
Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis

 ,
,  ,
, 
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Comparators
- Patients with CE vs. non-CE: defined as patients suffering from CE (i.e., untreated or persistent after antibiotic therapy) versus those without CE (with normal endometrial histology);
- Patients with CE vs. cured CE: defined as patients suffering from CE (i.e., untreated or persistent after antibiotic therapy) versus those in which (after antibiotic therapy) endometrial biopsy showed the resolution of CE;
- Patients with cured CE vs. non-CE: defined as women with CE resolution (after antibiotic therapy) versus women without CE (with normal endometrial histology);
- Patients with CE vs. not tested for CE: defined as patients with CE (i.e., untreated or persistent after antibiotic therapy) versus those in which CE was not investigated.
2.5. Study Outcomes
- OPR/LBR: “Ongoing pregnancy” defined as a pregnancy beyond 12 weeks’ gestation; “live birth” defined as the delivery of one or more living infants;
- CPR: defined as the presence of a gestational sac on transvaginal ultrasound or other definitive clinical signs;
- MR: defined as fetal loss prior to the 20th week of gestation.
2.6. Study Selection and Data Extraction
2.7. Risk of Bias in Individual Studies
2.8. Statistical Analysis
3. Results
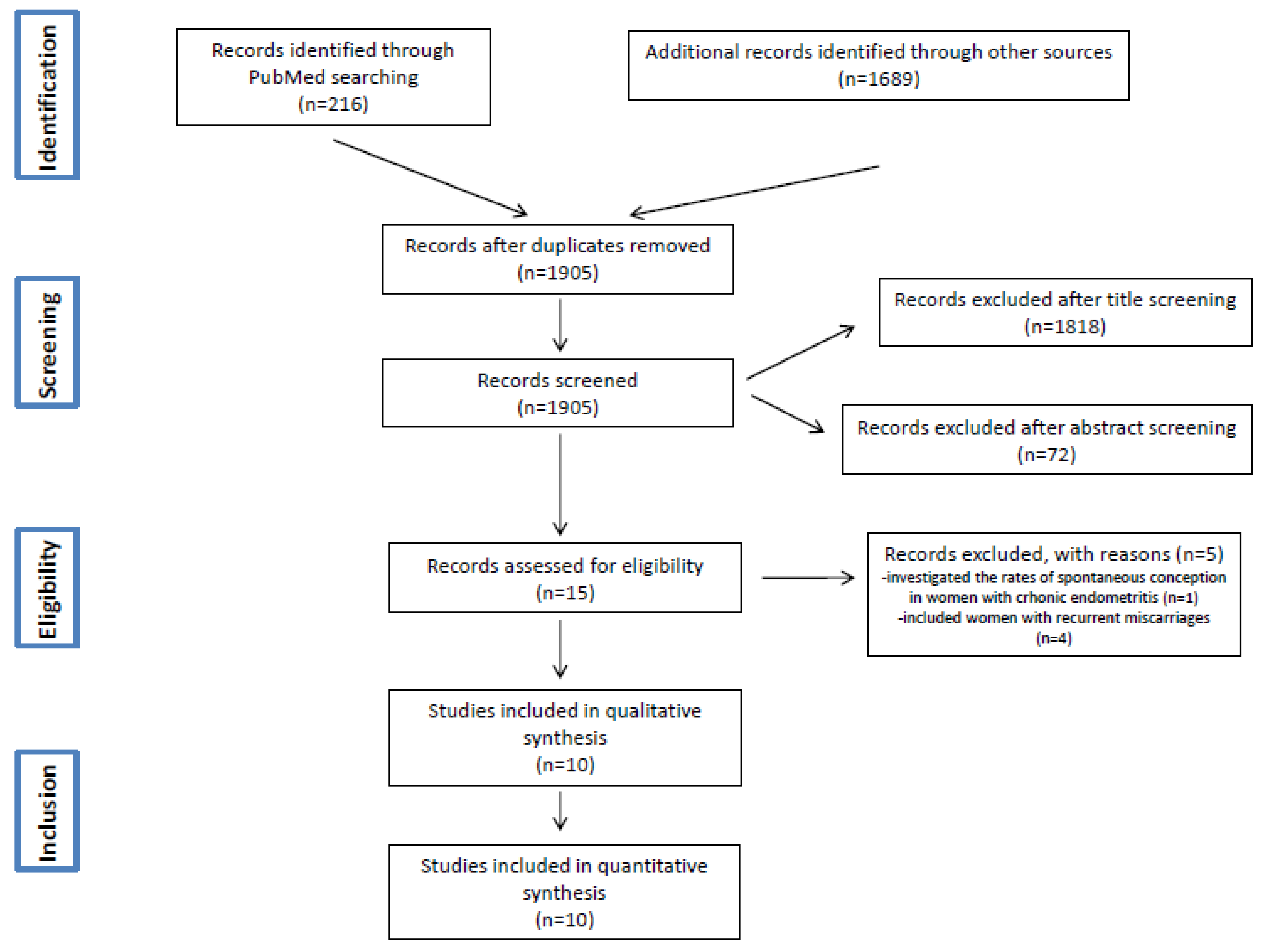
3.1. Study Selection
3.2. Included Studies
3.3. Patients
3.4. IVF-Embryo Transfer Cycle
3.5. Diagnosis of Chronic Endometritis
3.6. Therapy of Chronic Endometritis
3.7. Assessment of Study Quality and Risk of Bias
3.8. Synthesis of Results
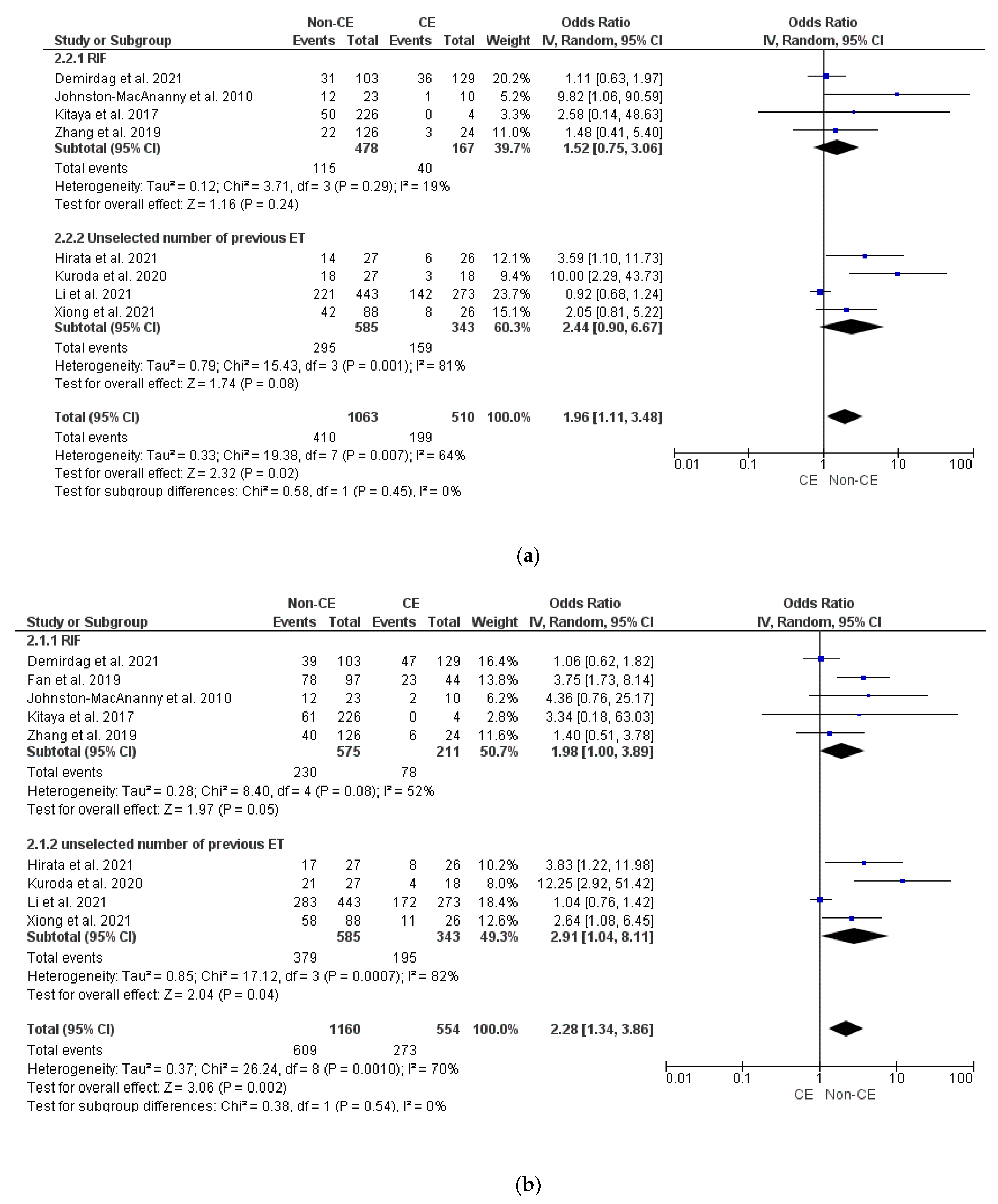
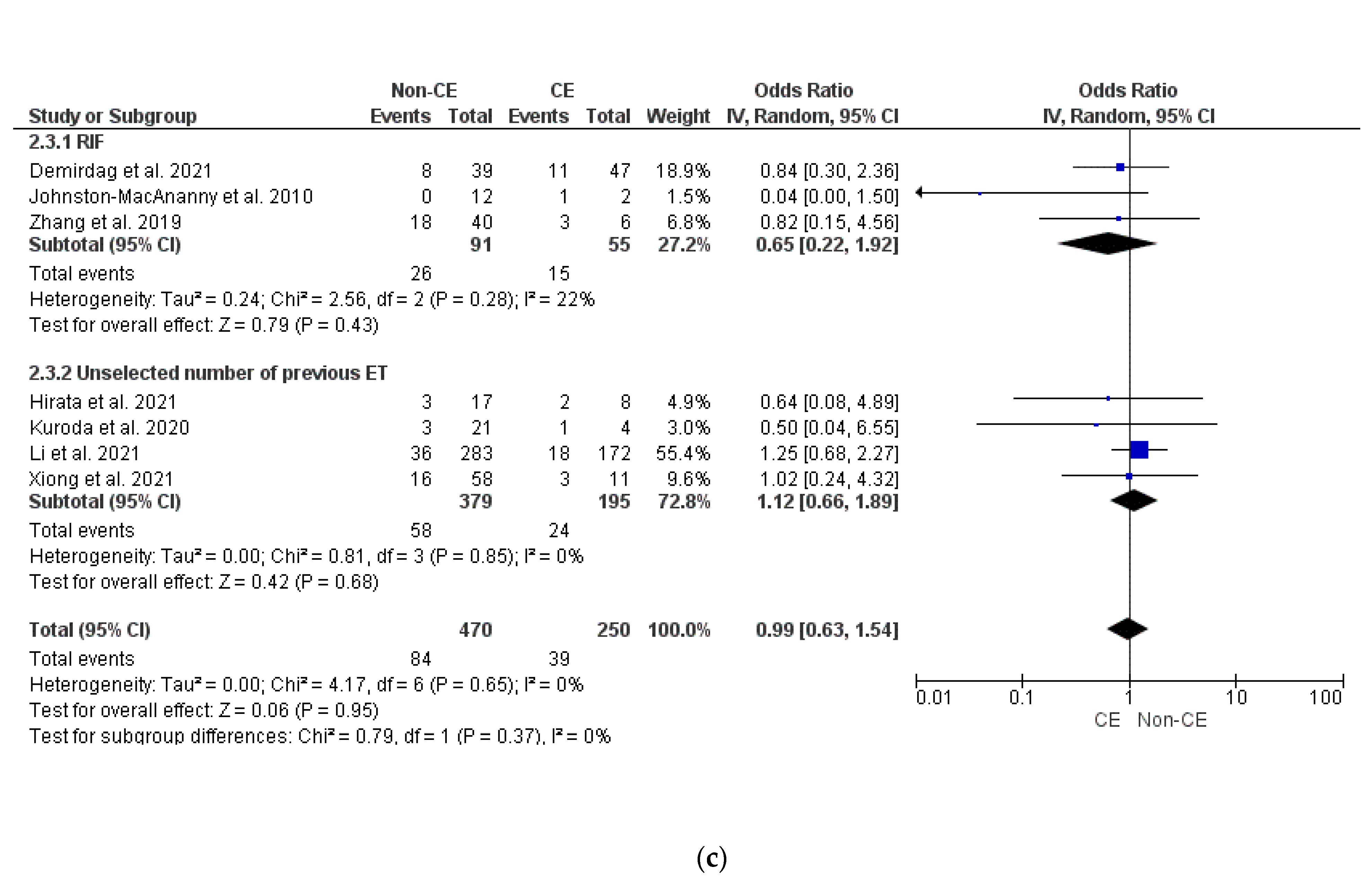
- CE vs. non-CE
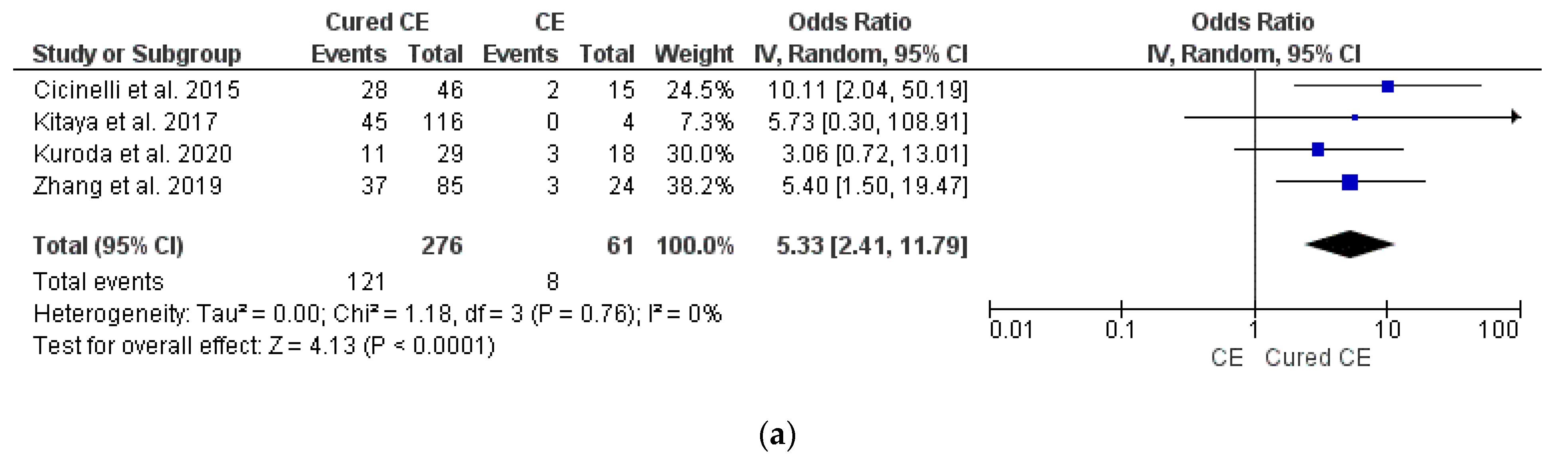
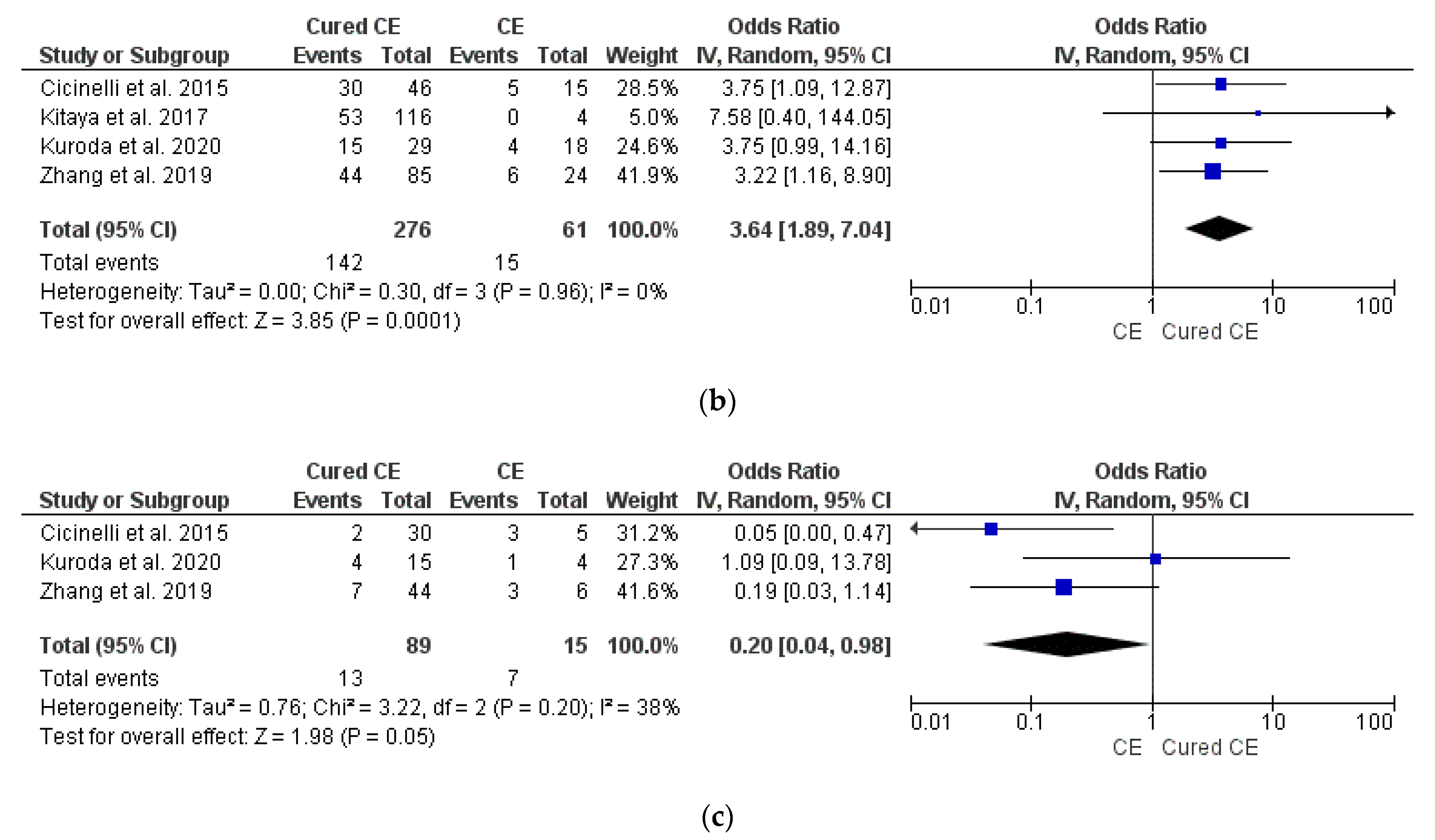
- CE vs. cured CE
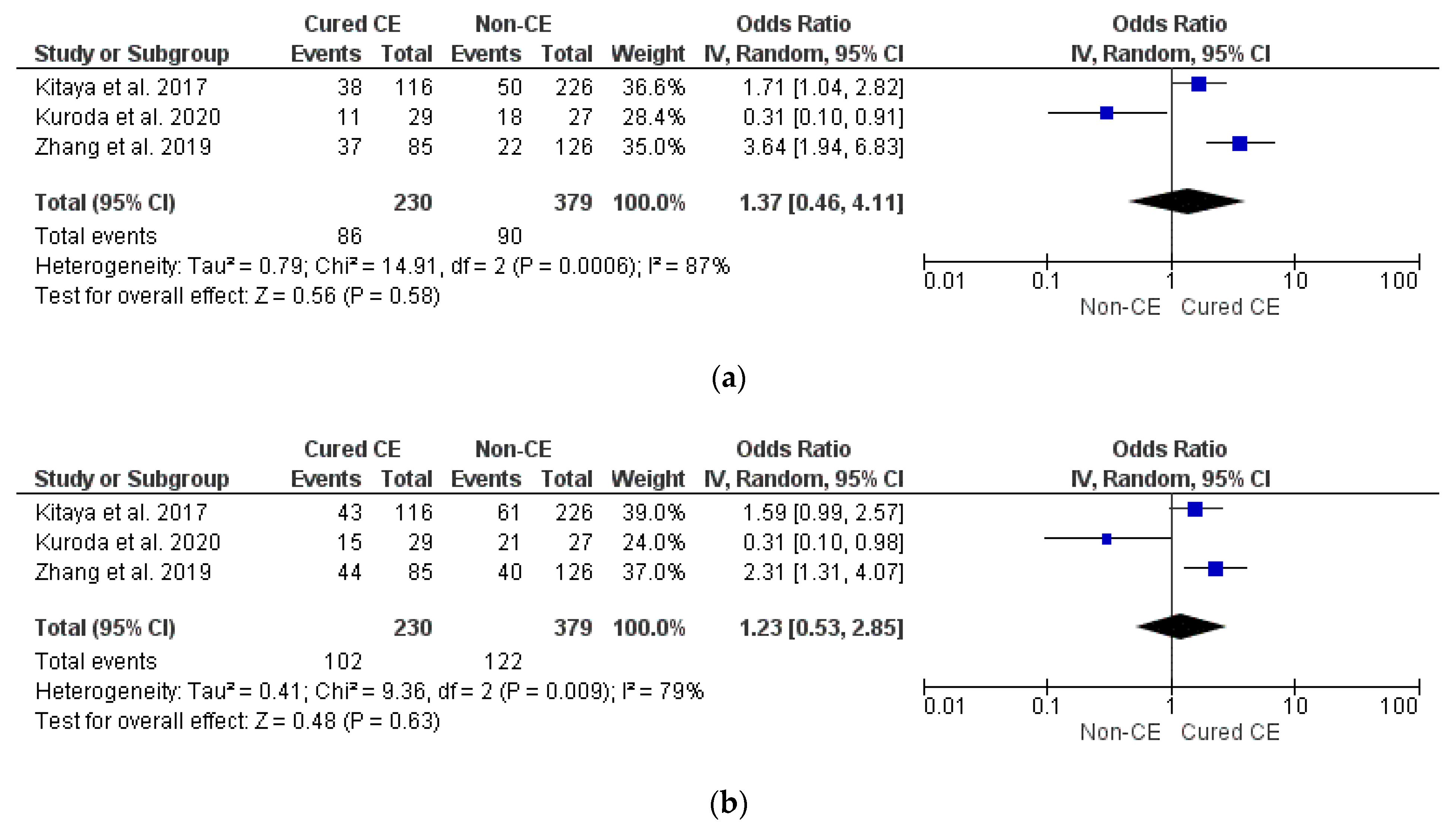
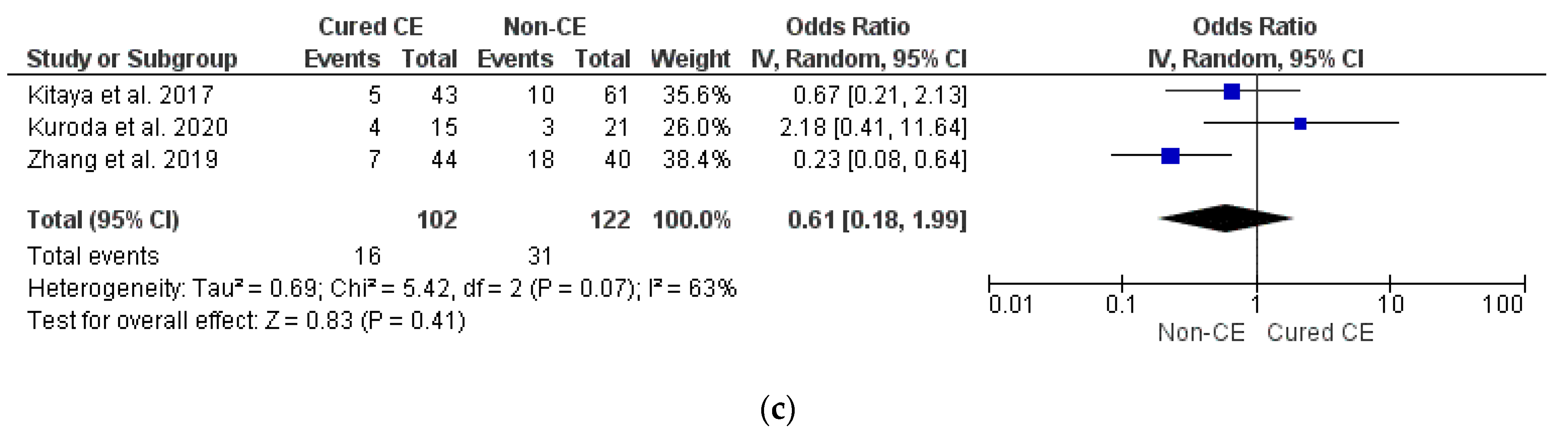
- Cured CE vs. non-CE
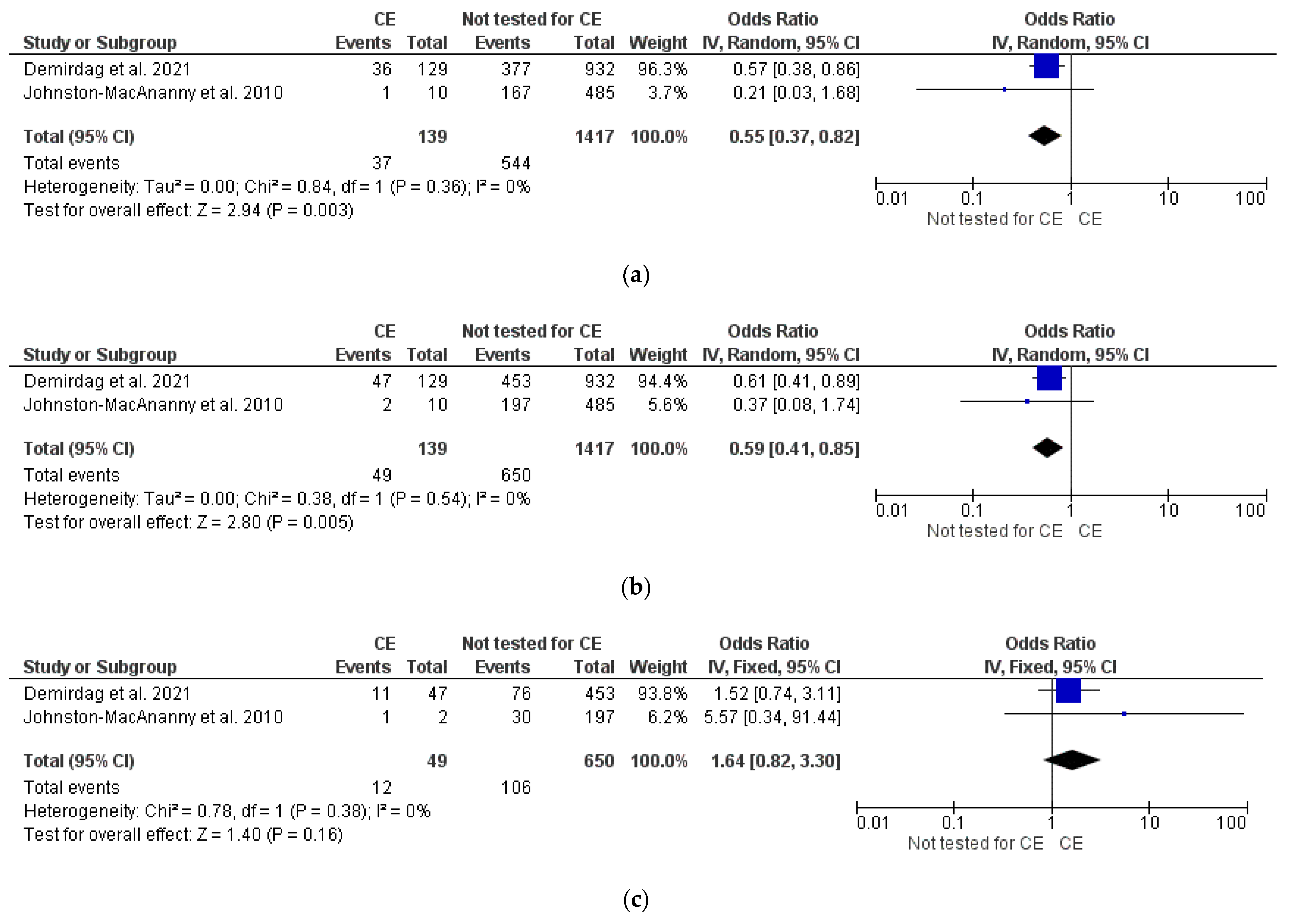
- CE vs. non-tested for CE
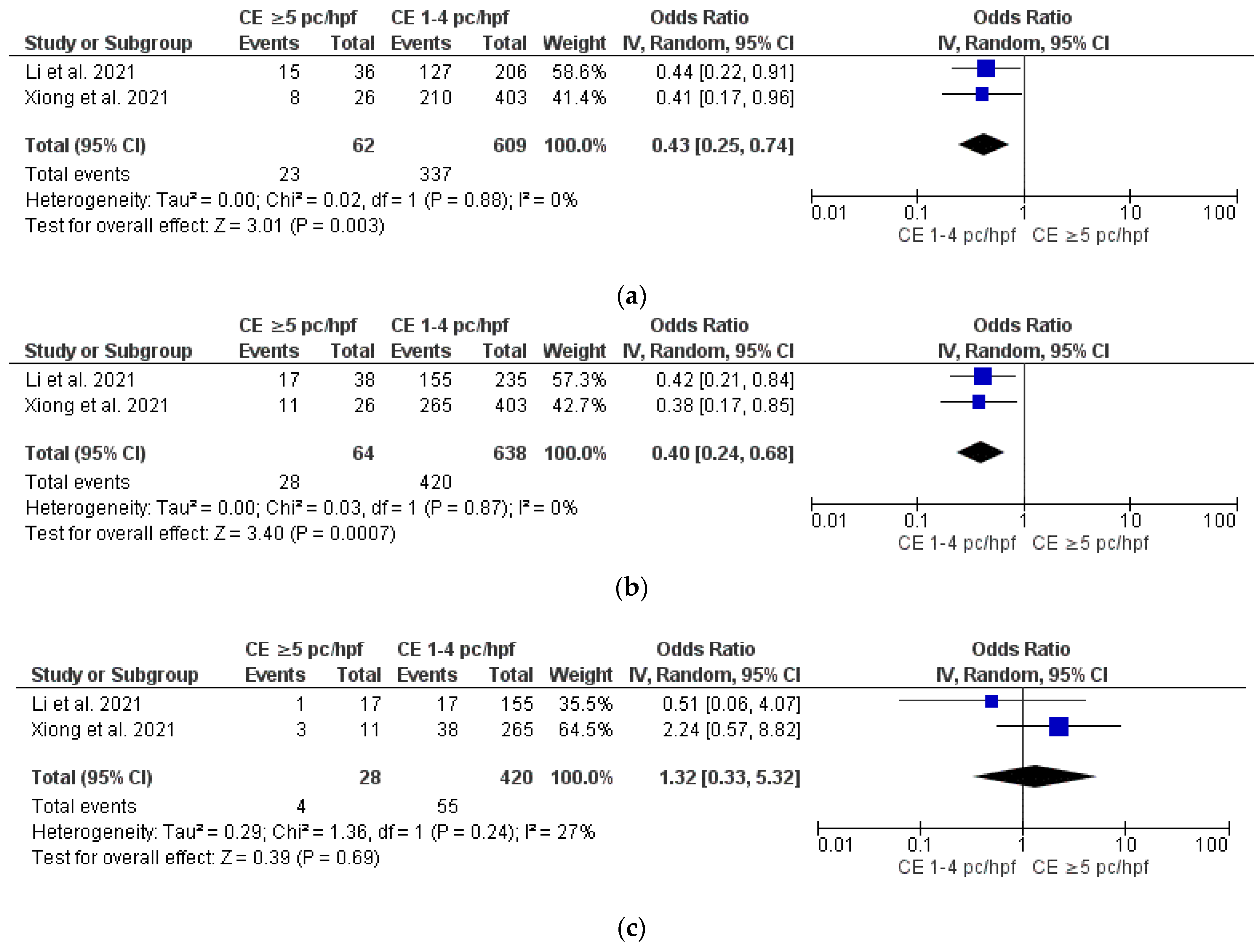
- Severe CE vs. mild CE
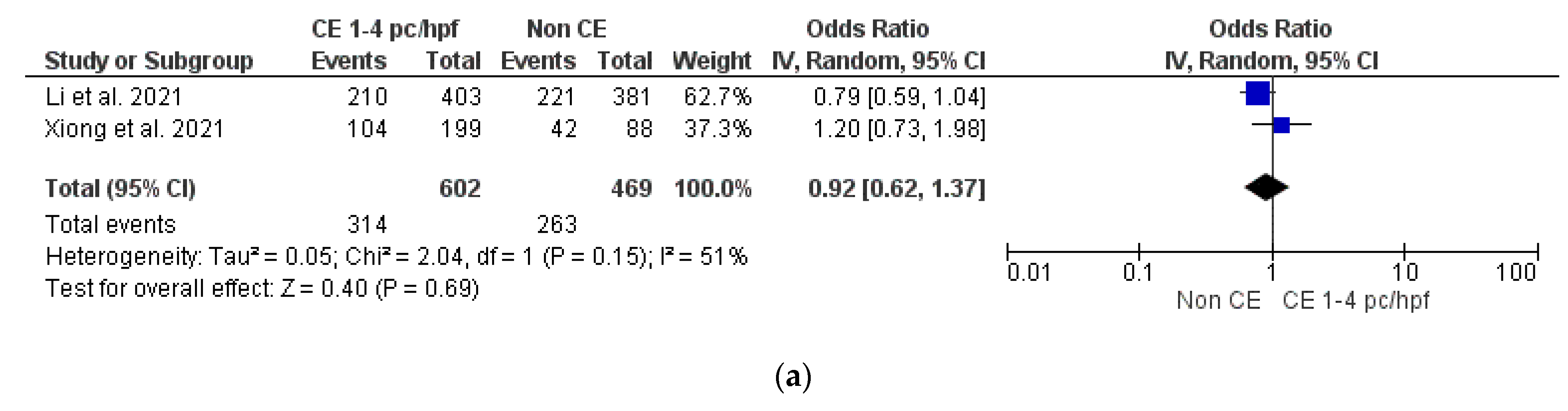
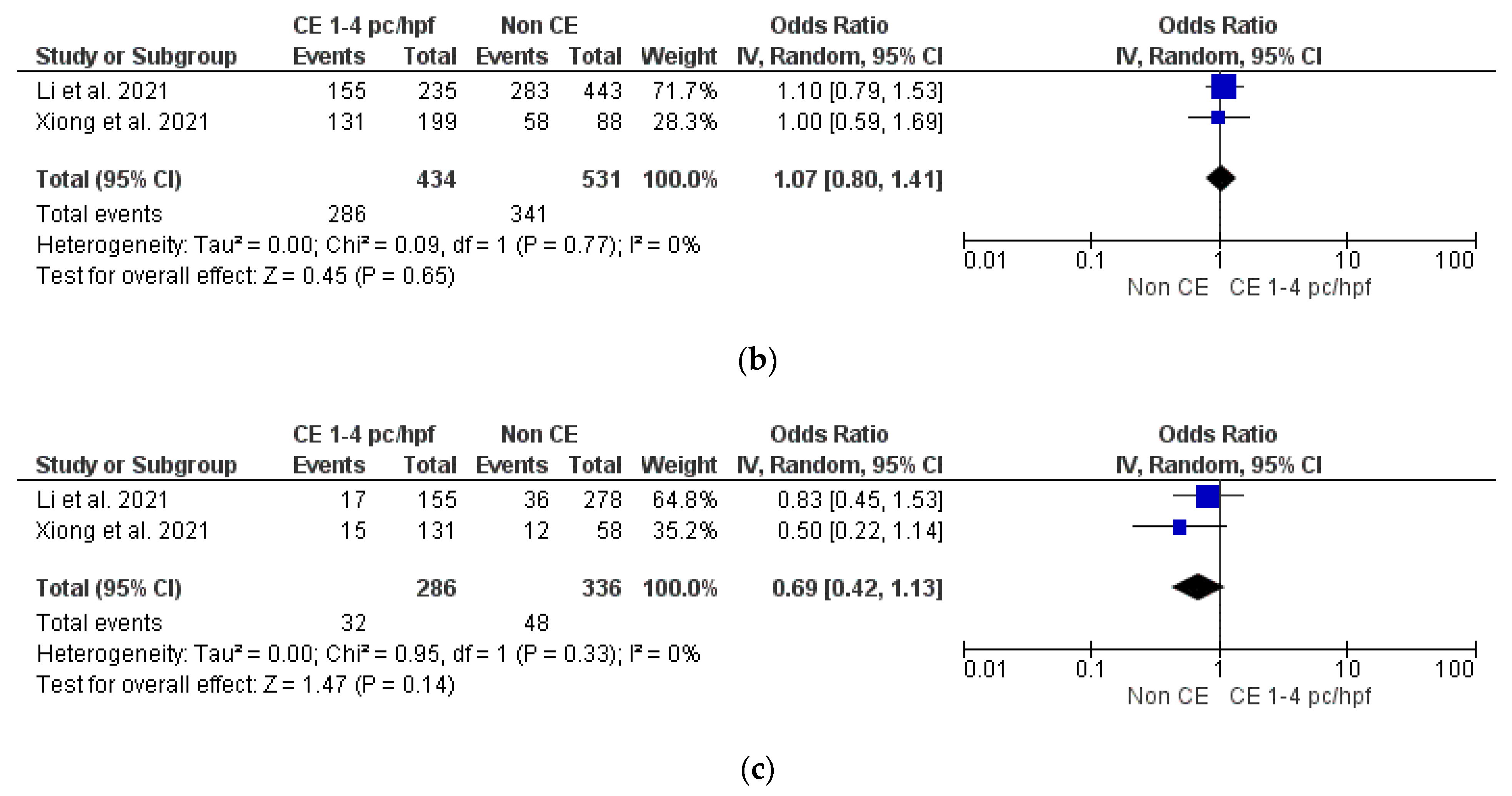
- Mild CE vs. non-CE
4. Discussion
4.1. Main Findings and Implications
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Modified Newcastle–Ottawa Scoring Items
- (1)
- Sample representativeness:
- (2)
- Sampling technique:
- (3)
- Ascertainment of chronic endometritis diagnosis:
- (4)
- Quality of population description:
- (5)
- Incomplete outcome data:
Appendix B. General Features of the Studies
| Authors and Year | Study Design, Country, and Period of Enrollment | Participants and Main Inclusion Criteria | IVF-ET Cycle | Methods | Diagnostic Criteria of CE | Groups | Outcomes |
| Cicinelli et al. 2015 [4] | Retrospective study ------ Italy ------- January 2009–June 2012 | 106 RIF patients undergoing IVF-ET cycle ------- -Unexplained infertility -Age < 40 years -At least 6 good quality embryos transferred in ≥3 previous IVF/ICSI cycles -Normal karyotype -FSH on day 3 ≤10 mUI/mL -BMI ≤ 30 kg/m2 -No previous surgery for myoma and/or endometriosis -No condition interfering with immune system -No antiphospholipid syndrome or thrombophilic condition -No antisperm antibodies | -GnRH-ant with flexible or fixed scheme -rFSH (175–225 IU/day) -U-Hcg (10,000 UI) at follicle size 17 mm (≥2). -Egg retrieval 34 h after ovulation induction -≤3 embryos transferred (of which at least one with good quality) on day 3 of culture -Luteal phase support with vaginal progesterone | -Diagnostic HSC -EB -HIS examination -Endometrial culture -Antibiotic therapy (when appropriate) -Control EB -IVF cycle | 1–5 plasma cells/HPF or discrete clusters of <20 plasma cells by CD138 staining | Group A: patients with cured CE (n = 46) Group B: patients with persistent CE (n = 15) | -Clinical pregnancy rate -Ongoing pregnancy/live birth rate -Miscarriage rate |
| Demirdag et al. 2021 [11] | Retrospective study ------ Turkey ------- September 2016–December 2019 | 1164 patients undergoing IVF-ET cycle (232 RIF) ------- -At least 4 good quality embryos transferred in ≥3 previous IVF/ICSI cycles -Age < 40 years -Normal karyotype -Normal uterine cavity -normal antiphospholipid antibody testing -no previous surgery for myoma and/or endometriosis -no male factors infertility - no autoimmune diseases, antiphospholipid antibody syndrome, endocrinological disorders | Exogenous gonadotropins, rFSH alone or with hMG - GnRH antagonist cetrorelix at follicle size ≥14 mm or E2 > 300 pg/mL -rhCG (250 mcg) at follicle size 18 mm (≥2). -Egg retrieval 36 h after ovulation induction -1 to 2 top-quality embryos transferred on day 3 or 5 -Luteal phase support with vaginal progesterone | -EB - HIS examination -Antibiotic therapy (when appropriate) -IVF cycle | ≥1 plasma cell/HPF | Group 1: patients with treated CE (n = 129) Group 2: patients without CE (n = 103) Group 3: patients undergoing the first IVF cycle (n = 932) | -Implantation rate -Clinical pregnancy rate -Live birth rate |
| Fan et al. 2019 [33] | Retrospective study ------ China ------- December 2016–July 2018 | 141 patients undergoing 1 IVF-ET cycle ------- -At least 2 high quality fresh embryos transferred in a previous IVF/ICSI cycle -Age 20–38 years BMI: 18–25 Kg/m2 - Normal uterine cavity -no endometriosis, adenomyosis, hydrosalpinx, fibroids | - | -EB -HIS examination --IVF cycle | Two methods: ≥1 plasma cell/section or ≥1 plasma cell/mm2 | Group 1: <1 CD138+(n = 97) Group 2: ≥1 CD138+ (n = 44) | -Implantation rate -Clinical pregnancy rate |
| Hirata et al. 2021 [32] | Prospective study ------ Japan ------- June 2014–September 2017 | 53 patients undergoing IVF-ET cycle ------- -Age <41 years -Normal uterine cavity -Unexplained infertility - No history of RIF or RPL - No genetic disorders, endocrine diseases or autoimmune diseases | -GnRH-a or GnRH ant protocol -oocyte retrieval and blastocyst freezing -Single blastocyst transfer within 90 days of endometrial tissue sampling with a hormone replacement cycle | -Oocyte retrieval and blastocyst freezing -Diagnostic HSC -EB -HIS examination - single blastocyst transfer | Four different diagnostic criteria: -≥1 plasma cell/10 HPFs -≥2 plasma cell/10 HPFs -≥3 plasma cell/10 HPFs -≥4 plasma cell/10 HPFs | Based on the diagnostic criterion: (≥1; ≥2; ≥3, ≥4) Group A: patients with CE (26; 19; 14; 11) Group B: patients without CE (27; 34; 39; 42) | -Clinical pregnancy rate -Live birth rate -Miscarriage rate |
| Johnston-MacAnanny et al. 2010 [6] | Prospective study ------ USA ------- 2001–2007 | 518 RIF patients undergoing IVF-ET cycle 33 with an EB and 485 without an EB ------- -At least 1 good quality embryos transferred in ≥2 previous IVF/ICSI cycles | -GnRH-a or GnRH ant protocol -rFSH alone or with hMG -U-Hcg (5000 or 10000 UI) at follicle size 17 mm (≥2). -Egg retrieval 35 h after ovulation induction -Luteal phase support with vaginal progesterone | -EB -HIS examination -Antibiotic therapy (when appropriate) -Control EB -IVF cycle | ≥1 plasma cell/HPF | Group 1: patients with treated CE (n = 10) Group 2: patients without CE (n = 23) Group 3: RIF patients who did not have an EB (n = 485) | -Clinical pregnancy rate -Ongoing pregnancy rate |
| Kitaya et al. 2017 [12] | Prospective cohort study ------- Japan --- November 2011– July 2014 | 421 RIF patients undergoing up to three IVF-ET cycle ------- -IVF failure with three or more morphologically good cleavage-stage embryos and/or blastocysts transferred. -No intrauterine pathology | - | -Diagnostic HSC -EB -HIS examination -Endometrial culture -Antibiotic therapy (when appropriate) -Control EB -IVF cycle | ESPDI ≥ 0.25 The endometrial stromal plasmacyte density index (ESPDI) was calculated as the sum of the stromal CD138+ cell counts divided by the number of the HPF evaluated. | Group A: patients with cured CE (n = 116) Group B: patients with persistent CE (n = 4) Group C: patients without CE (n = 226) | Clinical pregnancy rate -Ongoing pregnancy/live birth rate -Miscarriage rate |
| Kuroda et al. 2020 [8] | Cross sectional study ------ Japan ------ June 2018– February 2020 | 88 infertile women ------ -No intrauterine pathology | -clomiphene citrate or letrozole in combination with rFSH or hMG -hCG 250 μg or nasal buserelin acetate spray 600 μg at follicle size ≥17 mm (≥2) -Egg retrieval 35 h after ovulation induction -Conventional IVF or ICSI - All embryos were cryopreserved at blastocyst developmental stage ≥4 in the Gardner classification using the vitrification method -endometrium prepared for ET via a hormone replacement cycle | -EB -IHC staining -ERA testing -Antiobiotic therapy (when appropriate) -Control EB -IVF cycle | ≥5 CD138+ plasma cells per 10 random stromal areas at ×400 magnification. | Group A: non CE patients (n = 33); Group B: CE patients (n = 19) at ERA testing; Group C: cured-CE patients (n = 36) | -hCG positive rate -Clinical pregnancy rate -Miscarriage rate -Ongoing pregnancy rate |
| Li et al. 2021 [9] | Retrospective study ------ China ------ Between 2017 and 2018 | 716 infertile patients undergoing IVF-ET cycle ------- - <45 years; - endometrial scratching - previous antibiotic treatment for CE | - | - endometrial scratching -EB -HIS examination -IVF | Six different diagnostic criteria - 0 plasma cell/HPF in all of the 30 selected HPFs; -1 plasma cell/hpfs in at least 1 out of 30 selected HPFs; -2 plasma cell/HPFs in at least 1 out of 30 selected HPFs; -3 plasma cell/HPFs in at least 1 out of 30 selected HPFs; -4 plasma cell/HPFs in at least 1 out of 30 selected HPFs; -≥5 plasma cell/HPFs in at least 1 out of 30 selected HPFs; | Group A: 0 CD138+/HPF in all of the 30 selected HPFs (n = 433); Group B: 1 CD138+/HPF in at least 1 out of 30 selected HPFs (n = 178); Group C: 2 CD138+/HPF in at least 1 out of 30 selected HPFs (n = 33); Group D: 3 CD138+/HPF in at least 1 out of 30 selected HPFs (n = 18); Group E: 4 CD138+/HPF in at least 1 out of 30 selected HPFs (n = 6); Group F: ≥5 CD138+/HPF in at least 1 out of 30 selected HPFs (n = 38); | -Clinical pregnancy rate -Live birth rate -Miscarriage rate |
| Xiong et al. 2021 [10] | Retrospective study ------ China ------ June 2017–June 2018 | 640 infertile patients undergoing IVF-ET cycle ------- -No antibiotic treatments before the hysteroscopy - age < 40 years; -Normal basal hormone levels (FSH < 10 IU/L and E2 < 60 pg/mL); -BMI < 30 Kg/m2; -Normal parental peripheral karyotypes; -Frozen embryo transfer cycles within 6 months after antibiotic treatment - No RPL - no primary ovarian insufficiency - no previous surgery for myoma or endometriosis, - normal uterine cavity | -GnRH a or GnRH ant protocol: -rFSH or hMG -GnRH a or GnRH ant mild stimulation protocol: oral clomiphene citrate 100mg/day + hMG from the fifth day -hCG (10,000 IU) or recombinant hCG (250 mg) when >3 follicles reached a mean diameter of 18 mm; - Oocyte retrieval was performed 36 h after hCG administration; -Luteal phase support with intra- muscular injection of progesterone (60 mg daily) or once daily vaginal progesterone combined with dydrogesterone (10 mg 3 times a day). | -Diagnostic HSC -EB -HIS examination -Antibiotic therapy (when appropriate) -Control EB -IVF cycle | ≥1 plasma cell/HPF | Group 1: patients with CD138+/HPF = 0 (n = 88); Group 2: patients with CD138+/HPF 1–4 with antibiotic treatment (n = 116); Group 3: patients with CD138+/HPF 1–4 without antibiotic treatment (n = 199). ------- Group 1: patients with CD138+/HPF 0–4 (n = 403); Group 2: patients with cured CE (n = 211); ------- Group 1: patients with CD138+/HPF 0–4 (n = 403); Group 2: patients with persistent CE (n = 26); | -Implantation rate -Clinical pregnancy rate -Live birth rate -Early pregnancy loss rate -Cumulative live birth rate |
| Zhang et al. 2019 [34] | Prospective cohort study ------- China ------- February 2015–June 2017 | 298 RIF patients undergoing 1 IVF-ET cycle ------- -age < 35 years -≥three failed IVF-ET cycles or ≥6 high-quality embryo transferred -Normal uterine cavity -Normal parental peripheral karyotype. | -rFSH (175–225 IU/day) -U-Hcg (10,000 UI) at follicle size 17 mm (≥2) -Egg retrieval 36 h after ovulation induction -≤3 embryos transferred (of which at least one with good quality) on day 3 of culture - Luteal phase support with intramuscular progesterone 60 mg daily | -Diagnostic HSC -EB - HIS examination -intrauterine antibiotic therapy (when appropriate) -Control EB -IVF cycle | ≥1 plasma cell/HPF | Group 1: patients without CE (n = 126) Group 2: patients with cured CE (n = 85) Group 3: patients with persistent CE (n = 24) | -Implantation rate -Clinical pregnancy rate -Live birth rate -Clinical loss rate |
| BMI: body mass index; CE: chronic endometritis; E2: estradiol; EB: endometrial biopsy; ERA testing: endometrial receptivity array testing; ET: embryo transfer; FSH: follicle-stimulating hormone; GnRH-a: GnRH agonist; GnRH-ant: gonadotropin releasing hormone antagonist; HIS: histology; hMG: human menopausal gonadotropin; HPF: high power fields; HSC: hysteroscopy; ICSI: intracytoplasmatic sperm injection; IU: international unit; IVF: in vitro fertilization; RIF: recurrent implantation failure; RPL: recurrent pregnancy loss; rFSH: recombinant FSH; r-Hcg: recombinant human chorionic gonadotropin; U-Hcg: urinary human chorionic gonadotropin. | |||||||
References
- Moreno, I.; Cicinelli, E.; Garcia-Grau, I.; Gonzalez-Monfort, M.; Bau, D.; Vilella, F.; De Ziegler, D.; Resta, L.; Valbuena, D.; Simon, C. The Diagnosis of Chronic Endometritis in Infertile Asymptomatic Women: A Comparative Study of Histology, Microbial Cultures, Hysteroscopy, and Molecular Microbiology. Am. J. Obstet. Gynecol. 2018, 218, 602.e1–602.e16. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K. Prevalence of Chronic Endometritis in Recurrent Miscarriages. Fertil. Steril. 2011, 95, 1156–1158. [Google Scholar] [CrossRef]
- McQueen, D.B.; Perfetto, C.O.; Hazard, F.K.; Lathi, R.B. Pregnancy Outcomes in Women with Chronic Endometritis and Recurrent Pregnancy Loss. Fertil. Steril. 2015, 104, 927–931. [Google Scholar] [CrossRef]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Lepera, A.; Alfonso, R.; Indraccolo, U.; Marrocchella, S.; Greco, P.; Resta, L. Prevalence of Chronic Endometritis in Repeated Unexplained Implantation Failure and the IVF Success Rate after Antibiotic Therapy. Hum. Reprod. 2015, 30, 323–330. [Google Scholar] [CrossRef]
- Cicinelli, E.; Matteo, M.; Trojano, G.; Mitola, P.C.; Tinelli, R.; Vitagliano, A.; Crupano, F.M.; Lepera, A.; Miragliotta, G.; Resta, L. Chronic Endometritis in Patients with Unexplained Infertility: Prevalence and Effects of Antibiotic Treatment on Spontaneous Conception. Am. J. Reprod. Immunol. 2018, 79, e12782. [Google Scholar] [CrossRef] [PubMed]
- Johnston-MacAnanny, E.B.; Hartnett, J.; Engmann, L.L.; Nulsen, J.C.; Sanders, M.M.; Benadiva, C.A. Chronic Endometritis is a Frequent Finding in Women with Recurrent Implantation Failure after in Vitro Fertilization. Fertil. Steril. 2010, 93, 437–441. [Google Scholar] [CrossRef]
- Zargar, M.; Ghafourian, M.; Nikbakht, R.; Mir Hosseini, V.; Moradi Choghakabodi, P. Evaluating Chronic Endometritis in Women with Recurrent Implantation Failure and Recurrent Pregnancy Loss by Hysteroscopy and Immunohistochemistry. J. Minim. Invasive Gynecol. 2020, 27, 116–121. [Google Scholar] [CrossRef]
- Kuroda, K.; Horikawa, T.; Moriyama, A.; Nakao, K.; Juen, H.; Takamizawa, S.; Ojiro, Y.; Nakagawa, K.; Sugiyama, R. Impact of Chronic Endometritis on Endometrial Receptivity Analysis Results and Pregnancy Outcomes. Immun. Inflamm. Dis. 2020, 8, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, S.; Yu, S.; Huang, C.; Lin, S.; Chen, W.; Mo, M.; Lian, R.; Diao, L.; Ding, L.; et al. Diagnosis of Chronic Endometritis: How Many CD138+ Cells/HPF in Endometrial Stroma Affect Pregnancy Outcome of Infertile Women? Am. J. Reprod. Immunol. 2021, 85, e13369. [Google Scholar] [CrossRef]
- Xiong, Y.; Chen, Q.; Chen, C.; Tan, J.; Wang, Z.; Gu, F.; Xu, Y. Impact of Oral Antibiotic Treatment for Chronic Endometritis on Pregnancy Outcomes in the Following Frozen-Thawed Embryo Transfer Cycles of Infertile Women: A Cohort Study of 640 Embryo Transfer Cycles. Fertil. Steril. 2021, 116, 413–421. [Google Scholar] [CrossRef]
- Demirdag, E.; Guler, I.; Cevher Akdulum, M.F.; Sahin, E.; Erdem, O.; Erdem, A.; Erdem, M. Subsequent IVF Outcomes Following Antibiotic Therapy for Chronic Endometritis in Patients with Recurrent Implantation Failure. J. Obstet. Gynaecol. Res. 2021, 47, 4350–4356. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K.; Matsubayashi, H.; Takaya, Y.; Nishiyama, R.; Yamaguchi, K.; Takeuchi, T.; Ishikawa, T. Live Birth Rate Following Oral Antibiotic Treatment for Chronic Endometritis in Infertile Women with Repeated Implantation Failure. Am. J. Reprod. Immunol. 2017, 78, e12719. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.-J.; Zhang, H.; Chen, Z.-Q.; Zhang, W.; Liu, X.-M.; Fang, J.-Y.; Liu, F.-J.; Kwak-Kim, J. Endometrial TGF-β, IL-10, IL-17 and Autophagy Are Dysregulated in Women with Recurrent Implantation Failure with Chronic Endometritis. Reprod. Biol. Endocrinol. 2019, 17, 2. [Google Scholar] [CrossRef]
- Buzzaccarini, G.; Vitagliano, A.; Andrisani, A.; Santarsiero, C.M.; Cicinelli, R.; Nardelli, C.; Ambrosini, G.; Cicinelli, E. Chronic Endometritis and Altered Embryo Implantation: A Unified Pathophysiological Theory from a Literature Systematic Review. J. Assist. Reprod. Genet. 2020, 37, 2897–2911. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K.; Yasuo, T. Aberrant Expression of Selectin E, CXCL1, and CXCL13 in Chronic Endometritis. Mod. Pathol. 2010, 23, 1136–1146. [Google Scholar] [CrossRef]
- Di Pietro, C.; Cicinelli, E.; Guglielmino, M.R.; Ragusa, M.; Farina, M.; Palumbo, M.A.; Cianci, A. Altered Transcriptional Regulation of Cytokines, Growth Factors, and Apoptotic Proteins in the Endometrium of Infertile Women with Chronic Endometritis. Am. J. Reprod. Immunol. 2013, 69, 509–517. [Google Scholar] [CrossRef]
- Wu, D.; Kimura, F.; Zheng, L.; Ishida, M.; Niwa, Y.; Hirata, K.; Takebayashi, A.; Takashima, A.; Takahashi, K.; Kushima, R.; et al. Chronic Endometritis Modifies Decidualization in Human Endometrial Stromal Cells. Reprod. Biol. Endocrinol. 2017, 15, 16. [Google Scholar] [CrossRef]
- Cicinelli, E.; Vitagliano, A.; Loizzi, V.; De Ziegler, D.; Fanelli, M.; Bettocchi, S.; Nardelli, C.; Trojano, G.; Cicinelli, R.; Minervini, C.F.; et al. Altered Gene Expression Encoding Cytochines, Grow Factors and Cell Cycle Regulators in the Endometrium of Women with Chronic Endometritis. Diagnostics 2021, 11, 471. [Google Scholar] [CrossRef]
- Matteo, M.; Cicinelli, E.; Greco, P.; Massenzio, F.; Baldini, D.; Falagario, T.; Rosenberg, P.; Castellana, L.; Specchia, G.; Liso, A. Abnormal Pattern of Lymphocyte Subpopulations in the Endometrium of Infertile Women with Chronic Endometritis. Am. J. Reprod. Immunol. 2009, 61, 322–329. [Google Scholar] [CrossRef]
- Kitaya, K.; Tada, Y.; Hayashi, T.; Taguchi, S.; Funabiki, M.; Nakamura, Y. Comprehensive Endometrial Immunoglobulin Subclass Analysis in Infertile Women Suffering from Repeated Implantation Failure with or without Chronic Endometritis. Am. J. Reprod. Immunol. 2014, 72, 386–391. [Google Scholar] [CrossRef]
- Pinto, V.; Matteo, M.; Tinelli, R.; Mitola, P.C.; De Ziegler, D.; Cicinelli, E. Altered Uterine Contractility in Women with Chronic Endometritis. Fertil. Steril. 2015, 103, 1049–1052. [Google Scholar] [CrossRef] [PubMed]
- Mishra, K.; Wadhwa, N.; Guleria, K.; Agarwal, S. ER, PR and Ki-67 Expression Status in Granulomatous and Chronic Non-Specific Endometritis. J. Obstet. Gynaecol. Res. 2008, 34, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, F.M.; Aguiar, F.N.; Tomioka, R.; de Oliveira, R.M.; Frantz, N.; Ueno, J. Functional Endometrial Polyps in Infertile Asymptomatic Patients: A Possible Evolution of Vascular Changes Secondary to Endometritis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 152–156. [Google Scholar] [CrossRef]
- Cicinelli, E.; Vitagliano, A.; Kumar, A.; Lasmar, R.B.; Bettocchi, S.; Haimovich, S.; International Working Group for Standardization of Chronic Endometritis Diagnosis. Unified Diagnostic Criteria for Chronic Endometritis at Fluid Hysteroscopy: Proposal and Reliability Evaluation through an International Randomized-Controlled Observer Study. Fertil. Steril. 2019, 112, 162–173.e2. [Google Scholar] [CrossRef]
- Cicinelli, E.; Haimovich, S.; De Ziegler, D.; Raz, N.; Ben-Tzur, D.; Andrisani, A.; Ambrosini, G.; Picardi, N.; Cataldo, V.; Balzani, M.; et al. MUM-1 Immunohistochemistry Has High Accuracy and Reliability in the Diagnosis of Chronic Endometritis: A Multi-Centre Comparative Study with CD-138 Immunostaining. J. Assist. Reprod. Genet. 2022, 39, 219–226. [Google Scholar] [CrossRef]
- Cicinelli, E.; Resta, L.; Loizzi, V.; Pinto, V.; Santarsiero, C.; Cicinelli, R.; Greco, P.; Vitagliano, A. Antibiotic Therapy versus No Treatment for Chronic Endometritis: A Case-Control Study. Fertil. Steril. 2021, 115, 1541–1548. [Google Scholar] [CrossRef]
- Cicinelli, E.; Cicinelli, R.; Vitagliano, A. Consistent Evidence on the Detrimental Role of Severe Chronic Endometritis on in Vitro Fertilization Outcome and the Reproductive Improvement after Antibiotic Therapy: On the Other Hand, Mild Chronic Endometritis Appears a More Intricate Matter. Fertil. Steril. 2021, 116, 345–346. [Google Scholar] [CrossRef]
- Vitagliano, A.; Saccardi, C.; Noventa, M.; Di Spiezio Sardo, A.; Saccone, G.; Cicinelli, E.; Pizzi, S.; Andrisani, A.; Litta, P.S. Effects of Chronic Endometritis Therapy on in Vitro Fertilization Outcome in Women with Repeated Implantation Failure: A Systematic Review and Meta-Analysis. Fertil. Steril. 2018, 110, 103–112.e1. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Cumpston, M.S.; McKenzie, J.E.; Welch, V.A.; Brennan, S.E. Strengthening Systematic Reviews in Public Health: Guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd Edition. J. Public Health 2022, fdac036. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Kimura, F.; Nakamura, A.; Kitazawa, J.; Morimune, A.; Hanada, T.; Takebayashi, A.; Takashima, A.; Amano, T.; Tsuji, S.; et al. Histological Diagnostic Criterion for Chronic Endometritis Based on the Clinical Outcome. BMC Womens Health 2021, 21, 94. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Li, X.; Li, Y.; Liao, J.; Chen, H.; Li, Y.; Lu, G.-X.; Lin, G.; Gong, F. Endometrial CD138 Count Appears to Be a Negative Prognostic Indicator for Patients Who Have Experienced Previous Embryo Transfer Failure. Fertil. Steril. 2019, 112, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, H.; Liu, Y.; Zheng, S.; Zhao, W.; Wu, D.; Lei, L.; Chen, G. Confirmation of Chronic Endometritis in Repeated Implantation Failure and Success Outcome in IVF-ET after Intrauterine Delivery of the Combined Administration of Antibiotic and Dexamethasone. Am. J. Reprod. Immunol. 2019, 82, e13177. [Google Scholar] [CrossRef] [PubMed]
- Moreno, I.; Simon, C. Deciphering the Effect of Reproductive Tract Microbiota on Human Reproduction. Reprod. Med. Biol. 2019, 18, 40–50. [Google Scholar] [CrossRef]
- Lozano, F.M.; Bernabeu, A.; Lledo, B.; Morales, R.; Diaz, M.; Aranda, F.I.; Llacer, J.; Bernabeu, R. Characterization of the Vaginal and Endometrial Microbiome in Patients with Chronic Endometritis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 25–32. [Google Scholar] [CrossRef]
- Cicinelli, E.; Cicinelli, R.; Vitagliano, A. Antibiotic Therapy for Chronic Endometritis and Its Reproductive Implications: A Step Forward, with Some Uncertainties. Fertil. Steril. 2021, 115, 1445–1446. [Google Scholar] [CrossRef]
- Cicinelli, E.; Bettocchi, S.; de Ziegler, D.; Loizzi, V.; Cormio, G.; Marinaccio, M.; Trojano, G.; Crupano, F.M.; Francescato, R.; Vitagliano, A.; et al. Chronic Endometritis, a Common Disease Hidden Behind Endometrial Polyps in Premenopausal Women: First Evidence From a Case-Control Study. J. Minim. Invasive Gynecol. 2019, 26, 1346–1350. [Google Scholar] [CrossRef]
- Vitagliano, A.; Cialdella, M.; Cicinelli, R.; Santarsiero, C.M.; Greco, P.; Buzzaccarini, G.; Noventa, M.; Cicinelli, E. Association between Endometrial Polyps and Chronic Endometritis: Is It Time for a Paradigm Shift in the Pathophysiology of Endometrial Polyps in Pre-Menopausal Women? Results of a Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 2182. [Google Scholar] [CrossRef]
- Ishida, M.; Takebayashi, A.; Kimura, F.; Nakamura, A.; Kitazawa, J.; Morimune, A.; Hanada, T.; Tsuta, K.; Murakami, T. Induction of the Epithelial-Mesenchymal Transition in the Endometrium by Chronic Endometritis in Infertile Patients. PLoS ONE 2021, 16, e0249775. [Google Scholar] [CrossRef]
- Hodes-Wertz, B.; Grifo, J.; Ghadir, S.; Kaplan, B.; Laskin, C.A.; Glassner, M.; Munné, S. Idiopathic Recurrent Miscarriage is Caused Mostly by Aneuploid Embryos. Fertil. Steril. 2012, 98, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Vitagliano, A.; Noventa, M.; Gizzo, S. Autoimmunity, Systemic Inflammation, and Their Correlation with Repeated Implantation Failure and Recurrent Miscarriage: Is Chronic Endometritis the Missing Piece of the Jigsaw? Am. J. Reprod. Immunol. 2017, 77. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.C.; Christiansen, O.B.; Kolte, A.M.; Macklon, N. New Insights into Mechanisms behind Miscarriage. BMC Med. 2013, 11, 154. [Google Scholar] [CrossRef]
- Noventa, M.; Vitagliano, A.; Andrisani, A.; Blaganje, M.; Viganò, P.; Papaelo, E.; Scioscia, M.; Cavallin, F.; Ambrosini, G.; Cozzolino, M. Testosterone Therapy for Women with Poor Ovarian Response Undergoing IVF: A Meta-Analysis of Randomized Controlled Trials. J. Assist. Reprod. Genet. 2019, 36, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Padula, F.; Laganà, A.S.; Vitale, S.G.; D’Emidio, L.; Coco, C.; Giannarelli, D.; Cariola, M.; Favilli, A.; Giorlandino, C. The Introduction of the Absolute Risk for the Detection of Fetal Aneuploidies in the First-Trimester Screening. J. Matern.-Fetal Neonatal Med. 2017, 30, 1249–1253. [Google Scholar] [CrossRef]
- Ciancimino, L.; Laganà, A.S.; Chiofalo, B.; Granese, R.; Grasso, R.; Triolo, O. Would It Be Too Late? A Retrospective Case-Control Analysis to Evaluate Maternal-Fetal Outcomes in Advanced Maternal Age. Arch. Gynecol. Obstet. 2014, 290, 1109–1114. [Google Scholar] [CrossRef]
- Drizi, A.; Djokovic, D.; Laganà, A.S.; van Herendael, B. Impaired Inflammatory State of the Endometrium: A Multifaceted Approach to Endometrial Inflammation. Current Insights and Future Directions. Prz. Menopauzalny 2020, 19, 90–100. [Google Scholar] [CrossRef]
- Puente, E.; Alonso, L.; Laganà, A.S.; Ghezzi, F.; Casarin, J.; Carugno, J. Chronic Endometritis: Old Problem, Novel Insights and Future Challenges. Int. J. Fertil. Steril. 2020, 13, 250–256. [Google Scholar] [CrossRef]
- Vitale, S.G.; Haimovich, S.; Laganà, A.S.; Alonso, L.; Di Spiezio Sardo, A.; Carugno, J.; From the Global Community of Hysteroscopy Guidelines Committee Endometrial Polyps. An Evidence-Based Diagnosis and Management Guide. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 260, 70–77. [Google Scholar] [CrossRef]
- Yang, R.; Du, X.; Wang, Y.; Song, X.; Yang, Y.; Qiao, J. The Hysteroscopy and Histological Diagnosis and Treatment Value of Chronic Endometritis in Recurrent Implantation Failure Patients. Arch. Gynecol. Obstet. 2014, 289, 1363–1369. [Google Scholar] [CrossRef]
- Bedner, R.; Rzepka-Górska, I. Hysteroscopy with Directed Biopsy versus Dilatation and Curettage for the Diagnosis of Endometrial Hyperplasia and Cancer in Perimenopausal Women. Eur. J. Gynaecol. Oncol. 2007, 28, 400–402. [Google Scholar] [PubMed]
- Saccardi, C.; Vitagliano, A.; Marchetti, M.; Lo Turco, A.; Tosatto, S.; Palumbo, M.; De Lorenzo, L.S.; Vitale, S.G.; Scioscia, M.; Noventa, M. Endometrial Cancer Risk Prediction According to Indication of Diagnostic Hysteroscopy in Post-Menopausal Women. Diagnostics 2020, 10, 257. [Google Scholar] [CrossRef]
- Carugno, J.; Marbin, S.J.; LaganÀ, A.S.; Vitale, S.G.; Alonso, L.; DI Spiezio Sardo, A.; Haimovich, S. New Development on Hysteroscopy for Endometrial Cancer Diagnosis: State of the Art. Minerva Med. 2021, 112, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Luerti, M.; Vitagliano, A.; Di Spiezio Sardo, A.; Angioni, S.; Garuti, G.; De Angelis, C. Italian School of Minimally Invasive Gynecological Surgery Hysteroscopists Group Effectiveness of Hysteroscopic Techniques for Endometrial Polyp Removal: The Italian Multicenter Trial. J. Minim. Invasive Gynecol. 2019, 26, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.-L.; Liang, X.-D.; Wang, J.-L.; Cui, H.; Wei, L.-H. Hysteroscopy and Directed Biopsy in the Diagnosis of Endometrial Carcinoma. Chin. Med. J. 2010, 123, 3524–3528. [Google Scholar] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Sample Representativeness | Sampling Technique | Ascertainment of CE Diagnosis | Quality of Description of the Population | Incomplete Outcome Data | Total Score | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Cicinelli et al. 2015 [4] | ★ | - | ★ | ★ | ★ | ★★★★ | Low |
| Demirdag et al. 2021 [11] | ★ | ★ | ★ | ★ | - | ★★★★ | Low |
| Fan et al. 2019 [33] | ★ | - | ★ | ★ | - | ★★★ | Low |
| Hirata et al. 2021 [32] | - | - | ★ | ★ | ★ | ★★★ | Low |
| Johnston-MacAnanny et al. 2010 [6] | - | - | ★ | ★ | ★ | ★★★ | Low |
| Kitaya et al. 2017 [12] | ★ | ★ | ★ | - | - | ★★★ | Low |
| Kuroda et al. 2020 [8] | - | ★ | ★ | ★ | ★ | ★★★★ | Low |
| Li et al. 2021 [9] | ★ | - | ★ | ★ | ★ | ★★★★ | Low |
| Xiong et al. 2021 [10] | ★ | - | ★ | ★ | ★ | ★★★★ | Low |
| Zhang et al. 2019 [34] | ★ | - | ★ | - | ★ | ★★★ | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitagliano, A.; Laganà, A.S.; De Ziegler, D.; Cicinelli, R.; Santarsiero, C.M.; Buzzaccarini, G.; Chiantera, V.; Cicinelli, E.; Marinaccio, M. Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2250. https://doi.org/10.3390/diagnostics12092250
Vitagliano A, Laganà AS, De Ziegler D, Cicinelli R, Santarsiero CM, Buzzaccarini G, Chiantera V, Cicinelli E, Marinaccio M. Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(9):2250. https://doi.org/10.3390/diagnostics12092250
Chicago/Turabian StyleVitagliano, Amerigo, Antonio Simone Laganà, Dominique De Ziegler, Rossana Cicinelli, Carla Mariaflavia Santarsiero, Giovanni Buzzaccarini, Vito Chiantera, Ettore Cicinelli, and Marco Marinaccio. 2022. "Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis" Diagnostics 12, no. 9: 2250. https://doi.org/10.3390/diagnostics12092250
APA StyleVitagliano, A., Laganà, A. S., De Ziegler, D., Cicinelli, R., Santarsiero, C. M., Buzzaccarini, G., Chiantera, V., Cicinelli, E., & Marinaccio, M. (2022). Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis. Diagnostics, 12(9), 2250. https://doi.org/10.3390/diagnostics12092250