnapurkar, S.H.; Mitra, D.K.; Kadav, M.S.; Shah, R.A.; Rodrigues, S.V.; Prithyani, S.S. The effect of indocyanine green-mediated photodynamic therapy as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A comparative split-mouth randomized clinical trial. Indian J. Dent. Res. 2016, 27, 609–617. [Google Scholar] [CrossRef]
- Bassir, S.H.; Moslemi, N.; Jamali, R.; Mashmouly, S.; Fekrazad, R.; Chiniforush, N.; Shamshiri, A.R.; Nowzari, H. Photoactivated disinfection using light-emitting diode as an adjunct in the management of chronic periodontitis: A pilot double-blind split-mouth randomized clinical trial. J. Clin. Periodontol. 2013, 40, 65–72. [Google Scholar] [CrossRef]
- Fekrazad, R.; Khoei, F.; Bahador, A.; Hakimiha, N. Photo-activated elimination of Aggregatibacter actinomycetemcomitans in planktonic culture: Comparison of photodynamic therapy versus photothermal therapy method. Photodiagn. Photodyn. Ther. 2017, 19, 28–32. [Google Scholar] [CrossRef]
- Chiang, C.P.; Hsieh, O.; Tai, W.C.; Chen, Y.J.; Chang, P.C. Clinical outcomes of adjunctive indocyanine green-diode lasers therapy for treating refractory periodontitis: A randomized controlled trial with in vitro assessment. J. Formos. Med. Assoc. 2020, 119, 652–659. [Google Scholar] [CrossRef]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.K.; Lee, S.G.; Choi, Y.H.; Won, J.S.; Merchant, A.T.; Lee, H.K. Association between diabetes-related factors and clinical periodontal parameters in type-2 diabetes mellitus. BMC Oral Health 2013, 13, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | SRP Group | SRP + aPDT Group | |
|---|---|---|---|
| Subjects number (n) | 25 | 24 | |
| Number of sites | 474 | 445 | |
| Age (years) (mean±standard deviation) | 55.24 ± 3.41 | 55.58 ± 3.62 | |
| Gender n (%) | Male | 14 (56.00%) | 13 (54.16%) |
| Female | 11 (44.00%) | 11 (45.84%) | |
| Parameter | SRP Group (n = 25) | SRP + aPDT Group (n = 24) | ||||
|---|---|---|---|---|---|---|
| Baselin * | +6 Month * | Δ # | Baselin * | +6 Months * | Δ # | |
| PI | 79.44 ± 6.31 | 17.72 ± 6.38 a | 62 (60–66) | 80.04 ± 5.90 | 17.08 ± 5.14 a | 63 (60–67) |
| BOP | 67.76 ± 6.57 | 8.08 ± 5.09 a | 60 (55–66) | 68.67 ± 6.10 | 4.21 ± 3.85 ab | 65 c (55–69) |
| PD (mm) | 5.54 ± 0.24 | 4.10 ± 0.22 a | 1.4 (1.4–1.5) | 5.53 ± 0.24 | 3.56 ± 0.19 ab | 1.9 c (1.8–2.2) |
| CAL (mm) | 4.51 ± 0.20 | 3.15 ± 0.17 a | 1.40 (1.20–1.50) | 4.50 ± 0.22 | 2.58 ± 0.19 ab | 1.95 c (1.70–2.10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sufaru, I.-G.; Martu, M.-A.; Luchian, I.; Stoleriu, S.; Diaconu-Popa, D.; Martu, C.; Teslaru, S.; Pasarin, L.; Solomon, S.M. The Effects of 810 nm Diode Laser and Indocyanine Green on Periodontal Parameters and HbA1c in Patients with Periodontitis and Type II Diabetes Mellitus: A Randomized Controlled Study. Diagnostics 2022, 12, 1614. https://doi.org/10.3390/diagnostics12071614
Sufaru I-G, Martu M-A, Luchian I, Stoleriu S, Diaconu-Popa D, Martu C, Teslaru S, Pasarin L, Solomon SM. The Effects of 810 nm Diode Laser and Indocyanine Green on Periodontal Parameters and HbA1c in Patients with Periodontitis and Type II Diabetes Mellitus: A Randomized Controlled Study. Diagnostics. 2022; 12(7):1614. https://doi.org/10.3390/diagnostics12071614
Chicago/Turabian StyleSufaru, Irina-Georgeta, Maria-Alexandra Martu, Ionut Luchian, Simona Stoleriu, Diana Diaconu-Popa, Cristian Martu, Silvia Teslaru, Liliana Pasarin, and Sorina Mihaela Solomon. 2022. "The Effects of 810 nm Diode Laser and Indocyanine Green on Periodontal Parameters and HbA1c in Patients with Periodontitis and Type II Diabetes Mellitus: A Randomized Controlled Study" Diagnostics 12, no. 7: 1614. https://doi.org/10.3390/diagnostics12071614
APA StyleSufaru, I. -G., Martu, M. -A., Luchian, I., Stoleriu, S., Diaconu-Popa, D., Martu, C., Teslaru, S., Pasarin, L., & Solomon, S. M. (2022). The Effects of 810 nm Diode Laser and Indocyanine Green on Periodontal Parameters and HbA1c in Patients with Periodontitis and Type II Diabetes Mellitus: A Randomized Controlled Study. Diagnostics, 12(7), 1614. https://doi.org/10.3390/diagnostics12071614