
Prognostic Impact of Myosteatosis on Mortality in Hospitalized Patients with COVID-19

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
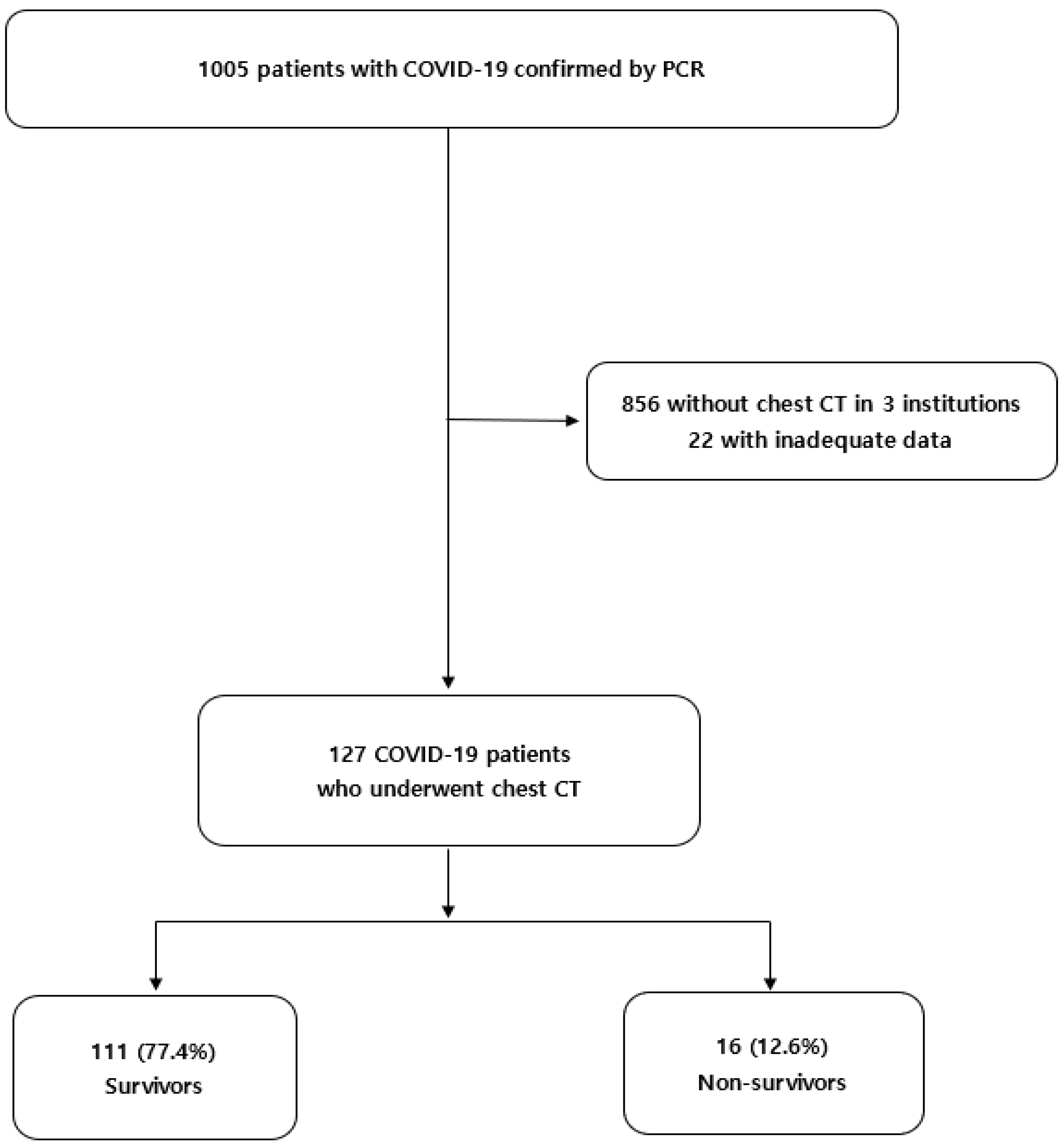
2.1. Patients and Data Collection
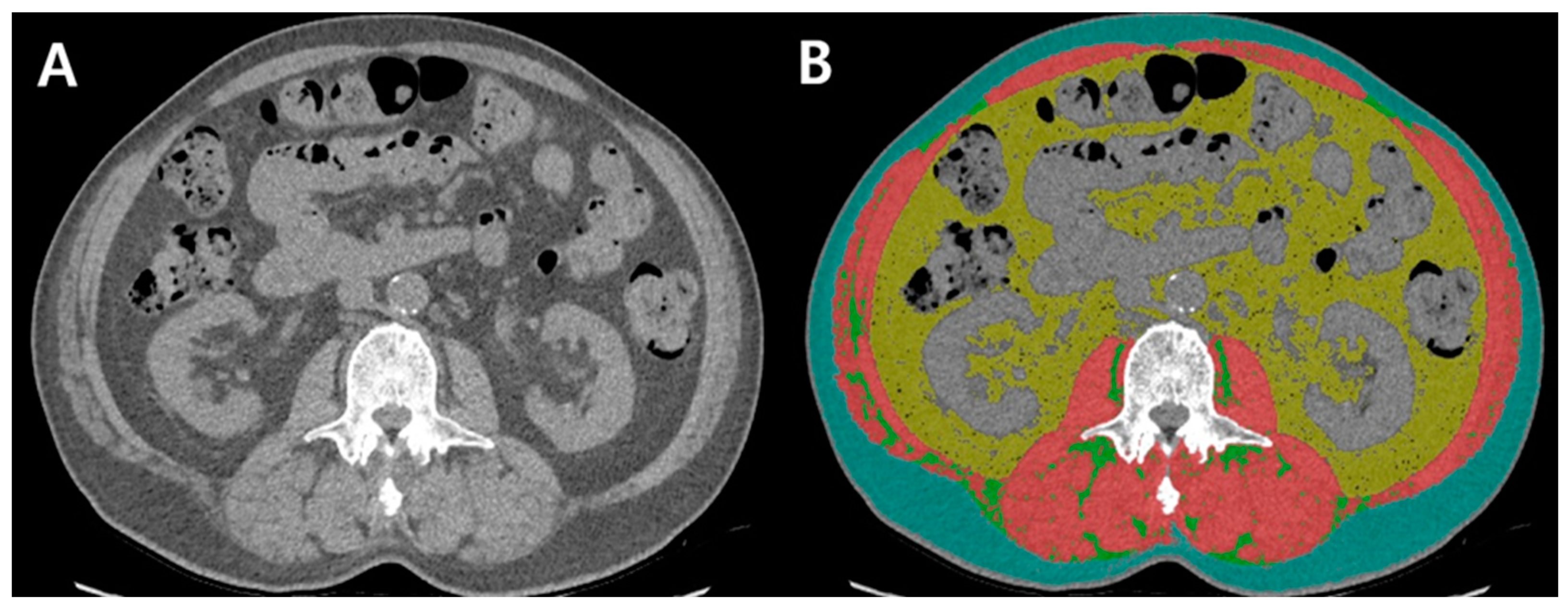
2.2. Assessment of Body Composition
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
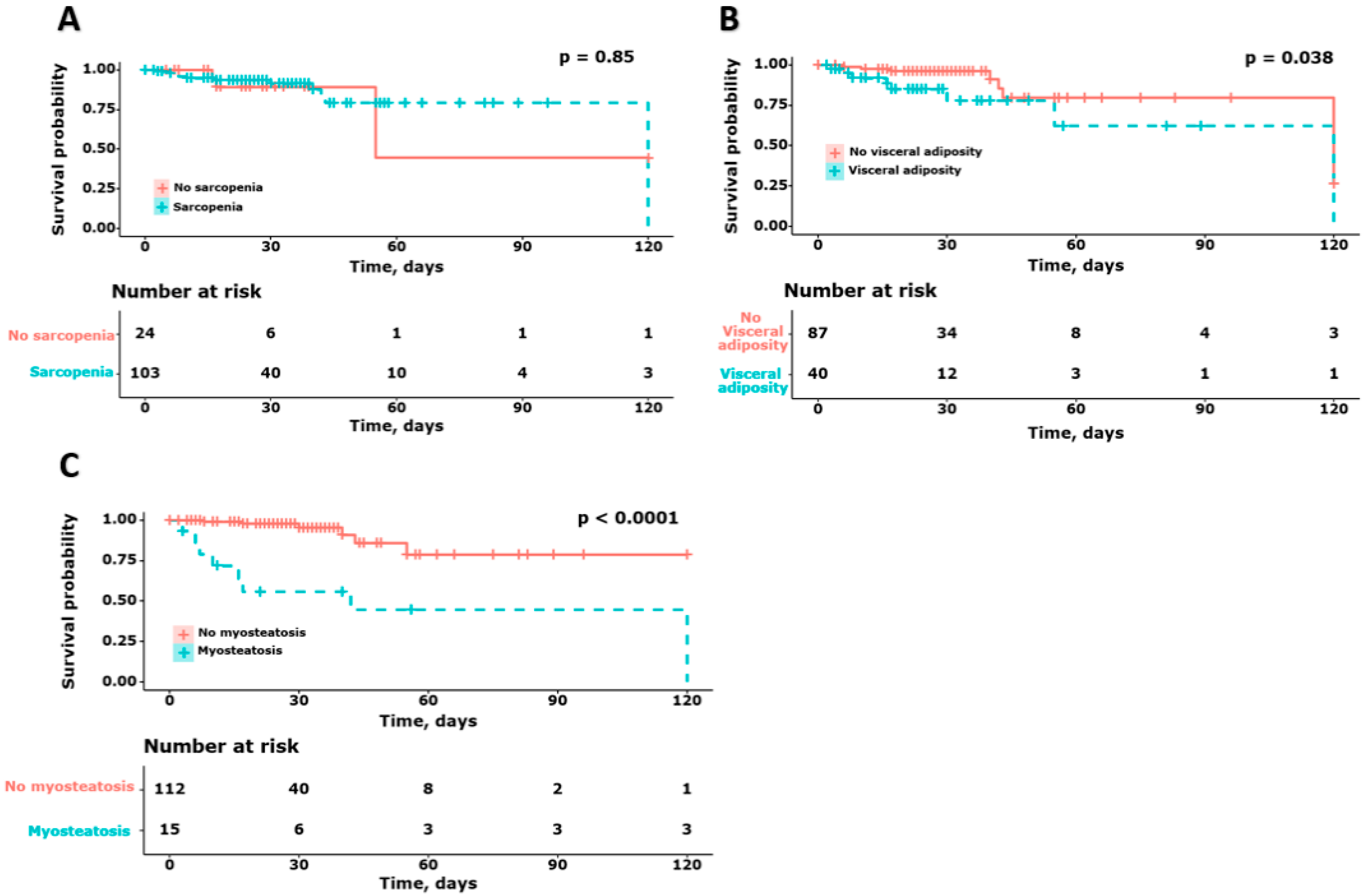
3.2. Survival Probability According to the Body Composition in Patients with COVID-19
3.3. Risk Factors for Mortality in Patients with COVID-19, including Body Composition
3.4. Association between Myosteatosis and Mortality in Patients with COVID-19
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.; Cheruiyot, I.; Vikse, J.; Mutua, V.; Kipkorir, V.; Benoit, J.; Plebani, M.; Bragazzi, N.; Lippi, G. Lymphopenia and neutrophilia at admission predicts severity and mortality in patients with COVID-19: A meta-analysis. Acta Biomed. 2020, 91, e2020008. [Google Scholar] [CrossRef] [PubMed]
- Ibanez-Samaniego, L.; Bighelli, F.; Uson, C.; Caravaca, C.; Fernandez Carrillo, C.; Romero, M.; Barreales, M.; Perello, C.; Madejon, A.; Marcos, A.C.; et al. Elevation of Liver Fibrosis Index FIB-4 Is Associated With Poor Clinical Outcomes in Patients With COVID-19. J. Infect. Dis. 2020, 222, 726–733. [Google Scholar] [CrossRef]
- Illg, Z.; Muller, G.; Mueller, M.; Nippert, J.; Allen, B. Analysis of absolute lymphocyte count in patients with COVID-19. Am. J. Emerg. Med. 2021, 46, 16–19. [Google Scholar] [CrossRef]
- Li, Y.; Regan, J.; Fajnzylber, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Atyeo, C.; Fischinger, S.; Gillespie, E.; et al. Liver Fibrosis Index FIB-4 Is Associated With Mortality in COVID-19. Hepatol. Commun. 2020, 5, 434–445. [Google Scholar] [CrossRef]
- Park, J.G.; Kang, M.K.; Lee, Y.R.; Song, J.E.; Kim, N.Y.; Kweon, Y.O.; Tak, W.Y.; Jang, S.Y.; Lee, C.; Kim, B.S.; et al. Fibrosis-4 index as a predictor for mortality in hospitalised patients with COVID-19: A retrospective multicentre cohort study. BMJ Open 2020, 10, e041989. [Google Scholar] [CrossRef]
- Pranata, R.; Yonas, E.; Huang, I.; Lim, M.A.; Nasution, S.A.; Kuswardhani, R.A.T. Fibrosis-4 index and mortality in coronavirus disease 2019: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, e368–e374. [Google Scholar] [CrossRef]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging (Albany NY) 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Lee, Y.R.; Kang, M.K.; Song, J.E.; Kim, H.J.; Kweon, Y.O.; Tak, W.Y.; Jang, S.Y.; Park, J.G.; Lee, C.; Hwang, J.S.; et al. Clinical outcomes of coronavirus disease 2019 in patients with pre-existing liver diseases: A multicenter study in South Korea. Clin. Mol. Hepatol. 2020, 26, 562–576. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Wang, X.B.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, e72–e74. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.P.; Gottin, L.; Donadello, K.; Schweiger, V.; Brandimarte, P.; Zamboni, G.A.; Florio, A.; Boetti, R.; Pavan, G.; Zamboni, M.; et al. Intermuscular Adipose Tissue as a Risk Factor for Mortality and Muscle Injury in Critically Ill Patients Affected by COVID-19. Front. Physiol. 2021, 12, 651167. [Google Scholar] [CrossRef] [PubMed]
- Yates, T.; Summerfield, A.; Razieh, C.; Banerjee, A.; Chudasama, Y.; Davies, M.J.; Gillies, C.; Islam, N.; Lawson, C.; Mirkes, E.; et al. A population-based cohort study of obesity, ethnicity and COVID-19 mortality in 12.6 million adults in England. Nat. Commun. 2022, 13, 624. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.K.; Baek, J.H.; Kweon, Y.O.; Tak, W.Y.; Jang, S.Y.; Lee, Y.R.; Hur, K.; Kim, G.; Lee, H.W.; Han, M.H.; et al. Association of Skeletal Muscle and Adipose Tissue Distribution with Histologic Severity of Non-Alcoholic Fatty Liver. Diagnostics 2021, 11, 1061. [Google Scholar] [CrossRef]
- Yang, Y.; Ding, L.; Zou, X.; Shen, Y.; Hu, D.; Hu, X.; Li, Z.; Kamel, I.R. Visceral Adiposity and High Intramuscular Fat Deposition Independently Predict Critical Illness in Patients with SARS-CoV-2. Obesity (Silver Spring) 2020, 28, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Jacob Filho, W.; Shinjo, S.K.; Ferriolli, E.; Busse, A.L.; Avelino-Silva, T.J.; Longobardi, I.; de Oliveira Junior, G.N.; Swinton, P.; Gualano, B.; et al. Muscle strength and muscle mass as predictors of hospital length of stay in patients with moderate to severe COVID-19: A prospective observational study. J. Cachexia Sarcopenia Muscle 2021, 12, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Martone, A.M.; Tosato, M.; Ciciarello, F.; Galluzzo, V.; Zazzara, M.B.; Pais, C.; Savera, G.; Calvani, R.; Marzetti, E.; Robles, M.C.; et al. Sarcopenia as potential biological substrate of long COVID-19 syndrome: Prevalence, clinical features, and risk factors. J. Cachexia Sarcopenia Muscle 2022, 13, 1974–1982. [Google Scholar] [CrossRef]
- Osuna-Padilla, I.A.; Rodriguez-Moguel, N.C.; Rodriguez-Llamazares, S.; Orsso, C.E.; Prado, C.M.; Rios-Ayala, M.A.; Villanueva-Camacho, O.; Aguilar-Vargas, A.; Pensado-Piedra, L.E.; Juarez-Hernandez, F.; et al. Low muscle mass in COVID-19 critically-ill patients: Prognostic significance and surrogate markers for assessment. Clin. Nutr, 2022; in press. [Google Scholar] [CrossRef]
- Battisti, S.; Pedone, C.; Napoli, N.; Russo, E.; Agnoletti, V.; Nigra, S.G.; Dengo, C.; Mughetti, M.; Conte, C.; Pozzilli, P.; et al. Computed Tomography Highlights Increased Visceral Adiposity Associated With Critical Illness in COVID-19. Diabetes Care 2020, 43, e129–e130. [Google Scholar] [CrossRef]
- Viddeleer, A.R.; Raaphorst, J.; Min, M.; Beenen, L.F.M.; Scheerder, M.J.; Vlaar, A.P.J.; Amsterdam UMC COVID-19 Biobank; Beudel, M.; Hemke, R. Intramuscular adipose tissue at level Th12 is associated with survival in COVID-19. J. Cachexia Sarcopenia Muscle 2021, 12, 823–827. [Google Scholar] [CrossRef]
- Paris, M.T.; Tandon, P.; Heyland, D.K.; Furberg, H.; Premji, T.; Low, G.; Mourtzakis, M. Automated body composition analysis of clinically acquired computed tomography scans using neural networks. Clin. Nutr. 2020, 39, 3049–3055. [Google Scholar] [CrossRef] [PubMed]
- Carey, E.J.; Lai, J.C.; Wang, C.W.; Dasarathy, S.; Lobach, I.; Montano-Loza, A.J.; Dunn, M.A.; Fitness, L.E.; Exercise in Liver Transplantation, C. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl. 2017, 23, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Nakagawa, H.; Kudo, Y.; Tateishi, R.; Taguri, M.; Watadani, T.; Nakagomi, R.; Kondo, M.; Nakatsuka, T.; Minami, T.; et al. Sarcopenia, intramuscular fat deposition, and visceral adiposity independently predict the outcomes of hepatocellular carcinoma. J. Hepatol. 2015, 63, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.J.; Qi, G.Q.; Gu, X.; Zhang, X.Y.; Fang, Y.F.; Jiang, H.; Zhao, Y.J. Lymphocyte blood levels that remain low can predict the death of patients with COVID-19. Medicine 2021, 100, e26503. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Pizzocaro, A.; Vena, W.; Rastrelli, G.; Semeraro, F.; Isidori, A.M.; Pivonello, R.; Salonia, A.; Sforza, A.; Maggi, M. Diabetes is most important cause for mortality in COVID-19 hospitalized patients: Systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 275–296. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, R.; Palmisano, A.; Esposito, A.; Gnasso, C.; Nicoletti, V.; Leone, R.; Vignale, D.; Falbo, E.; Ferrante, M.; Cilla, M.; et al. Myosteatosis Significantly Predicts Persistent Dyspnea and Mobility Problems in COVID-19 Survivors. Front. Nutr. 2022, 9, 846901. [Google Scholar] [CrossRef] [PubMed]
- Ogata, H.; Mori, M.; Jingushi, Y.; Matsuzaki, H.; Katahira, K.; Ishimatsu, A.; Enokizu-Ogawa, A.; Taguchi, K.; Moriwaki, A.; Yoshida, M. Impact of visceral fat on the prognosis of coronavirus disease 2019: An observational cohort study. BMC Infect. Dis 2021, 21, 1240. [Google Scholar] [CrossRef]
- Yi, X.; Liu, H.; Zhu, L.; Wang, D.; Xie, F.; Shi, L.; Mei, J.; Jiang, X.; Zeng, Q.; Hu, P.; et al. Myosteatosis predicting risk of transition to severe COVID-19 infection. Clin. Nutr. 2021; in press. [Google Scholar] [CrossRef]
- Pinto, F.C.S.; Andrade, M.F.; Gatti da Silva, G.H.; Faiad, J.Z.; Barrere, A.P.N.; Goncalves, R.C.; de Castro, G.S.; Seelaender, M. Function Over Mass: A Meta-Analysis on the Importance of Skeletal Muscle Quality in COVID-19 Patients. Front. Nutr. 2022, 9, 837719. [Google Scholar] [CrossRef]
- Baggerman, M.R.; Dekker, I.M.; Winkens, B.; Olde Damink, S.W.M.; Weijs, P.J.M.; van de Poll, M.C.G. Computed tomography reference values for visceral obesity and increased metabolic risk in a Caucasian cohort. Clin. Nutr. ESPEN 2022, 48, 408–413. [Google Scholar] [CrossRef]
- Watanabe, M.; Caruso, D.; Tuccinardi, D.; Risi, R.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Tarallo, M.; Strigari, L.; Manfrini, S.; et al. Visceral fat shows the strongest association with the need of intensive care in patients with COVID-19. Metabolism 2020, 111, 154319. [Google Scholar] [CrossRef]
- Gonzalez-Islas, D.; Sanchez-Moreno, C.; Orea-Tejeda, A.; Hernandez-Lopez, S.; Salgado-Fernandez, F.; Keirns-Davis, C.; Galicia-Amor, S.; Trejo-Mellado, E.; Gochicoa-Rangel, L.; Castorena-Maldonado, A. Body composition and risk factors associated with sarcopenia in post-COVID patients after moderate or severe COVID-19 infections. BMC Pulm. Med. 2022, 22, 223. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Caan, B.J.; Meyerhardt, J.A.; Weltzien, E.; Xiao, J.; Cespedes Feliciano, E.M.; Kroenke, C.H.; Castillo, A.; Kwan, M.L.; Prado, C.M. The deterioration of muscle mass and radiodensity is prognostic of poor survival in stage I-III colorectal cancer: A population-based cohort study (C-SCANS). J. Cachexia Sarcopenia Muscle 2018, 9, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Koon-Yee Lee, G.; Chun-Ming Au, P.; Hoi-Yee Li, G.; Chan, M.; Li, H.L.; Man-Yung Cheung, B.; Chi-Kei Wong, I.; Ho-Fun Lee, V.; Mok, J.; Hon-Kei Yip, B.; et al. Sarcopenia and mortality in different clinical conditions: A meta-analysis. Osteoporos Sarcopenia 2021, 7, S19–S27. [Google Scholar] [CrossRef]
- Rubio-Ruiz, M.E.; Guarner-Lans, V.; Perez-Torres, I.; Soto, M.E. Mechanisms Underlying Metabolic Syndrome-Related Sarcopenia and Possible Therapeutic Measures. Int. J. Mol. Sci. 2019, 20, 647. [Google Scholar] [CrossRef] [PubMed]
- Kuk, J.L.; Church, T.S.; Blair, S.N.; Ross, R. Does measurement site for visceral and abdominal subcutaneous adipose tissue alter associations with the metabolic syndrome? Diabetes Care 2006, 29, 679–684. [Google Scholar] [CrossRef]
- Lee, K.; Shin, Y.; Huh, J.; Sung, Y.S.; Lee, I.S.; Yoon, K.H.; Kim, K.W. Recent Issues on Body Composition Imaging for Sarcopenia Evaluation. Korean J. Radiol. 2019, 20, 205–217. [Google Scholar] [CrossRef]
- Anand, A.; Mohta, S.; Agarwal, S.; Sharma, S.; Gopi, S.; Gunjan, D.; Madhusudhan, K.S.; Singh, N.; Saraya, A. European Working Group on Sarcopenia in Older People (EWGSOP2) Criteria With Population-Based Skeletal Muscle Index Best Predicts Mortality in Asians With Cirrhosis. J. Clin. Exp. Hepatol. 2022, 12, 52–60. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Enrolled Patients n = 127 |
|---|---|
| Age (yr) | 61.0 [50.0–70.0] |
| Men, n (%) | 67 (52.8) |
| BMI, kg/m2 | 23.6 [21.4–25.4] |
| Comorbidities, n (%) | |
| T2DM | 25 (19.7) |
| Hypertension | 46 (36.2) |
| COPD | 7 (5.5) |
| Chronic kidney disease | 4 (3.1) |
| Laboratory profiles | |
| White cell count, ×103/µL | 6000.0 [4690.0–7715.0] |
| Lymphocyte count, ×103/µL | 1209.3 [771.3–1810.1] |
| Hemoglobin, g/dL | 13.1 [12.1–14.0] |
| Platelet count, ×109/µL | 225.0 [158.5–298.0] |
| C reactive protein, mg/L | 2.3 [0.2–10.7] |
| Aspartate aminotransferase, U/L | 32.0 [24.0–47.0] |
| Alanine aminotransferase, U/L | 22.0 [15.0–38.0] |
| Total bilirubin, mg/dL | 0.7 [0.5–1.0] |
| Gamma glutamyl transferase, U/L | 24.0 [17.0–44.0] |
| Creatinine kinase, U/L | 67.0 [46.0–96.5] |
| Serum ferritin, ng/mL | 747.3 [479.9–2023.0] |
| Treatments, n (%) | |
| Oxygen therapy | 24 (18.9) |
| CRRT | 3 (2.4) |
| ECMO | 6 (4.7) |
| Clinical outcomes, n (%) | |
| SIRS on admission | 32 (25.2) |
| ICU admission | 20 (15.7) |
| Septic shock | 20 (15.7) |
| ARDS | 20 (15.7) |
| Acute kidney injury | 8 (6.3) |
| Body composition | |
| SMI, cm2/m2 | 38.0 [33.1–44.3] |
| VATI, cm2/m2 | 32.0 [20.5–49.8] |
| SATI, cm2/m2 | 41.1 [29.0–56.3] |
| VSR | 0.7 [0.4–1.3] |
| Muscle HU | 41.3 [37.8–44.5] |
| Sarcopenia, n (%) | 103 (81.1) |
| Visceral adiposity, n (%) | 40 (31.5) |
| Myosteatosis, n (%) | 15 (11.8) |
| Duration of hospital stay, days | 27.0 [17.0–36.5] |
| Variable | Survivors n = 111 (77.4%) | Non-Survivors n = 16 (12.6%) | p-Value |
|---|---|---|---|
| Age (yr) | 60.0 [46.5–68.5] | 74.5 [66.0–79.5] | <0.001 |
| Men, n (%) | 53 (47.7) | 14 (87.5) | 0.007 |
| BMI, kg/m2 | 23.6 [21.2–25.4] | 22.0 [22.0–27.0] | 0.290 |
| Comorbidities, n (%) | |||
| T2DM | 17 (15.3) | 8 (50.0) | 0.003 |
| Hypertension | 39 (35.1) | 7 (43.8) | 0.695 |
| COPD | 4 (3.6) | 3 (18.8) | 0.218 |
| Chronic kidney disease | 2 (1.8) | 2 (12.5) | 0.127 |
| Laboratory profiles | |||
| White cell count, ×103/µL | 5880 [4610–7570] | 7030 [5940–11,720] | 0.034 |
| Lymphocyte count, ×103/µL | 1350 [946.4–1836.4] | 586.9 [500.0–689.4] | <0.001 |
| Hemoglobin, g/dL | 13.1 [12.1–14.2] | 12.4 [10.8–13.2] | 0.042 |
| Platelet count, ×109/µL | 234.0 [164.0–299.5] | 165.0 [124.5–268.5] | 0.038 |
| C reactive protein, mg/L | 1.2 [0.1–7.0] | 11.1 [7.6–15.4] | <0.001 |
| Aspartate aminotransferase, U/L | 31.0 [23.0–45.0] | 48.5 [31.5–63.5] | 0.004 |
| Alanine aminotransferase, U/L | 21.5 [15.0–37.0] | 30.0 [18.0–47.0] | 0.412 |
| Total bilirubin, mg/dL | 0.7 [0.5–1.0] | 0.8 [0.5–0.9] | 0.679 |
| Gamma glutamyl transferase, U/L | 24.0 [16.0–41.0] | 154.5 [75.0–323.0] | 0.010 |
| Creatinine kinase, U/L | 63.0 [45.0–94.0] | 122.0 [94.5–260.0] | 0.005 |
| Serum ferritin, ng/mL | 620.5 [317.6–1470.6] | 868.0 [766.5–2336.5] | 0.152 |
| Treatments, n (%) | |||
| Oxygen therapy | 14 (12.6) | 10 (62.5) | <0.001 |
| CRRT | 1 (0.9) | 2 (12.5) | 0.048 |
| ECMO | 4 (3.6) | 2 (12.5) | 0.348 |
| Clinical outcomes, n (%) | |||
| SIRS on admission | 25 (22.5) | 8 (43.8) | 0.128 |
| ICU admission | 11 (9.9) | 9 (56.2) | <0.001 |
| Septic shock | 9 (8.1) | 11 (68.8) | <0.001 |
| ARDS | 8 (7.2) | 12 (75.0) | <0.001 |
| Acute kidney injury | 3 (2.7) | 5 (31.2) | <0.001 |
| Body composition | |||
| SMI, cm2/m2 | 37.8 [33.2–43.2] | 43.0 [32.7–48.5] | 0.358 |
| VATI, cm2/m2 | 31.6 [19.9–46.7] | 48.2 [21.5–63.0] | 0.104 |
| SATI, cm2/m2 | 42.9 [29.6–59.5] | 36.3 [18.9–45.2] | 0.035 |
| VSR | 0.6 [0.4–1.3] | 1.3 [1.0–1.7] | 0.002 |
| Muscle HU | 41.9 [38.8–45.2] | 32.2 [28.0–37.7] | <0.001 |
| Sarcopenia, n (%) | 90 (81.1) | 13 (81.2) | 1.000 |
| Visceral adiposity, n (%) | 32 (28.8) | 8 (50.0) | 0.157 |
| Myosteatosis, n (%) | 5 (4.5) | 10 (62.5) | <0.001 |
| Duration of hospital stay, days | 27.0 [17.5–33.5] | 23.5 [9.0–49.0] | 0.942 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.066 (1.018–1.115) | 0.006 | ||
| Male | 0.230 (0.051–1.039) | 0.056 | ||
| BMI | 1.204 (1.027–1.411) | 0.042 | ||
| Type 2 DM | 4.054 (1.430–11.494) | 0.009 | 3.587 (1.218–10.562) | 0.020 |
| Lymphocyte count, ×103/µL | 0.998 (0.997–0.999) | 0.003 | 0.998 (0.997–1.000) | 0.065 |
| C reactive protein, mg/L | 1.074 (1.1017–1.135) | 0.011 | ||
| SIRS on admission | 3.297 (1.105–9.836) | 0.032 | ||
| Sarcopenia | 0.696 (0.191–2.533) | 0.583 | ||
| Visceral adiposity | 2.070 (0.745–5.753) | 0.163 | ||
| Myosteatosis | 8.182 (2.693–24.859) | <0.001 | 3.667 (1.195–11.250) | 0.023 |
| Fibrosis-4 index | 1.286 (1.152–1.436) | <0.001 | 1.213 (1.067–1.378) | 0.003 |
| Myosteatosis | ||
|---|---|---|
| HR (95% CI) | p-Value | |
| Unadjusted | 8.182 (2.693–24.859) | <0.001 |
| Age, sex-adjusted | 4.748 (1.432–15.740) | 0.011 |
| Multivariate model 1 | 4.585 (1.505–13.963) | 0.007 |
| Multivariate model 2 | 3.667 (1.195–11.250) | 0.023 |
| Multivariate model 3 | 3.667 (1.195–11.250) | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.-K.; Lee, Y.-R.; Song, J.-E.; Kweon, Y.-O.; Tak, W.-Y.; Jang, S.-Y.; Park, J.-G.; Park, S.-Y. Prognostic Impact of Myosteatosis on Mortality in Hospitalized Patients with COVID-19. Diagnostics 2022, 12, 2255. https://doi.org/10.3390/diagnostics12092255
Kang M-K, Lee Y-R, Song J-E, Kweon Y-O, Tak W-Y, Jang S-Y, Park J-G, Park S-Y. Prognostic Impact of Myosteatosis on Mortality in Hospitalized Patients with COVID-19. Diagnostics. 2022; 12(9):2255. https://doi.org/10.3390/diagnostics12092255
Chicago/Turabian StyleKang, Min-Kyu, Yu-Rim Lee, Jeung-Eun Song, Young-Oh Kweon, Won-Young Tak, Se-Young Jang, Jung-Gil Park, and Soo-Young Park. 2022. "Prognostic Impact of Myosteatosis on Mortality in Hospitalized Patients with COVID-19" Diagnostics 12, no. 9: 2255. https://doi.org/10.3390/diagnostics12092255
APA StyleKang, M. -K., Lee, Y. -R., Song, J. -E., Kweon, Y. -O., Tak, W. -Y., Jang, S. -Y., Park, J. -G., & Park, S. -Y. (2022). Prognostic Impact of Myosteatosis on Mortality in Hospitalized Patients with COVID-19. Diagnostics, 12(9), 2255. https://doi.org/10.3390/diagnostics12092255