
Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA)

 , , , and
, , , and 
Abstract
:1. Introduction
Auto Machine Learning (AutoML)
- is the default pre-defined operation set;
- indicates the operations selected by the algorithms;
- represents the generator function for developing new features;
- N is the number of features selected;
- NM = maximum number of features to be chosen.
2. Materials and Method
2.1. Study Population
2.2. Workflow
2.3. Image Acquisition
2.4. Pre-Processing
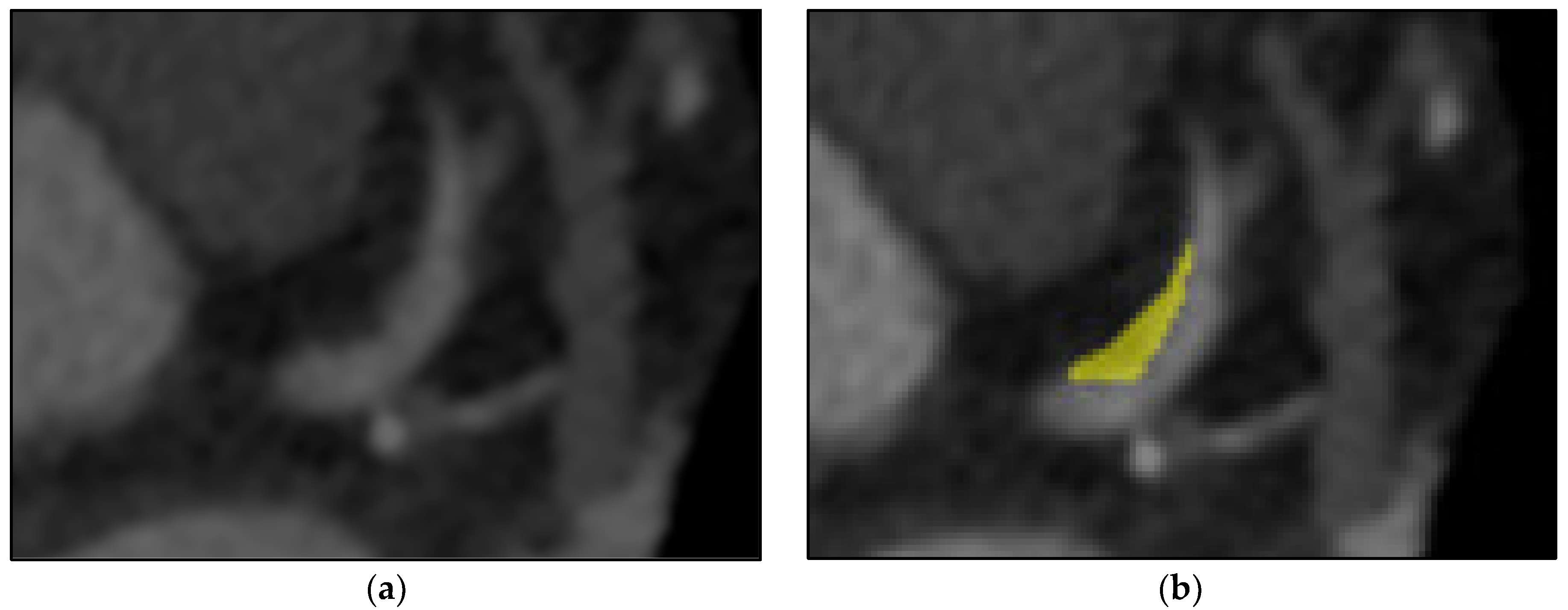
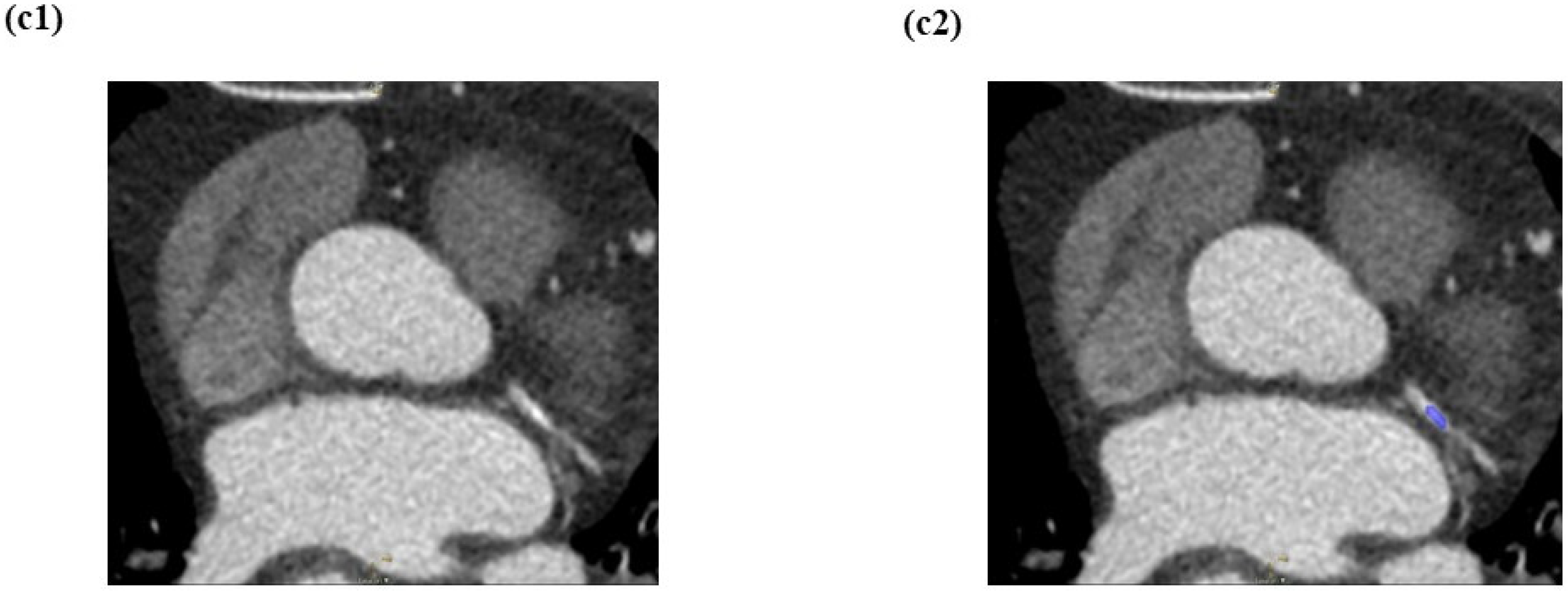
2.5. Segmentation Process
2.6. Feature Extraction Process
2.7. Tree-Based Pipeline Optimisation Tool (TPOT) Multiclass Classification of Atherosclerotic Plaques
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaptoge, S.; Pennells, L.; De Bacquer, D.; Cooney, M.T.; Kavousi, M.; Stevens, G.; Di Angelantonio, E. World Health Organization Cardiovascular Disease Risk Charts: Revised Models to Estimate Risk in 21 Global Regions. Lancet Glob. Health 2019, 7, e1332–e1345. [Google Scholar] [CrossRef] [Green Version]
- Plank, F. The Diagnostic and Prognostic Value of Coronary CT Angiography in Asymptomatic High-Risk Patients: A Cohort Study. Open Heart 2014, 1, e000096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahlgren, C.M.; Zheng, W.; Shaalan, W.; Tang, J.; Bassiouny, H.S. Human Carotid Plaque Calcification and Vulnerability. Relationship between Degree of Plaque Calcification, Fibrous Cap Inflammatory Gene Expression and Symptomatology. Cerebrovasc. Dis. 2009, 27, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Ito, H.; Sarai, M.; Kondo, T.; Kawai, H.; Nagahara, Y.; Harigaya, H.; Kan, S.; Anno, H.; Takahashi, H.; et al. Plaque Characterization by Coronary Computed Tomography Angiography and the Likelihood of Acute Coronary Events in Mid-Term Follow-Up. J. Am. Coll. Cardiol. 2015, 66, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic Performance of 64-Multidetector Row Coronary Computed Tomographic Angiography for Evaluation of Coronary Artery Stenosis in Individuals without Known Coronary Artery Disease. Results from the Prospective Multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) Trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Puchner, S.B.; Liu, T.; Mayrhofer, T.; Truong, Q.A.; Lee, H.; Fleg, J.L.; Nagurney, J.T.; Udelson, J.E.; Hoffmann, U.; Ferencik, M. High-Risk Plaque Detected on Coronary CT Angiography Predicts Acute Coronary Syndromes Independent of Significant Stenosis in Acute Chest Pain: Results from the ROMICAT-II Trial. J. Am. Coll. Cardiol. 2014, 64, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.L.; Hsu, W.Y.; Lee, M.H.; Weng, H.H.; Chang, S.W.; Yang, J.T.; Tsai, Y.H. Automatic Machine-Learning-Based Outcome Prediction in Patients with Primary Intracerebral Hemorrhage. Front. Neurol. 2019, 10, 910. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.C.; Moss, A.J.; Dweck, M.; Adamson, P.D.; Alam, S.; Hunter, A.; Shah, A.S.V.; Pawade, T.; Weir-McCall, J.R.; Roditi, G.; et al. Coronary Artery Plaque Characteristics Associated with Adverse Outcomes in the SCOT-HEART Study. J. Am. Coll. Cardiol. 2019, 73, 291–301. [Google Scholar] [CrossRef]
- Otsuka, K.; Fukuda, S.; Tanaka, A.; Nakanishi, K.; Taguchi, H.; Yoshikawa, J.; Shimada, K.; Yoshiyama, M. Napkin-Ring Sign on Coronary CT Angiography for the Prediction of Acute Coronary Syndrome. JACC Cardiovasc. Imaging 2013, 6, 448–457. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Ye, W.; Ou, J.; Li, X.; Tan, Z.; Li, T.; Liu, H. Coronary Computed Tomography Angiography Assessment of High-Risk Plaques in Predicting Acute Coronary Syndrome. Front. Cardiovasc. Med. 2021, 8, 743538. [Google Scholar] [CrossRef]
- Rybicki, F.J.; Udelson, J.E.; Peacock, W.F.; Goldhaber, S.Z.; Isselbacher, E.M.; Kazerooni, E.; Kontos, M.C.; Litt, H.; Woodard, P.K. Appropriate Utilization of Cardiovascular Imaging in Emergency Department Patients with Chest Pain: A Joint Document of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Appropriate Use Criteria Ta. J. Am. Coll. Cardiol. 2016, 67, 853–879. [Google Scholar] [CrossRef] [PubMed]
- Sabarudin, A.; Siong, T.W.; Chin, A.W.; Hoong, N.K.; Karim, M.K.A. A Comparison Study of Radiation Effective ose in ECG-Gated Coronary CT Angiography and Calcium Scoring Examinations Performed with a Dual-Source CT Scanner. Sci. Rep. 2019, 9, 4374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramjattan, N.A.; Lala, V.; Kousa, O.; Makaryus, A.N. Coronary CT Angiography; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lefere, P. Teleradiology Based CT Colonography to Screen a Population Group of a Remote Island; at Average Risk for Colorectal Cancer. Eur. J. Radiol. 2013, 82, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R. Automated Diagnosis of Focal Liver Lesions Using Bidirectional Empirical Mode Decomposition Features. Comput. Biol. Med. 2018, 94, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, A.M.; Hamimi, A.H.; Matta, J.R.; Carass, A.; Elgarf, R.M.; Gharib, A.M.; Abd-Elmoniem, K.Z. Automatic Coronary Wall and Atherosclerotic Plaque Segmentation from 3D Coronary CT Angiography. Sci. Rep. 2019, 9, 47. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; Van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Haniff, N.S.M.; Karim, M.K.A.; Osman, N.H.; Saripan, M.I.; Isa, I.N.C.; Ibahim, M.J. Stability and Reproducibility of Radiomic Features Based Various Segmentation Technique on MR Images of Hepatocellular Carcinoma (HCC). Diagnostics 2021, 11, 1573. [Google Scholar] [CrossRef]
- Mat Radzi, S.F.; Abdul Karim, M.K.; Saripan, M.I.; Abd Rahman, M.A.; Osman, N.H.; Dalah, E.Z.; Mohd Noor, N. Impact of Image Contrast Enhancement on Stability of Radiomics Feature Quantification on a 2D Mammogram Radiograph. IEEE Access 2020, 8, 127720–127731. [Google Scholar] [CrossRef]
- Mohd Yunus, M.; Hui Sin, N.; Sabarudin, A.; Abdul Karim, M.K.; Ar, R.; Mohd Shamsul, M.S. Comparative Study of the Manual and Semi- Automated Segmentation Technique in Computed Tomography (CT) Lung Cancer: A Radiomics Study. J. Med. Health 2021, 16, 1–62. [Google Scholar]
- Koçak, B.; Durmaz, E.Ş.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with Artificial Intelligence: A Practical Guide for Beginners. Diagn. Interv. Radiol. 2019, 25, 485–495. [Google Scholar] [CrossRef]
- Acharya, U.R.; Hagiwara, Y.; Sudarshan, V.K.; Chan, W.Y.; Ng, K.H. Towards Precision Medicine: From Quantitative Imaging to Radiomics. J. Zhejiang Univ. B 2018, 19, 6–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Hu, X.; Tao, X.; Shi, X.; Zhou, W.; Hu, H.; Hu, X. Radiomic Features of Plaques Derived from Coronary CT Angiography to Identify Hemodynamically Significant Coronary Stenosis, Using Invasive FFR as the Reference Standard. Eur. J. Radiol. 2021, 140, 109769. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Dey, D.; Slomka, P.J.; Arsanjani, R.; Nakazato, R.; Ko, H.; Berman, D.S.; Li, D.; Kuo, C.-C.J. Structured Learning Algorithm for Detection of Nonobstructive and Obstructive Coronary Plaque Lesions from Computed Tomography Angiography. J. Med. Imaging 2015, 2, 014003. [Google Scholar] [CrossRef]
- Freiman, M.; Manjeshwar, R.; Goshen, L. Unsupervised Abnormality Detection through Mixed Structure Regularization (MSR) in Deep Sparse Autoencoders. Med. Phys. 2019, 46, 2223–2231. [Google Scholar] [CrossRef] [Green Version]
- Choi, A.D.; Marques, H.; Kumar, V.; Griffin, W.F.; Rahban, H.; Karlsberg, R.P.; Zeman, R.K.; Katz, R.J.; Earls, J.P. CT EvaLuation by ARtificial Intelligence for Atherosclerosis, Stenosis and Vascular MorphologY (CLARIFY): A Multi-Center, International Study. J. Cardiovasc. Comput. Tomogr. 2021, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Griffin, W.F.; Choi, A.D.; Riess, J.S.; Marques, H.; Chang, H.-J.; Choi, J.H.; Doh, J.-H.; Her, A.-Y.; Koo, B.-K.; Nam, C.-W.; et al. AI Evaluation of Stenosis on Coronary CT Angiography, Comparison With Quantitative Coronary Angiography and Fractional Flow Reserve. JACC Cardiovasc. Imaging 2022. [Google Scholar] [CrossRef]
- Jordan, M.I.; Mitchell, T.M. Machine Learning: Trends, Perspectives, and Prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Yunus, M.M.; Sabarudin, A.; Hamid, N.I.; Yusof, A.K.M.; Nohuddin, P.N.E.; Karim, M.K.A. Automated Classification of Atherosclerosis in Coronary Computed Tomography Angiography Images Based on Radiomics Study Using Automatic Machine Learning. In Proceedings of the 2022 International Conference on Electronics and Renewable Systems (ICEARS), Tuticorin, India, 16–18 March 2022; pp. 1895–1903. [Google Scholar] [CrossRef]
- Izdihar, K.; Karim, M.K.A.; Aresli, N.N.; Radzi, S.F.M.; Sabarudin, A.; Yunus, M.M.; Rahman, M.A.A.; Shamsul, S. Detection of Novel Coronavirus from Chest X-Ray Radiograph Images via Automated Machine Learning and CAD4COVID. In Proceedings of the 2021 International Congress of Advanced Technology and Engineering (ICOTEN), Taiz, Yemen, 4–5 July 2021; pp. 1–4. [Google Scholar] [CrossRef]
- Radzi, S.F.M.; Karim, M.K.A.; Saripan, M.I.; Rahman, M.A.A.; Isa, I.N.C.; Ibahim, M.J. Hyperparameter Tuning and Pipeline Optimization via Grid Search Method and Tree-Based AutoML in Breast Cancer Prediction. J. Pers. Med. 2021, 11, 978. [Google Scholar] [CrossRef]
- Thornton, C.; Hutter, F.; Hoos, H.H.; Leyton-Brown, K. Auto-WEKA: Combined Selection and Hyperparameter Optimization of Classification Algorithms. In Proceedings of the ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Chicago, IL, USA, 11–14 August 2013; pp. 847–855. [Google Scholar]
- Olson, R.S.; Bartley, N.; Urbanowicz, R.J.; Moore, J.H. Evaluation of a Tree-Based Pipeline Optimization Tool for Automating Data Science. In Proceedings of the GECCO 2016—Proceedings of the 2016 Genetic and Evolutionary Computation Conference, New York, NY, USA, 24 July 2016; pp. 485–492. [Google Scholar]
- Feurer, M.; Klein, A.; Jost, K.E.; Springenberg, T.; Blum, M.; Hutter, F. Efficient and Robust Automated Machine Learning. In Advances in Neural Information Processing Systems; The MIT Press: Cambridge, MA, USA, 2015; Volume 28, pp. 1–9. [Google Scholar]
- Singh, G.; Al’Aref, S.J.; Van Assen, M.; Kim, T.S.; van Rosendael, A.; Kolli, K.K.; Dwivedi, A.; Maliakal, G.; Pandey, M.; Wang, J.; et al. Machine Learning in Cardiac CT: Basic Concepts and Contemporary Data. J. Cardiovasc. Comput. Tomogr. 2018, 12, 192–201. [Google Scholar] [CrossRef]
- Dafflon, J. An Automated Machine Learning Approach to Predict Brain Age from Cortical Anatomical Measures. Hum. Brain Mapp. 2020, 41, 3555–3566. [Google Scholar] [CrossRef]
- Orlenko, A.; Kofink, D.; Lyytikäinen, L.P.; Nikus, K.; Mishra, P.; Kuukasjärvi, P.; Karhunen, P.J.; Kähönen, M.; Laurikka, J.O.; Lehtimäki, T.; et al. Model Selection for Metabolomics: Predicting Diagnosis of Coronary Artery Disease Using Automated Machine Learning. Bioinformatics 2020, 36, 1772–1778. [Google Scholar] [CrossRef] [PubMed]
- Waring, J.; Lindvall, C.; Umeton, R. Automated Machine Learning: Review of the State-of-the-Art and Opportunities for Healthcare. Artif. Intell. Med. 2020, 104, 101822. [Google Scholar] [CrossRef] [PubMed]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, T.T.; Fu, W.; Moore, J.H. Scaling Tree-Based Automated Machine Learning to Biomedical Big Data with a Feature Set Selector. Bioinformatics 2020, 36, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halevy, A.; Norvig, P.; Pereira, F. The Unreasonable Effectiveness of Data. IEEE Intell. Syst. 2009, 24, 8–12. [Google Scholar] [CrossRef]
- Rahmat, S.M.S.S. Effect of Miscentering and Low-Dose Protocols on Contrast Resolution in Computed Tomography Head Examination. Comput. Biol. Med. 2020, 123, 103840. [Google Scholar] [CrossRef]
- Harun, H.H. Task-Based Assessment on Various Optimization Protocols of Computed Tomography Pulmonary Angiography Examination. Radiat. Phys. Chem. 2021, 188, 109692. [Google Scholar] [CrossRef]
- Pednekar, G.V.; Udupa, J.K.; McLaughlin, D.J.; Wu, X.; Tong, Y.; Simone, C.B., II; Camaratta, J.; Torigian, D.A. Image Quality and Segmentation. Proc. SPIE Int. Soc. Opt. Eng. 2018, 10576, 85. [Google Scholar] [CrossRef]
- Zhang, Y.; Oikonomou, A.; Wong, A.; Haider, M.A.; Khalvati, F. Radiomics-Based Prognosis Analysis for Non-Small Cell Lung Cancer. Sci. Rep. 2017, 7, 46349. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.B. The Study of Automatic Machine Learning Base on Radiomics of Non-Focus Area in the First Chest CT of Different Clinical Types of COVID-19 Pneumonia. Sci. Rep. 2020, 10, 18926. [Google Scholar] [CrossRef]
- Hossin, M.; Sulaiman, M.N. A Review on Evaluation Metrics for Data Classification Evaluations. Int. J. Data Min. Knowl. Manag. Process. 2015, 5, 1–11. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumberger, J.A.; Simons, D.B.; Fitzpatrick, L.A.; Sheedy, P.F.; Schwartz, R.S. Coronary Artery Calcium Area by Electron-Beam Computed Tomography and Coronary Atherosclerotic Plaque Area. Circulation 1995, 92, 2157–2162. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Xue, Y.; Schoepf, U.J.; Varga-Szemes, A.; Griffith, J.; Yacoub, B.; Zhou, F.; Zhou, C.; Yang, Y.; Xing, W.; et al. Radiomics: The Next Frontier of Cardiac Computed Tomography. Circ. Cardiovasc. Imaging 2021, 14, 256–264. [Google Scholar] [CrossRef]
- Kolossváry, M.; Karády, J.; Szilveszter, B.; Kitslaar, P.; Hoffmann, U.; Merkely, B.; Maurovich-Horvat, P. Radiomic Features Are Superior to Conventional Quantitative Computed Tomographic Metrics to Identify Coronary Plaques with Napkin-Ring Sign. Circ. Cardiovasc. Imaging 2017, 10, e006843. [Google Scholar] [CrossRef]
- Wei, J.; Zhou, C.; Chan, H.P.; Chughtai, A.; Agarwal, P.; Kuriakose, J.; Hadjiiski, L.; Patel, S.; Kazerooni, E. Computerized Detection of Noncalcified Plaques in Coronary CT Angiography: Evaluation of Topological Soft Gradient Prescreening Method and Luminal Analysis. Med. Phys. 2014, 41, 081901. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The Facts and the Challenges of Image Analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef]
- Cheng, K.; Lin, A.; Yuvaraj, J.; Nicholls, S.J.; Wong, D.T.L. Cardiac Computed Tomography Radiomics for the Non-Invasive Assessment of Coronary Inflammation. Cells 2021, 10, 879. [Google Scholar] [CrossRef]
- Kolossváry, M.; Karády, J.; Kikuchi, Y.; Ivanov, A.; Schlett, C.L.; Lu, M.T.; Foldyna, B.; Merkely, B.; Aerts, H.J.; Hoffmann, U.; et al. Radiomics versus Visual and Histogram-Based Assessment to Identify Atheromatous Lesions at Coronary CT Angiography: An Ex Vivo Study. Radiology 2019, 293, 89–96. [Google Scholar] [CrossRef]
- Mackin, D. Measuring Computed Tomography Scanner Variability of Radiomics Features. Investig. Radiol. 2015, 50, 757–765. [Google Scholar] [CrossRef]
- Shiri, I.; Rahmim, A.; Ghaffarian, P.; Geramifar, P.; Abdollahi, H.; Bitarafan-Rajabi, A. The Impact of Image Reconstruction Settings on 18F-FDG PET Radiomic Features: Multi-Scanner Phantom and Patient Studies. Eur. Radiol. 2017, 27, 4498–4509. [Google Scholar] [CrossRef] [PubMed]
- Altazi, B.A. Reproducibility of F18-FDG PET Radiomic Features for Different Cervical Tumor Segmentation Methods, Gray-Level Discretization, and Reconstruction Algorithms. J. Appl. Clin. Med. Phys. 2017, 18, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Haniff, N.S.M.; Karim, M.K.B.A.; Ali, N.S.; Rahman, M.A.A.; Osman, N.H.; Saripan, M.I. Magnetic Resonance Imaging Radiomics Analysis for Predicting Hepatocellular Carcinoma. In Proceedings of the 2021 International Congress of Advanced Technology and Engineering (ICOTEN), Makkah, Saudi Arabia, 4–5 July 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Eng, D.; Chute, C.; Khandwala, N.; Rajpurkar, P.; Long, J.; Shleifer, S.; Khalaf, M.H.; Sandhu, A.T.; Rodriguez, F.; Maron, D.J.; et al. Automated Coronary Calcium Scoring Using Deep Learning with Multicenter External Validation. NPJ Digit. Med. 2021, 4, 88. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 202) |
|---|---|
| Patients’ Demographic Characteristics | |
| Gender | |
| Male, n (%) | 138 (68.3%) |
| Female, n (%) | 64 (31.7%) |
| Ethnicity | |
| Malay, n (%) | 104 (51.5%) |
| Chinese, n (%) | 46 (22.8%) |
| Indian, n (%) | 51 (25.2%) |
| Others, n (%) | 1 (0.5%) |
| Age (years ± SD) | 58.84 ± 9.497 |
| Body Mass Index (kg/m2 ± SD) | 26.81 ± 3.746 |
| Patients’ Distribution based on CAD-RADS | |
| CAD-RADS 0, n (%) | 6 (3.0%) |
| CAD-RADS 1, n (%) | 9 (4.5%) |
| CAD-RADS 2, n (%) | 54 (26.7%) |
| CAD-RADS 3, n (%) | 36 (17.8%) |
| CAD-RADS 4, n (%) | 95 (47.0%) |
| CAD-RADS 5, n (%) | 2 (1.0%) |
| Image Acquisition Characteristics | |
| Total DLP (mGy × cm ± SD) | 322.00 ± 167.926 |
| Heart rate (bpm ± SD) | 70.20 ± 10.522 |
| Contrast medium (mL ± SD) | 59.57 ± 2.347 |
| First Order Features (n = 29) | Second Order Features (n = 31) | Shape Order Features (n = 5) |
|---|---|---|
| Conventional: CONVENTIONAL_min CONVENTIONAL_mean CONVENTIONAL_std CONVENTIONAL_max CONVENTIONAL_Q1 CONVENTIONAL_Q2 CONVENTIONAL_Q3 CONVENTIONAL_Skewness CONVENTIONAL_Kurtosis CONVENTIONAL_Excess_Kurtosis CONVENTIONAL_peak_Sphere_0.5mL CONVENTIONAL_peak_Sphere_1mL CONVENTIONAL_calcium_AgatstonScore Discretized: DISCRETIZED_min DISCRETIZED_mean DISCRETIZED_std DISCRETIZED_max DISCRETIZED_Q1 DISCRETIZED_Q2 DISCRETIZED_Q3 DISCRETIZED_Skewness DISCRETIZED_Kurtosis DISCRETIZED_ExcessKurtosis DISCRETIZED_peakSphere0.5 mL DISCRETIZED_peakSphere1 mL DISCRETIZED_HISTO_Entropy_log10 DISCRETIZED_HISTO_Entropy_log2 DISCRETIZED_HISTO_Energy DISCRETIZED_AUC_CSH | Gray Level Co-Occurrence Matrix (GLCM): GLCM_Homogeneity GLCM_Energy GLCM_Contrast GLCM_Correlation GLCM_Entropy_log10 GLCM_Entropy_log2 GLCM_Dissimilarity Gray Level Run length Matrix (GLRLM): GLRLM_ Short Run Emphasis (SRE) GLRLM_Long Run Emphasis (LRE) GLRLM_Low Gray Run Emphasis (LGRE) GLRLM_High Gray Run Emphasis (HGRE) GLRLM__ Short Run Low Gray level Emphasis (SRLGE) GLRLM_ Short Run High Gray level Emphasis (SRHGE) GLRLM_Long Run Low Gray Level Emphasis (LRLGE) GLRLM_ Long Run High Gray Level Emphasis (LRHGE) GLRLM_GLNU (Gray-Level Non-Uniformity) GLRLM_Run-Length Non-Uniformity (RLNU) GLRLM_Run Percentage (RP) Neighborhood Grey-Level Differences Matrix (NGLDM): NGLDM_Coarseness NGLDM_Contrast NGLDM_Busyness Grey Level Zone Length Matrix (GLZLM): GLZLM_Short Zone Emphasis (SZE) GLZLM_Long Zone Emphasis (LZE) GLZLM_Low Grey-level Zone Emphasis (LGZE) GLZLM_ High Grey-level Zone Emphasis (HGZE) GLZLM_Short Zone High Grey-level Emphasize (SZHGE) GLZLM_ Long Zone Low Grey-level Emphasize (LZLGE) GLZLM_ Long Zone High Grey-level Emphasize (LZHGE) GLZLM_Gray-Level Non-Uniformity (GLNU) GLZLM_Zone-Length Non-Uniformity (ZLNU) GLZLM_Zone Percentage (ZP) | Shape Features: SHAPE Volume(mL) SHAPE_Volume(vx) SHAPE_Sphericity SHAPE_Surface(mm2) SHAPE_Compacity |
| Atherosclerotic Plaques (Output) | ML Model | Recall (Sensitivity) | Precision (PPV) | F1- Score | Inverse Recall (Specificity) | Inverse Precision (NPV) | Inverse F1- Score | Accuracy |
|---|---|---|---|---|---|---|---|---|
| 1 | 0.97 | 0.80 | 0.88 * | 0.90 | 0.99 | 0.94 * | 0.92 * | |
| Normal | 2 | 0.83 | 0.73 | 0.77 | 0.88 | 0.93 | 0.90 | 0.86 |
| 3 | 0.24 | 0.33 | 0.28 | 0.79 | 0.70 | 0.74 | 0.62 | |
| 4 | 1.00 | 0.72 | 0.84 | 0.85 | 1.00 | 0.92 | 0.89 | |
| 1 | 0.71 | 0.86 | 0.78 * | 0.95 | 0.87 | 0.91 * | 0.87 * | |
| Calcified | 2 | 0.66 | 0.82 | 0.73 | 0.93 | 0.85 | 0.89 | 0.84 |
| 3 | 0.63 | 0.59 | 0.61 | 0.71 | 0.74 | 0.72 | 0.68 | |
| 4 | 0.74 | 0.74 | 0.74 | 0.88 | 0.88 | 0.88 | 0.83 | |
| 1 | 0.53 | 0.67 | 0.59 | 0.94 | 0.90 | 0.92 * | 0.87 * | |
| Non-calcified | 2 | 0.58 | 0.69 | 0.63 * | 0.94 | 0.91 | 0.92 * | 0.87 * |
| 3 | 0.16 | 0.75 | 0.26 | 0.98 | 0.78 | 0.87 | 0.78 | |
| 4 | 0.37 | 0.78 | 0.50 | 0.98 | 0.87 | 0.92 * | 0.87 * | |
| 1 | 0.79 | 0.72 | 0.76 * | 0.84 | 0.89 | 0.86 * | 0.82 * | |
| Mixed | 2 | 0.79 | 0.69 | 0.74 | 0.81 | 0.88 | 0.84 | 0.80 |
| 3 | 0.69 | 0.45 | 0.55 | 0.49 | 0.73 | 0.59 | 0.57 | |
| 4 | 0.72 | 0.74 | 0.73 | 0.86 | 0.85 | 0.85 | 0.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yunus, M.M.; Mohamed Yusof, A.K.; Ab Rahman, M.Z.; Koh, X.J.; Sabarudin, A.; Nohuddin, P.N.E.; Ng, K.H.; Kechik, M.M.A.; Karim, M.K.A. Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA). Diagnostics 2022, 12, 1660. https://doi.org/10.3390/diagnostics12071660
Yunus MM, Mohamed Yusof AK, Ab Rahman MZ, Koh XJ, Sabarudin A, Nohuddin PNE, Ng KH, Kechik MMA, Karim MKA. Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA). Diagnostics. 2022; 12(7):1660. https://doi.org/10.3390/diagnostics12071660
Chicago/Turabian StyleYunus, Mardhiyati Mohd, Ahmad Khairuddin Mohamed Yusof, Muhd Zaidi Ab Rahman, Xue Jing Koh, Akmal Sabarudin, Puteri N. E. Nohuddin, Kwan Hoong Ng, Mohd Mustafa Awang Kechik, and Muhammad Khalis Abdul Karim. 2022. "Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA)" Diagnostics 12, no. 7: 1660. https://doi.org/10.3390/diagnostics12071660
APA StyleYunus, M. M., Mohamed Yusof, A. K., Ab Rahman, M. Z., Koh, X. J., Sabarudin, A., Nohuddin, P. N. E., Ng, K. H., Kechik, M. M. A., & Karim, M. K. A. (2022). Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA). Diagnostics, 12(7), 1660. https://doi.org/10.3390/diagnostics12071660