
Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration in the Diagnosis of Focal Liver Lesions: Prospective Head-to-Head Comparison

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Data Collection
2.2. Study Outcome and Definitions
2.3. Procedure
2.4. Preparation of Samples
2.5. Statistics
3. Results
3.1. Participant Characteristics
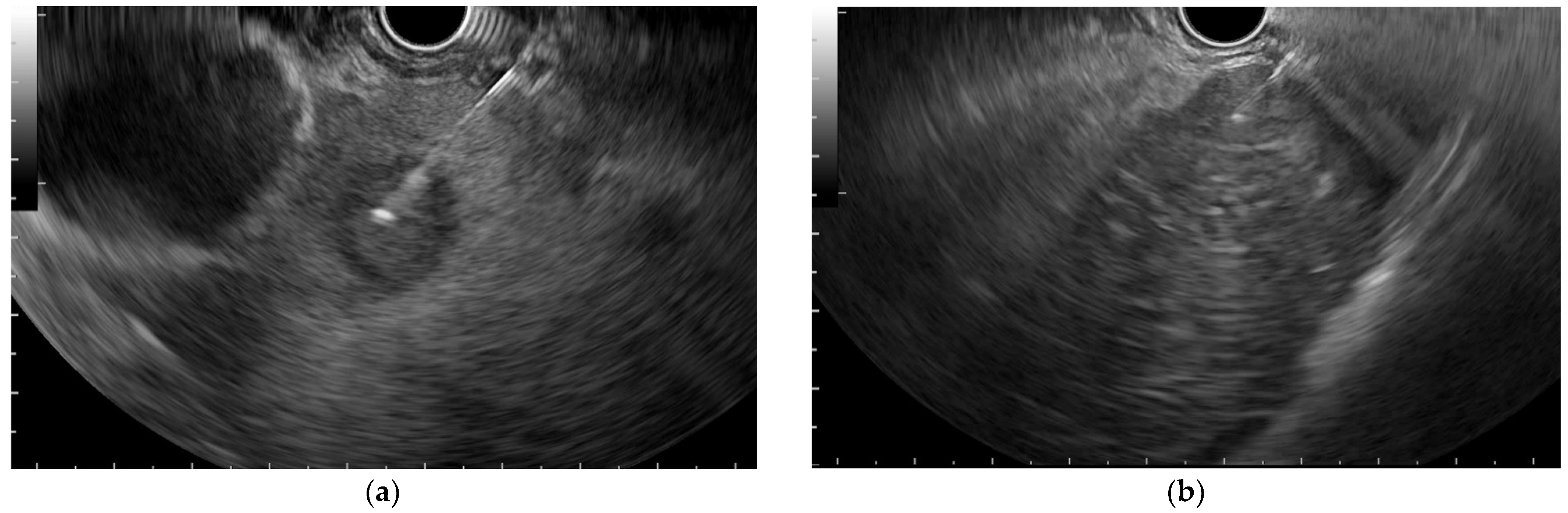
3.2. B-Mode EUS Assessment
3.3. Diagnostic Yields in EUS-FNA Compared to EUS-FNA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edelson, J.C.; Mitchell, N.E.; Rockey, D.C. Endohepatology—Current status. Curr. Opin. Gastroenterol. 2022, 38, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Pouw, R.E.; Barret, M.; Biermann, K.; Bisschops, R.; Czakó, L.; Gecse, K.B.; de Hertogh, G.; Hucl, T.; Iacucci, M.; Jansen, M.; et al. Endoscopic tissue sampling—Part 1: Upper gastrointestinal and hepatopancreatobiliary tracts. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53, 1174–1188. [Google Scholar] [CrossRef] [PubMed]
- Shuja, A.; Alkhasawneh, A.; Fialho, A.; Fialho, A.; Shukri, A.; Harris, C.; Smotherman, C.; Malespin, M.; de Melo, S.W., Jr. Comparison of EUS-guided versus percutaneous and transjugular approaches for the performance of liver biopsies. Dig. Liver Dis. 2019, 51, 826–830. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.P.; Shakhatreh, M.; Garg, R.; Ponnada, S.; Adler, D.G. Efficacy and safety of EUS-guided liver biopsy: A systematic review and meta-analysis. Gastrointest. Endosc. 2019, 89, 238–246.e3. [Google Scholar] [CrossRef]
- Baran, B.; Kale, S.; Patil, P.; Kannadath, B.; Ramireddy, S.; Badillo, R.; DaVee, R.T.; Thosani, N. Endoscopic ultrasound-guided parenchymal liver biopsy: A systematic review and meta-analysis. Surg. Endosc. 2021, 35, 5546–5557. [Google Scholar] [CrossRef]
- Fryer, E.; Wang, L.M.; Verrill, C.; Fleming, K. How often do our liver core biopsies reach current definitions of adequacy? J. Clin. Pathol. 2013, 66, 1087–1089. [Google Scholar] [CrossRef]
- Ching-Companioni, R.A.; Diehl, D.L.; Johal, A.S.; Confer, B.D.; Khara, H.S. 19 G aspiration needle versus 19 G core biopsy needle for endoscopic ultrasound-guided liver biopsy: A prospective randomized trial. Endoscopy 2019, 51, 1059–1065. [Google Scholar] [CrossRef]
- Mok, S.; Diehl, D.L.; Johal, A.S.; Khara, H.S.; Confer, B.D.; Mudireddy, P.R.; Kovach, A.H.; Diehl, M.M.; Kirchner, H.L.; Chen, Z.E. Endoscopic ultrasound-guided biopsy in chronic liver disease: A randomized comparison of 19-G FNA and 22-G FNB needles. Endosc. Int. Open 2019, 7, E62–E71. [Google Scholar] [CrossRef]
- Akay, E.; Atasoy, D.; Altınkaya, E.; Koç, A.; Ertan, T.; Karaman, H.; Caglar, E. Endoscopic Ultrasound-Guided Fine Needle Aspiration Using a 22G Needle for Hepatic Lesions: Single-Center Experience. Clin. Endosc. 2021, 54, 404–412. [Google Scholar] [CrossRef]
- Oh, D.; Seo, D.W.; Hong, S.M.; Jun, J.H.; Song, T.J.; Park, D.H.; Son, B.K.; Lee, S.S.; Lee, S.K.; Kim, M.H. The usefulness of contrast-enhanced harmonic EUS-guided fine-needle aspiration for evaluation of hepatic lesions (with video). Gastrointest. Endosc. 2018, 88, 495–501. [Google Scholar] [CrossRef]
- Lee, Y.N.; Moon, J.H.; Kim, H.K.; Choi, H.J.; Choi, M.H.; Kim, D.C.; Lee, T.H.; Lee, T.H.; Cha, S.W.; Kim, S.G.; et al. Usefulness of endoscopic ultrasound-guided sampling using core biopsy needle as a percutaneous biopsy rescue for diagnosis of solid liver mass: Combined histological-cytological analysis. J. Gastroenterol. Hepatol. 2015, 30, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Bao, H.; Deng, Z.; Zhao, Q.; Tian, G.; Jiang, T.A. Endoscopic ultrasound-guided sampling using core biopsy needle for diagnosis of left-lobe hepatocellular carcinoma in patients with underlying cirrhosis. J. Cancer Res. Ther. 2020, 16, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Chon, H.K.; Yang, H.C.; Choi, K.H.; Kim, T.H. Endoscopic Ultrasound-Guided Liver Biopsy Using a Core Needle for Hepatic Solid Mass. Clin. Endosc. 2019, 52, 340–346. [Google Scholar] [CrossRef]
- Lee, B.S.; Cho, C.M.; Jung, M.K.; Jang, J.S.; Bae, H.I. Comparison of Histologic Core Portions Acquired from a Core Biopsy Needle and a Conventional Needle in Solid Mass Lesions: A Prospective Randomized Trial. Gut Liver 2017, 11, 559–566. [Google Scholar] [CrossRef] [PubMed]
- van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2021, 53, 411–423. [Google Scholar] [CrossRef]
- Iwashita, T.; Yasuda, I.; Mukai, T.; Doi, S.; Nakashima, M.; Uemura, S.; Mabuchi, M.; Shimizu, M.; Hatano, Y.; Hara, A.; et al. Macroscopic on-site quality evaluation of biopsy specimens to improve the diagnostic accuracy during EUS-guided FNA using a 19-gauge needle for solid lesions: A single-center prospective pilot study (MOSE study). Gastrointest. Endosc. 2015, 81, 177–185. [Google Scholar] [CrossRef]
- Mangiavillano, B.; Frazzoni, L.; Togliani, T.; Fabbri, C.; Tarantino, I.; De Luca, L.; Staiano, T.; Binda, C.; Signoretti, M.; Eusebi, L.H.; et al. Macroscopic on-site evaluation (MOSE) of specimens from solid lesions acquired during EUS-FNB: Multicenter study and comparison between needle gauges. Endosc. Int. Open 2021, 9, E901–E906. [Google Scholar] [CrossRef]
- Mohan, B.P.; Madhu, D.; Reddy, N.; Sordi Chara, B.; Khan, S.R.; Garg, G.; Kassab, L.L.; Muthusamy, A.K.; Singh, A.; Chandan, S.; et al. Diagnostic accuracy of endoscopic ultrasound (EUS) guided fine needle biopsy (FNB) by macroscopic on-site evaluation (MOSE): A systematic review and meta-analysis. Gastrointest Endosc. 2022. [Google Scholar] [CrossRef]
- Gerke, H.; Rizk, M.K.; Vanderheyden, A.D.; Jensen, C.S. Randomized study comparing endoscopic ultrasound-guided Trucut biopsy and fine needle aspiration with high suction. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2010, 21, 44–51. [Google Scholar] [CrossRef]
- Mitchell, A.J. Sensitivity×PPV is a recognized test called the clinical utility index (CUI+). Eur. J. Epidemiol. 2011, 26, 251–252. [Google Scholar] [CrossRef] [Green Version]
- Goldhoff, P.E.; Vohra, P.; Kolli, K.P.; Ljung, B.M. Fine-Needle Aspiration Biopsy of Liver Lesions Yields Higher Tumor Fraction for Molecular Studies: A Direct Comparison with Concurrent Core Needle Biopsy. J. Natl. Compr. Cancer Netw. JNCCN 2019, 17, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Crinò, S.F.; Ramai, D.; Fabbri, C.; Mangiavillano, B.; Lisotti, A.; Muscatiello, N.; Cotsoglou, C.; Fusaroli, P. Diagnostic yield of endoscopic ultrasound-guided liver biopsy in comparison to percutaneous liver biopsy: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.K.; Saxena, R.; Rush, N.; Patel, S.K.; Dasari, C.S.; Mneimneh, W.; Quickery, A.; Rahal, M.A.; Temnykh, L.; DeWitt, J.; et al. A Comparative Study of 22G versus 19G Needles for EUS-Guided Biopsies for Parenchymal Liver Disease: Are Thinner Needles Better? Dig. Dis. Sci. 2021, 66, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.K.; Kadkhodayan, K.; Idrisov, E.; Ali, S.; Rafiq, E.; Ben-Ami Shor, D.; Abdel-Jalil, A.; Navaneethan, U.; Bang, J.; Varadarajulu, S.; et al. Endoscopic ultrasound-guided liver biopsy using a 22-G fine needle biopsy needle: A prospective study. Endoscopy 2019, 51, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Nieto, J.; Dawod, E.; Deshmukh, A.; Penn, E.; Adler, D.; Saab, S. EUS-guided fine-needle core liver biopsy with a modified one-pass, one-actuation wet suction technique comparing two types of EUS core needles. Endosc. Int. Open 2020, 8, E938–E943. [Google Scholar] [CrossRef]
- Platt, K.D.; Schulman, A.R. Closing in on an optimal EUS-guided liver biopsy technique… but when should we use it? Gastrointest. Endosc. 2021, 94, 559–561. [Google Scholar] [CrossRef]
- Zeng, K.; Jiang, Z.; Yang, J.; Chen, K.; Lu, Q. Role of endoscopic ultrasound-guided liver biopsy: A meta-analysis. Scand. J. Gastroenterol. 2022, 57, 545–557. [Google Scholar] [CrossRef]
- Dhar, J.; Samanta, J. Role of endoscopic ultrasound in the field of hepatology: Recent advances and future trends. World J. Hepatol. 2021, 13, 1459–1483. [Google Scholar] [CrossRef]
- Takano, Y.; Noda, J.; Yamawaki, M.; Azami, T.; Kobayashi, T.; Niiya, F.; Maruoka, N.; Norose, T.; Ohike, N.; Wakabayashi, T.; et al. Comparative Study of an Ultrasound-guided Percutaneous Biopsy and Endoscopic Ultrasound-guided Fine-needle Aspiration for Liver Tumors. Intern. Med. 2021, 60, 1657–1664. [Google Scholar] [CrossRef]
- Aggarwal, S.N.; Magdaleno, T.; Klocksieben, F.; MacFarlan, J.E.; Goonewardene, S.; Zator, Z.; Shah, S.; Shah, H.N. A prospective, head-to-head comparison of 2 EUS-guided liver biopsy needles in vivo. Gastrointest. Endosc. 2021, 93, 1133–1138. [Google Scholar] [CrossRef]
- Kongkam, P.; Nalinthassanai, N.; Prueksapanich, P.; Sanpavat, A.; Cañones, A.R.; Luangsukrerk, T.; Angsuwatcharakon, P.; Ridtitid, W.; Kullavanijaya, P.; Treeprasertsuk, S.; et al. A comparison of the antegrade core trap and reverse bevel needles for EUS-guided fine-needle biopsy sampling of liver mass: A prospective randomized cross over study. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2022, 24, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Ramai, D.; Conti Bellocchi, M.C.; Bernardoni, L.; Manfrin, E.; Muscatiello, N.; Crinò, S.F. Diagnostic Yield of Endoscopic Ultrasound-Guided Liver Biopsy in Comparison to Percutaneous Liver Biopsy: A Two-Center Experience. Cancers 2021, 13, 3062. [Google Scholar] [CrossRef]
- So, H.; Seo, D.W.; Hwang, J.S.; Ko, S.W.; Oh, D.; Song, T.J.; Park, D.H.; Lee, S.K.; Kim, M.H. Macroscopic on-site evaluation after EUS-guided fine needle biopsy may replace rapid on-site evaluation. Endosc. Ultrasound 2021, 10, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Pinto, E.; Jalaj, S.; Grimm, I.S.; Baron, T.H. Impact of EUS-guided fine-needle biopsy sampling with a new core needle on the need for onsite cytopathologic assessment: A preliminary study. Gastrointest. Endosc. 2016, 84, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Crinò, S.F.; Di Mitri, R.; Nguyen, N.Q.; Tarantino, I.; de Nucci, G.; Deprez, P.H.; Carrara, S.; Kitano, M.; Shami, V.M.; Fernández-Esparrach, G.; et al. Endoscopic Ultrasound-guided Fine-needle Biopsy with or without Rapid On-site Evaluation for Diagnosis of Solid Pancreatic Lesions: A Randomized Controlled Non-Inferiority Trial. Gastroenterology 2021, 161, 899–909.e5. [Google Scholar] [CrossRef]
- Nieto, J.; Khaleel, H.; Challita, Y.; Jimenez, M.; Baron, T.H.; Walters, L.; Hathaway, K.; Patel, K.; Lankarani, A.; Herman, M.; et al. EUS-guided fine-needle core liver biopsy sampling using a novel 19-gauge needle with modified 1-pass, 1 actuation wet suction technique. Gastrointest. Endosc. 2018, 87, 469–475. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age, years | |
| mean ± SD | 60 ± 12 |
| {min to max} | {37 to 84} |
| Male sex, n (%) | 21 (70.0) |
| Mass size, cm | |
| mean ± SD | 21 ± 13 |
| Median (Q1 to Q3) | 20 (11 to 25) |
| {min to max} | {6 to 70} |
| Final diagnosis, n (%) | |
| Abscesses | 6 (20) |
| Metastasis of pancreatic adenocarcinoma | 14 (46.7) |
| Cholangiocarcinoma | 2 (6.7) |
| Hepatocarcinoma | 4 (13.3) |
| Lymphoma | 1 (3.3) |
| Metastasis of gallbladder carcinoma | 3 (10) |
| EUS-FNB (n = 30) | EUS-FNA (n = 30) | Stat. (p-Value) | |
|---|---|---|---|
| Tumor cellularity | |||
| mean ± SD | 53 ± 35 | 39 ± 34 | 2.9 (0.0039) |
| Median (Q1 to Q3) | 65 (18 to 80) | 50 (2 to 68) | |
| {min to max} | {0 to 95} | {0 to 90} | |
| Core tissue aggregate length, mm | |||
| mean ± SD | 12.1 ± 15.3 | 7.9 ± 13.7 | 2.6 (0.0085) |
| Median (Q1 to Q3) | 8 (3.9 to 15.8) | 3 (1.1 to 6.8) | |
| {min to max} | {0 to 71} | {0 to 68} | |
| Longest core tissue length, mm | |||
| mean ± SD | 2.3 ± 1.7 | 1.4 ± 1.2 | 2.5 (0.0114) |
| Median (Q1 to Q3) | 2 (1 to 3) | 1 (1 to 1.8) | |
| {min to max} | {0 to 7} | {0 to 4} | |
| Core surface, mm2 | |||
| mean ± SD | 7.1 ± 9.1 | 5 ± 8.3 | 2.4 (0.0179) |
| Median (Q1 to Q3) | 4.6 (2.3 to 8.6) | 2.1 (0.7 to 4.8) | |
| {min to max} | {0 to 42.6} | {0 to 40.8} | |
| Histology score | |||
| mean ± SD | 5 ± 1 | 4 ± 2 | 1.4 (0.1730) |
| Median (Q1 to Q3) | 5 (5 to 5) | 5 (5 to 5) | |
| {min to max} | {0 to 5} | {0 to 5} | |
| Adequate for IHC yield, no./30 (%) | 27/30 (90.0) | 19/30 (63.3) | 6.0 (0.0146) |
| Metric | EUS-FNB | EUS-FNA |
|---|---|---|
| True positives | 24 | 20 |
| True negatives | 6 | 6 |
| False negatives | 0 | 4 |
| False positives | 0 | 0 |
| Sensitivity (%) a | 100 | 83.3 [68.4 to 98.2] |
| Specificity (%) | 100 | 100 |
| Positive predictive value (%) | 100 | 100 |
| Negative predictive value (%) b | 100 | 60.0 [29.6 to 90.4] |
| Accuracy (%) c | 100 | 86.7 [74.5 to 98.8] |
| Negative likelihood | 0.17 [0.07 to 0.41] | |
| +CUI | 1 | 0.833 [0.692 to 0.975] |
| −CUI | 1 | 0.600 [0.374 to 0.826] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheorghiu, M.; Seicean, A.; Bolboacă, S.D.; Rusu, I.; Seicean, R.; Pojoga, C.; Moșteanu, O.; Sparchez, Z. Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration in the Diagnosis of Focal Liver Lesions: Prospective Head-to-Head Comparison. Diagnostics 2022, 12, 2214. https://doi.org/10.3390/diagnostics12092214
Gheorghiu M, Seicean A, Bolboacă SD, Rusu I, Seicean R, Pojoga C, Moșteanu O, Sparchez Z. Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration in the Diagnosis of Focal Liver Lesions: Prospective Head-to-Head Comparison. Diagnostics. 2022; 12(9):2214. https://doi.org/10.3390/diagnostics12092214
Chicago/Turabian StyleGheorghiu, Marcel, Andrada Seicean, Sorana D. Bolboacă, Ioana Rusu, Radu Seicean, Cristina Pojoga, Ofelia Moșteanu, and Zeno Sparchez. 2022. "Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration in the Diagnosis of Focal Liver Lesions: Prospective Head-to-Head Comparison" Diagnostics 12, no. 9: 2214. https://doi.org/10.3390/diagnostics12092214
APA StyleGheorghiu, M., Seicean, A., Bolboacă, S. D., Rusu, I., Seicean, R., Pojoga, C., Moșteanu, O., & Sparchez, Z. (2022). Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration in the Diagnosis of Focal Liver Lesions: Prospective Head-to-Head Comparison. Diagnostics, 12(9), 2214. https://doi.org/10.3390/diagnostics12092214