
Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers for VTE in Trauma-Immobilized Patients

 ,
,
Abstract
:1. Introduction
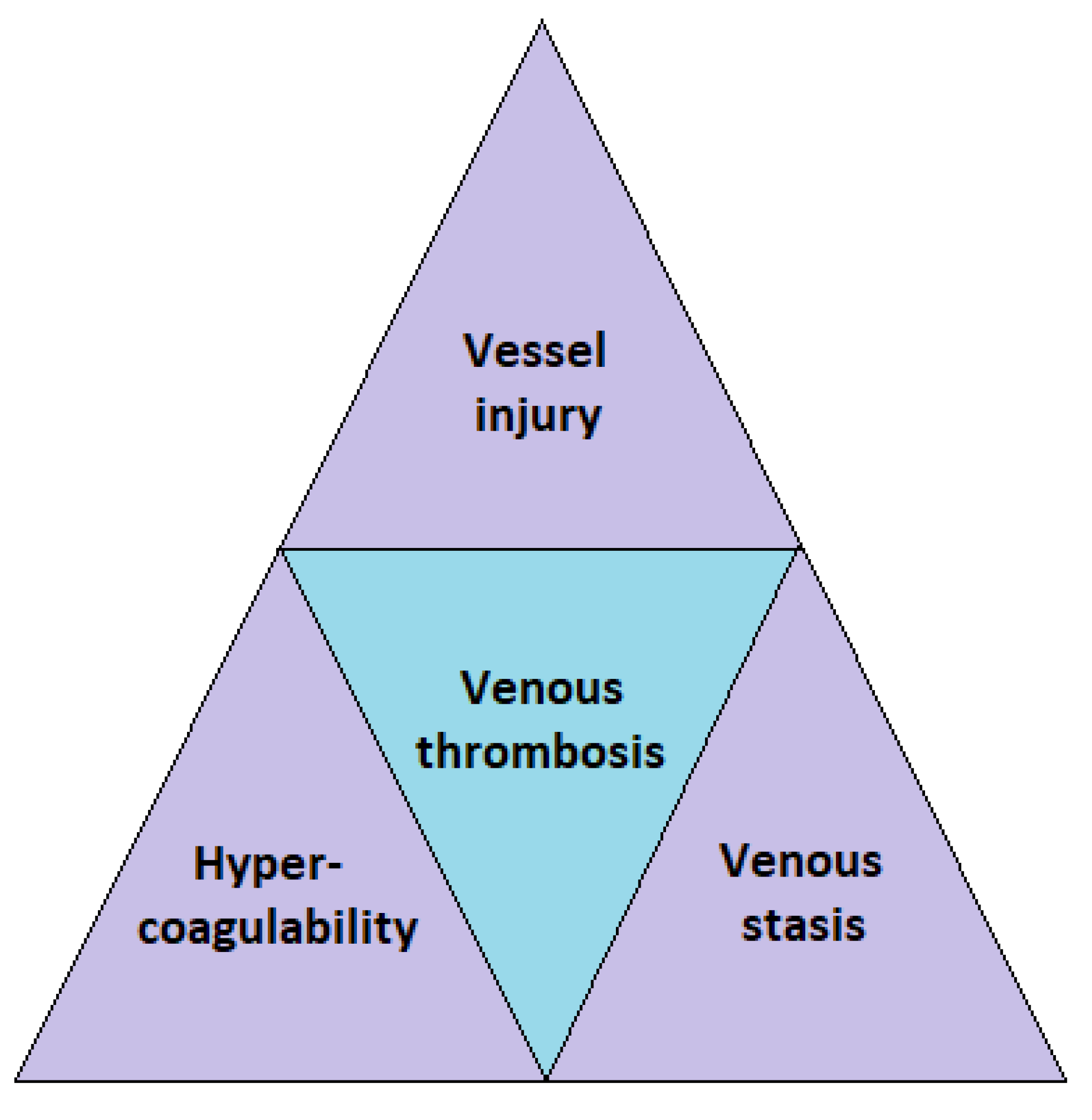
2. VTE in Trauma and Immobilized Patients
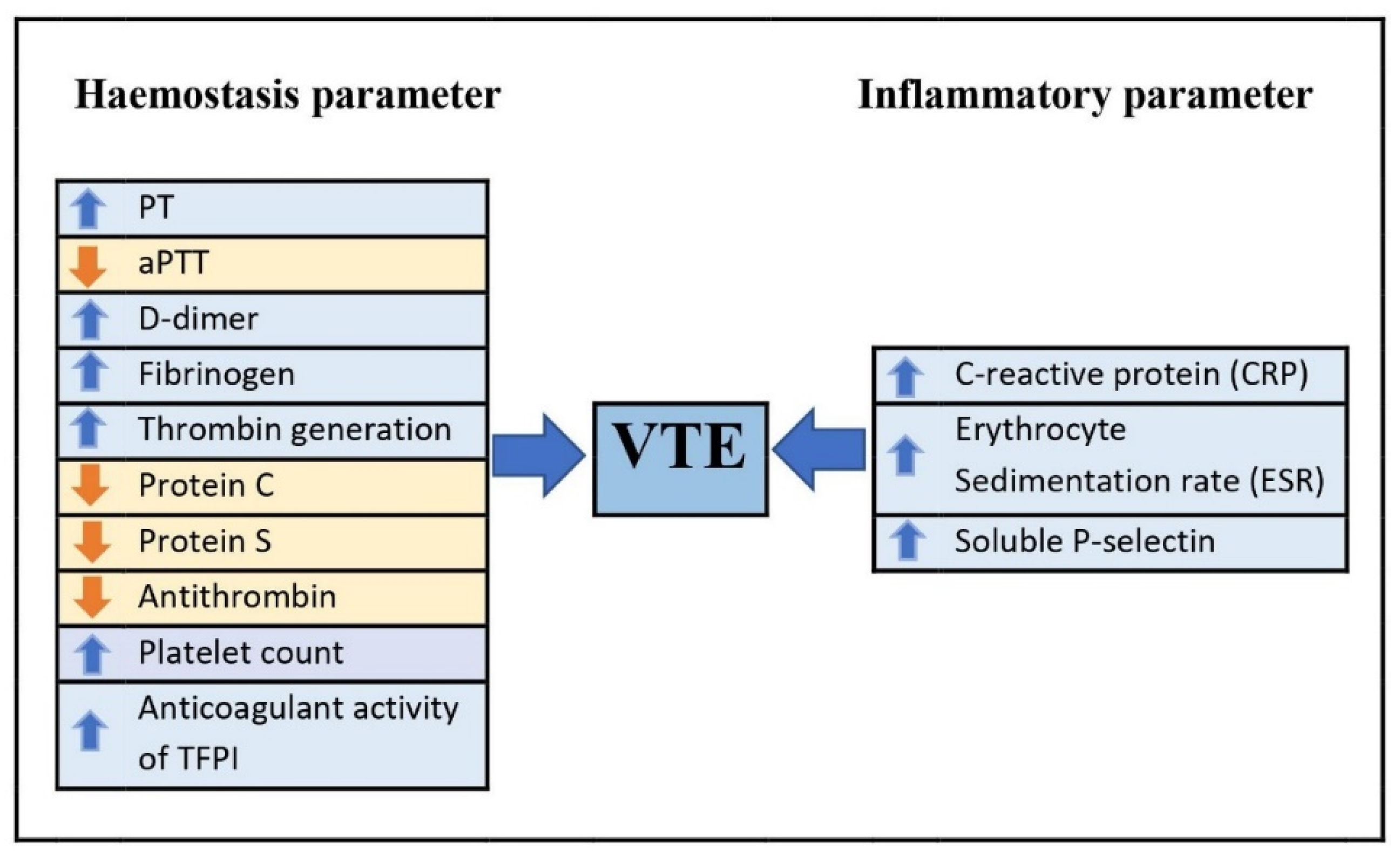
3. Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers in Diagnosing VTE
3.1. Effect of Trauma and Immobilization on Haemostasis Parameters
3.1.1. Prothrombin Time (PT) and activated Partial Thromboplastin Time (aPTT)
3.1.2. D-dimer
3.1.3. Fibrinogen
3.1.4. Thrombin Generation
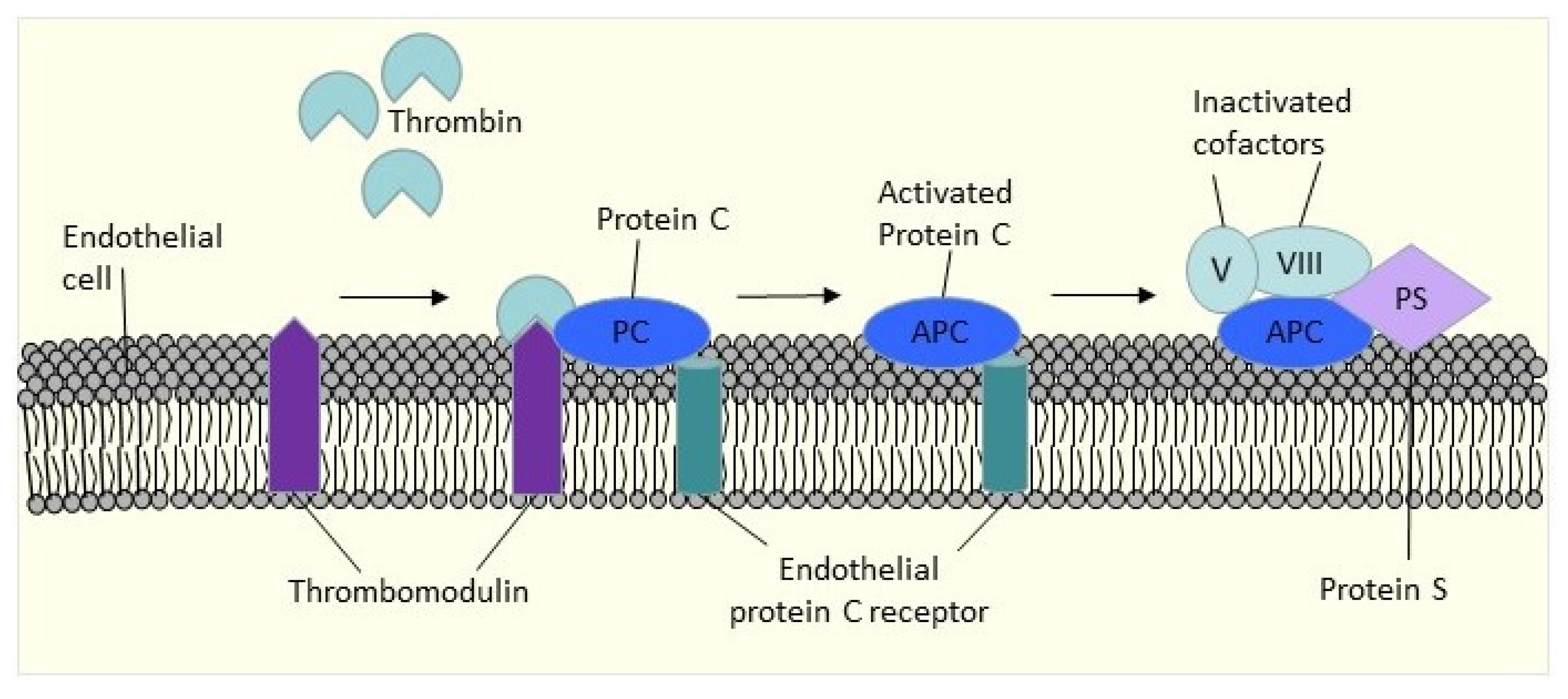
3.1.5. Protein C, Protein S, and Antithrombin
3.1.6. Platelet
3.1.7. Tissue Factor Pathway Inhibitor
3.2. Effect of Trauma and Immobilization on Inflammatory Parameters
3.2.1. C- Reactive Protein (CRP)
3.2.2. Erythrocyte Sedimentation Rate (ESR)
3.2.3. Soluble P-Selectin
4. Imaging Techniques in Diagnosing VTE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beckman, M.G.; Hooper, W.C.; Critchley, S.E.; Ortel, T.L. Venous thromboembolism: A public health concern. Am. J. Prev. Med. 2010, 38 (Suppl. S4), S495–S501. [Google Scholar] [CrossRef] [PubMed]
- Lichte, P.; Kobbe, P.; Almahmoud, K.; Pfeifer, R.; Andruszkow, H.; Hildebrand, F.; Lefering, R.; Pape, H.-C. Post-traumatic thrombo-embolic complications in polytrauma patients. Int. Orthop. 2015, 39, 947–954. [Google Scholar] [CrossRef]
- Paffrath, T.; Wafaisade, A.; Lefering, R.; Simanski, C.; Bouillon, B.; Spanholtz, T.; Wutzler, S.; Maegele, M.; Trauma Registry of DGU. Venous thromboembolism after severe trauma: Incidence, risk factors and outcome. Injury 2010, 41, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P. Acquired Risk Factors for Venous Thromboembolism in Medical Patients. Hematol. Am. Soc. Hematol. Educ. Program 2005, 2005, 458–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosse, S.D.; Nelson, R.E.; Nyarko, K.A.; Richardson, L.C.; Raskob, G.E. The economic burden of incident venous thromboembolism in the United States: A review of estimated attributable healthcare costs. Thromb. Res. 2016, 137, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerts, W.H.; Pineo, G.F.; Heit, J.A.; Bergqvist, D.; Lassen, M.R.; Colwell, C.W.; Ray, J.G. Prevention of Venous Thromboembolism: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004, 126 (Suppl. S3), 338S–400S. [Google Scholar] [CrossRef]
- Selby, R.; Geerts, W.; Ofosu, F.A.; Craven, S.; Dewar, L.; Phillips, A.; Szalai, J.P. Hypercoagulability after trauma: Hemostatic changes and relationship to venous thromboembolism. Thromb. Res. 2009, 124, 281–287. [Google Scholar] [CrossRef]
- Geerts, W.H.; Code, K.I.; Jay, R.M.; Chen, E.; Szalai, J.P. A prospective study of venous thromboembolism after major trauma. N. Engl. J. Med. 1994, 331, 1601–1606. [Google Scholar] [CrossRef]
- Scolaro, J.A.; Taylor, R.M.; Wigner, N.A. Venous thromboembolism in orthopaedic trauma. J. Am. Acad. Orthop. Surg. 2015, 23, 1–6. [Google Scholar] [CrossRef]
- Toker, S.; Hak, D.J.; Morgan, S.J. Deep vein thrombosis prophylaxis in trauma patients. Thrombosis 2011, 2011, 505373. [Google Scholar] [CrossRef]
- Tai, S.M.; Buddhdev, P.; Baskaradas, A.; Sivarasan, N.; Tai, N.R. Venous thromboembolism in the trauma patient. Orthop. Trauma 2013, 27, 379–392. [Google Scholar] [CrossRef]
- Wells, P.; Anderson, D. The diagnosis and treatment of venous thromboembolism. Hematol. Am. Soc. Hematol. Educ. Program 2013, 2013, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Kelsey, L.J.; Fry, D.M.; VanderKolk, W.E. Thrombosis risk in the trauma patient: Prevention and treatment. Hematol. Oncol. Clin. N. Am. 2000, 14, 417–430. [Google Scholar] [CrossRef]
- Engelman, D.T.; Gabram, S.G.; Allen, L.; Ens, G.E.; Jacobs, L.M. Hypercoagulability following multiple trauma. World J. Surg. 1996, 20, 5–10. [Google Scholar] [CrossRef]
- Owings, J.T.; Bagley, M.; Gosselin, R.; Romac, D.; Disbrow, E. Effect of critical injury on plasma antithrombin activity: Low antithrombin levels are associated with thromboembolic complications. J. Trauma Acute Care Surg. 1996, 41, 396–406. [Google Scholar] [CrossRef]
- Theusinger, O.M.; Baulig, W.; Seifert, B.; Müller, S.M.; Mariotti, S.; Spahn, D.R. Changes in Coagulation in Standard Laboratory Tests and ROTEM in Trauma Patients Between On-Scene and Arrival in the Emergency Department. Anesth. Analg. 2015, 120, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.D.; Daniels, A.H.; Evangelista, P.T.; Reinert, S.E.; Ritterman, S.; Christino, M.A.; Thakur, N.A.; Born, C.T. Predicting pulmonary embolus in orthopedic trauma patients using the wells score. Orthopedics 2013, 36, e642–e647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Testroote, M.; Stigter, W.A.H.; de Visser, D.C.; Janzing, H.M.J. Low molecular weight heparin for prevention of venous thromboembolism in patients with lower-leg immobilization. Cochrane Database Syst. Rev. 2008, 4, Cd006681. [Google Scholar]
- Van Adrichem, R.; Debeij, J.; Nelissen, R.; Schipper, I.; Rosendaal, F.; Cannegieter, S. Below-knee cast immobilization and the risk of venous thrombosis: Results from a large population-based case–control study. J. Thromb. Haemost. 2014, 12, 1461–1469. [Google Scholar] [CrossRef]
- Yumoto, T.; Naito, H.; Yamakawa, Y.; Iida, A.; Tsukahara, K.; Nakao, A. Venous thromboembolism in major trauma patients: A single-center retrospective cohort study of the epidemiology and utility of D-dimer for screening. Acute Med. Surg. 2017, 4, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Brakenridge, S.C.; Henley, S.S.; Kashner, T.M.; Golden, R.M.; Paik, D.-H.; Phelan, H.A.; Cohen, M.J.; Sperry, J.L.; Moore, E.E.; Minei, J.P.; et al. Comparing clinical predictors of deep venous thrombosis vs. pulmonary embolus after severe injury: A new paradigm for post-traumatic venous thromboembolism? J. Trauma Acute Care Surg. 2013, 74, 1231–1237. [Google Scholar]
- Abdullah, W.Z. Hemostatic Biomarkers: Future Prospects and Challenges. In General Methods in Biomarker Research and Their Applications; Preedy, V.R., Patel, V.B., Eds.; Springer Netherlands: Dordrecht, The Netherlands, 2015; pp. 841–859. [Google Scholar]
- Ma, J.; Qin, J.; Hu, J.; Shang, M.; Zhou, Y.; Liang, N.; Zhang, Y.; Zhu, Y. Incidence and Hematological Biomarkers Associated With Preoperative Deep Venous Thrombosis Following Foot Fractures. Foot Ankle Int. 2020, 41, 1563–1570. [Google Scholar] [CrossRef]
- Zhang, L.D.; Liu, H.B.; Li, Y.N.; Ma, H.M.; Liu, Y.B.; Wang, M.Y. Correlation analysis between plasma D-dimer levels and orthopedic trauma severity. Chin. Med. J. 2012, 125, 3133–3136. [Google Scholar] [PubMed]
- Campbell, S. Chapter 26—Hemostasis. In Contemporary Practice in Clinical Chemistry, 4th ed.; Clarke, W., Marzinke, M.A., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 445–467. [Google Scholar]
- Levy, J.H.; Szlam, F.; Wolberg, A.S.; Winkler, A. Clinical use of the activated partial thromboplastin time and prothrombin time for screening: A review of the literature and current guidelines for testing. Clin. Lab. Med. 2014, 34, 453–477. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.H.; Tefferi, A.; Pruthi, R.K. How to Interpret and Pursue an Abnormal Prothrombin Time, Activated Partial Thromboplastin Time, and Bleeding Time in Adults. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2007; Volume 82, pp. 864–873. [Google Scholar]
- Yuan, S.; Ferrell, C.; Chandler, W.L. Comparing the prothrombin time INR versus the APTT to evaluate the coagulopathy of acute trauma. Thromb. Res. 2007, 120, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Zakai, N.A.; Ohira, T.; White, R.; Folsom, A.R.; Cushman, M. Activated Partial Thromboplastin Time and Risk of Future Venous Thromboembolism. Am. J. Med. 2008, 121, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, A.; Chantarangkul, V.; Martinelli, I.; Bucciarelli, P.; Mannucci, P.M. A shortened activated partial thromboplastin time is associated with the risk of venous thromboembolism. Blood 2004, 104, 3631–3634. [Google Scholar] [CrossRef] [Green Version]
- Cao, X.; Su, Y.; Zhang, W.; Zhao, H.; Wen, M.; Lu, S.; Zhao, Y.; Chen, Y.; Liu, L.; Zang, X.; et al. The Impact of Anticoagulant Activity of Tissue Factor Pathway Inhibitor Measured by a Novel Functional Assay for Predicting Deep Venous Thrombosis in Trauma Patients: A Prospective Nested Case-Control Study. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211063877. [Google Scholar] [CrossRef]
- Park, M.S.; Martini, W.Z.; Dubick, M.A.; Salinas, J.; Butenas, S.; Kheirabadi, B.S.; Pusateri, A.E.; Wang, J.; Vos, J.A.; Guymon, C.H.; et al. Thromboelastography as a better indicator of postinjury hypercoagulable state than prothrombin time or activated partial thromboplastin time. J. Trauma 2009, 67, 266–275. [Google Scholar]
- Favresse, J.; Lippi, G.; Roy, P.-M.; Chatelain, B.; Jacqmin, H.; ten Cate, H.; Mullier, F. D-dimer: Preanalytical, analytical, postanalytical variables, and clinical applications. Crit. Rev. Clin. Lab. Sci. 2018, 55, 548–577. [Google Scholar] [CrossRef]
- Vanfleteren, L.; Wesseling, G. Evaluation of the diagnostic yield of D-dimer testing in suspected venous thromboembolism in primary care: A 2-year retrospective analysis. Prim. Care Respir. J. 2011, 20, 102–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Huai, Y.; Wang, W.; Xue, K.; Chen, L.; Chen, C.; Qian, A. A Retrospective cohort study on the risk factors of deep vein thrombosis (DVT) for patients with traumatic fracture at Honghui Hospital. BMJ Open 2019, 9, e024247. [Google Scholar] [CrossRef]
- Cheng, J.; Fu, Z.; Zhu, J.; Zhou, L.; Song, W. The predictive value of plasminogen activator inhibitor-1, fibrinogen, and D-dimer for deep venous thrombosis following surgery for traumatic lower limb fracture. Ann. Palliat. Med. 2020, 9, 3385–3392. [Google Scholar] [CrossRef] [PubMed]
- Zamir, M.; Najjad, M.K.R.; Yousuf, N.; Noor, S.S.; Intikhab, O.; Mughal, I.S.; Sufyan, M. Can D-dimers detect the deep venous thromboembolism after total knee arthroplasty? Pak. J. Surg. 2015, 31, 124–127. [Google Scholar]
- Geersing, G.J.; Zuithoff, N.P.; Kearon, C.; Anderson, D.R.; Ten Cate-Hoek, A.J.; Elf, J.L.; Bates, S.M.; Hoes, A.W.; Kraaijenhagen, R.A.; Oudega, R.; et al. Exclusion of deep vein thrombosis using the Wells rule in clinically important subgroups: Individual patient data meta-analysis. BMJ 2014, 348, g1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Forgie, M.; Kearon, C.; Dreyer, J.; Kovacs, G.; Mitchell, M.; Lewandowski, B.; Kovacs, M.J. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N. Engl. J. Med. 2003, 349, 1227–1235. [Google Scholar] [CrossRef] [Green Version]
- Kamath, S.; Lip, G.Y.H. Fibrinogen: Biochemistry, epidemiology and determinants. QJM 2003, 96, 711–729. [Google Scholar] [CrossRef] [Green Version]
- Machlus, K.R.; Cardenas, J.C.; Church, F.C.; Wolberg, A.S. Causal relationship between hyperfibrinogenemia, thrombosis, and resistance to thrombolysis in mice. Blood 2011, 117, 4953–4963. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Topete, D.; Iwaki, T.; Ploplis, V.; Castellino, F. Delayed inflammatory responses to endotoxin in fibrinogen-deficient mice. J. Pathol. 2006, 210, 325–333. [Google Scholar] [CrossRef]
- Lin, C.; Chen, Y.; Chen, B.; Zheng, K.; Luo, X.; Lin, F. D-Dimer Combined with Fibrinogen Predicts the Risk of Venous Thrombosis in Fracture Patients. Emerg. Med. Int. 2020, 2020, 1930405. [Google Scholar] [CrossRef]
- Hou, H.; Ge, Z.; Ying, P.; Dai, J.; Shi, D.; Xu, Z.; Chen, D.; Jiang, Q. Biomarkers of deep venous thrombosis. J. Thromb. Thrombolysis 2012, 34, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, I.; Ay, C. Biomarkers and venous thromboembolism. Arter. Thromb. Vasc. Biol. 2009, 29, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Binder, N.B.; Depasse, F.; Mueller, J.; Wissel, T.; Schwers, S.; Germer, M.; Hermes, B.; Turecek, P.L. Clinical use of thrombin generation assays. J. Thromb. Haemost. 2021, 19, 2918–2929. [Google Scholar] [CrossRef] [PubMed]
- van Veen, J.J.; Gatt, A.; Makris, M. Thrombin generation testing in routine clinical practice: Are we there yet? Br. J. Haematol. 2008, 142, 889–903. [Google Scholar] [CrossRef]
- Brummel-Ziedins, K.E.; Vossen, C.Y.; Butenas, S.; Mann, K.G.; Rosendaal, F.R. Thrombin generation profiles in deep venous thrombosis. J. Thromb. Haemost. 2005, 3, 2497–2505. [Google Scholar] [CrossRef] [Green Version]
- Tappenden, K.A.; Gallimore, M.J.; Evans, G.; Mackie, I.J.; Jones, D.W. Thrombin generation: A comparison of assays using platelet-poor and -rich plasma and whole blood samples from healthy controls and patients with a history of venous thromboembolism. Br. J. Haematol. 2007, 139, 106–112. [Google Scholar] [CrossRef]
- Van Hylckama Vlieg, A.; Christiansen, S.C.; Luddington, R.; Cannegieter, S.C.; Rosendaal, F.R.; Baglin, T.P. Elevated endogenous thrombin potential is associated with an increased risk of a first deep venous thrombosis but not with the risk of recurrence. Br. J. Haematol. 2007, 138, 769–774. [Google Scholar] [CrossRef]
- Park, M.S.; Spears, G.M.; Bailey, K.R.; Xue, A.; Ferrara, M.J.; Headlee, A.; Dhillon, S.K.; Jenkins, D.H.; Zietlow, S.P.; Harmsen, W.S.; et al. Thrombin generation profiles as predictors of symptomatic venous thromboembolism after trauma: A prospective cohort study. J. Trauma Acute Care Surg. 2017, 83, 381–387. [Google Scholar] [CrossRef]
- Ferrara, M.J.; MacArthur, T.A.; Butenas, S.; Mann, K.G.; Immermann, J.M.; Spears, G.M.; Bailey, K.R.; Kozar, R.A.; Heller, S.F.; Loomis, E.A.; et al. Exploring the utility of a novel point-of-care whole blood thrombin generation assay following trauma: A pilot study. Res. Pract. Thromb. Haemost. 2021, 5, 395–402. [Google Scholar] [CrossRef]
- Walenga, J.M.; Kaiser, P.C.; Prechel, M.M.; Hoppensteadt, D.; Jeske, W.P.; Misselwitz, F.; Bacher, P.; Lassen, M.R.; Fareed, J. Sustained Release of Tissue Factor Following Thrombosis of Lower Limb Trauma. Clin. Appl. Thromb. Hemost. 2014, 20, 678–686. [Google Scholar] [CrossRef] [Green Version]
- Lovren, F.; Verma, S. Evolving role of microparticles in the pathophysiology of endothelial dysfunction. Clin. Chem. 2013, 59, 1166–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.S.; Owen, B.A.; Ballinger, B.A.; Sarr, M.G.; Schiller, H.J.; Zietlow, S.P.; Jenkins, D.H.; Ereth, M.H.; Owen, W.G.; Heit, J.A. Quantification of hypercoagulable state after blunt trauma: Microparticle and thrombin generation are increased relative to injury severity, while standard markers are not. Surgery 2012, 151, 831–836. [Google Scholar] [CrossRef] [Green Version]
- Hoffbrand, A.V.; Higgs, D.R.; Keeling, D.M.; Mehta, A.B. Postgraduate Haematology, 7th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Comp, P.; Doray, D.; Patton, D.; Esmon, C. An abnormal plasma distribution of protein S occurs in functional protein S deficiency. Blood 1986, 67, 504–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Meijden, P.E.J.; Heemskerk, J.W.M. Platelet biology and functions: New concepts and clinical perspectives. Nat. Rev. Cardiol. 2019, 16, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Schafer, A.I. Thrombocytosis. N. Engl. J. Med. 2004, 350, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Valade, N.; Decailliot, F.; Rébufat, Y.; Heurtematte, Y.; Duvaldestin, P.; Stéphan, F. Thrombocytosis after trauma: Incidence, aetiology, and clinical significance. Br. J. Anaesth. 2005, 94, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Kaser, A.; Brandacher, G.; Steurer, W.; Kaser, S.; Offner, F.A.; Zoller, H.; Theurl, I.; Widder, W.; Molnar, C.; Ludwiczek, O.; et al. Interleukin-6 stimulates thrombopoiesis through thrombopoietin: Role in inflammatory thrombocytosis. Blood 2001, 98, 2720–2725. [Google Scholar] [CrossRef] [Green Version]
- Kaushansky, K.; Lok, S.; Holly, R.D.; Broudy, V.C.; Lin, N.; Bailey, M.C.; Forstrom, J.W.; Buddle, M.M.; Oort, P.J.; Hagen, F.S.; et al. Promotion of megakaryocyte progenitor expansion and differentiation by the c-Mpl ligand thrombopoietin. Nature 1994, 369, 568–571. [Google Scholar] [CrossRef]
- Zhang, L.; He, M.; Jia, W.; Xie, W.; Song, Y.; Wang, H.; Peng, J.; Li, Y.; Wang, Z.; Lin, Z. Analysis of high-risk factors for preoperative DVT in elderly patients with simple hip fractures and construction of a nomogram prediction model. BMC Musculoskelet. Disord. 2022, 23, 441. [Google Scholar] [CrossRef]
- Bajaj, M.S.; Kuppuswamy, M.N.; Saito, H.; Spitzer, S.G.; Bajaj, S.P. Cultured normal human hepatocytes do not synthesize lipoprotein-associated coagulation inhibitor: Evidence that endothelium is the principal site of its synthesis. Proc. Natl. Acad. Sci. USA 1990, 87, 8869–8873. [Google Scholar] [CrossRef] [Green Version]
- Hackeng, T.M.; Maurissen, L.F.; Castoldi, E.; Rosing, J. Regulation of TFPI function by protein S. J. Thromb. Haemost. 2009, 7 (Suppl. S1), 165–168. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Kanse, S.M.; Kothari, H.; Reinhardt, C.; Fletcher, C. Post-transcriptional, post-translational and pharmacological regulation of tissue factor pathway inhibitor. Blood Coagul. Fibrinolysis 2018, 29, 668–682. [Google Scholar] [CrossRef] [PubMed]
- Broze, G.J., Jr.; Warren, L.A.; Novotny, W.F.; Higuchi, D.A.; Girard, J.J.; Miletich, J.P. The lipoprotein-associated coagulation inhibitor that inhibits the factor VII-tissue factor complex also inhibits factor Xa: Insight into its possible mechanism of action. Blood 1988, 71, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girard, T.J.; Warren, L.A.; Novotny, W.F.; Likert, K.M.; Brown, S.G.; Miletich, J.P.; Broze, G.J., Jr. Functional significance of the Kunitz-type inhibitory domains of lipoprotein-associated coagulation inhibitor. Nature 1989, 338, 518–520. [Google Scholar] [CrossRef]
- Sidelmann, J.J.; Bladbjerg, E.M.; Gram, J.; Münster, A.M.; Jespersen, J. Tissue factor pathway inhibitor relates to fibrin degradation in patients with acute deep venous thrombosis. Blood Coagul. Fibrinolysis 2008, 19, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Greven, J.; Pfeifer, R.; Zhi, Q.; Pape, H.C. Update on the role of endothelial cells in trauma. Eur. J. Trauma Emerg. Surg. 2018, 44, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Dahm, A.; Van Hylckama Vlieg, A.; Bendz, B.; Rosendaal, F.; Bertina, R.M.; Sandset, P.M. Low levels of tissue factor pathway inhibitor (TFPI) increase the risk of venous thrombosis. Blood 2003, 101, 4387–4392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, T.M.; Kim, D.H. C-reactive protein and erythrocyte sedimentation rate in orthopaedics. Univ. Pa. Orthop. J. 2002, 15, 13–16. [Google Scholar]
- Reiter, M.; Bucek, R.A.; Koca, N.; Dirisamer, A.; Minar, E. Deep vein thrombosis and systemic inflammatory response: A pilot trial. Wien. Klin. Wochenschr. 2003, 115, 111–114. [Google Scholar] [CrossRef]
- Ng, T. Erythrocyte sedimentation rate, plasma viscosity and C-reactive protein in clinical practice. Br. J. Hosp. Med. 1997, 58, 521–523. [Google Scholar]
- Xiong, X.; Cheng, B. Preoperative risk factors for deep vein thrombosis in knee osteoarthritis patients undergoing total knee arthroplasty. J. Orthop. Sci. 2021, in press. [CrossRef] [PubMed]
- Schaefer, J.K.; Jacobs, B.; Wakefield, T.W.; Sood, S.L. New biomarkers and imaging approaches for the diagnosis of deep venous thrombosis. Curr. Opin. Hematol. 2017, 24, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.; Abt, M.; Ciorciaro, C.; Kling, D.; Jamois, C.; Schick, E.; Solier, C.; Benghozi, R.; Gaudreault, J. First-in-Man Study With Inclacumab, a Human Monoclonal Antibody Against P-selectin. J. Cardiovasc. Pharm. 2015, 65, 611–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blann, A.D.; Faragher, E.B.; McCollum, C.N. Increased soluble P-selectin following myocardial infarction: A new marker for the progression of atherosclerosis. Blood Coagul. Fibrinolysis 1997, 8, 383–390. [Google Scholar] [CrossRef]
- Tang, N.; Yin, S.; Sun, Z.; Pan, Y. Time course of soluble P-selectin and von Willebrand factor levels in trauma patients: A prospective observational study. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 70. [Google Scholar] [CrossRef] [Green Version]
- Antonopoulos, C.N.; Sfyroeras, G.S.; Kakisis, J.D.; Moulakakis, K.G.; Liapis, C.D. The role of soluble P selectin in the diagnosis of venous thromboembolism. Thromb. Res. 2014, 133, 17–24. [Google Scholar] [CrossRef]
- Blann, A.D.; Noteboom, W.M.; Rosendaal, F.R. Increased soluble P-selectin levels following deep venous thrombosis: Cause or effect? Br. J. Haematol. 2000, 108, 191–193. [Google Scholar] [CrossRef] [Green Version]
- Rectenwald, J.E.; Myers, D.D., Jr.; Hawley, A.E.; Longo, C.; Henke, P.K.; Guire, K.E.; Schmaier, A.H.; Wakefield, T.W. D-dimer, P-selectin, and microparticles: Novel markers to predict deep venous thrombosis. A pilot study. Thromb. Haemost. 2005, 94, 1312–1317. [Google Scholar] [CrossRef]
- Ramacciotti, E.; Blackburn, S.; Hawley, A.E.; Vandy, F.; Ballard-Lipka, N.; Stabler, C.; Baker, N.; Guire, K.E.; Rectenwald, J.E.; Henke, P.K.; et al. Evaluation of Soluble P-Selectin as a Marker for the Diagnosis of Deep Venous Thrombosis. Clin. Appl. Thromb. Hemost. 2011, 17, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Vandy, F.C.; Stabler, C.; Eliassen, A.M.; Hawley, A.E.; Guire, K.E.; Myers, D.D.; Henke, P.K.; Wakefield, T.W. Soluble P-selectin for the diagnosis of lower extremity deep venous thrombosis. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, N.K.; Barmparas, G.; Lin, T.L.; Linaval, N.T.; Yang, A.R.; Sekhon, H.K.; Mason, R.; Margulies, D.R.; Gewertz, B.L.; Ley, E.J. A Systems-based Approach to Reduce Deep Venous Thrombosis and Pulmonary Embolism in Trauma Patients. World J. Surg. 2021, 45, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Hoang, P.; Wallace, A.; Sugi, M.; Fleck, A.; Pershad, Y.; Dahiya, N.; Albadawi, H.; Knuttinen, G.; Naidu, S.; Oklu, R. Elastography techniques in the evaluation of deep vein thrombosis. Cardiovasc. Diagn. Ther. 2017, 7 (Suppl. S3), S238. [Google Scholar] [CrossRef] [PubMed]
- Yusof, N.N.M.; McCann, A.; Little, P.J.; Ta, H.T. Non-invasive imaging techniques for the differentiation of acute and chronic thrombosis. Thromb. Res. 2019, 177, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Ginsberg, J.S.; Hirsh, J. The role of venous ultrasonography in the diagnosis of suspected deep venous thrombosis and pulmonary embolism. Ann. Intern. Med. 1998, 129, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, M.; Braun, C.; Patel, P.; Patel, P.; Begum, H.; Wiercioch, W.; Varghese, J.; Wooldridge, D.; Alturkmani, H.J.; Thomas, M.; et al. Diagnosis of deep vein thrombosis of the lower extremity: A systematic review and meta-analysis of test accuracy. Blood Adv. 2020, 4, 1250–1264. [Google Scholar] [CrossRef] [PubMed]
- Da Costa Rodrigues, J.; Alzuphar, S.; Combescure, C.; Le Gal, G.; Perrier, A. Diagnostic characteristics of lower limb venous compression ultrasonography in suspected pulmonary embolism: A meta-analysis. J. Thromb. Haemost. 2016, 14, 1765–1772. [Google Scholar] [CrossRef]
- Kay, A.B.; Morris, D.S.; Woller, S.C.; Stevens, S.M.; Bledsoe, J.R.; Lloyd, J.F.; Collingridge, D.S.; Majercik, S. Trauma patients at risk for venous thromboembolism who undergo routine duplex ultrasound screening experience fewer pulmonary emboli: A prospective randomized trial. J. Trauma Acute Care Surg. 2021, 90, 787–796. [Google Scholar] [CrossRef]
- Baker, J.E.; Niziolek, G.M.; Elson, N.C.; Pugh, A.M.; Nomellini, V.; Makley, A.T.; Pritts, T.A.; Goodman, M.D. Optimizing Lower Extremity Duplex Ultrasound Screening After Traumatic Injury. J. Surg. Res. 2019, 243, 143–150. [Google Scholar] [CrossRef]
- Maufus, M.; Elias, A.; Barrellier, M.-T.; Pernod, G. Diagnosis of deep vein thrombosis recurrence: Ultrasound criteria. Thromb. Res. 2018, 161, 78–83. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Biomarkers | Results | References |
|---|---|---|
| PT | PT cutoff value more reliable in detecting coagulation factor deficiency with a sensitivity of 84% | [28] |
| The PT optimal cut-off value for diagnosing DVT in trauma patients was 12.05 s with a sensitivity of 72.92% and specificity of 47.92% (AUC 0.617, 95% CI 0.505–0.730, p = 0.048) | [31] | |
| aPTT | Lower aPTT was associated with a two-fold increased risk of VTE | [29] |
| D-dimer | The D-dimer optimal cut-off value was 3.825 mg/L with a sensitivity of 85.42% and specificity of 51.11% (AUC 0.624, 95% CI 0.505–0.744, p = 0.039) for diagnosing DVT in trauma patients | [31] |
| D-dimer cut-off value of 4.01 mg/L for DVT in traumatic fracture patients, with AUC of 0.593, 71.2% sensitivity, and 44.8% specificity | [35] | |
| Fibrinogen | Fibrinogen cut-off value of 3.543 g/L for the diagnosis of VTE in elderly fracture patients, with a sensitivity of 26.90% and specificity of 77.70% (AUC 0.5209, 95% CI 0.500 to 0.542) | [43] |
| Thrombin generation | First time to peak (ttpeak) value appears to be an independent predictor of VTE with a HR of 2.26, 95% CI [1.61, 3.18] per 1 (minute) decrease, p < 0.0001 | [51] |
| Platelet count | Platelet count was one of the independent risk factors for DVT (p < 0.05), with a cutoff value of 200.5 × 109/L, sensitivity of 38.9% and specificity of 85.9% (AUC = 0.642 (95% CI: 0.569~0.714)) | [63] |
| TFPI | The optimal cut-off value for the TFPI initial anticoagulant time ratio for diagnosing DVT in trauma patients was 33.53%, with a sensitivity of 71.11% and specificity of 55.32% (AUC 0.646, 95% CI 0.533–0.759) | [31] |
| CRP | CRP was found to be higher in DVT patients (2.5 mg/dL ± 3.2) compared with controls (1.0 mg/dL ± 2.5) | [73] |
| ESR | An increase in ESR values was associated with the development of DVT before TKA | [75] |
| Soluble P-selectin | Increased levels of soluble P-selectin in DVT patients | [81,82] |
| The pooled sensitivity of sPsel was 0.57 (95% CI = 0.30–0.82), while the pooled specificity was 0.73 (95% CI = 0.51–0.90). | [80] | |
| sPsel levels > 90 ng/mL with a Wells scores ≥ 2 was found to be effective in diagnosing DVT, whereas sPsel levels < 60 ng/mL with Wells scores < 2 was able to effectively ‘rule-out’ DVT | [83] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramli, N.N.; Iberahim, S.; Mohd Noor, N.H.; Zulkafli, Z.; Tengku Md Shihabuddin, T.M.; Din, M.H.; Mohamed Saat, M.A.; Samsudin, A.H.Z. Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers for VTE in Trauma-Immobilized Patients. Diagnostics 2023, 13, 150. https://doi.org/10.3390/diagnostics13010150
Ramli NN, Iberahim S, Mohd Noor NH, Zulkafli Z, Tengku Md Shihabuddin TM, Din MH, Mohamed Saat MA, Samsudin AHZ. Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers for VTE in Trauma-Immobilized Patients. Diagnostics. 2023; 13(1):150. https://doi.org/10.3390/diagnostics13010150
Chicago/Turabian StyleRamli, Noor Nabila, Salfarina Iberahim, Noor Haslina Mohd Noor, Zefarina Zulkafli, Tengku Muzaffar Tengku Md Shihabuddin, Mohd Hadizie Din, Muhamad Aizat Mohamed Saat, and Ahmad Hadif Zaidin Samsudin. 2023. "Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers for VTE in Trauma-Immobilized Patients" Diagnostics 13, no. 1: 150. https://doi.org/10.3390/diagnostics13010150
APA StyleRamli, N. N., Iberahim, S., Mohd Noor, N. H., Zulkafli, Z., Tengku Md Shihabuddin, T. M., Din, M. H., Mohamed Saat, M. A., & Samsudin, A. H. Z. (2023). Haemostasis and Inflammatory Parameters as Potential Diagnostic Biomarkers for VTE in Trauma-Immobilized Patients. Diagnostics, 13(1), 150. https://doi.org/10.3390/diagnostics13010150