
An AI-Powered Clinical Decision Support System to Predict Flares in Rheumatoid Arthritis: A Pilot Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Rheuma Care Manager (RCM) including Flare Prediction Tool
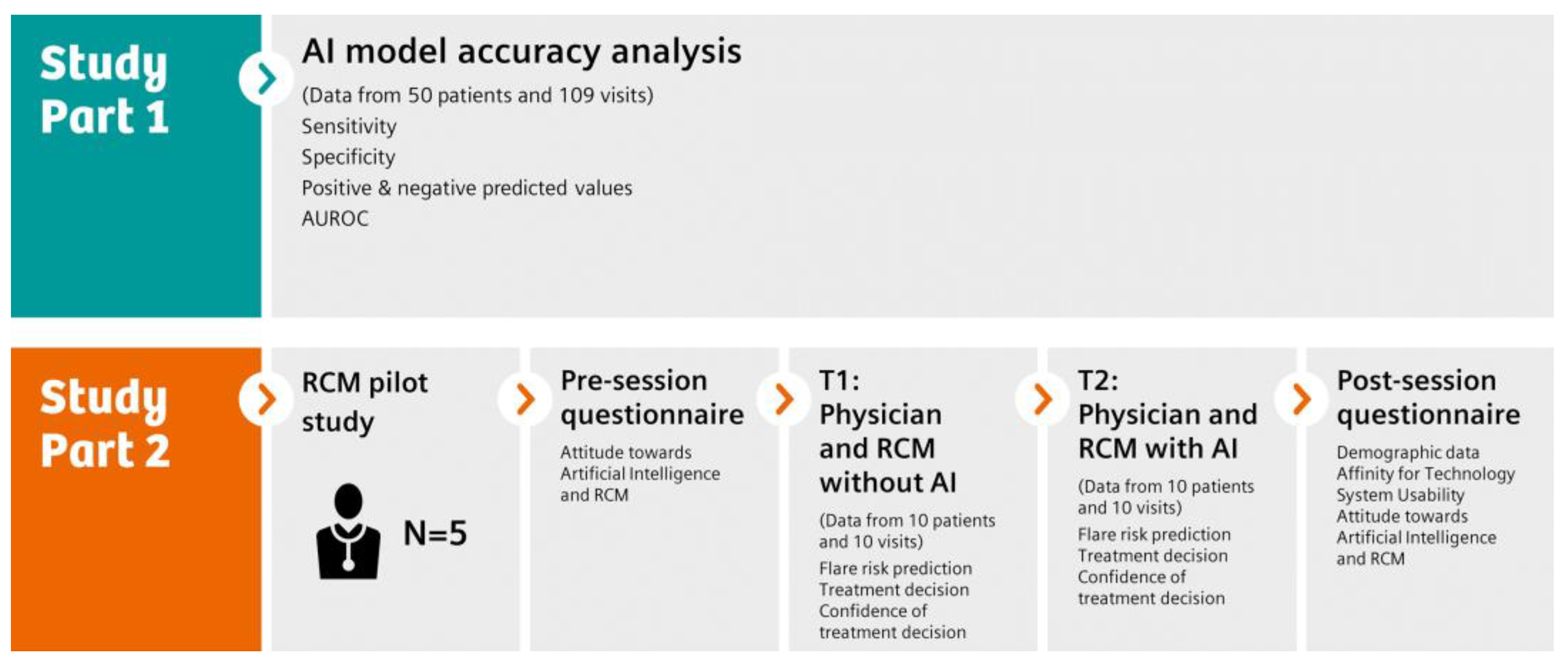
2.2. Study Design
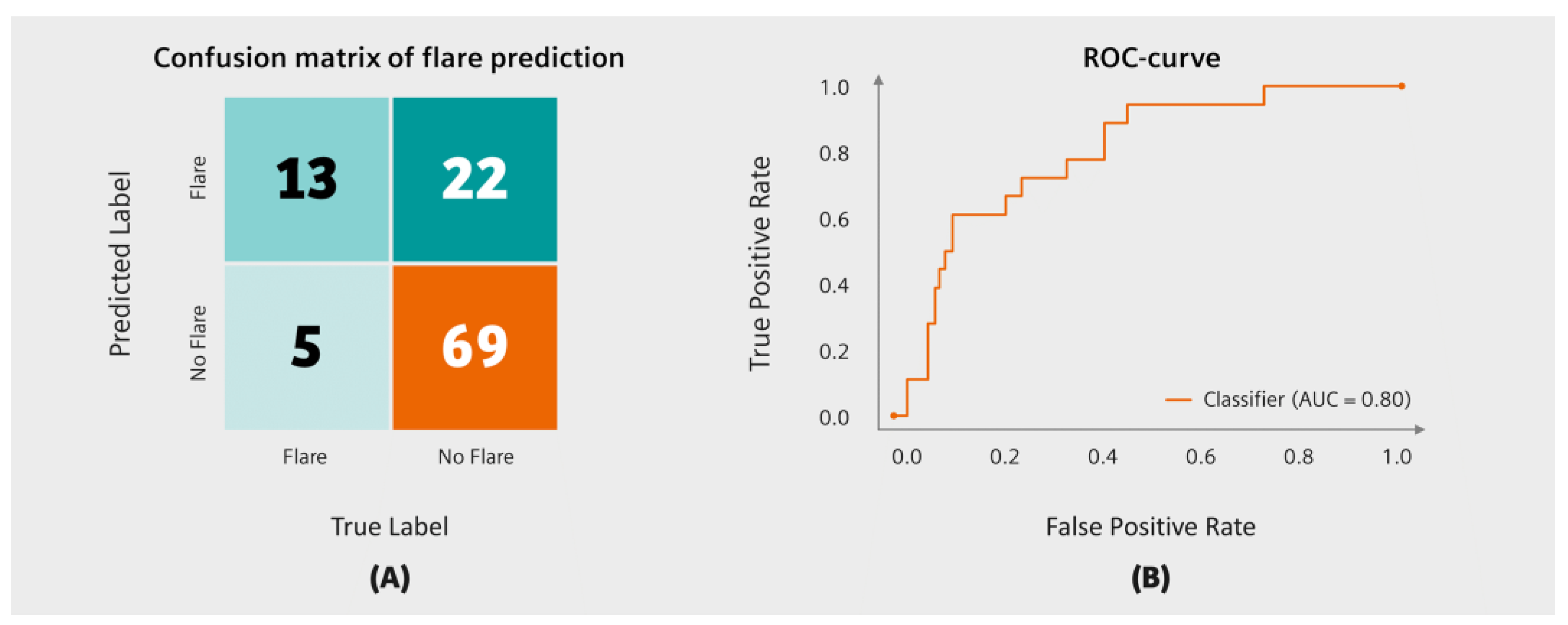
2.3. Flare Prediction Accuracy
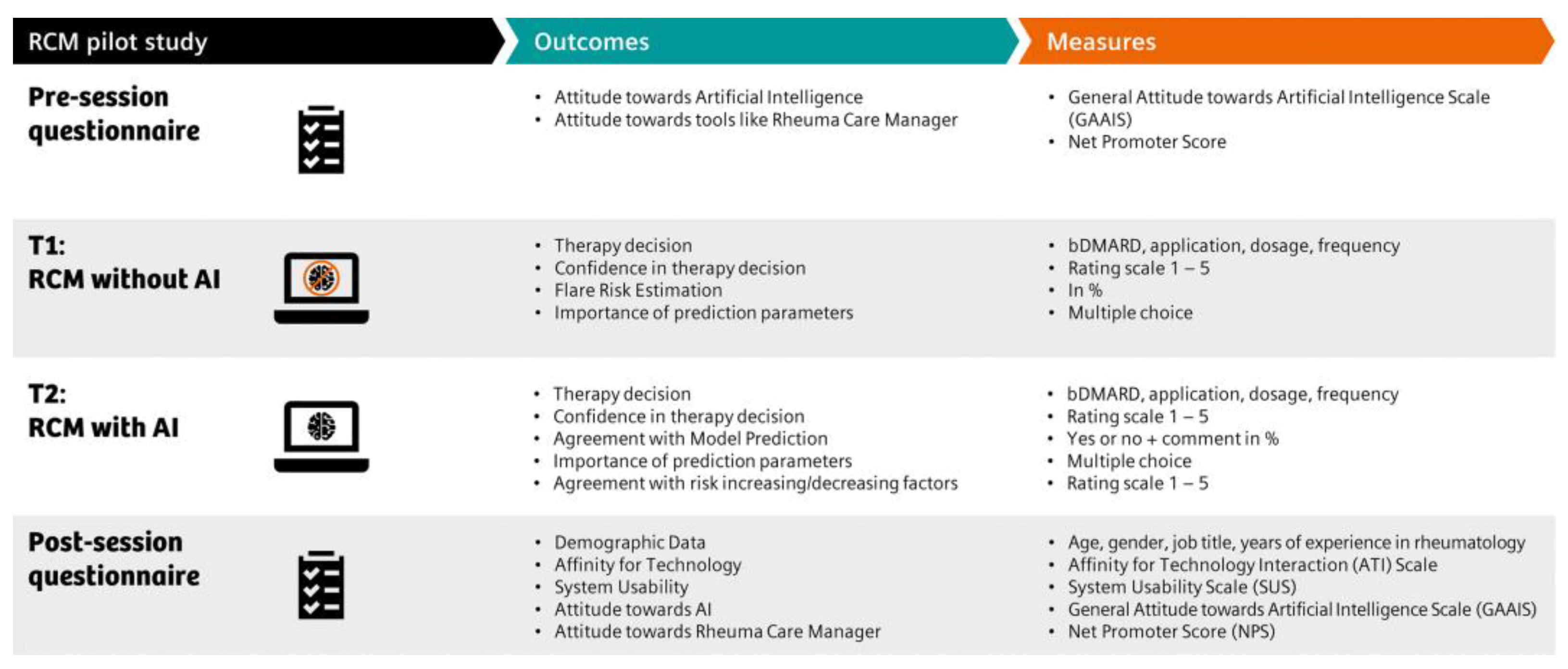
2.4. Attitudes towards Technology and AI
2.5. Comparison of Flare Prediction with and without Access to the Flare Risk Prediction Tool
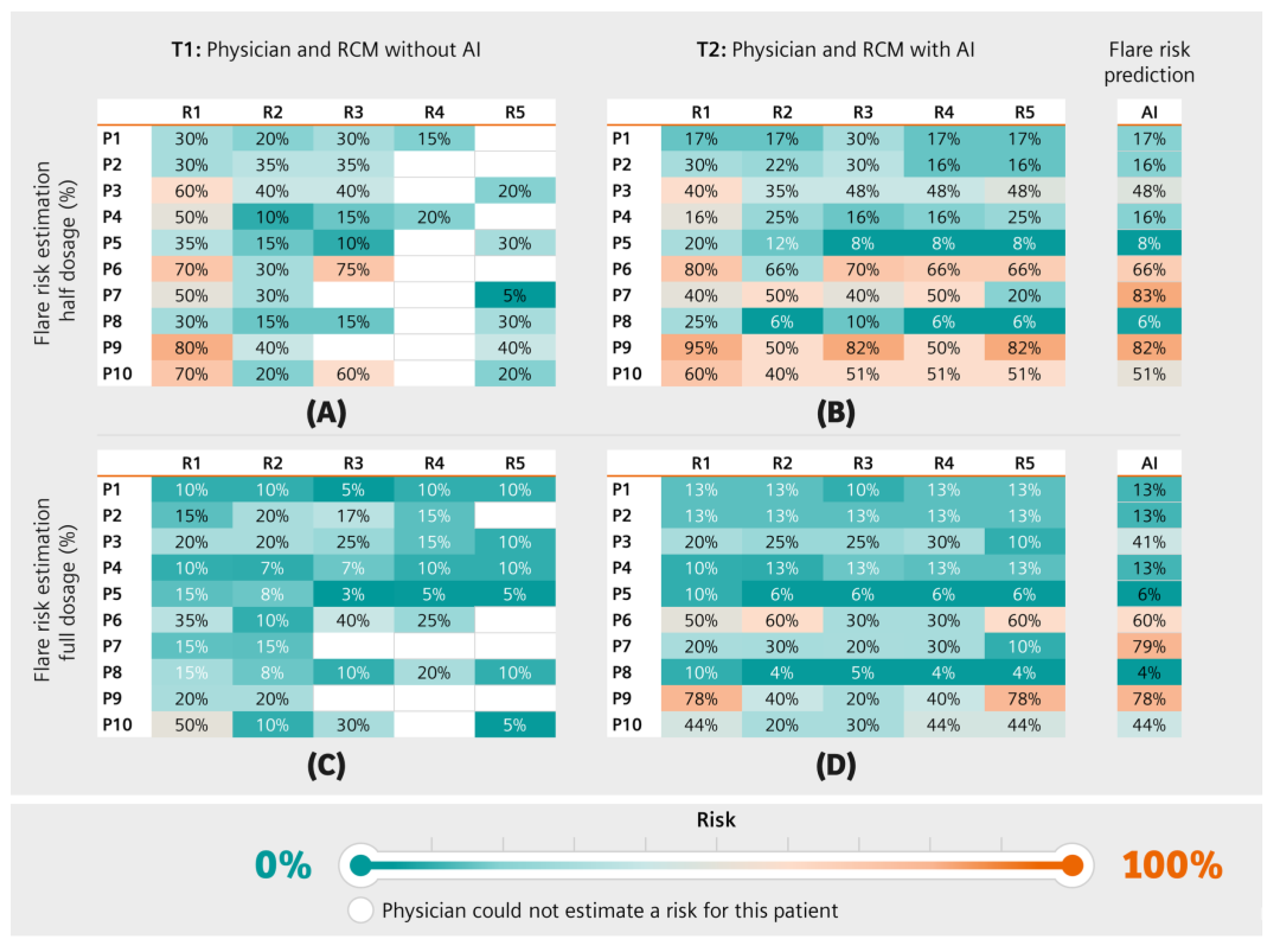
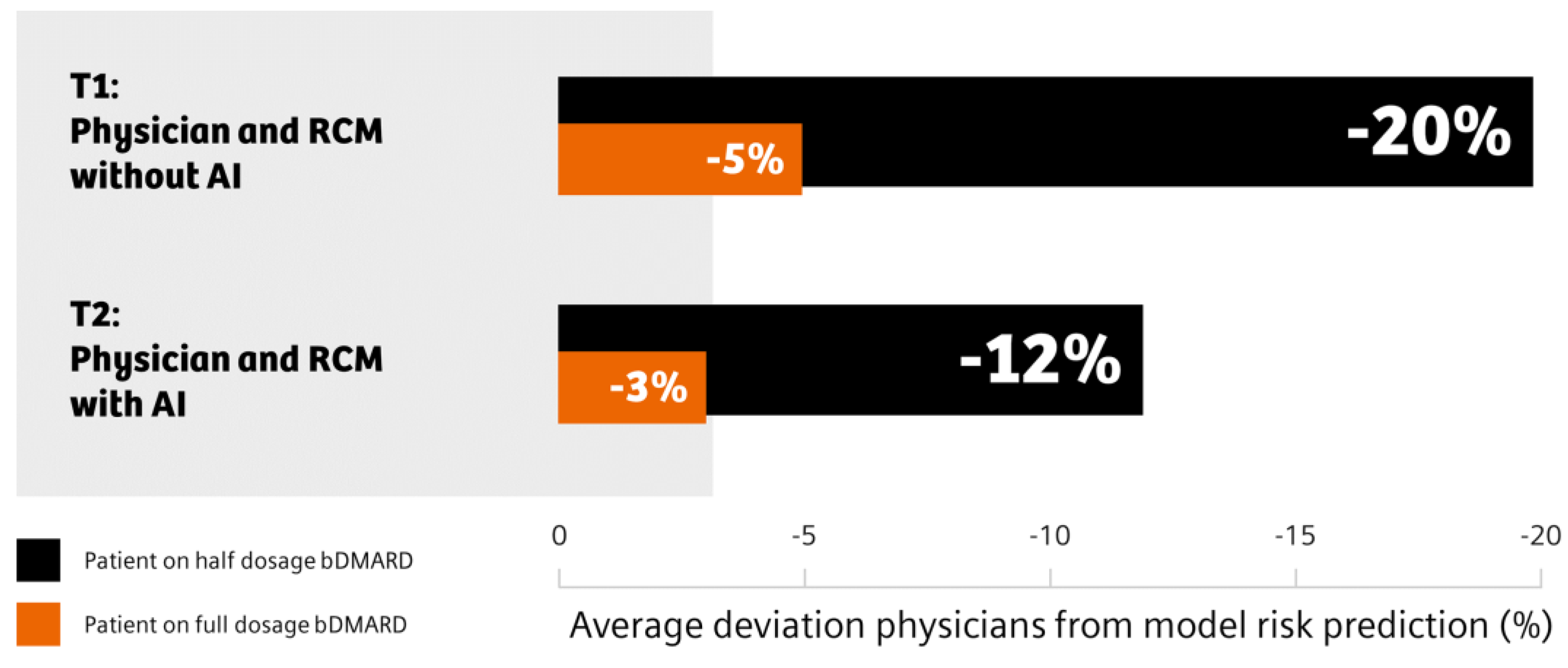
2.5.1. Flare Risk Estimation
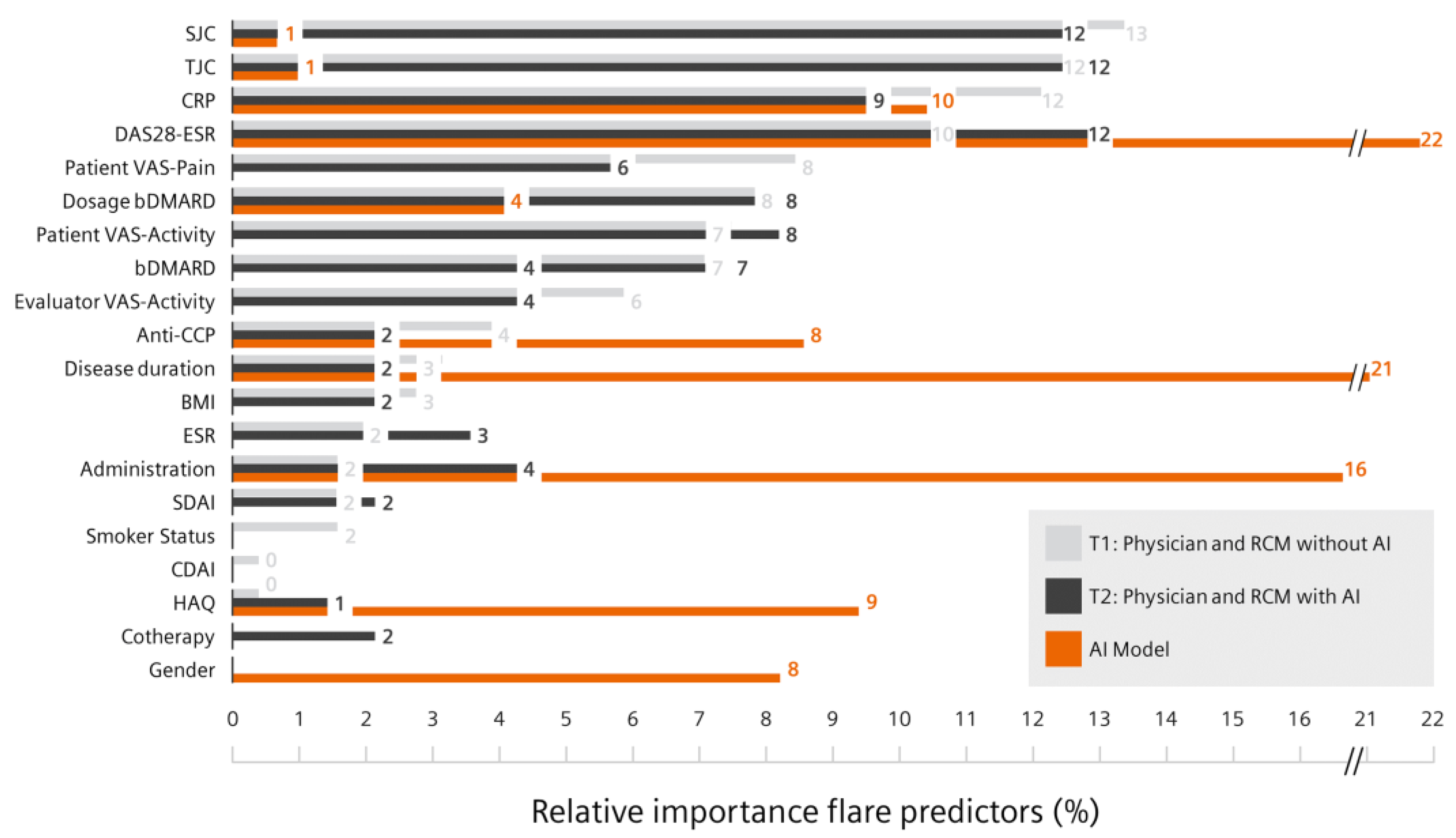
2.5.2. Patient Features Relevant for Flare Prediction
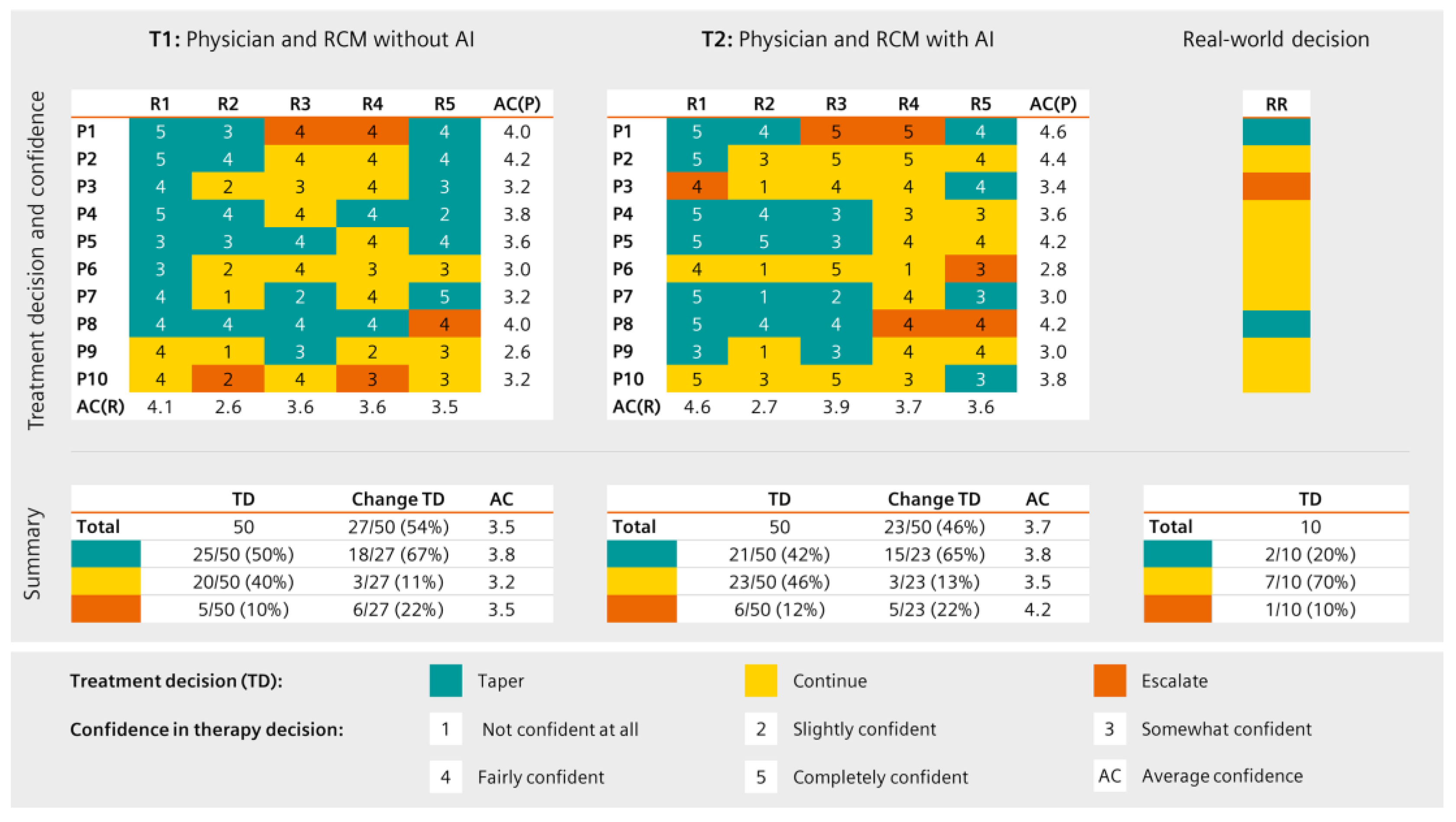
2.5.3. Therapeutic Decisions and Confidence
2.6. Inter-Rater Agreement
2.7. Usability and Acceptance
3. Results
3.1. Flare Prediction Accuracy
3.2. Pilot Study
3.2.1. Technology and AI Affinity
3.2.2. Flare Risk Prediction
3.2.3. Treatment Decisions and Perceived Confidence
3.2.4. RCM Usability and Acceptance
3.2.5. Perceived RCM Advantages and Barriers
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choy, E.H.; Panayi, G.S. Cytokine pathways and joint inflammation in rheumatoid arthritis. N. Engl. J. Med. 2001, 344, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Pincus, T.; Callahan, L.F. Taking mortality in rheumatoid arthritis seriously--predictive markers, socioeconomic status and comorbidity. J. Rheumatol. 1986, 13, 841–845. [Google Scholar] [PubMed]
- Schett, G.; Emery, P.; Tanaka, Y.; Burmester, G.; Pisetsky, D.S.; Naredo, E.; Fautrel, B.; van Vollenhoven, R. Tapering biologic and conventional DMARD therapy in rheumatoid arthritis: Current evidence and future directions. Ann. Rheum. Dis. 2016, 75, 1428–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraenkel, L.; Bathon, J.M.; England, B.R.; St Clair, E.W.; Arayssi, T.; Carandang, K.; Deane, K.D.; Genovese, M.; Huston, K.K.; Kerr, G.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. (Hoboken) 2021, 73, 924–939. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewe, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [Green Version]
- Aga, A.B.; Lie, E.; Uhlig, T.; Olsen, I.C.; Wierod, A.; Kalstad, S.; Rodevand, E.; Mikkelsen, K.; Kvien, T.K.; Haavardsholm, E.A. Time trends in disease activity, response and remission rates in rheumatoid arthritis during the past decade: Results from the NOR-DMARD study 2000–2010. Ann. Rheum. Dis. 2015, 74, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Haschka, J.; Englbrecht, M.; Hueber, A.J.; Manger, B.; Kleyer, A.; Reiser, M.; Finzel, S.; Tony, H.P.; Kleinert, S.; Feuchtenberger, M.; et al. Relapse rates in patients with rheumatoid arthritis in stable remission tapering or stopping antirheumatic therapy: Interim results from the prospective randomised controlled RETRO study. Ann. Rheum. Dis. 2016, 75, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Rech, J.; Hueber, A.J.; Finzel, S.; Englbrecht, M.; Haschka, J.; Manger, B.; Kleyer, A.; Reiser, M.; Cobra, J.F.; Figueiredo, C.; et al. Prediction of disease relapses by multibiomarker disease activity and autoantibody status in patients with rheumatoid arthritis on tapering DMARD treatment. Ann. Rheum. Dis. 2016, 75, 1637–1644. [Google Scholar] [CrossRef]
- van der Woude, D.; Young, A.; Jayakumar, K.; Mertens, B.J.; Toes, R.E.; van der Heijde, D.; Huizinga, T.W.; van der Helm-van Mil, A.H. Prevalence of and predictive factors for sustained disease-modifying antirheumatic drug-free remission in rheumatoid arthritis: Results from two large early arthritis cohorts. Arthritis Rheum. 2009, 60, 2262–2271. [Google Scholar] [CrossRef]
- Grove, W.M.; Zald, D.H.; Lebow, B.S.; Snitz, B.E.; Nelson, C. Clinical versus mechanical prediction: A meta-analysis. Psychol. Assess. 2000, 12, 19–30. [Google Scholar] [CrossRef]
- Miller, D.D.; Brown, E.W. Artificial Intelligence in Medical Practice: The Question to the Answer? Am. J. Med. 2018, 131, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Hunt, D.L.; Haynes, R.B.; Hanna, S.E.; Smith, K. Effects of computer-based clinical decision support systems on physician performance and patient outcomes: A systematic review. JAMA 1998, 280, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ 2005, 330, 765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Roa, A.A.; Arevalo Ovalle, J.E.; Madabhushi, A.; Gonzalez Osorio, F.A. A deep learning architecture for image representation, visual interpretability and automated basal-cell carcinoma cancer detection. In Medical Image Computing and Computer-Assisted Intervention—MICCAI 2013; Springer: Berlin/Heidelberg, Germany, 2013; Volume 16, pp. 403–410. [Google Scholar] [CrossRef]
- Wang, D.; Khosla, A.; Gargeya, R.; Irshad, H.; Beck, A.H. Deep Learning for Identifying Metastatic Breast Cancer. Available online: https://arxiv.org/pdf/1606.05718v1.pdf (accessed on 20 July 2022).
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [Green Version]
- Schnyer, D.M.; Clasen, P.C.; Gonzalez, C.; Beevers, C.G. Evaluating the diagnostic utility of applying a machine learning algorithm to diffusion tensor MRI measures in individuals with major depressive disorder. Psychiatry Res. Neuroimaging 2017, 264, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vodencarevic, A.; Tascilar, K.; Hartmann, F.; Reiser, M.; Hueber, A.J.; Haschka, J.; Bayat, S.; Meinderink, T.; Knitza, J.; Mendez, L.; et al. Advanced machine learning for predicting individual risk of flares in rheumatoid arthritis patients tapering biologic drugs. Arthritis Res. Ther. 2021, 23, 67. [Google Scholar] [CrossRef] [PubMed]
- Tascilar, K.; Hagen, M.; Kleyer, A.; Simon, D.; Reiser, M.; Hueber, A.J.; Manger, B.; Englbrecht, M.; Finzel, S.; Tony, H.P.; et al. Treatment tapering and stopping in patients with rheumatoid arthritis in stable remission (RETRO): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Rheumatol. 2021, 3, e767–e777. [Google Scholar] [CrossRef]
- Lundberg, S.M. GitHub—Slundberg/Shap: A Game Theoretic Approach to Explain the Output of Any Machine Learning Model. Available online: https://github.com/slundberg/shap (accessed on 26 July 2022).
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. In Proceedings of the 1st Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2007. [Google Scholar]
- Paskin, N. Toward unique identifiers. In Proceedings of the IEEE; IEEE: Piscataway, NJ, USA, 1999; Volume 87, pp. 1208–1227. [Google Scholar]
- Franke, T.; Attig, C.; Wessel, D. A Personal Resource for Technology Interaction: Development and Validation of the Affinity for Technology Interaction (ATI) Scale. Int. J. Hum. Comput. Interact. 2019, 35, 456–467. [Google Scholar] [CrossRef]
- Schepman, A.; Rodway, P. Initial validation of the general attitudes towards Artificial Intelligence Scale. Comput. Hum. Behav. Rep. 2020, 1, 100014. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Brooke, J. SUS—A Quick and Dirty Usability Scale. Available online: https://hell.meiert.org/core/pdf/sus.pdf (accessed on 26 July 2022).
- Lewis, J.R.; Sauro, J. The Factor Structure of the System Usability Scale. In Proceedings of the International Conference on Human Centered Design, San Diego, CA, USA, 19–24 July 2009; pp. 94–103. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.T.; Miller, J.T. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Reichheld, F.F. The one number you need to grow. Harv. Bus. Rev. 2003, 81, 46–54, 124. [Google Scholar] [PubMed]
- Alder, H.; Marx, C.; Steurer, J.; Wertli, M.; Korner-Nievergelt, P.; Tamborrini, G.; Langenegger, T.; Eichholzer, A.; Andor, M.; Krebs, A.; et al. RheumaTool, a novel clinical decision support system for the diagnosis of rheumatic diseases, and its first validation in a retrospective chart analysis. Swiss Med. Wkly. 2020, 150, w20369. [Google Scholar] [CrossRef] [PubMed]
- Knitza, J.; Tascilar, K.; Gruber, E.; Kaletta, H.; Hagen, M.; Liphardt, A.M.; Schenker, H.; Krusche, M.; Wacker, J.; Kleyer, A.; et al. Accuracy and usability of a diagnostic decision support system in the diagnosis of three representative rheumatic diseases: A randomized controlled trial among medical students. Arthritis Res. Ther. 2021, 23, 233. [Google Scholar] [CrossRef]
- Messelink, M.A.; van der Leeuw, M.S.; den Broeder, A.A.; Tekstra, J.; van der Goes, M.C.; Heijstek, M.W.; Lafeber, F.; Welsing, P.M.J. Prediction Aided Tapering In rheumatoid arthritis patients treated with biOlogicals (PATIO): Protocol for a randomized controlled trial. Trials 2022, 23, 494. [Google Scholar] [CrossRef]
- Venerito, V.; Angelini, O.; Fornaro, M.; Cacciapaglia, F.; Lopalco, G.; Iannone, F. A Machine Learning Approach for Predicting Sustained Remission in Rheumatoid Arthritis Patients on Biologic Agents. J. Clin. Rheumatol. 2022, 28, e334–e339. [Google Scholar] [CrossRef]
- Venerito, V.; Emmi, G.; Cantarini, L.; Leccese, P.; Fornaro, M.; Fabiani, C.; Lascaro, N.; Coladonato, L.; Mattioli, I.; Righetti, G.; et al. Validity of Machine Learning in Predicting Giant Cell Arteritis Flare After Glucocorticoids Tapering. Front. Immunol. 2022, 13, 860877. [Google Scholar] [CrossRef]
- Dong, Z.; Lin, Y.; Lin, F.; Luo, X.; Lin, Z.; Zhang, Y.; Li, L.; Li, Z.P.; Feng, S.T.; Cai, H.; et al. Prediction of Early Treatment Response to Initial Conventional Transarterial Chemoembolization Therapy for Hepatocellular Carcinoma by Machine-Learning Model Based on Computed Tomography. J. Hepatocell. Carcinoma 2021, 8, 1473–1484. [Google Scholar] [CrossRef]
- Morshid, A.; Elsayes, K.M.; Khalaf, A.M.; Elmohr, M.M.; Yu, J.; Kaseb, A.O.; Hassan, M.; Mahvash, A.; Wang, Z.; Hazle, J.D.; et al. A machine learning model to predict hepatocellular carcinoma response to transcatheter arterial chemoembolization. Radiol. Artif. Intell. 2019, 1, e180021. [Google Scholar] [CrossRef] [PubMed]
- Komiya, T.; Takase-Minegishi, K.; Sakurai, N.; Nagai, H.; Hamada, N.; Soejima, Y.; Sugiyama, Y.; Tsuchida, N.; Kunishita, Y.; Kishimoto, D.; et al. Dose down-titration of biological disease-modifying antirheumatic drugs in daily clinical practice: Shared decision-making and patient treatment preferences in Japanese patients with rheumatoid arthritis. Int. J. Rheum. Dis. 2019, 22, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Dierckx, S.; Sokolova, T.; Lauwerys, B.R.; Avramovska, A.; de Bellefon, L.M.; Toukap, A.N.; Stoenoiu, M.; Houssiau, F.A.; Durez, P. Tapering of biological antirheumatic drugs in rheumatoid arthritis patients is achievable and cost-effective in daily clinical practice: Data from the Brussels UCLouvain RA Cohort. Arthritis Res. Ther. 2020, 22, 96. [Google Scholar] [CrossRef]
- Krause, D.; Krause, C.; Rudolf, H.; Baraliakos, X.; Braun, J.; Schmitz, E. Dose tapering of biologic agents in patients with rheumatoid arthritis-results from a cohort study in Germany. Clin. Rheumatol. 2021, 40, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Redelmeier, D.; Ruff, C.C.; Tobler, P.N. Cognitive biases associated with medical decisions: A systematic review. BMC Med. Inform. Decis. Mak. 2016, 16, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips-Wren, G.; Adya, M. Decision making under stress: The role of information overload, time pressure, complexity, and uncertainty. J. Decis. Syst. 2020, 29, 213–225. [Google Scholar] [CrossRef]
- Ranganath, V.K.; Hammer, H.B.; McQueen, F.M. Contemporary imaging of rheumatoid arthritis: Clinical role of ultrasound and MRI. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101593. [Google Scholar] [CrossRef]
- Han, J.; Geng, Y.; Deng, X.; Zhang, Z. Subclinical Synovitis Assessed by Ultrasound Predicts Flare and Progressive Bone Erosion in Rheumatoid Arthritis Patients with Clinical Remission: A Systematic Review and Metaanalysis. J. Rheumatol. 2016, 43, 2010–2018. [Google Scholar] [CrossRef]
- Orange, D.E.; Yao, V.; Sawicka, K.; Fak, J.; Frank, M.O.; Parveen, S.; Blachere, N.E.; Hale, C.; Zhang, F.; Raychaudhuri, S.; et al. RNA Identification of PRIME Cells Predicting Rheumatoid Arthritis Flares. N. Engl. J. Med. 2020, 383, 218–228. [Google Scholar] [CrossRef]
- Kameda, H.; Hirata, A.; Katagiri, T.; Takakura, Y.; Inoue, Y.; Takenaka, S.; Ito, H.; Mizushina, K.; Ogura, T. Prediction of disease flare by biomarkers after discontinuing biologics in patients with rheumatoid arthritis achieving stringent remission. Sci. Rep. 2021, 11, 6865. [Google Scholar] [CrossRef]
- O’Neil, L.J.; Hu, P.; Liu, Q.; Islam, M.M.; Spicer, V.; Rech, J.; Hueber, A.; Anaparti, V.; Smolik, I.; El-Gabalawy, H.S.; et al. Proteomic Approaches to Defining Remission and the Risk of Relapse in Rheumatoid Arthritis. Front. Immunol. 2021, 12, 729681. [Google Scholar] [CrossRef] [PubMed]
- Fautrel, B.; Pham, T.; Alfaiate, T.; Gandjbakhch, F.; Foltz, V.; Morel, J.; Dernis, E.; Gaudin, P.; Brocq, O.; Solau-Gervais, E.; et al. Step-down strategy of spacing TNF-blocker injections for established rheumatoid arthritis in remission: Results of the multicentre non-inferiority randomised open-label controlled trial (STRASS: Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study). Ann. Rheum. Dis. 2016, 75, 59–67. [Google Scholar] [CrossRef] [PubMed]
- van Herwaarden, N.; van der Maas, A.; Minten, M.J.; van den Hoogen, F.H.; Kievit, W.; van Vollenhoven, R.F.; Bijlsma, J.W.; van den Bemt, B.J.; den Broeder, A.A. Disease activity guided dose reduction and withdrawal of adalimumab or etanercept compared with usual care in rheumatoid arthritis: Open label, randomised controlled, non-inferiority trial. BMJ 2015, 350, h1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- den Broeder, N.; Bouman, C.A.M.; Kievit, W.; van Herwaarden, N.; van den Hoogen, F.H.J.; van Vollenhoven, R.F.; Bijlsma, H.W.J.; van der Maas, A.; den Broeder, A.A. Three-year cost-effectiveness analysis of the DRESS study: Protocolised tapering is key. Ann. Rheum. Dis. 2019, 78, 141–142. [Google Scholar] [CrossRef]
- Thyberg, I.; Dahlstrom, O.; Bjork, M.; Arvidsson, P.; Thyberg, M. Potential of the HAQ score as clinical indicator suggesting comprehensive multidisciplinary assessments: The Swedish TIRA cohort 8 years after diagnosis of RA. Clin. Rheumatol. 2012, 31, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, H.A.; Baker, J.F.; Conaghan, P.G.; Emery, P.; Huizinga, T.W.J.; Elbez, Y.; Banerjee, S.; Ostergaard, M. Prediction of flare following remission and treatment withdrawal in early rheumatoid arthritis: Post hoc analysis of a phase IIIb trial with abatacept. Arthritis Res. Ther. 2022, 24, 47. [Google Scholar] [CrossRef]
- Oh, Y.J.; Moon, K.W. Predictors of Flares in Patients with Rheumatoid Arthritis Who Exhibit Low Disease Activity: A Nationwide Cohort Study. J. Clin. Med. 2020, 9, 3219. [Google Scholar] [CrossRef]
- Krusche, M.; Klemm, P.; Grahammer, M.; Mucke, J.; Vossen, D.; Kleyer, A.; Sewerin, P.; Knitza, J. Acceptance, Usage, and Barriers of Electronic Patient-Reported Outcomes Among German Rheumatologists: Survey Study. JMIR mHealth uHealth 2020, 8, e18117. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics Study Part 1 (n = 50) | |
|---|---|
| DAS-28 ESR, units | 1.32 (0.61) |
| Disease duration, years | 11.34 (9.61) |
| IV administration, N (%) | 38 (34.9) |
| Anti-CCP positive, N (%) | 73 (66.9) |
| Female gender, N (%) | 65 (59.6) |
| HAQ, mean score | 0.38 (0.8) |
| CRP, mg/dL | 0.3 (0.78) |
| Full dosage bDMARD, visits (%) | 334 (70.5) |
| SJC, N | 0.2 (0.66) |
| TJC, N | 0.17 (0.48) |
| Patient Characteristics Study Part 2 (n = 10) | |
|---|---|
| Age, years | 57.7 (6.2) |
| Female gender, N (%) | 7 (70) |
| Disease duration, years | 15.7 (10.8) |
| Smoking, N (%) | |
| Current smoker | 4 (40) |
| Ex-smoker | 2 (20) |
| Never smoker | 3 (30) |
| Remission duration, months | 58.3 (7.6) |
| DAS-28 ESR, units | 1.5 (0.6) |
| TJC, N | 0.65 (0.81) |
| SJC, N | 0.36 (0.44) |
| CRP, mg/dL | 4.8 (4.1) |
| Patient VAS activity (mm) | 12.6 (7.35) |
| IV administration, N (%) | 7 (70) |
| Evaluator VAS activity (mm) | 7.3 (5.4) |
| ESR, mm/h | 6.2 (3.5) |
| (Current) anti-CCP positive, N (%) | 8 (80) |
| BMI, kg/m² | 27.8 (6.9) |
| SDAI, units | 7.8 (4.7) |
| HAQ, units | 0.9 (0.8) |
| CDAI, units | 2.7 (2) |
| Methotrexate use, N (%) | 4 (40) |
| Other csDMARD use, N (%) | 3 (30) |
| bDMARD use, N (%) | 10 (100) |
| Adalimumab | 2 (20) |
| Tocilizumab | 5 (50) |
| Certolizumab pegol | 1 (10) |
| Rituximab | 2 (20) |
| (Current) dosage, % | 80 (27.4) |
| Patients with flare, N (%) | 3 (30) |
| Patient (P) | Characteristics (Reason for Selection) |
|---|---|
| P1 | Low disease duration |
| P2 | High CRP |
| P3 | High CRP |
| P4 | High TJC |
| P5 | High disease duration, low DAS28 |
| P6 | High HAQ |
| P7 | High disease duration, high DAS28 |
| P8 | At least one TJC and SJC |
| P9 | Random |
| P10 | Random |
| Rater (R) | GAAIS | NPS | ATI | SUS | ||||
|---|---|---|---|---|---|---|---|---|
| Positive Subscale | Negative Subscale | |||||||
| Pre-Study | Post-Study | Pre-Study | Post-Study | Pre-Study | Post-Study | |||
| R1 | 4.75 | 5.00 | 3.88 | 4.25 | 9 | 10 | 4.33 | 100.0 |
| R2 | 4.08 | 4.25 | 3.13 | 3.63 | 7 | 6 | 4.22 | 80.0 |
| R3 | 4.50 | 4.58 | 3.63 | 3.50 | 7 | 7 | 4.67 | 92.5 |
| R4 | 3.50 | 3.67 | 4.13 | 4.38 | 9 | 7 | 3.78 | 75.0 |
| R5 | 3.67 | 3.33 | 3.50 | 3.63 | 8 | 5 | 3.67 | 62.5 |
| Mean | 4.10 | 4.17 | 3.65 | 3.88 | 8 | 7 | 4.13 | 82 |
| SD | 0.53 | 0.67 | 0.38 | 0.41 | 1 | 1.87 | 0.41 | 14.73 |
| Advantages Mentioned | Problems Mentioned |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labinsky, H.; Ukalovic, D.; Hartmann, F.; Runft, V.; Wichmann, A.; Jakubcik, J.; Gambel, K.; Otani, K.; Morf, H.; Taubmann, J.; et al. An AI-Powered Clinical Decision Support System to Predict Flares in Rheumatoid Arthritis: A Pilot Study. Diagnostics 2023, 13, 148. https://doi.org/10.3390/diagnostics13010148
Labinsky H, Ukalovic D, Hartmann F, Runft V, Wichmann A, Jakubcik J, Gambel K, Otani K, Morf H, Taubmann J, et al. An AI-Powered Clinical Decision Support System to Predict Flares in Rheumatoid Arthritis: A Pilot Study. Diagnostics. 2023; 13(1):148. https://doi.org/10.3390/diagnostics13010148
Chicago/Turabian StyleLabinsky, Hannah, Dubravka Ukalovic, Fabian Hartmann, Vanessa Runft, André Wichmann, Jan Jakubcik, Kira Gambel, Katharina Otani, Harriet Morf, Jule Taubmann, and et al. 2023. "An AI-Powered Clinical Decision Support System to Predict Flares in Rheumatoid Arthritis: A Pilot Study" Diagnostics 13, no. 1: 148. https://doi.org/10.3390/diagnostics13010148
APA StyleLabinsky, H., Ukalovic, D., Hartmann, F., Runft, V., Wichmann, A., Jakubcik, J., Gambel, K., Otani, K., Morf, H., Taubmann, J., Fagni, F., Kleyer, A., Simon, D., Schett, G., Reichert, M., & Knitza, J. (2023). An AI-Powered Clinical Decision Support System to Predict Flares in Rheumatoid Arthritis: A Pilot Study. Diagnostics, 13(1), 148. https://doi.org/10.3390/diagnostics13010148