
Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives


 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Article Identification
2.2. Article Selection
- Be original research articles published in a peer-reviewed journal with full-text access offered by the University of Bologna;
- Involve the use of any kind of MR images;
- Be published in English;
- Be concerned with the application of CNN deep learning techniques for brain tumor classification.
- Review articles;
- Book or book chapters;
- Conference papers or abstracts;
- Short communications or case reports;
- Unclear descriptions of data;
- No validation performed.
3. Literature Review
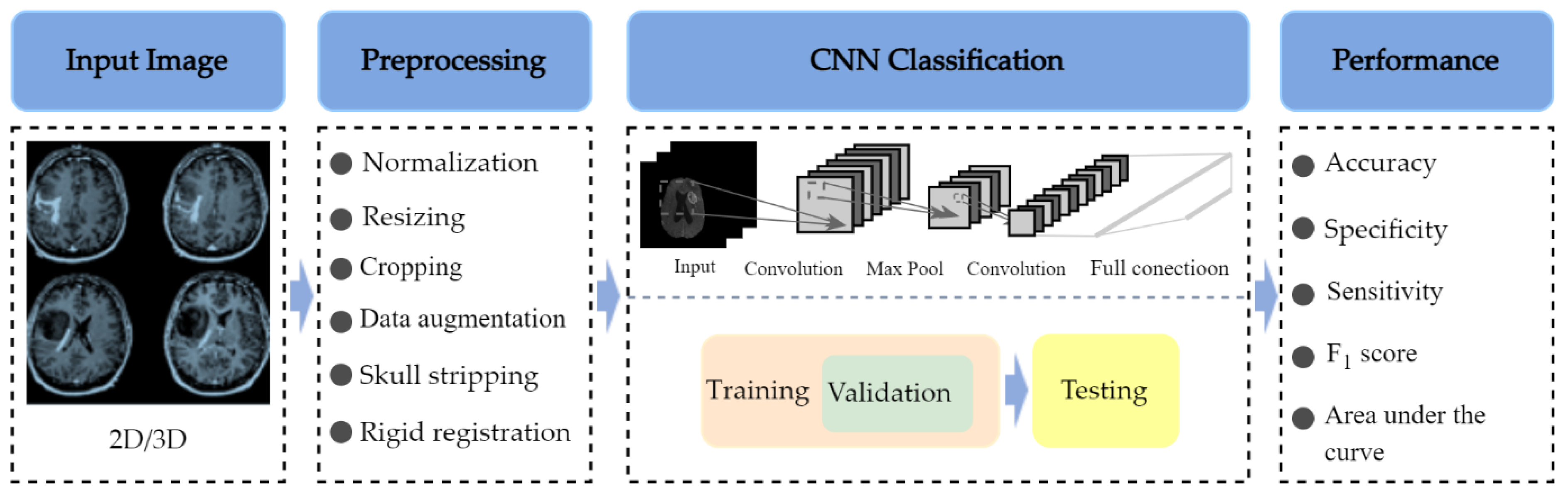
3.1. Basic Architecture of CNN-Based Methods
3.2. Datasets

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset Name | Available Sequences | Size | Classes | Unbiased Gini Coefficient | Source |
|---|---|---|---|---|---|
| TCGA-GBM | T1w, ceT1w, T2w, FLAIR | 199 patients | N/D | N/D | [53] |
| TCGA-LGG | T1w, ceT1ce, T2w, FLAIR | 299 patients | N/D | N/D | [54] |
| Brain tumor dataset from Figshare (Cheng et al., 2017) | ceT1w | 233 patients (82 MEN, 89 Glioma, 62 PT), 3064 images (708 MEN, 1426 Glioma, 930 PT) | Patients (82 MEN, 89 Glioma, 62 PT), images (708 MEN, 1426 Glioma, 930 PT) | 0.116 (patients), 0.234 (images) | [55] |
| Kaggle (Navoneel et al., 2019) | No information given | 253 images (98 normal, 155 tumorous) | 98 normal, 155 tumorous | 0.225 | [56] |
| REMBRANDT | T1w, T2w, FLAIR, DWI | 112 patients (30 AST-II, 17 AST-II, 14 OLI-II, 7 OLI-III, 44 GBM) | 30 AST-II, 17 AST-II, 14 OLI-II, 7 OLI-III, 44 GBM | 0.402 | [57] |
| BraTS | T1w, ceT1w, T2w, FLAIR | 2019: 335 patients (259 HGG, 76 LGG); 2018: 284 patients (209 HGG, 75 LGG); 2017: 285 patients (210 HGG, 75 LGG); 2015: 274 patients (220 HGG, 54 LGG) | 2019: 259 HGG, 76 LGG;2018: 209 HGG, 75 LGG;2017: 210 HGG, 75 LGG; 2015: 220 HGG, 54 LGG | 0.546 (2019); 0.472 (2018); 0.474 (2017); 0.606 (2015) | [58] |
| ClinicalTrials.gov (Liu et al., 2017) | T1w, ceT1w, T2w, FLAIR | 113 patients (52 LGG, 61 HGG) | 52 LGG, 61 HGG | 0.080 | [59] |
| CPM-RadPath 2019 | T1w, ceT1w, T2w, FLAIR | 329 patients | N/D | N/D | [60] |
| IXI dataset | T1w, T2w, DWI | 600 normal images | N/D | N/D | [61] |
| RIDER | T1w, T2w, DCE-MRI, ce-FLAIR | 19 GBM patients (70,220 images) | 70,220 images | N/D | [62] |
| Harvard Medical School Data | T2w | 42 patients (2 normal, 40 tumor), 540 images (27 normal, 513 tumorous) | Patients (2 normal, 40 tumorous), images (27 normal, 513 tumorous) | 0.905 (patients), 0.900 (images) | [63] |
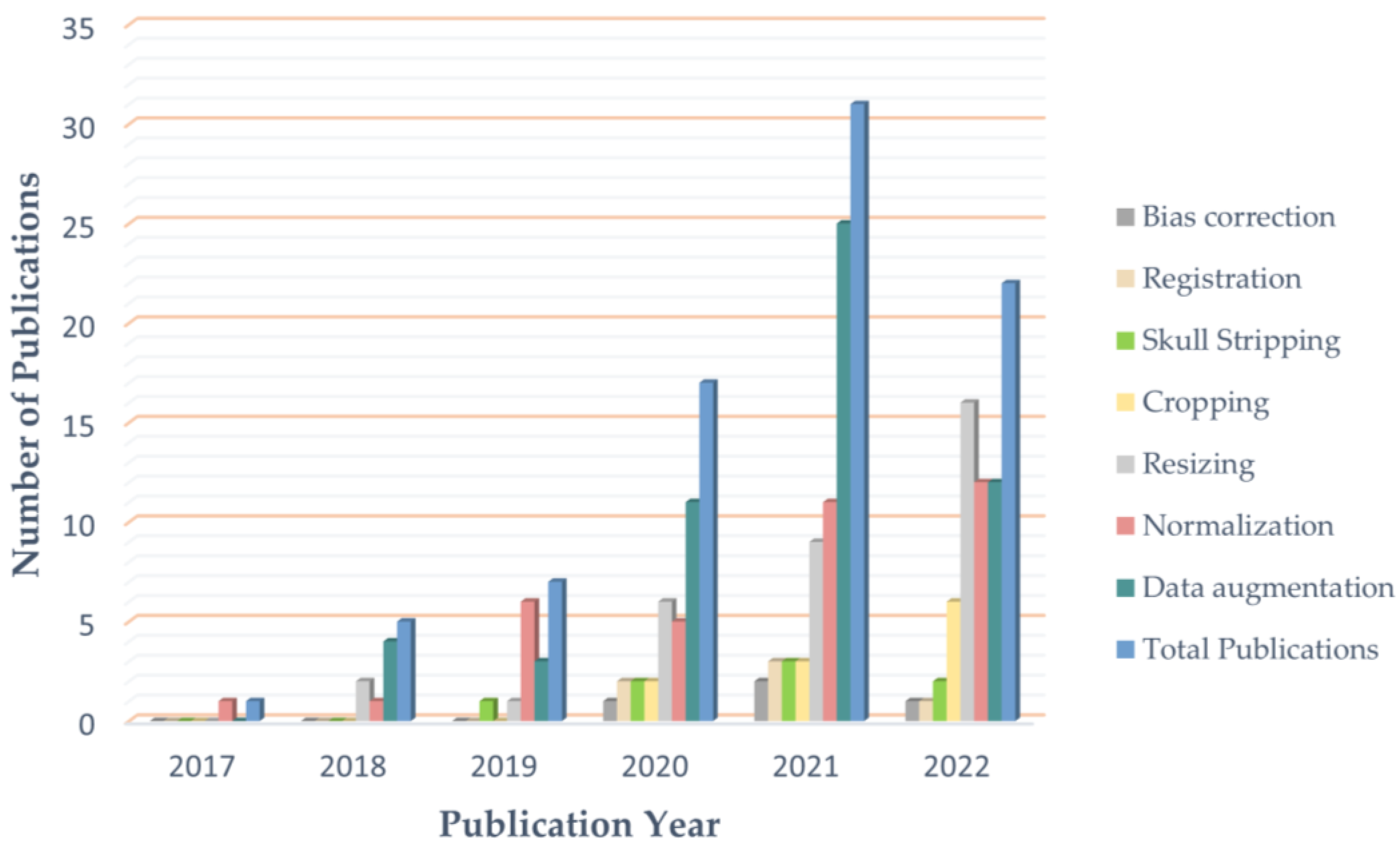
3.3. Preprocessing
3.3.1. Normalization
3.3.2. Skull Stripping
3.3.3. Resizing
3.3.4. Image Registration
3.3.5. Bias Field Correction
3.4. Data Augmentation
3.5. Performance Measures
3.5.1. Accuracy
3.5.2. Specificity
3.5.3. Precision
3.5.4. Sensitivity
3.5.5. F1 Score
3.5.6. Area under the Curve
4. Results
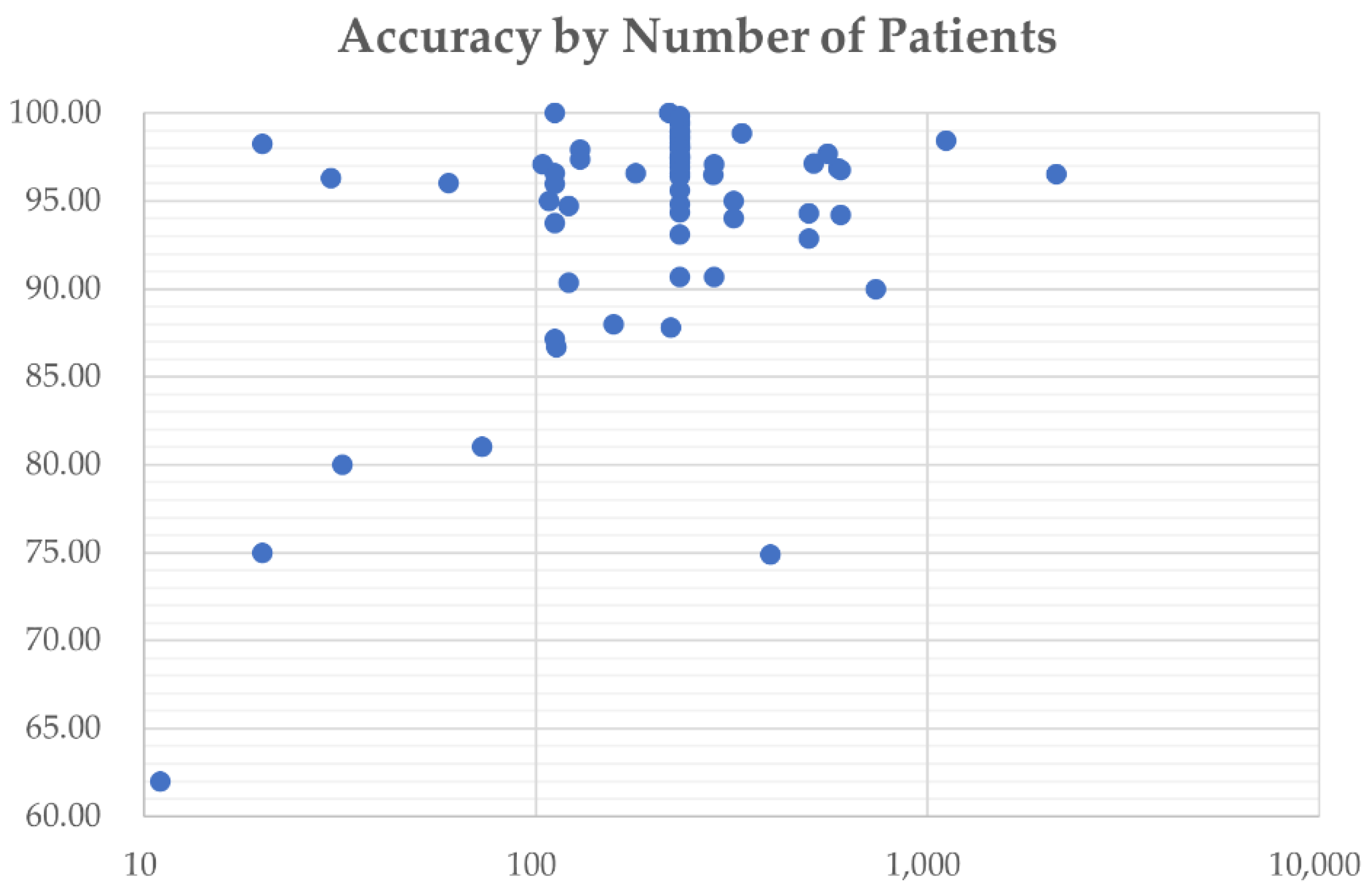
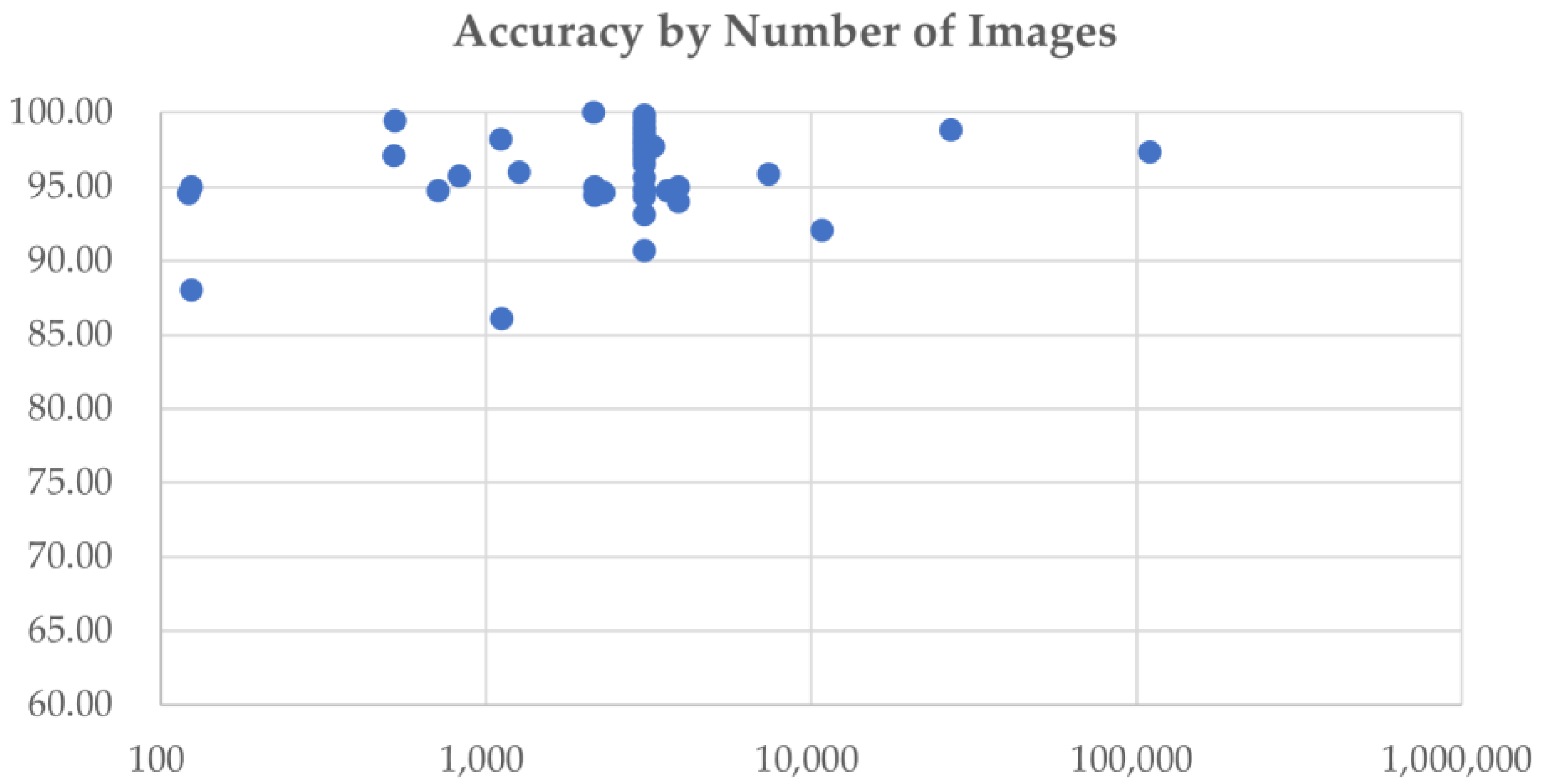
4.1. Quantitative Analysis
4.2. Clinical Applicability Degrading Factors
4.2.1. Data Quality
4.2.2. Data Scarcity
4.2.3. Data Mismatch
4.2.4. Class Imbalance
4.2.5. Research Value towards Clinical Needs
4.2.6. Classification Performance
4.2.7. Black-Box Characteristics of CNN Models
4.3. Overview of Included Studies
| (a) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author and Year | Datasets | MRI Sequences | Size of Dataset | Pre-Processing | Data Augmentation | ||||||||||||
| Patients | Images | Cropping | Normalization | Resizing | Skull Stripping | Registration 1 | Other | Translation 2 | Rotation | Scaling 3 | Reflection 4 | Shearing | Cropping | Other (X = Unspecified) | |||
| Özcan et al. [27] 2021 | Private dataset | T2w/FLAIR | 104 (50 LGG, 54 HGG) | 518 | x | x | Conversion to BMP | x | x | x | x | ||||||
| Hao et al. [102] 2021 | BraTS 2019 | T1w, ceT1w, T2w | 335 (259 HGG, 76 LGG) | 6700 | x | x | x | ||||||||||
| Tripathi et al. [103] 2021 | 1. TCGA-GBM, 2. LGG-1p19qDeletion | T2w | 322 (163 HGG, 159 LGG) | 7392 (5088 LGG, 2304 HGG) | x | x | x | x | x | x | |||||||
| Ge et al. [40] 2020 | BraTS 2017 | T1w, ceT1w, T2w, FLAIR | 285 (210 HGG, 75 LGG) | x | x | ||||||||||||
| Mzoughi et al. [28] 2020 | BraTS 2018 | ceT1w | 284 (209 HGG, 75 LGG) | x | x | Contrast enhancement | x | ||||||||||
| Yang et al. [45] 2018 | ClinicalTrials.gov (NCT026226201) | ceT1w | 113 (52 LGG, 61 HGG) | Conversion to BMP | x | x | x | Histogram equalization, adding noise | |||||||||
| Zhuge et al. [77] 2020 | 1.TCIA-LGG, 2. BraTS 2018 | T1w, T2w, FLAIR, ceT1w | 315 (210 HGG, 105 LGG) | x | x | Clipping, bias field correction | x | x | x | ||||||||
| Decuyper et al. [73] 2021 | 1. TCGA-LGG, 2. TCGA-GBM, 3. TCGA-1p19qDeletion, 4. BraTS 2019. 5. GUH dataset | T1w, ceT1w, T2w, FLAIR | 738 (164 from TCGA-GBM, 121 from TCGA-LGG, 141 from 1p19qDeletion, 202 from BraTS 2019, 110 from GUH dataset) (398 GBM vs. 340 LGG) | x | x | x | Interpolation | x | x | Elastic transform | |||||||
| He et al. [78] 2021 | 1.Dataset from TCIA | FLAIR, ceT1w | 214 (106 HGG, 108 LGG) | x | x | x | x | ||||||||||
| 2. BraTS 2017 | FLAIR, ceT1w | 285 (210 HGG, 75 LGG) | x | x | x | x | |||||||||||
| Hamdaoui et al. [104] 2021 | BraTS 2019 | T1w, ceT1w, T2w, FLAIR | 285 (210 HGG, 75 LGG) | 53,064 (26,532 HGG, 26,532 LGG) | x | x | x | ||||||||||
| Chikhalikar et al. [105] 2021 | BraTS 2015 | T2w, FLAIR | 274 (220 HGG, 54 LGG) | 521 | Contrast enhancement | ||||||||||||
| Ahmad [106] 2019 | BraTS 2015 | No info shared | 124 (99 HGG, 25 LGG) | x | |||||||||||||
| Naser et al. [96] 2020 | TCGA-LGG | T1W, FLAIR, ceT1w | 108 (50 Grade II, 58 Grade III) | x | x | x | Padding | x | x | x | x | x | |||||
| Allah et al. [44] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | PGGAN | |||||||||
| Swati et al. [50] 2019 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | |||||||||||
| Guan et al. [43] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | Contrast enhancement | x | x | ||||||||
| Deepak et al. [39] 2019 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | |||||||||||
| Díaz-Pernas et al. [42] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | Elastic transform | |||||||||||
| Ismael et al. [49] 2020 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | x | x | x | x | Whitening, brightness manipulation | |||||
| Alhassan et al. [107] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | ||||||||||||
| Bulla et al. [108] 2020 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | |||||||||||
| Ghassemi et al. [109] 2020 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | ||||||||||
| Kakarla et al. [110] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | Contrast enhancement | ||||||||||
| Noreen et al. [111] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | ||||||||||||
| Noreen et al. [112] 2020 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | ||||||||||||
| Kumar et al. [113] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | ||||||||||||
| Badža et al. [114] 2020 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | x | |||||||||
| Alaraimi et al. [115] 2021 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | x | x | x | x | ||||||
| Lo et al. [116] 2019 | Dataset from TCIA ** | ceT1w | 130 (30 Grade II, 43 Grade III, 57 Grade IV) | x | x | Contrast enhancement | x | x | x | x | x | ||||||
| Kurc et al. [117] 2020 | Data from TCGA | ceT1w, T2-FLAIR | 32 (16 OLI, 16 AST) | x | x | Bias field correction | x | x | |||||||||
| Pei et al. [118] 2020 | 1. CPM-RadPath 2019, 2. BraTS 2019 | T1w, ceT1w, T2w, FLAIR | 398 (329 from CPM-RadPath 2019, 69 from BraTS 2019) | x | x | x | Noise reduction | x | x | x | |||||||
| Ahammed et al. [72] 2019 | Private dataset | T2w | 20 | 557 (130 Grade I, 169 Grade II, Grade III 103, Grade IV 155) | x | Filtering, enhancement | x | x | x | x | |||||||
| Mohammed et al. [51] 2020 | Radiopaedia | No info shared | 60 (15 of each class) | 1258 (311 EP, 286 normal, 380 MEN, 281 MB) | x | Denoising | x | x | x | x | x | ||||||
| McAvoy et al. [119] 2021 | Private dataset | ceT1w | 320 (160 GBM, 160 PCNSL) | 3887 (2332 GBM, 1555 PCNSL) | x | x | Random changes to color, noise sampling | x | |||||||||
| Gilanie et al. [120] 2021 | Private dataset | T1w, T2w, FLAIR | 180 (50 AST-I, 40 AST-II, 40 AST-III, 50 AST-IV) | 30240 (8400 AST-I, 6720 AST-II, 6720 AST-III, 8400 AST-IV) | x | Bias field correction | x | ||||||||||
| Kulkarni et al. [121] 2021 | Private dataset | T1w, T2w, FLAIR | 200 (100 benign, 100 malignant) | Denoising, contrast enhancement | x | x | x | x | x | ||||||||
| Artzi et al. [122] 2021 | Private dataset | T1w, FLAIR, DTI | 158 (22 Normal, 63 PA, 57 MB, 16 EP) | 731 (110 Normal, 280 PA, 266 MB, 75 EP) | x | x | x | Background removal, bias field correction | x | x | x | Brightness changes | |||||
| Tariciotti et al. [123] 2022 | Private dataset | ceT1w | 121 (47 GBM, 37 PCNSL, 37 Metastasis) | 3597 (1481 GBM, 1073 PCNSL, 1043 Metastasis)) | x | x | Conversion to PNG | ||||||||||
| Ait et al. [124] 2022 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | |||||||||||
| Alanazi et al. [125] 2022 | 1. Dataset from Kaggle | No info shared | 826 Glioma, 822 MEN, 395 no tumor, and 827 PT | x | x | x | Noise removal | ||||||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | Noise removal | ||||||||||
| Ye et al. [126] 2022 | Private dataset | ceT1w | 73 | x | x | Image transformation | x | Blurring, ghosting, motion, affining, random elastic deformation | |||||||||
| Gaur et al. [127] 2022 | MRI dataset by Bhuvaji | No info shared | 2296 | x | Gaussian noise adding | ||||||||||||
| Guo et al. [128] 2022 | CPM-RadPath 2020 | T1w, ceT1w, T2w, FLAIR | 221 (133 GBM, 54 AST, 34 OLI) | x | x | Bias field correction, Gaussian noise adding | x | x | Random contrast adjusting | ||||||||
| Aamir et al. [129] 2022 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | Contrast enhancement | x | x | |||||||||
| Rizwan et al. [130] 2022 | Figshare (Cheng et al., 2017) | ceT1w | 230 (81 MEN, 90 Glioma, 59 PT) | 3061 (707 MEN, 1425 Glioma, 929 PT) | x | x | Noise filtering and smoothing | salt-noise/grayscale di stortion | |||||||||
| Dataset from TCIA | T1w | 513 (204 Grade II, 128 Grade III, 181 Grade IV) | 70 (32 Grade II, 18 Grade III, 20 Grade IV) | x | x | Noise filtering and smoothing | salt-noise/grayscale di stortion | ||||||||||
| Nayak et al. [131] 2022 | 1.daataset from Kaggle, 2. Figshare (Cheng et al., 2017) | ceT1w | 1. No info shared, 2. 233 (as shown in Table 2) | 3260 (196 Normal, 3064 (as shown in Table 2)) | x | Gaussian blurring, noise removal | x | x | x | ||||||||
| Chatterjee et al. [132] 2022 | 1.BraTS2019, 2. IXI Dataset | ceT1w | 1. 332 (259 HGG, 73 LGG), 2. 259 Normal | x | x | x | x | Affine | |||||||||
| Khazaee et al. [133] 2022 | BraTS2019 | ceT1w, T2w, FLAIR | 335 (259 HGG, 76 LGG) | 26,904 (13,233 HGG, 13,671 LGG) | x | x | |||||||||||
| Isunuri et al. [134] 2022 | Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | |||||||||||
| Gu et al. [30] 2021 | 1. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | ||||||||||||
| 2. REMBRANDT | No info shared | 130 | 110,020 | x | |||||||||||||
| Rajini [135] 2019 | 1. IXI dataset, REMBRANDT, TCGA-GBM, TCGA-LGG | No info shared | 600 normal images from IXI dataset, 130 patients from REMBRANDT, 200 patients from TCGA-GBM, 299 patients from TCGA-LGG | ||||||||||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | ||||||||||||||
| Anaraki et al. [136] 2019 | 1: IXI dataset, REMBRANDT, TCGA-GBM, TCGA-LGG, private dataset | no info of IXI, ceT1w from REMBRANDT, TCGA-GBM, TCGA-LGG | 600 normal images from IXI dataset, 130 patients from REMBRANDT, 199 patients from TCGA-GBM, 299 patients from TCGA-LGG, 60 patients from private dataset | x | x | x | x | x | x | ||||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | x | x | x | x | ||||||||
| Sajjad et al. [100] 2019 | 1. Radiopaedia | No info shared | 121 (36 Grade I, 32 Grade II, 25 Grade III, 28 Grade IV) | x | x | Denoising, bias field correction | x | x | x | Gaussian blurring, sharpening, embossing, skewing | |||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | x | Denoising, bias field correction | x | x | x | Gaussian blurring, sharpening, embossing, skewing | |||||||
| Wahlang et al. [137] 2020 | 1. Radiopaedia | FLAIR | 11 (2 Metastasis, 6 Glioma, 3 MEN) | x | |||||||||||||
| 2. BraTS 2017 | No info shared | 20 | 3100 | Median filtering | |||||||||||||
| Tandel et al. [138] 2021 | REMBRANDT | T2w | See 1–4 below | See 1–4 below | x | Converted to RGB | x | x | |||||||||
| 130 | 1. 2156 (1041 normal, 1091 tumorous) | ||||||||||||||||
| 47 | 2. 557 (356 AST-II, 201 AST-III) | ||||||||||||||||
| 21 | 3. 219 (128 OLI-II, 91 OLI-III) | ||||||||||||||||
| 112 | 4. 1115 (484 LGG, 631 HGG) | ||||||||||||||||
| Xiao et al. [97] 2021 | 1. Private dataset | No info shared | 1109 (495 MT, 614 Normal) | x | |||||||||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | x | |||||||||||||
| 3. Brain Tumor Classification (MRI) Dataset from Kaggle | No info shared | 3264 (937 MEN, 926 Glioma, 901 PT, 500 Normal) | x | ||||||||||||||
| Tandel et al. [24] 2020 | REMBRANDT | T2w | 112 (30 AST-II, 17 AST-II, 14 OLI-II, 7 OLI-III, 44 GBM) | See 1–5 below | x | x | x | ||||||||||
| 1. 2132 (1041 normal, 1091 tumorous) | |||||||||||||||||
| 2. 2156 (1041 normal, 484 LGG, 631 HGG) | |||||||||||||||||
| 3. 2156 (1041 normal, 557 AST, 219 OLI, 339 GBM) | |||||||||||||||||
| 4. 1115 (356 AST-II, 201 AST-III, 128 OLI-II, 91 OLI-III, 339 GBM) 5. 2156 (1041 normal, 356 AST-II, 201 AST-III, 128 OLI-II, 91 OLI-III, 339 GBM) | |||||||||||||||||
| Ayadi et al. [98] 2021 | 1. Radiopaedia | No info shared | 121 (36 Grade I, 32 Grade II, 25 Grade III, 28 Grade IV) | x | x | Gaussian blurring, sharpening | |||||||||||
| 2. Figshare (Cheng et al., 2017) | ceT1w | 233 (as shown in Table 2) | 3064 (as shown in Table 2) | ||||||||||||||
| 3. REMBRANDT | FLAIR, T1w, T2w | 130 (47 AST, 21 OLI, 44 GBM, 18 unknown) | See 1–5 below | x | x | Gaussian blurring, sharpening | |||||||||||
| 1. 2132 (1041 normal, 1091 tumorous) 2. 2156 (1041 normal, 484 LGG, 631 HGG) 3. 2156 (1041 normal, 557 AST, 219 OLI, 339 GBM) 4. 1115 (356 AST-II, 201 AST-III, 128 OLI-II, 91 OLI-III, 339 GBM) 5. 2156 (1041 normal, 356 AST-II, 201 AST-III, 128 OLI-II, 91 OLI-III, 339 GBM) | |||||||||||||||||
| (b) | |||||||||||||||||
| Author and Year | Classification Tasks | Model Architecture | Validation | Performance | ACC% 5 | ||||||||||||
| 2 classes | |||||||||||||||||
| Özcan et al. [27] 2021 | LGG (grade II) vs. HGG (grade IV) | Custom CNN model | 5-fold CV | SEN = 98.0%, SPE = 96.3%, F1 score = 97.0%, AUC = 0.989 | 97.1 | ||||||||||||
| Hao et al. [102] 2021 | LGG vs. HGG | Transfer learning with AlexNet | No info shared | AUC = 82.89% | |||||||||||||
| Tripathi et al. [103] 2021 | LGG vs. HGG | Transfer learning with Resnet18 | No info shared | 95.87 | |||||||||||||
| Ge et al. [40] 2020 | LGG vs. HGG | Custom CNN model | No info shared | SEN = 84.35%, SPE = 93.65% | 90.7 | ||||||||||||
| Mzoughi et al. [28] 2020 | LGG vs. HGG | Multi-scale 3D CNN | No info shared | 96.49 | |||||||||||||
| Yang et al. [45] 2018 | LGG vs. HGG | Transfer learning with AlexNet, GoogLeNet | 5-fold CV | AUC = 0.939 | 86.7 | ||||||||||||
| Zhuge et al. [77] 2020 | LGG vs. HGG | Transfer learning with ResNet50 | 5-fold CV | SEN = 93.5%, SPE = 97.2% | 96.3 | ||||||||||||
| 3D CNN | 5-fold CV | SEN = 94.7%, SPE = 96.8% | 97.1 | ||||||||||||||
| Decuyper et al. [73] 2021 | LGG vs. GBM | 3D CNN | No info shared | SEN = 90.16%, SPE = 89.80%, AUC = 0.9398 | 90 | ||||||||||||
| He et al. [78] 2021 | LGG vs. HGG | Custom CNN model | 5-fold CV | TCIA: SEN = 97.14%, SPE = 90.48%, AUC = 0.9349 | 92.86 | ||||||||||||
| BraTS 2017: SEN = 95.24%, SPE = 92%, AUC = 0.952 | 94.39 | ||||||||||||||||
| Hamdaoui et al. [104] 2021 | LGG vs. HGG | Transfer learning with stacking VGG16, VGG19, MobileNet, InceptionV3, Xception, Inception ResNetV2, DenseNet121 | 10-fold CV | PRE = 98.67%, F1 score = 98.62%, SEN = 98.33% | 98.06 | ||||||||||||
| Chikhalikar et al. [105] 2021 | LGG vs. HGG | Custom CNN model | No info shared | 99.46 | |||||||||||||
| Ahmad [106] 2019 | LGG vs. HGG | Custom CNN model | No info shared | 88 | |||||||||||||
| Khazaee et al. [133] 2022 | LGG vs. HGG | Transfer learning with EfficientNetB0 | CV | PRE = 98.98%, SEN = 98.86%, SPE = 98.79% | 98.87% | ||||||||||||
| Naser et al. [96] 2020 | LGG (Grade II) vs. LGG (Grade III) | Transfer learning with VGG16 | 5-fold CV | SEN = 97%, SPE = 98% | 95 | ||||||||||||
| Kurc et al. [117] 2020 | OLI vs. AST | 3D CNN | 5-fold CV | 80 | |||||||||||||
| McAvoy et al. [119] 2021 | GBM vs. PCNSL | Transfer learning with EfficientNetB4 | No info shared | GBM: AUC = 0.94, PCNSL: AUC = 0.95 | |||||||||||||
| Kulkarni et al. [121] 2021 | Benign vs. Malignant | Transfer learning with AlexNet | 5-fold CV | PRE = 93.7%, RE = 100%, F1 score = 96.77% | 96.55 | ||||||||||||
| Transfer learning with VGG16 | 5-fold CV | PRE = 55%, RE = 50%, F1 score = 52.38% | 50 | ||||||||||||||
| Transfer learning with ResNet18 | 5-fold CV | PRE = 78.94%, RE = 83.33%, F1 score = 81.07% | 82.5 | ||||||||||||||
| Transfer learning with ResNet50 | 5-fold CV | PRE = 95%, RE = 55.88%, F1 score = 70.36% | 60 | ||||||||||||||
| Transfer learning with GoogLeNet | 5-fold CV | PRE = 75%, RE = 100%, F1 score = 85.71% | 87.5 | ||||||||||||||
| Wahlang et al. [137] 2020 | HGG vs. LGG | AlexNet | No info shared | 62 | |||||||||||||
| U-Net | No info shared | 60 | |||||||||||||||
| Xiao et al. [97] 2021 | MT vs. Normal | Transfer learning with ResNet50 | 3-fold, 5-fold, 10-fold CV | AUC = 0.9530 | 98.2 | ||||||||||||
| Alanazi et al. [125] 2022 | Normal vs. Tumorous | Custom CNN | No info shared | 95.75% | |||||||||||||
| Tandel et al. [138] 2021 | 1. Normal vs. Tumorous | DL-MajVot (AlexNet, VGG16, ResNet18, GoogleNet, ResNet50) | 5-fold CV | SEN = 96.76%, SPE = 96.43%, AUC = 0.966 | 96.51 | ||||||||||||
| 2. AST-II vs. AST-III | DL-MajVot (AlexNet, VGG16, ResNet18, GoogleNet, ResNet50) | 5-fold CV | SEN = 94.63%, SPE = 99.44%, AUC = 0.9704 | 97.7 | |||||||||||||
| 3. OLI-II vs. OLI-III | DL-MajVot (AlexNet, VGG16, ResNet18, GoogleNet, ResNet50) | 5-fold CV | SEN = 100%, SPE = 100%, AUC = 1 | 100 | |||||||||||||
| 4. LGG vs. HGG | DL-MajVot (AlexNet, VGG16, ResNet18, GoogleNet, ResNet50) | 5-fold CV | SEN = 98.33%, SPE = 98.57%, AUC = 0.9845 | 98.43 | |||||||||||||
| Tandel et al. [24] 2020 | Normal vs. Tumorous | Transfer learning with AlexNet | Multiple CV (K2, K5, K10) | RE = 100%, PRE = 100%, F1 score = 100% | 100 | ||||||||||||
| Ayadi et al. [98] 2021 | Normal vs. Tumorous | Custom CNN model | 5-fold CV | 100 | |||||||||||||
| Ye et al. [126] 2022 | Germinoma vs. Glioma | Transfer learning with ResNet18 | 5-fold CV | AUC = 0.88 | 81% | ||||||||||||
| 3 classes | |||||||||||||||||
| Allah et al. [44] 2021 | MEN vs. Glioma vs. PT | PGGAN-augmentation VGG19 | No info shared | 98.54 | |||||||||||||
| Swati et al. [50] 2019 | MEN vs. Glioma vs. PT | Transfer learning with VGG19 | 5-fold CV | SEN = 94.25%, SPE = 94.69%, PRE = 89.52%, F1 score = 91.73% | 94.82 | ||||||||||||
| Guan et al. [43] 2021 | MEN vs. Glioma vs. PT | EfficientNet | 5-fold CV | 98.04 | |||||||||||||
| Deepak et al. [39] 2019 | MEN vs. Glioma vs. PT | Transfer learning with GoogleNet | 5-fold CV | 98 | |||||||||||||
| Díaz-Pernas et al. [42] 2021 | MEN vs. Glioma vs. PT | Multiscale CNN | 5-fold CV | 97.3 | |||||||||||||
| Ismael et al. [49] 2020 | MEN vs. Glioma vs. PT | Residual networks | 5-fold CV | PRE = 99.0%, RE = 99.0%, F1 score = 99.0% | 99 | ||||||||||||
| Alhassan et al. [107] 2021 | MEN vs. Glioma vs. PT | Custom CNN model | k-fold CV | PRE = 99.6%, RE = 98.6%, F1 score = 99.0% | 98.6 | ||||||||||||
| Bulla et al. [108] 2020 | MEN vs. Glioma vs. PT | Transfer learning with InceptionV3 CNN model | holdout validation, 10-fold CV, stratified 10-fold CV, group 10-fold CV | Under group 10-fold CV: PRE = 97.57%, RE = 99.47%, F1 score = 98.40%, AUC = 0.995 | 99.82 | ||||||||||||
| Ghassemi et al. [109] 2020 | MEN vs. Glioma vs. PT | CNN-GAN | 5-fold CV | PRE = 95.29%, SEN = 94.91%, SPE = 97.69%, F1 score = 95.10% | 95.6 | ||||||||||||
| Kakarla et al. [110] 2021 | MEN vs. Glioma vs. PT | Custom CNN model | 5-fold CV | PRE = 97.41%, RE = 97.42% | 97.42 | ||||||||||||
| Noreen et al. [111] 2021 | MEN vs. Glioma vs. PT | Transfer learning with Inception-v3 | K-fold CV | 93.31 | |||||||||||||
| Transfer learning with Inception model | K-fold CV | 91.63 | |||||||||||||||
| Noreen et al. [112] 2020 | MEN vs. Glioma vs. PT | Transfer learning with Inception-v3 | No info shared | 99.34 | |||||||||||||
| Transfer learning with DensNet201 | No info shared | 99.51 | |||||||||||||||
| Kumar et al. [113] 2021 | MEN vs. Glioma vs. PT | Transfer learning with ResNet50 | 5-fold CV | PRE = 97.20%, RE = 97.20%, F1 score = 97.20% | |||||||||||||
| Badža et al. [114] 2020 | MEN vs. Glioma vs. PT | Custom CNN model | 10-fold CV | PRE = 95.79%, RE = 96.51%, F1 score = 96.11% | 96.56 | ||||||||||||
| Ait et al. [124] 2022 | MEN vs. Glioma vs. PT | Custom CNN | No info shared | PRE = 98.3%, SEN = 98.6%, F1 score = 98.6% | 98.70% | ||||||||||||
| Alanazi et al. [125] 2022 | MEN vs. Glioma vs. PT | Custom CNN | No info shared | 96.90% | |||||||||||||
| Gaur et al. [127] 2022 | MEN vs. Glioma vs. PT | Custom CNN | k-fold CV | 94.64% | |||||||||||||
| Aamir et al. [129] 2022 | MEN vs. Glioma vs. PT | Custom CNN | 5-fold CV | 98.95% | |||||||||||||
| Rizwan et al. [130] 2022 | MEN vs. Glioma vs. PT | Custom CNN | No info shared | 99.8% | |||||||||||||
| Isunuri et al. [134] 2022 | MEN vs. Glioma vs. PT | Custom CNN | 5-fold CV | PRE = 97.33%, SEN = 97.19%, F1 score = 97.26% | 97.52% | ||||||||||||
| Alaraimi et al. [115] 2021 | MEN vs. Glioma vs. PT | Transfer learning with AlexNet | No info shared | AUC = 0.976 | 94.4 | ||||||||||||
| Transfer learning with VGG16 | No info shared | AUC = 0.981 | 100 | ||||||||||||||
| Transfer learning with GoogLeNet | No info shared | AUC = 0.986 | 98.5 | ||||||||||||||
| Lo et al. [116] 2019 | Grade II vs. Grade III vs. Grade IV | Transfer learning with AlexNet | 10-fold CV | 97.9 | |||||||||||||
| Pei et al. [118] 2020 | GBM vs. AST vs. OLI | 3D CNN | No info shared | 74.9 | |||||||||||||
| Gu et al. [30] 2021 | 1. MEN vs. Glioma vs. PT | Custom CNN model | 5-fold CV | SEN = 94.64%, PRE = 94.61%, F1 score = 94.70% | 96.39 | ||||||||||||
| 2. GBM vs. AST vs. OLI | Custom CNN model | 5-fold CV | SEN = 93.66%, PRE = 95.12%, F1 score = 94.05% | 97.37 | |||||||||||||
| Rajini [135] 2019 | MEN vs. Glioma vs. PT | Custom CNN model | 5-fold CV | 98.16 | |||||||||||||
| Anaraki et al. [136] 2019 | MEN vs. Glioma vs. PT | Custom CNN model | 5-fold CV | 94.2 | |||||||||||||
| Sajjad et al. [100] 2019 | MEN vs. Glioma vs. PT | Transfer learning with VGG19 | No info shared | SEN = 88.41%, SPE = 96.12% | 94.58 | ||||||||||||
| Wahlang et al. [137] 2020 | Metastasis vs. Glioma vs. MEN | Lenet | No info shared | 48 | |||||||||||||
| AlexNet | No info shared | 75 | |||||||||||||||
| Xiao et al. [97] 2021 | MEN vs. Glioma vs. PT | Transfer learning with ResNet50 | 3-fold, 5-fold, 10-fold CV | 98.02 | |||||||||||||
| Tandel et al. [24] 2020 | Normal vs. LGG vs. HGG | Transfer learning with AlexNet | Multiple CV (K2, K5, K10) | RE = 94.85%, PRE = 94.75%, F1 score = 94.8% | 95.97 | ||||||||||||
| Chatterjee et al. [132] 2022 | Normal vs. HGG vs. LGG | Transfer learning with ResNet | 3-fold CV | F1 score = 93.45% | 96.84% | ||||||||||||
| Ayadi et al. [98] 2021 | 1. Normal vs. LGG vs. HGG | Custom CNN model | 5-fold CV | 95 | |||||||||||||
| 2. MEN vs. Glioma vs. PT | Custom CNN model | 5-fold CV | 94.74 | ||||||||||||||
| Guo et al. [128] 2022 | GBM vs. AST vs. OLI | Custom CNN | 3-fold CV | SEN = 0.772, SPE = 93.0%, AUC = 0.902 | 87.8% | ||||||||||||
| Rizwan et al. [130] 2022 | Grade I vs. Grade II vs. Grade III | Custom CNN | No info shared | 97.14% | |||||||||||||
| Tariciotti et al. [123] 2022 | Metastasis vs. GBM vs. PCNSL | Resnet101 | Hold-out | PRE = 91.88%, SEN = 90.84%, SPE = 96.34%, F1 score = 91.0%, AUC = 0.92 | 94.72% | ||||||||||||
| 4 classes | |||||||||||||||||
| Ahammed et al. [72] 2019 | Grade I vs. Grade II vs. Grade III vs. Grade IV | VGG19 | No info shared | PRE = 94.71%, SEN = 92.72%, SPE = 98.13%, F1 score = 93.71% | 98.25 | ||||||||||||
| Mohammed et al. [51] 2020 | EP vs. MEN vs. MB vs. Normal | Custom CNN model | No info shared | SEN = 96%, PRE = 100% | 96 | ||||||||||||
| Gilanie et al. [120] 2021 | AST-I vs. AST-II vs. AST-III vs. AST-IV | Custom CNN model | No info shared | 96.56 | |||||||||||||
| Artzi et al. [122] 2021 | Normal vs. PA vs. MB vs. EP | Custom CNN model | 5-fold CV | 88 | |||||||||||||
| Nayak et al. [131] 2022 | Normal vs. MEN vs. Glioma vs. PT | Transfer learning with EfficientNet | No info shared | PRE = 98.75%, F1 score = 98.75% | 98.78% | ||||||||||||
| Rajini [135] 2019 | Normal vs. Grade II vs. Grade III vs. Grade IV | Custom CNN model | 5-fold CV | 96.77 | |||||||||||||
| Anaraki et al. [136] 2019 | Normal vs. Grade II vs. Grade III vs. Grade IV | Custom CNN model | 5-fold CV | ||||||||||||||
| Sajjad et al. [100] 2019 | Grade I vs. Grade II vs. Grade III vs. Grade IV | Transfer learning with VGG19 | No info shared | 90.67 | |||||||||||||
| Xiao et al. [97] 2021 | MEN vs. Glioma vs. PT vs. Normal | Transfer learning with ResNet50 | 3-fold, 5-fold, 10-fold CV | PRE = 97.43%, RE = 97.67%, SPE = 99.24%, F1 score = 97.55% | 97.7 | ||||||||||||
| Tandel et al. [24] 2020 | Normal vs. AST vs. OLI vs. GBM | Transfer learning with AlexNet | Multiple CV (K2, K5, K10) | RE = 94.17%, PRE = 95.41%, F1 score = 94.78% | 96.56 | ||||||||||||
| Ayadi et al. [98] 2021 | 1. normal vs. AST vs. OLI vs. GBM | Custom CNN model | 5-fold CV | 94.41 | |||||||||||||
| 2. Grade I vs. Grade II vs. Grade III vs. Grade IV | Custom CNN model | 5-fold CV | 93.71 | ||||||||||||||
| 5 classes | |||||||||||||||||
| Tandel et al. [24] 2020 | AST-II vs. AST-III vs. OLI-II vs. OLI-III vs. GBM-IV | Transfer learning with AlexNet | Multiple CV (K2, K5, K10) | RE = 84.4%, PRE = 89.57%, F1 score = 86.89% | 87.14 | ||||||||||||
| Ayadi et al. [98] 2021 | AST-II vs. AST-III vs. OLI-II vs. OLI-III vs. GBM | Custom CNN model | 5-fold CV | 86.08 | |||||||||||||
| 6 classes | |||||||||||||||||
| Tandel et al. [24] 2020 | Normal vs. AST-II vs. AST-III vs. OLI-II vs. OLI-III vs. GBM-IV | Transfer learning with AlexNet | Multiple CV (K2, K5, K10) | RE = 91.51%, PRE = 92.46%, F1 score = 91.97% | 93.74 | ||||||||||||
| Ayadi et al. [98] 2021 | normal vs. AST-II vs. AST-III vs. OLI-II vs. OLI-III vs. GBM | Custom CNN model | 5-fold CV | 92.09 | |||||||||||||
5. Discussion
5.1. The Importance of the Classification Task
5.2. The Effect of the Dataset
5.3. The Effect of CNN Architecture
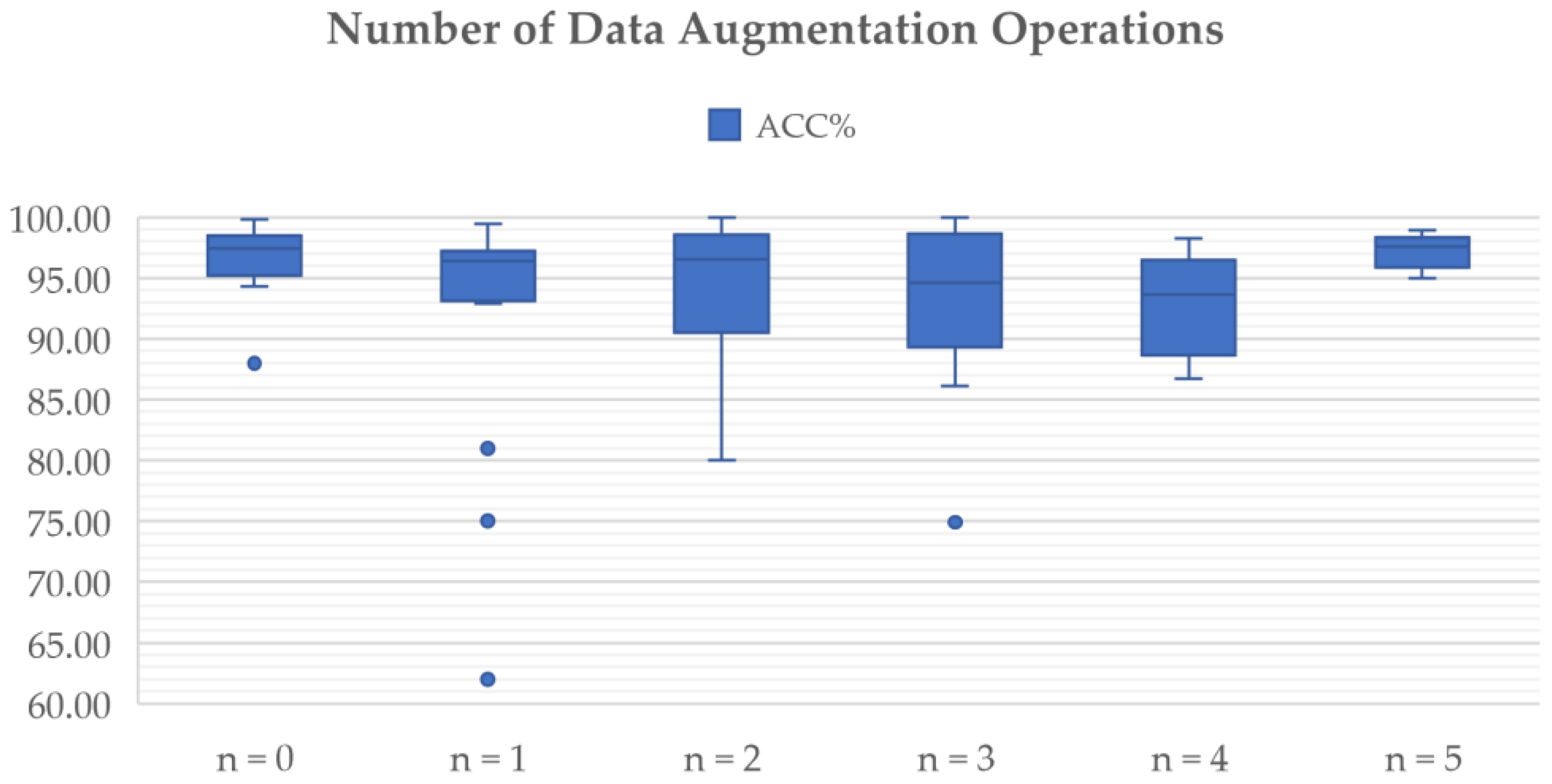
5.4. The Effect of Pre-Processing and Data Augmentation Methods
5.5. The Effect of Other Factors
5.6. Future Directions
5.6.1. The Training Data Problem
5.6.2. The Evaluation Problem
5.6.3. Explainability and Trust
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Branger, D.F.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/brain-other-cns-and-intracranial-tumours/incidence%23collapseTen#heading-One (accessed on 10 February 2022).
- Islami, F.; Ward, E.M.; Sung, H.; Cronin, K.A.; Tangka, F.K.L.; Sherman, R.L.; Zhao, J.X.; Anderson, R.N.; Henley, S.J.; Yabroff, K.R.; et al. Annual report to the nation on the status of cancer, part 1: National cancer statistics. JNCI J. Natl. Cancer Inst. 2021, 113, 1648–1669. [Google Scholar] [CrossRef]
- Johnson, D.R.; O’Neill, B.P. Glioblastoma survival in the United States before and during the temozolomide era. J. Neurooncol. 2012, 107, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Jiang, X. Progress on the diagnosis and evaluation of brain tumors. Cancer Imaging 2013, 13, 466. [Google Scholar] [CrossRef]
- Villanueva-Meyer, J.E.; Mabray, M.C.; Cha, S. Current clinical brain tumor imaging. Neurosurgery 2017, 81, 397–415. [Google Scholar] [CrossRef] [PubMed]
- Zaccagna, F.; Riemer, F.; Priest, A.N.; McLean, M.A.; Allinson, K.; Grist, J.T.; Dragos, C.; Matys, T.; Gillard, J.H.; Watts, C.; et al. Non-invasive assessment of glioma microstructure using VERDICT MRI: Correlation with histology. Eur. Radiol. 2019, 29, 5559–5566. [Google Scholar] [CrossRef] [PubMed]
- Radbruch, A.; Wiestler, B.; Kramp, L.; Lutz, K.; Bäumer, P.; Weiler, M.; Roethke, M.; Sahm, F.; Schlemmer, H.P.; Wick, W.; et al. Differentiation of glioblastoma and primary CNS lymphomas using susceptibility weighted imaging. Eur. J. Radiol. 2013, 82, 552–556. [Google Scholar] [CrossRef]
- Xiao, H.-F.; Chen, Z.-Y.; Lou, X.; Wang, Y.L.; Gui, Q.P.; Wang, Y.; Shi, K.N.; Zhou, Z.Y.; Zheng, D.D.; Wang, D.J.J.; et al. Astrocytic tumour grading: A comparative study of three-dimensional pseudo continuous arterial spin labelling, dynamic susceptibility contrast-enhanced perfusion-weighted imaging, and diffusion-weighted imaging. Eur. Radiol. 2015, 25, 3423–3430. [Google Scholar] [CrossRef] [PubMed]
- Zaccagna, F.; Grist, J.T.; Quartuccio, N.; Riemer, F.; Fraioli, F.; Caracò, C.; Halsey, R.; Aldalilah, Y.; Cunningham, C.H.; Massoud, T.F.; et al. Imaging and treatment of brain tumors through molecular targeting: Recent clinical advances. Eur. J. Radiol. 2021, 142, 109842. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, P.; Figueiredo, I.; Pinto, L.; Kumar, S.; Tsai, Y.; Mamonov, A. Polyp detection with computer-aided diagnosis in white light colonoscopy: Comparison of three different methods. Endosc. Int. Open 2019, 7, E209–E215. [Google Scholar] [CrossRef]
- Yeung, M.; Sala, E.; Schönlieb, C.B.; Rundo, L. Focus U-Net: A novel dual attention-gated CNN for polyp segmentation during colonoscopy. Comput. Biol. Med. 2021, 137, 104815. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Liu, J.Y.; Sun, X.W.; Zheng, B.; Nie, S.D. Computer-aided diagnosis of lung cancer: The effect of training data sets on classification accuracy of lung nodules. Phys. Med. Biol. 2018, 63, 035036. [Google Scholar] [CrossRef] [PubMed]
- Nishio, M.; Sugiyama, O.; Yakami, M.; Ueno, S.; Kubo, T.; Kuroda, T.; Togashi, K. Computer-aided diagnosis of lung nodule classification between benign nodule, primary lung cancer, and metastatic lung cancer at different image size using deep convolutional neural network with transfer learning. PLoS ONE 2018, 13, e0200721. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Wu, Y.; Ren, X.; Razmjooy, N. A new optimized sequential method for lung tumor diagnosis based on deep learning and converged search and rescue algorithm. Biomed. Signal Process. Control 2021, 68, 102761. [Google Scholar] [CrossRef]
- Buchlak, Q.D.; Esmaili, N.; Leveque, J.C.; Bennett, C.; Farrokhi, F.; Piccardi, M. Machine learning applications to neuroimaging for glioma detection and classification: An artificial intelligence augmented systematic review. J. Clin. Neurosci. 2021, 89, 177–198. [Google Scholar] [CrossRef]
- Ahmadi, M.; Dashti Ahangar, F.; Astaraki, N.; Abbasi, M.; Babaei, B. FWNNet: Presentation of a New Classifier of Brain Tumor Diagnosis Based on Fuzzy Logic and the Wavelet-Based Neural Network Using Machine-Learning Methods. Comput. Intell. Neurosci. 2021, 2021, 8542637. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, A.; Ramaniharan, A.K.; Gupta, R.K.; Agarwal, S.; Singh, A. Glioma grading using a machine-learning framework based on optimized features obtained from T1 perfusion MRI and volumes of tumor components. J. Magn. Reson. Imaging 2019, 50, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wu, W.; Zhu, B.; Wang, H.T.; Liu, R.Y.; Zhang, X.; Li, M.; Yang, Y.B.; Yan, J.; Niu, F.N.; et al. Cerebral glioma grading using Bayesian network with features extracted from multiple modalities of magnetic resonance imaging. PLoS ONE 2016, 11, e0153369. [Google Scholar]
- Raju, A.R.; Suresh, P.; Rao, R.R. Bayesian HCS-based multi-SVNN: A classification approach for brain tumor segmentation and classification using Bayesian fuzzy clustering. Biocybern. Biomed. Eng. 2018, 38, 646–660. [Google Scholar] [CrossRef]
- Schulz, M.A.; Yeo, B.T.; Vogelstein, J.T.; Miranada, J.M.; Kather, J.N.; Kording, K.; Richards, B.; Bzdok, D. Different scaling of linear models and deep learning in UKBiobank brain images versus machine-learning datasets. Nat. Commun. 2020, 11, 4238. [Google Scholar] [CrossRef]
- Schmidhuber, J. Deep learning in neural networks: An overview. Neural Netw. 2015, 61, 85–117. [Google Scholar] [CrossRef]
- Hu, A.; Razmjooy, N. Brain tumor diagnosis based on metaheuristics and deep learning. Int. J. Imaging Syst. Technol. 2021, 31, 657–669. [Google Scholar] [CrossRef]
- Tandel, G.S.; Balestrieri, A.; Jujaray, T.; Khanna, N.N.; Saba, L.; Suri, J.S. Multiclass magnetic resonance imaging brain tumor classification using artificial intelligence paradigm. Comput. Biol. Med. 2020, 122, 103804. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.; Wu, G.; Suk, H.I. Deep learning in medical image analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [PubMed]
- Yasaka, K.; Akai, H.; Kunimatsu, A.; Kiryu, S.; Abe, O. Deep learning with convolutional neural network in radiology. Jpn. J. Radiol. 2018, 36, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Özcan, H.; Emiroğlu, B.G.; Sabuncuoğlu, H.; Özdoğan, S.; Soyer, A.; Saygı, T. A comparative study for glioma classification using deep convolutional neural networks. Math. Biosci. Eng. MBE 2021, 18, 1550–1572. [Google Scholar] [CrossRef] [PubMed]
- Mzoughi, H.; Njeh, I.; Wali, A.; Slima, M.B.; BenHamida, A.; Mhiri, C.; Mahfoudhe, K.B. Deep multi-scale 3D convolutional neural network (CNN) for MRI gliomas brain tumor classification. J. Digit. Imaging 2020, 33, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Abd El Kader, I.; Xu, G.; Shuai, Z.; Saminu, S.; Javaid, I.; Salim Ahmad, I. Differential deep convolutional neural network model for brain tumor classification. Brain Sci. 2021, 11, 352. [Google Scholar] [CrossRef]
- Gu, X.; Shen, Z.; Xue, J.; Fan, Y.; Ni, T. Brain Tumor MR Image Classification Using Convolutional Dictionary Learning With Local Constraint. Front. Neurosci. 2021, 15, 679847. [Google Scholar] [CrossRef]
- Ali, S.; Li, J.; Pei, Y.; Khurram, R.; Mahmood, T. A Comprehensive Survey on Brain Tumor Diagnosis Using Deep Learning and Emerging Hybrid Techniques with Multi-modal MR Image. Arch. Comput. Methods Eng. 2022, 1–26. [Google Scholar] [CrossRef]
- Avorn, J.; Fischer, M. ‘Bench to behavior’: Translating comparative effectiveness research into improved clinical practice. Health Aff. 2010, 29, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Zadeh Shirazi, A.; Fornaciari, E.; McDonnell, M.D.; Yaghoobi, M.; Cevallos, Y.; Tello-Oquendo, L.; Inca, D.; Gomez, G.A. The application of deep convolutional neural networks to brain cancer images: A survey. J. Pers. Med. 2020, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Arabahmadi, M.; Farahbakhsh, R.; Rezazadeh, J. Deep Learning for Smart Healthcare—A Survey on Brain Tumor Detection from Medical Imaging. Sensors 2022, 22, 1960. [Google Scholar] [CrossRef]
- Nazir, M.; Shakil, S.; Khurshid, K. Role of Deep Learning in Brain Tumor Detection and Classification (2015 to 2020): A Review. Comput. Med. Imaging Graph. 2021, 91, 101940. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, K.; Khan, S.; Del Ser, J.; De Albuquerque, V.H.C. Deep learning for multigrade brain tumor classification in smart healthcare systems: A prospective survey. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 507–522. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Miotto, R.; Wang, F.; Wang, S.; Jiang, X.; Dudley, J.T. Deep learning for healthcare: Review, opportunities and challenges. Brief. Bioinform. 2018, 19, 1236–1246. [Google Scholar] [CrossRef] [PubMed]
- Deepak, S.; Ameer, P.M. Brain tumor classification using deep CNN features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef] [PubMed]
- Ge, C.; Gu, I.Y.H.; Jakola, A.S.; Yang, J. Deep semi-supervised learning for brain tumor classification. BMC Med. Imaging 2020, 20, 87. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Xu, H.; Su, S.; Wang, T.; Luo, Y.; Zhao, X.; Liu, Y.; Song, G.; Zhao, Y. A computer-aided diagnosis system for brain magnetic resonance imaging images using a novel differential feature neural network. Comput. Biol. Med. 2020, 121, 103818. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Pernas, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M.; González-Ortega, D. A deep learning approach for brain tumor classification and segmentation using a multiscale convolutional neural network. Healthcare 2021, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Aamir, M.; Rahman, Z.; Ali, A.; Abro, W.A.; Dayo, Z.; Bhutta, M.; Hu, Z. A framework for efficient brain tumor classification using MRI images. Math. Biosci. Eng. 2021, 18, 5790–5815. [Google Scholar] [CrossRef] [PubMed]
- Gab Allah, A.M.; Sarhan, A.M.; Elshennawy, N.M. Classification of Brain MRI Tumor Images Based on Deep Learning PGGAN Augmentation. Diagnostics 2021, 11, 2343. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yan, L.F.; Zhang, X.; Han, Y.; Nan, H.Y.; Hu, Y.C.; Hu, B.; Yan, S.L.; Zhang, J.; Cheng, D.L.; et al. Glioma grading on conventional MR images: A deep learning study with transfer learning. Front. Neurosci. 2018, 12, 804. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, J. What is the Difference Between Test and Validation Datasets? Available online: https://machinelearningmastery.com/difference-test-validation-datasets (accessed on 18 February 2022).
- Prechelt, L.; Geneviève, B. Early Stopping—But When? In Neural Networks: Tricks of the Trade; Lecture Notes in Computer Science; Montavon, G., Orr, G., Müller, K.R., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 53–67. [Google Scholar]
- F-Score, Wikipedia. Available online: https://en.wikipedia.org/wiki/F-score (accessed on 22 March 2022).
- Ismael, S.A.A.; Mohammed, A.; Hefny, H. An enhanced deep learning approach for brain cancer MRI images classification using residual networks. Artif. Intell. Med. 2020, 102, 101779. [Google Scholar] [CrossRef] [PubMed]
- Swati, Z.N.K.; Zhao, Q.; Kabir, M.; <monospace> </monospace>Ali, F.; Ali, Z.; Ahmed, S.; Lu, J. Brain tumor classification for MR images using transfer learning and fine-tuning. Comput. Med. Imaging Graph. 2019, 75, 34–46. [Google Scholar] [CrossRef]
- Mohammed, B.A.; Al-Ani, M.S. An efficient approach to diagnose brain tumors through deep CNN. Math. Biosci. Eng. 2020, 18, 851–867. [Google Scholar] [CrossRef]
- Signorell, A.; Aho, K.; Alfons, A.; Anderegg, N.; Aragon, T.; Arppe, A.; Baddeley, A.; Barton, K.; Bolker, B.; Borchers, H.W. DescTools: Tools for Descriptive Statistics. R Package Version 0.99.44. Available online: https://cran.r-project.org/package=DescTools (accessed on 4 May 2022).
- The Cancer Genome Atlas, TCGA-GBM. Available online: https://wiki.cancerimagingarchive.net/display/Public/TCGA-GBM (accessed on 30 April 2022).
- The Cancer Genome Atlas, TCGA-LGG. Available online: https://wiki.cancerimagingarchive.net/display/Public/TCGA-LGG (accessed on 30 April 2022).
- Figshare, Brain Tumor Dataset. Available online: https://figshare.com/articles/dataset/brain_tumor_dataset/1512427/5 (accessed on 30 April 2022).
- Navoneel, C. Available online: https://www.kaggle.com/navoneel/brain-mri-images-for-brain-tumor-detect (accessed on 30 April 2022).
- REMBRANDT. Available online: https://wiki.cancerimagingarchive.net/display/Public/REMBRANDT (accessed on 30 April 2022).
- Brain Tumor Segmentation (BraTS) Challenge. Available online: http://www.braintumorsegmentation.org/ (accessed on 30 April 2022).
- ClinicalTrials.gov. Available online: https://www.clinicaltrials.gov/ (accessed on 30 April 2022).
- Computational Precision Medicine: Radiology-Pathology Challenge on Brain Tumor Classification 2019. Available online: https://www.med.upenn.edu/cbica/cpm-rad-path-2019/ (accessed on 30 April 2022).
- IXI Dataset. Available online: https://brain-development.org/ixi-dataset/ (accessed on 30 April 2022).
- Rider Neuro MRI. Available online: https://wiki.cancerimagingarchive.net/display/Public/RIDER+NEURO+MRI (accessed on 30 April 2022).
- Harvard Medical School Data. Available online: http://www.med.harvard.edu/AANLIB/ (accessed on 30 April 2022).
- Wikipedia. MRI Sequence. Available online: https://en.wikipedia.org/wiki/MRI_sequence (accessed on 18 February 2022).
- My-MS.org. MRI Basics. Available online: https://my-ms.org/mri_basics.htm (accessed on 18 February 2022).
- Basic Proton MR Imaging. Harvard Medical School. Available online: http://www.med.harvard.edu/aanlib/basicsmr.html (accessed on 19 February 2022).
- Fluid Attenuation Inversion Recovery. Radiopaedia.org. Available online: https://radiopaedia.org/articles/fluid-attenuated-inversion-recovery (accessed on 19 February 2022).
- Chen, M.W.; King NK, K.; Selvarajan, S.; Low, D.C. Benign scalp lump as an unusual presentation of extranodal Rosai-Dorfman disease. Surg. Neurol. Int. 2014, 5, 99. [Google Scholar] [CrossRef]
- Mohan, G.; Subashini, M.M. MRI based medical image analysis: Survey on brain tumor grade classification. Biomed. Signal Processing Control 2018, 39, 139–161. [Google Scholar] [CrossRef]
- Collewet, G.; Strzelecki, M.; Mariette, F. Influence of MRI acquisition protocols and image intensity normalization methods on texture classification. Magn. Reson. Imaging 2004, 22, 81–91. [Google Scholar] [CrossRef]
- Eesa, A.S.; Arabo, W.K. A normalization methods for backpropagation: A comparative study. Sci. J. Univ. Zakho 2017, 5, 319–323. [Google Scholar] [CrossRef]
- Ahammed Muneer, K.V.; Rajendran, V.R. Glioma tumor grade identification using artificial intelligent techniques. J. Med. Syst. 2019, 43, 113. [Google Scholar] [CrossRef] [PubMed]
- Decuyper, M.; Bonte, S.; Deblaere, K.; Van Holen, R. Automated MRI based pipeline for segmentation and prediction of grade, IDH mutation and 1p19q co-deletion in glioma. Comput. Med. Imaging Graph. 2021, 88, 101831. [Google Scholar] [CrossRef]
- Hashemi, M. Enlarging smaller images before inputting into convolutional neural network: Zero-padding vs. interpolation. J. Big Data 2019, 6, 98. [Google Scholar] [CrossRef]
- Hashemi, M. Web page classification: A survey of perspectives, gaps, and future directions. Multimed. Tools Appl. 2020, 79, 11921–11945. [Google Scholar] [CrossRef]
- Karthick, S.; Maniraj, S. Different medical image registration techniques: A comparative analysis. Curr. Med. Imaging 2019, 15, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Zhuge, Y.; Ning, H.; Mathen, P.; Cheng, J.Y.; Krauze, A.V.; Camphausen, K.; Miller, R.W. Automated glioma grading on conventional MRI images using deep convolutional neural networks. Med. Phys. 2020, 47, 3044–3053. [Google Scholar] [CrossRef]
- He, M.; Han, K.; Zhang, Y.; Chen, W. Hierarchical-order multimodal interaction fusion network for grading gliomas. Phys. Med. Biol. 2021, 66, 215016. [Google Scholar] [CrossRef]
- Song, S.; Zheng, Y.; He, Y. A review of methods for bias correction in medical images. Biomed. Eng. Rev. 2017, 1, 1–10. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4itk: Improved n3bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [PubMed]
- Gispert, J.D.; Reig, S.; Pascau, J.; Vaquero, J.J.; García-Barreno, P.; Desco, M. Method for bias field correction of brain T1-weighted magnetic resonance images minimizing segmentation error. Hum. Brain Mapp. 2004, 22, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Introduction to Data Mismatch, Overfitting and Underfitting in Building Machine Learning Systems. Towards Data Science. Available online: https://towardsdatascience.com/introduction-to-overfitting-underfitting-and-data-mismatch-in-building-machine-learning-systems-52f1225a8a35 (accessed on 19 February 2022).
- Hicks, S.A.; Strümke, I.; Thambawita, V.; Hammou, M.; Riegler, M.A.; Halvorsen, P.; Parasa, S. On evaluation metrics for medical applications of artificial intelligence. Sci. Rep. 2022, 12, 5979. [Google Scholar] [CrossRef] [PubMed]
- Toshniwal, R. How to Select Performance Metrics for Classification Models. Available online: https://medium.com/analytics-vidhya/how-to-select-performance-metrics-for-classification-models-c847fe6b1ea3 (accessed on 13 July 2022).
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. NIPS 2012, 60, 84–90. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep CNN for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NA, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- The Perelman School of Medicine at the University of Pennsylvania. Multimodal Brain Tumor Segmentation Challenge 2019. Available online: http://braintumorsegmentation.org/ (accessed on 19 February 2022).
- Li, D.C.; Liu, C.W.; Hu, S.C. A learning method for the class imbalance problem with medical data sets. Comput. Biol. Med. 2010, 40, 509–518. [Google Scholar] [CrossRef] [PubMed]
- El Kader, I.A.; Xu, G.; Shuai, Z.; Saminu, S. Brain tumor detection and classification by hybrid CNN-DWA model using MR images. Curr. Med. Imaging 2021, 17, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.A.; Jue, W.; Mushtaq, M.; Mushtaq, M.U. Brain tumor classification in MRI image using convolutional neural network. Math. Biosci. Eng 2020, 17, 6203–6216. [Google Scholar] [CrossRef]
- Naser, M.A.; Deen, M.J. Brain tumor segmentation and grading of lower-grade glioma using deep learning in MRI images. Comput. Biol. Med. 2020, 121, 103758. [Google Scholar] [CrossRef] [PubMed]
- Xiao, G.; Wang, H.; Shen, J.; Chen, Z.; Zhang, Z.; Ge, X. Synergy Factorized Bilinear Network with a Dual Suppression Strategy for Brain Tumor Classification in MRI. Micromachines 2022, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Ayadi, W.; Elhamzi, W.; Charfi, I.; Atri, M. Deep CNN for brain tumor classification. Neural Process. Lett. 2021, 53, 671–700. [Google Scholar] [CrossRef]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef] [PubMed]
- Sajjad, M.; Khan, S.; Muhammad, K.; Wu, W.; Ullah, A.; Baik, S.W. Multi-grade brain tumor classification using deep CNN with extensive data augmentation. J. Comput. Sci. 2019, 30, 174–182. [Google Scholar] [CrossRef]
- Weiss, K.; Khoshgoftaar, T.M.; Wang, D.D. A survey of transfer learning. J. Big Data 2016, 3, 9. [Google Scholar] [CrossRef]
- Hao, R.; Namdar, K.; Liu, L.; Khalvati, F. A transfer learning–based active learning framework for brain tumor classification. Front. Artif. Intell. 2021, 4, 635766. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, P.C.; Bag, S. A computer-aided grading of glioma tumor using deep residual networks fusion. Comput. Methods Programs Biomed. 2022, 215, 106597. [Google Scholar] [CrossRef] [PubMed]
- El Hamdaoui, H.; Benfares, A.; Boujraf, S.; Chaoui, N.E.H.; Alami, B.; Maaroufi, M.; Qjidaa, H. High precision brain tumor classification model based on deep transfer learning and stacking concepts. Indones. J. Electr. Eng. Comput. Sci. 2021, 24, 167–177. [Google Scholar] [CrossRef]
- Chikhalikar, A.M.; Dharwadkar, N.V. Model for Enhancement and Segmentation of Magnetic Resonance Images for Brain Tumor Classification. Pattern Recognit. Image Anal. 2021, 31, 49–59. [Google Scholar] [CrossRef]
- Ahmad, F. Classification on magnetic resonance imaging (Mri) brain tumour using BPNN, SVM and CNN. Int. J. Recent Technol. Eng. (IJRTE) 2019, 8, 8601–8607. [Google Scholar]
- Alhassan, A.M.; Zainon, W.M.N.W. Brain tumor classification in magnetic resonance image using hard swish-based RELU activation function-convolutional neural network. Neural Comput. Appl. 2021, 33, 9075–9087. [Google Scholar] [CrossRef]
- Bulla, P.; Anantha, L.; Peram, S. Deep Neural Networks with Transfer Learning Model for Brain Tumors Classification. Traitement Du Signal 2020, 37, 593–601. [Google Scholar] [CrossRef]
- Ghassemi, N.; Shoeibi, A.; Rouhani, M. Deep neural network with generative adversarial networks pre-training for brain tumor classification based on MR images. Biomed. Signal Process. Control 2020, 57, 101678. [Google Scholar] [CrossRef]
- Kakarla, J.; Isunuri, B.V.; Doppalapudi, K.S.; Bylapudi, K.S.R. Three-class classification of brain magnetic resonance images using average-pooling convolutional neural network. Int. J. Imaging Syst. Technol. 2021, 31, 1731–1740. [Google Scholar] [CrossRef]
- Noreen, N.; Palaniappan, S.; Qayyum, A.; Ahmad, I.; Alassafi, M.O. Brain Tumor Classification Based on Fine-Tuned Models and the Ensemble Method. Cmc-Comput. Mater. Contin. 2021, 67, 3967–3982. [Google Scholar] [CrossRef]
- Noreen, N.; Palaniappan, S.; Qayyum, A.; Ahmad, I.; Imran, M.; Shoaib, M. A deep learning model based on concatenation approach for the diagnosis of brain tumor. IEEE Access 2020, 8, 55135–55144. [Google Scholar] [CrossRef]
- Kumar, R.L.; Kakarla, J.; Isunuri, B.V.; Singh, M. Multi-class brain tumor classification using residual network and global average pooling. Multimed. Tools Appl. 2021, 80, 13429–13438. [Google Scholar] [CrossRef]
- Badža, M.M.; Barjaktarović, M.Č. Classification of brain tumors from MRI images using a convolutional neural network. Appl. Sci. 2020, 10, 1999. [Google Scholar] [CrossRef]
- Alaraimi, S.; Okedu, K.E.; Tianfield, H.; Holden, R.; Uthmani, O. Transfer learning networks with skip connections for classification of brain tumors. Int. J. Imaging Syst. Technol. 2021, 31, 1564–1582. [Google Scholar] [CrossRef]
- Lo, C.M.; Chen, Y.C.; Weng, R.C.; Hsieh, K.L.C. Intelligent glioma grading based on deep transfer learning of MRI radiomic features. Appl. Sci. 2019, 9, 4926. [Google Scholar] [CrossRef]
- Kurc, T.; Bakas, S.; Ren, X.; Aditya, B.; Alexandre, M.; Huang, Y.; Zhang, L.; Ashish, K.; Marc, T.; Qi, Q.; et al. Segmentation and classification in digital pathology for glioma research: Challenges and deep learning approaches. Front. Neurosci. 2020, 14, 27. [Google Scholar] [CrossRef]
- Pei, L.; Vidyaratne, L.; Rahman, M.M.; Iftekharuddin, K.M. Context aware deep learning for brain tumor segmentation, subtype classification, and survival prediction using radiology images. Sci. Rep. 2020, 10, 19726. [Google Scholar] [CrossRef] [PubMed]
- McAvoy, M.; Prieto, P.C.; Kaczmarzyk, J.R.; Fernández, I.S.; McNulty, J.; Smith, T. Classification of glioblastoma versus primary central nervous system lymphoma using convolutional neural networks. Sci. Rep. 2021, 11, 15219. [Google Scholar] [CrossRef] [PubMed]
- Gilanie, G.; Bajwa, U.I.; Waraich, M.M.; Anwar, M.W. Risk-free WHO grading of astrocytoma using convolutional neural networks from MRI images. Multimed. Tools Appl. 2021, 80, 4295–4306. [Google Scholar] [CrossRef]
- Kulkarni, S.M.; Sundari, G. Comparative Analysis of Performance of Deep CNN Based Framework for Brain Mri Classification Using Transfer Learning. J. Eng. Sci. Technol. 2021, 16, 2901–2917. [Google Scholar]
- Artzi, M.; Redmard, E.; Tzemach, O.; Zeltser, J.; Gropper, O.; Roth, J.; Shofty, B.; Kozyrev, D.A.; Constantini, S.; Sira, L.B. Classification of pediatric posterior fossa tumors using convolutional neural network and tabular data. IEEE Access 2021, 9, 91966–91973. [Google Scholar] [CrossRef]
- Tariciotti, L.; Caccavella, V.M.; Fiore, G.; Schisano, L.; Carrabba, G.; Borsa, S.; Giordano, M.; Palmisciano, P.; Remoli, G.; Remore, L.G.; et al. A Deep Learning Model for Preoperative Differentiation of Glioblastoma, Brain Metastasis and Primary Central Nervous System Lymphoma: A Pilot Study. Front. Oncol. 2022, 12, 816638. [Google Scholar] [CrossRef]
- Ait Amou, M.; Xia, K.; Kamhi, S.; Mouhafid, M. A Novel MRI Diagnosis Method for Brain Tumor Classification Based on CNN and Bayesian Optimization. Healthcare 2022, 10, 494. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, M.F.; Ali, M.U.; Hussain, S.J.; Zafar, A.; Mohatram, M.; Irfan, M.; AlRuwaili, R.; Alruwaili, M.; Ali, N.H.; Albarrak, A.M.; et al. Brain tumor/mass classification framework using magnetic-resonance-imaging-based isolated and developed transfer deep-learning model. Sensors 2022, 22, 372. [Google Scholar] [CrossRef]
- Ye, N.; Yang, Q.; Chen, Z.; Teng, C.; Liu, P.; Liu, X.; Xiong, Y.; Lin, X.; Li, S.; Li, X. Classification of Gliomas and Germinomas of the Basal Ganglia by Transfer Learning. Front. Oncol. 2022, 12, 844197. [Google Scholar] [CrossRef]
- Gaur, L.; Bhandari, M.; Razdan, T.; Mallik, S.; Zhao, Z. Explanation-Driven Deep Learning Model for Prediction of Brain Tumour Status Using MRI Image Data. Front. Genet. 2022, 13, 822666. [Google Scholar] [CrossRef]
- Guo, S.; Wang, L.; Chen, Q.; Wang, L.; Zhang, J.; Zhu, Y. Multimodal MRI Image Decision Fusion-Based Network for Glioma Classification. Front. Oncol. 2022, 12, 819673. [Google Scholar] [CrossRef]
- Aamir, M.; Rahman, Z.; Dayo, Z.A.; Abro, W.A.; Uddin, M.I.; Khan, I.; Imran, A.S.; Ali, Z.; Ishfaq, M.; Guan, Y.; et al. A deep learning approach for brain tumor classification using MRI images. Comput. Electr. Eng. 2022, 101, 108105. [Google Scholar] [CrossRef]
- Rizwan, M.; Shabbir, A.; Javed, A.R.; Shabbir, M.; Baker, T.; Obe, D.A.J. Brain tumor and glioma grade classification using gaussian convolutional neural network. IEEE Access 2022, 10, 29731–29740. [Google Scholar] [CrossRef]
- Nayak, D.R.; Padhy, N.; Mallick, P.K.; Zymbler, M.; Kumar, S. Brain Tumor Classification Using Dense Efficient-Net. Axioms 2022, 11, 34. [Google Scholar] [CrossRef]
- Chatterjee, S.; Nizamani, F.A.; Nürnberger, A.; Speck, O. Classification of brain tumours in MR images using deep spatiospatial models. Sci. Rep. 2022, 12, 1505. [Google Scholar] [CrossRef] [PubMed]
- Khazaee, Z.; Langarizadeh, M.; Ahmadabadi, M.E.S. Developing an Artificial Intelligence Model for Tumor Grading and Classification, Based on MRI Sequences of Human Brain Gliomas. Int. J. Cancer Manag. 2022, 15, e120638. [Google Scholar] [CrossRef]
- Isunuri, B.V.; Kakarla, J. Three-class brain tumor classification from magnetic resonance images using separable convolution based neural network. Concurr. Comput. Pract. Exp. 2022, 34, e6541. [Google Scholar] [CrossRef]
- Rajini, N.H. Brain tumor image classification and grading using convolutional neural network and particle swarm optimization algorithm. Int. J. Eng. Adv. Technol. (IJEAT) 2019, 8, 2249–8958. [Google Scholar]
- Anaraki, A.K.; Ayati, M.; Kazemi, F. Magnetic resonance imaging-based brain tumor grades classification and grading via convolutional neural networks and genetic algorithms. Biocybern. Biomed. Eng. 2019, 39, 63–74. [Google Scholar] [CrossRef]
- Wahlang, I.; Sharma, P.; Sanyal, S.; Saha, G.; Maji, A.K. Deep learning techniques for classification of brain MRI. Int. J. Intell. Syst. Technol. Appl. 2020, 19, 571–588. [Google Scholar] [CrossRef]
- Tandel, G.S.; Tiwari, A.; Kakde, O.G. Performance optimisation of deep learning models using majority voting algorithm for brain tumour classification. Comput. Biol. Med. 2021, 135, 104564. [Google Scholar] [CrossRef] [PubMed]
- Bento, M.; Fantini, I.; Park, J.; Rittner, L.; Frayne, R. Deep Learning in Large and Multi-Site Structural Brain MR Imaging Datasets. Front. Neuroinform. 2022, 15, 805669. [Google Scholar] [CrossRef] [PubMed]
- Thompson, N.C.; Greenewald, K.; Lee, K.; Manso, G.F. The Computational Limits of Deep Learning. arXiv 2020, arXiv:2007.05558. [Google Scholar]
- Goodkin, O.; Pemberton, H.; Vos, S.B.; Prados, F.; Sudre, C.H.; Moggridge, J.; Cardoso, M.J.; Ourselin, S.; Bisdas, S.; White, M.; et al. The quantitative neuroradiology initiative framework: Application to dementia. Br. J. Radiol. 2019, 92, 20190365. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Li, O.; Tao, D.; Barnett, A.; Rudin, C.; Su, J.K. This looks like that: Deep learning for interpretable image recognition. Adv. Neural Inf. Process. Syst. 2019, 32, 8930–8941. [Google Scholar]
- Barnett, A.J.; Schwartz, F.R.; Tao, C.; Chen, C.; Ren, Y.; Lo, J.Y.; Rudin, C. A case-based interpretable deep learning model for classification of mass lesions in digital mammography. Nat. Mach. Intell. 2021, 3, 1061–1070. [Google Scholar] [CrossRef]
- Singh, G.; Yow, K.C. An interpretable deep learning model for COVID-19 detection with chest X-ray images. IEEE Access 2021, 9, 85198–85208. [Google Scholar] [CrossRef]
- Kim, E.; Kim, S.; Seo, M.; Yoon, S. XProtoNet: Diagnosis in chest radiography with global and local explanations. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Virtual, 19–25 June 2021; pp. 15719–15728. [Google Scholar]
- Mohammadjafari, S.; Cevik, M.; Thanabalasingam, M.; Basar, A. Using ProtoPNet for interpretable Alzheimer’s disease classification. In Proceedings of the 34th Canadian Conference on Artificial Intelligence, Vancouver, BC, Canada, 25–28 May 2021. [Google Scholar]














| PubMed /Scopus | (deep learning OR deep model OR artificial intelligence OR artificial neural network OR autoencoder OR generative adversarial network) OR convolutional OR (neural network) OR neural network OR deep model OR convolutional) | AND |
| (brain tumor OR glioma OR brain cancer OR glioblastoma OR astrocytoma OR oligodendroglioma OR ependymoma) | AND | |
| (classification OR grading OR classify) | AND | |
| (MRI OR Magnetic Resonance OR MR images OR radiographic OR radiology) | IN | |
| Title/Abstract |
| Sequence | Sequence Characteristics | Main Clinical Distinctions | Example * |
|---|---|---|---|
| T1w | Uses short TR and TE [64] |  | |
| T2w | Uses long TR and TE [64] |  | |
| ceT1w | Uses the same TR and TE as T1w; employs contrast agents [64] |
|  |
| FLAIR | Uses very long TR and TE; the inversion time nulls the signal from fluid [67] |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.; Zaccagna, F.; Rundo, L.; Testa, C.; Agati, R.; Lodi, R.; Manners, D.N.; Tonon, C. Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives. Diagnostics 2022, 12, 1850. https://doi.org/10.3390/diagnostics12081850
Xie Y, Zaccagna F, Rundo L, Testa C, Agati R, Lodi R, Manners DN, Tonon C. Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives. Diagnostics. 2022; 12(8):1850. https://doi.org/10.3390/diagnostics12081850
Chicago/Turabian StyleXie, Yuting, Fulvio Zaccagna, Leonardo Rundo, Claudia Testa, Raffaele Agati, Raffaele Lodi, David Neil Manners, and Caterina Tonon. 2022. "Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives" Diagnostics 12, no. 8: 1850. https://doi.org/10.3390/diagnostics12081850
APA StyleXie, Y., Zaccagna, F., Rundo, L., Testa, C., Agati, R., Lodi, R., Manners, D. N., & Tonon, C. (2022). Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives. Diagnostics, 12(8), 1850. https://doi.org/10.3390/diagnostics12081850