
Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022?

Abstract
:1. Introduction
2. Mass Versus Targeted Screening
2.1. Type 2 Diabetes Mellitus
2.2. Factors Related to Metabolic Conditions
2.3. Alcohol Use Disorders
2.4. Elevated Liver Enzymes
3. What Do the Guidelines Say about Screening for Advanced Liver Fibrosis?
4. Tools for Screening
5. Simple Blood Tests
5.1. FIB-4
5.2. NFS
6. Specialized Test
6.1. Elastography-Based Techniques
6.2. Specialized Blood Test
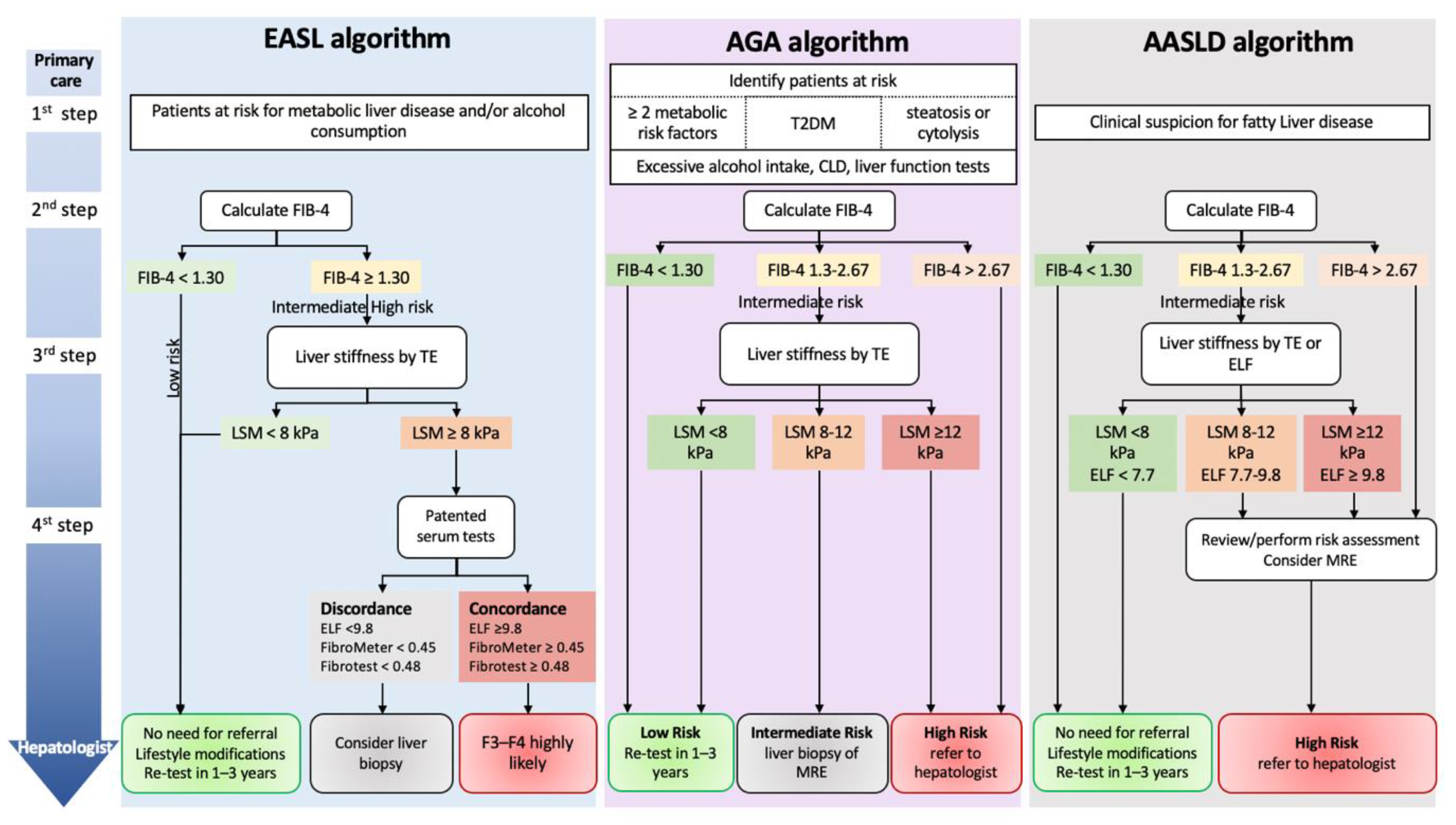
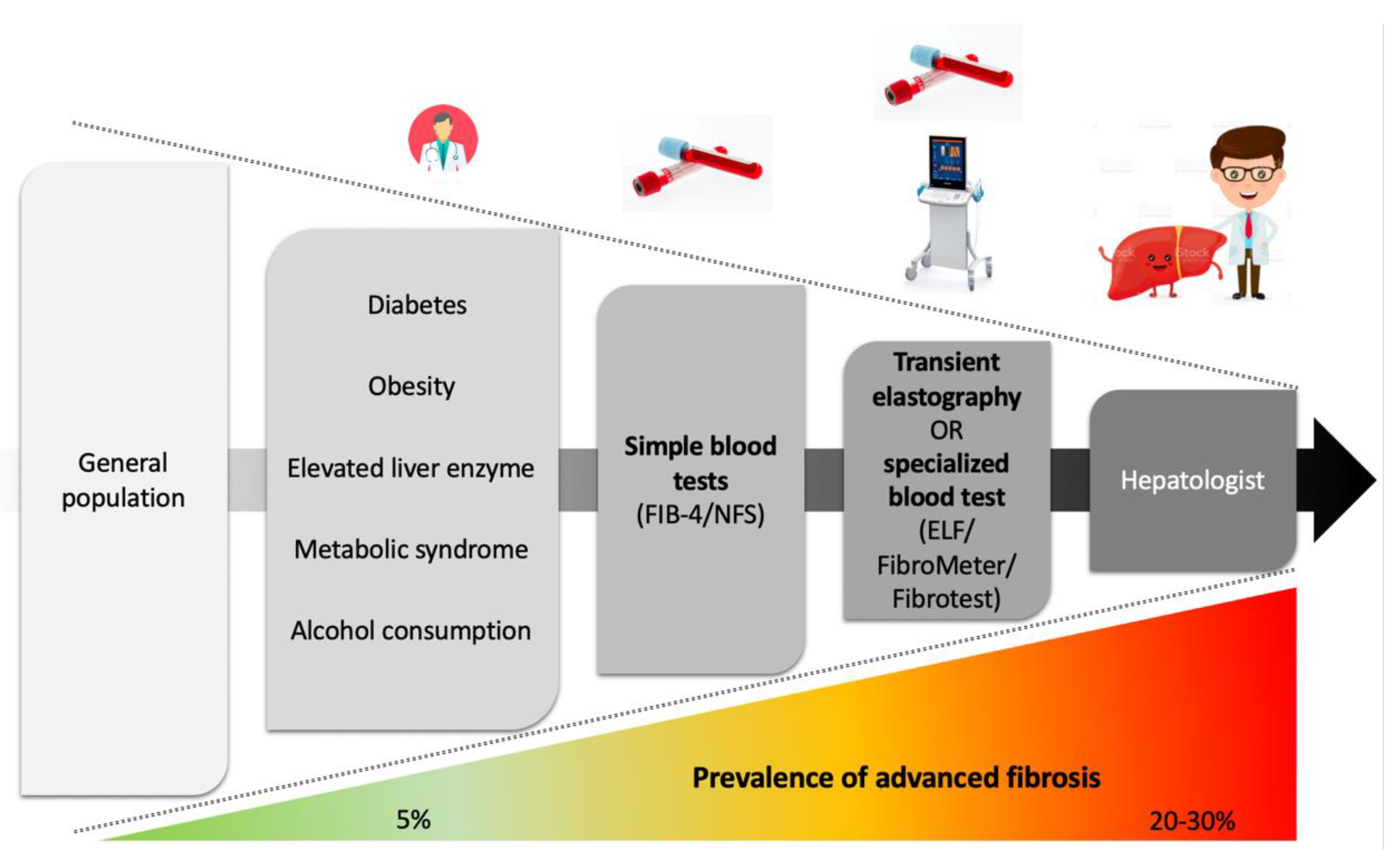
7. Referral Pathways with Algorithms
8. Algorithms in Primary Care
9. What Do the Guidelines Say about Referral Pathways Based on Noninvasive Tests?
10. Awareness of Chronic Liver Diseases
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Cirrhosis Collaborators The Global, Regional, and National Burden of Cirrhosis by Cause in 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol 2020, 5, 245–266. [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Hepatology. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 2650–2666. [Google Scholar] [CrossRef] [PubMed]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of Liver Diseases in the World. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagström, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wai-Sun Wong, V.; Peleg, N.; et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625.e12. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.J.; Van Natta, M.L.; Clark, J.; Neuschwander-Tetri, B.A.; Diehl, A.; Dasarathy, S.; Loomba, R.; Chalasani, N.; Kowdley, K.; Hameed, B.; et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2021, 385, 1559–1569. [Google Scholar] [CrossRef]
- Lackner, C.; Stauber, R.E.; Davies, S.; Denk, H.; Dienes, H.P.; Gnemmi, V.; Guido, M.; Miquel, R.; Paradis, V.; Schirmacher, P.; et al. Development and Prognostic Relevance of a Histologic Grading and Staging System for Alcohol-Related Liver Disease. J. Hepatol. 2021, 75, 810–819. [Google Scholar] [CrossRef]
- Fialla, A.D.; de Muckadell, O.B.S.; Touborg Lassen, A. Incidence, Etiology and Mortality of Cirrhosis: A Population-Based Cohort Study. Scand. J. Gastroenterol. 2012, 47, 702–709. [Google Scholar] [CrossRef]
- Goutté, N.; Sogni, P.; Bendersky, N.; Barbare, J.C.; Falissard, B.; Farges, O. Geographical Variations in Incidence, Management and Survival of Hepatocellular Carcinoma in a Western Country. J. Hepatol. 2017, 66, 537–544. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis—2021 Update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Roulot, D.; Costes, J.-L.; Buyck, J.-F.; Warzocha, U.; Gambier, N.; Czernichow, S.; Le Clesiau, H.; Beaugrand, M. Transient Elastography as a Screening Tool for Liver Fibrosis and Cirrhosis in a Community-Based Population Aged over 45 Years. Gut 2011, 60, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Fabrellas, N.; Alemany, M.; Urquizu, M.; Bartres, C.; Pera, G.; Juvé, E.; Rodríguez, L.; Torán, P.; Caballería, L. Using Transient Elastography to Detect Chronic Liver Diseases in a Primary Care Nurse Consultancy. Nurs. Res. 2013, 62, 450–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballería, L.; Pera, G.; Arteaga, I.; Rodríguez, L.; Alumà, A.; Morillas, R.M.; de la Ossa, N.; Díaz, A.; Expósito, C.; Miranda, D.; et al. High Prevalence of Liver Fibrosis Among European Adults With Unknown Liver Disease: A Population-Based Study. Clin. Gastroenterol. Hepatol. 2018, 16, 1138–1145.e5. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Plompen, E.P.C.; Schouten, J.N.L.; Hansen, B.E.; Murad, S.D.; Taimr, P.; Leebeek, F.W.G.; Hofman, A.; Stricker, B.H.; Castera, L.; et al. Presence of Diabetes Mellitus and Steatosis Is Associated with Liver Stiffness in a General Population: The Rotterdam Study. Hepatology 2016, 63, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Llop, E.; Iruzubieta, P.; Perelló, C.; Fernández Carrillo, C.; Cabezas, J.; Escudero, M.D.; González, M.; Hernández Conde, M.; Puchades, L.; Arias-Loste, M.T.; et al. High Liver Stiffness Values by Transient Elastography Related to Metabolic Syndrome and Harmful Alcohol Use in a Large Spanish Cohort. United Eur. Gastroenterol. J. 2021, 9, 892–902. [Google Scholar] [CrossRef]
- You, S.C.; Kim, K.J.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, W.J.; Han, K.-H. Factors Associated with Significant Liver Fibrosis Assessed Using Transient Elastography in General Population. World J. Gastroenterol. 2015, 21, 1158–1166. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Hiriart, J.B.; Lupsor-Platon, M.; Bronte, F.; Boursier, J.; Elshaarawy, O.; Marra, F.; Thiele, M.; Markakis, G.; Payance, A.; et al. Refining the Baveno VI Elastography Criteria for the Definition of Compensated Advanced Chronic Liver Disease. J. Hepatol. 2021, 74, 1109–1116. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Chu, W.C.-W.; Wong, G.L.-H.; Chan, R.S.-M.; Chim, A.M.-L.; Ong, A.; Yeung, D.K.-W.; Yiu, K.K.-L.; Chu, S.H.-T.; Woo, J.; et al. Prevalence of Non-Alcoholic Fatty Liver Disease and Advanced Fibrosis in Hong Kong Chinese: A Population Study Using Proton-Magnetic Resonance Spectroscopy and Transient Elastography. Gut 2012, 61, 409–415. [Google Scholar] [CrossRef]
- Nah, E.-H.; Cho, S.; Kim, S.; Chu, J.; Kwon, E.; Cho, H.-I. Prevalence of Liver Fibrosis and Associated Risk Factors in the Korean General Population: A Retrospective Cross-Sectional Study. BMJ Open 2021, 11, e046529. [Google Scholar] [CrossRef]
- Roulot, D.; Roudot-Thoraval, F.; NKontchou, G.; Kouacou, N.; Costes, J.-L.; Elourimi, G.; Le Clesiau, H.; Ziol, M.; Beaugrand, M. Concomitant Screening for Liver Fibrosis and Steatosis in French Type 2 Diabetic Patients Using Fibroscan. Liver Int. 2017, 37, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Turino, T.; Lando, M.G.; Gjini, K.; Byrne, C.D.; Zusi, C.; Ravaioli, F.; Colecchia, A.; Maffeis, C.; Salvagno, G.; et al. Screening for Non-Alcoholic Fatty Liver Disease Using Liver Stiffness Measurement and Its Association with Chronic Kidney Disease and Cardiovascular Complications in Patients with Type 2 Diabetes. Diabetes Metab. 2020, 46, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Monti, T.; Perseghin, G. High Prevalence of Advanced Liver Fibrosis Assessed by Transient Elastography Among U.S. Adults With Type 2 Diabetes. Diabetes Care 2021, 44, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Lai, L.-L.; Wan Yusoff, W.N.I.; Vethakkan, S.R.; Nik Mustapha, N.R.; Mahadeva, S.; Chan, W.-K. Screening for Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus Using Transient Elastography. J. Gastroenterol. Hepatol. 2019, 34, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Kwok, R.; Choi, K.C.; Wong, G.L.-H.; Zhang, Y.; Chan, H.L.-Y.; Luk, A.O.-Y.; Shu, S.S.-T.; Chan, A.W.-H.; Yeung, M.-W.; Chan, J.C.-N.; et al. Screening Diabetic Patients for Non-Alcoholic Fatty Liver Disease with Controlled Attenuation Parameter and Liver Stiffness Measurements: A Prospective Cohort Study. Gut 2016, 65, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- Sporea, I.; Mare, R.; Popescu, A.; Nistorescu, S.; Baldea, V.; Sirli, R.; Braha, A.; Sima, A.; Timar, R.; Lupusoru, R. Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience. J. Clin. Med. 2020, 9, 1032. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Anoop, S.; Ansari, I.A.; Prakash, S.; Misra, A. High Prevalence of Hepatic Steatosis and Hepatic Fibrosis in Patients with Type 2 Diabetes Mellitus. Clin. Nutr. ESPEN 2021, 46, 519–526. [Google Scholar] [CrossRef]
- de Lédinghen, V.; Vergniol, J.; Gonzalez, C.; Foucher, J.; Maury, E.; Chemineau, L.; Villars, S.; Gin, H.; Rigalleau, V. Screening for Liver Fibrosis by Using FibroScan® and FibroTest in Patients with Diabetes. Dig. Liver Dis. 2012, 44, 413–418. [Google Scholar] [CrossRef]
- Alexopoulos, A.-S.; Crowley, M.J.; Wang, Y.; Moylan, C.A.; Guy, C.D.; Henao, R.; Piercy, D.L.; Seymour, K.A.; Sudan, R.; Portenier, D.D.; et al. Glycemic Control Predicts Severity of Hepatocyte Ballooning and Hepatic Fibrosis in Nonalcoholic Fatty Liver Disease. Hepatology 2021, 74, 1220–1233. [Google Scholar] [CrossRef]
- Diabetes Mellitus, Fasting Glucose, and Risk of Cause-Specific Death. N. Engl. J. Med. 2011, 364, 829–841. [CrossRef]
- EASL–EASD–EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [CrossRef] [PubMed]
- American Diabetes Association. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S37–S47. [Google Scholar]
- Zhang, X.; Heredia, N.I.; Balakrishnan, M.; Thrift, A.P. Prevalence and Factors Associated with NAFLD Detected by Vibration Controlled Transient Elastography among US Adults: Results from NHANES 2017–2018. PLoS ONE 2021, 16, e0252164. [Google Scholar] [CrossRef] [PubMed]
- Long, M.T.; Zhang, X.; Xu, H.; Liu, C.-T.; Corey, K.E.; Chung, R.T.; Loomba, R.; Benjamin, E.J. Hepatic Fibrosis Associates With Multiple Cardiometabolic Disease Risk Factors: The Framingham Heart Study. Hepatology 2021, 73, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Milic, S.; Orlic, L.; Stimac, D.; Franjic, N.; Targher, G. Factors Associated with Significant Liver Steatosis and Fibrosis as Assessed by Transient Elastography in Patients with One or More Components of the Metabolic Syndrome. J. Diabetes Its Complicat. 2016, 30, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Card, T.R.; Delahooke, T.; Aithal, G.P.; Guha, I.N. Obesity Is the Most Common Risk Factor for Chronic Liver Disease: Results From a Risk Stratification Pathway Using Transient Elastography. Am. J. Gastroenterol. 2019, 114, 1744–1752. [Google Scholar] [CrossRef]
- Petta, S.; Di Marco, V.; Pipitone, R.M.; Grimaudo, S.; Buscemi, C.; Craxì, A.; Buscemi, S. Prevalence and Severity of Nonalcoholic Fatty Liver Disease by Transient Elastography: Genetic and Metabolic Risk Factors in a General Population. Liver Int. 2018, 38, 2060–2068. [Google Scholar] [CrossRef]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD Disease Burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the Period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef]
- Hagström, H.; Thiele, M.; Roelstraete, B.; Söderling, J.; Ludvigsson, J.F. Mortality in Biopsy-Proven Alcohol-Related Liver Disease: A Population-Based Nationwide Cohort Study of 3453 Patients. Gut 2021, 70, 170–179. [Google Scholar] [CrossRef]
- Rhodes, F.A.; Cococcia, S.; Patel, P.; Panovska-Griffiths, J.; Tanwar, S.; Westbrook, R.H.; Rodger, A.; Rosenberg, W. Is There Scope to Improve the Selection of Patients with Alcohol-Related Liver Disease for Referral to Secondary Care? A Retrospective Analysis of Primary Care Referrals to a UK Liver Centre, Incorporating Simple Blood Tests. BMJ Open 2021, 11, e047786. [Google Scholar] [CrossRef]
- Lyu, H.; Tang, H.; Liang, Y.; Huang, S.; Wang, Y.; Huang, W.; Zhou, Y. Alcohol Consumption and Risk of Liver Fibrosis in People Living With HIV: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 841314. [Google Scholar] [CrossRef] [PubMed]
- Glyn-Owen, K.; Böhning, D.; Parkes, J.; Roderick, P.; Buchanan, R. The Combined Effect of Alcohol and Body Mass Index on Risk of Chronic Liver Disease: A Systematic Review and Meta-Analysis of Cohort Studies. Liver Int. 2021, 41, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Decraecker, M.; Dutartre, D.; Hiriart, J.-B.; Irles-Depé, M.; Marraud des Grottes, H.; Chermak, F.; Foucher, J.; Delamarre, A.; de Ledinghen, V. Long-Term Prognosis of Patients with Alcohol-Related Liver Disease or Non-Alcoholic Fatty Liver Disease According to Metabolic Syndrome or Alcohol Use. Liver Int. 2022, 42, 350–362. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases: Hepatology, Vol. XX, No. X, 2017. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanwal, F.; Shubrook, J.H.; Adams, L.A.; Pfotenhauer, K.; Wai-Sun Wong, V.; Wright, E.; Abdelmalek, M.F.; Harrison, S.A.; Loomba, R.; Mantzoros, C.S.; et al. Clinical Care Pathway for the Risk Stratification and Management of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2021, 161, 1657–1669. [Google Scholar] [CrossRef]
- Thomaides-Brears, H.B.; Alkhouri, N.; Allende, D.; Harisinghani, M.; Noureddin, M.; Reau, N.S.; French, M.; Pantoja, C.; Mouchti, S.; Cryer, D.R.H. Incidence of Complications from Percutaneous Biopsy in Chronic Liver Disease: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2022, 67, 3366–3394. [Google Scholar] [CrossRef]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver Biopsy. N. Engl. J Med. 2001, 344, 495–500. [Google Scholar] [CrossRef]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic Accuracy of FIB-4, NAFLD Fibrosis Score and APRI for NAFLD-Related Events: A Systematic Review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Löffler, J.; Verheij, J.; Brosnan, M.J.; Böcskei, Z.; Anstee, Q.M.; Bossuyt, P.M.; et al. Enhanced Liver Fibrosis Test for the Non-Invasive Diagnosis of Fibrosis in Patients with NAFLD: A Systematic Review and Meta-Analysis. J. Hepatol. 2020, 73, 252–262. [Google Scholar] [CrossRef]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Verheij, J.; Brosnan, M.J.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H.; on behalf of the LITMUS Systematic Review Team. FibroTest for Evaluating Fibrosis in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2415. [Google Scholar] [CrossRef]
- Van Dijk, A.-M.; Vali, Y.; Mak, A.L.; Lee, J.; Tushuizen, M.E.; Zafarmand, M.H.; Anstee, Q.M.; Brosnan, M.J.; Nieuwdorp, M.; Bossuyt, P.M.; et al. Systematic Review with Meta-Analyses: Diagnostic Accuracy of FibroMeter Tests in Patients with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2021, 10, 2910. [Google Scholar] [CrossRef] [PubMed]
- Boursier, J.; Vergniol, J.; Guillet, A.; Hiriart, J.-B.; Lannes, A.; Le Bail, B.; Michalak, S.; Chermak, F.; Bertrais, S.; Foucher, J.; et al. Diagnostic Accuracy and Prognostic Significance of Blood Fibrosis Tests and Liver Stiffness Measurement by FibroScan in Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 65, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, M.; Moal, V.; Delabaudiere, C.; Zuberbuhler, F.; Robic, M.-A.; Lannes, A.; Metivier, S.; Oberti, F.; Gourdy, P.; Fouchard-Hubert, I.; et al. Direct Comparison of the Specialised Blood Fibrosis Tests FibroMeterV2G and Enhanced Liver Fibrosis Score in Patients with Non-Alcoholic Fatty Liver Disease from Tertiary Care Centres. Aliment. Pharmacol. Ther. 2019, 50, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Imbert-Bismut, F.; Munteanu, M.; Messous, D.; Myers, R.P.; Thabut, D.; Ratziu, V.; Mercadier, A.; Benhamou, Y.; Hainque, B. Overview of the Diagnostic Value of Biochemical Markers of Liver Fibrosis (FibroTest, HCV FibroSure) and Necrosis (ActiTest) in Patients with Chronic Hepatitis C. Comp. Hepatol. 2004, 3, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, B.A.; Harrison, S.A.; Cotter, G.; Alkhouri, N.; Sanyal, A.; Edwards, C.; Colca, J.R.; Iwashita, J.; Koch, G.G.; Dittrich, H.C. Suboptimal Reliability of Liver Biopsy Evaluation Has Implications for Randomized Clinical Trials. J. Hepatol. 2020, 73, 1322–1332. [Google Scholar] [CrossRef]
- Poynard, T.; Munteanu, M.; Imbert-Bismut, F.; Charlotte, F.; Thabut, D.; Le Calvez, S.; Messous, D.; Thibault, V.; Benhamou, Y.; Moussalli, J.; et al. Prospective Analysis of Discordant Results between Biochemical Markers and Biopsy in Patients with Chronic Hepatitis C. Clin. Chem. 2004, 50, 1344–1355. [Google Scholar] [CrossRef] [Green Version]
- Fontanges, T.; Bailly, F.; Trepo, E.; Chevallier, M.; Maynard-Muet, M.; Nalet, B.; Beorchia, S.; Pillon, D.; Moindrot, H.; Froissart, B.; et al. Discordance between Biochemical Markers of Liver Activity and Fibrosis (Actitest®–Fibrotest®) and Liver Biopsy in Patients with Chronic Hepatitis C. Gastroentérologie Clin. Biol. 2008, 32, 858–865. [Google Scholar] [CrossRef]
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Ability of Noninvasive Scoring Systems to Identify Individuals in the Population at Risk for Severe Liver Disease. Gastroenterology 2020, 158, 200–214. [Google Scholar] [CrossRef] [Green Version]
- Unalp-Arida, A.; Ruhl, C.E. Liver Fibrosis Scores Predict Liver Disease Mortality in the United States Population. Hepatology 2017, 66, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Bugianesi, E.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Barrera, F.; Haflidadottir, S.; Day, C.P.; George, J. Simple Noninvasive Systems Predict Long-Term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2013, 145, 782–789.e4. [Google Scholar] [CrossRef] [Green Version]
- Hagström, H.; Nasr, P.; Ekstedt, M.; Stål, P.; Hultcrantz, R.; Kechagias, S. Accuracy of Noninvasive Scoring Systems in Assessing Risk of Death and Liver-Related Endpoints in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 1148–1156.e4. [Google Scholar] [CrossRef]
- Boursier, J.; Hagstrom, H.; Ekstedt, M.; Moreau, C.; Bonacci, M.; Cure, S.; Ampuero, J. Prognostic Risk Stratification Using Non-Invasive Tests with Comparison to Liver Biopsy in Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2022, 76, 1013–1020. [Google Scholar] [CrossRef]
- Braude, M.; Roberts, S.; Majeed, A.; Lubel, J.; Prompen, J.; Dev, A.; Sievert, W.; Bloom, S.; Gow, P.; Kemp, W. Liver Stiffness (Fibroscan®) Is a Predictor of All-Cause Mortality in People with Non-Alcoholic Fatty Liver Disease. Liver Int. 2022. [Google Scholar] [CrossRef]
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Repeated FIB-4 Measurements Can Help Identify Individuals at Risk of Severe Liver Disease. J. Hepatol. 2020, 73, 1023–1029. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a Simple Noninvasive Index to Predict Significant Fibrosis in Patients with HIV/HCV Coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Siddiqui, M.S.; Yamada, G.; Vuppalanchi, R.; Van Natta, M.; Loomba, R.; Guy, C.; Brandman, D.; Tonascia, J.; Chalasani, N.; Neuschwander-Tetri, B.; et al. Diagnostic Accuracy of Noninvasive Fibrosis Models to Detect Change in Fibrosis Stage. Clin. Gastroenterol. Hepatol. 2019, 17, 1877–1885.e5. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Comparison of Noninvasive Markers of Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Thiele, M.; Madsen, B.S.; Hansen, J.F.; Detlefsen, S.; Antonsen, S.; Krag, A. Accuracy of the Enhanced Liver Fibrosis Test vs FibroTest, Elastography, and Indirect Markers in Detection of Advanced Fibrosis in Patients With Alcoholic Liver Disease. Gastroenterology 2018, 154, 1369–1379. [Google Scholar] [CrossRef] [Green Version]
- Graupera, I.; Thiele, M.; Serra-Burriel, M.; Caballeria, L.; Roulot, D.; Wong, G.L.-H.; Fabrellas, N.; Guha, I.N.; Arslanow, A.; Expósito, C.; et al. Low Accuracy of FIB-4 and NAFLD Fibrosis Scores for Screening for Liver Fibrosis in the Population. Clin. Gastroenterol. Hepatol. 2022, 20, 2567–2576. [Google Scholar] [CrossRef]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic Accuracy of Non-Invasive Tests for Advanced Fibrosis in Patients with NAFLD: An Individual Patient Data Meta-Analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of Laboratory Tests, Ultrasound, or Magnetic Resonance Elastography to Detect Fibrosis in Patients with Nonalcoholic Fatty Liver Disease: A Meta-Analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hossain, F.; Horsfall, L.U.; Banh, X.; Hayward, K.L.; Williams, S.; Johnson, T.; Bernard, A.; Brown, N.N.; Lampe, G.; et al. A Pragmatic Approach Identifies a High Rate of Nonalcoholic Fatty Liver Disease With Advanced Fibrosis in Diabetes Clinics and At-Risk Populations in Primary Care. Hepatol. Commun. 2018, 2, 897–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciardullo, S.; Muraca, E.; Perra, S.; Bianconi, E.; Zerbini, F.; Oltolini, A.; Cannistraci, R.; Parmeggiani, P.; Manzoni, G.; Gastaldelli, A.; et al. Screening for Non-Alcoholic Fatty Liver Disease in Type 2 Diabetes Using Non-Invasive Scores and Association with Diabetic Complications. BMJ Open Diabetes Res. Care 2020, 8, e000904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boursier, J.; Canivet, C.M.; Costentin, C.; Lannes, A.; Delamarre, A.; Sturm, N.; Le Bail, B.; Michalak, S.; Oberti, F.; Hilleret, M.-N.; et al. Impact of Type 2 Diabetes on the Accuracy of Noninvasive Tests of Liver Fibrosis With Resulting Clinical Implications. Clin. Gastroenterol. Hepatol. 2022, S1542-3565(22)00248-8. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, E.A.; Mózes, F.E.; Jayaswal, A.N.A.; Zafarmand, M.H.; Vali, Y.; Lee, J.A.; Levick, C.K.; Young, L.A.J.; Palaniyappan, N.; Liu, C.-H.; et al. Diagnostic Accuracy of Elastography and Magnetic Resonance Imaging in Patients with NAFLD: A Systematic Review and Meta-Analysis. J. Hepatol. 2021, 75, 770–785. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [Green Version]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.-M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient Elastography: A New Noninvasive Method for Assessment of Hepatic Fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef]
- Cassinotto, C.; Boursier, J.; de Lédinghen, V.; Lebigot, J.; Lapuyade, B.; Cales, P.; Hiriart, J.-B.; Michalak, S.; Bail, B.L.; Cartier, V.; et al. Liver Stiffness in Nonalcoholic Fatty Liver Disease: A Comparison of Supersonic Shear Imaging, FibroScan, and ARFI with Liver Biopsy. Hepatology 2016, 63, 1817–1827. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Bae, J.M.; Joo, S.K.; Woo, H.; Lee, D.H.; Jung, Y.J.; Kim, B.G.; Lee, K.L.; Kim, W. Prospective Comparison among Transient Elastography, Supersonic Shear Imaging, and ARFI Imaging for Predicting Fibrosis in Nonalcoholic Fatty Liver Disease. PLoS ONE 2017, 12, e0188321. [Google Scholar] [CrossRef]
- Herrmann, E.; de Lédinghen, V.; Cassinotto, C.; Chu, W.C.-W.; Leung, V.Y.-F.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of Biopsy-proven Liver Fibrosis by Two-dimensional Shear Wave Elastography: An Individual Patient Data-based Meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.; Chen, Y.; Lyu, G.; Wang, H.; Lin, G.; Gu, J. Diagnostic Accuracy of Two-dimensional Shear Wave Elastography and Magnetic Resonance Elastography for Staging Liver Fibrosis in Patients with Chronic Hepatitis B: A Systematic Review and Meta-analysis. J. Gastroenterol. Hepatol. 2022, 37, 1646. [Google Scholar] [CrossRef]
- Bauer, D.J.; Matic, V.; Mare, R.; Maiocchi, L.; Chromy, D.; Müllner-Bucsics, T.; Mandorfer, M.; Mustapic, S.; Sporea, I.; Ferraioli, G.; et al. Point Shear Wave Elastography by ElastPQ for Fibrosis Screening in Patients with NAFLD: A Prospective, Multicenter Comparison to Vibration-Controlled Elastography. Ultraschall Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Rao, J.; Wu, X.; Deng, R.; Ma, Y. Comparison of 2-D Shear Wave Elastography and Point Shear Wave Elastography for Assessing Liver Fibrosis. Ultrasound Med. Biol. 2021, 47, 408–427. [Google Scholar] [CrossRef]
- Paisant, A.; Lemoine, S.; Cassinotto, C.; de Lédinghen, V.; Ronot, M.; Irlès-Depé, M.; Vilgrain, V.; Le Bail, B.; Paradis, V.; Canivet, C.M.; et al. Reliability Criteria of Two-Dimensional Shear Wave Elastography: Analysis of 4277 Measurements in 788 Patients. Clinical Gastroenterol. Hepatol. 2022, 20, 400–408.e10. [Google Scholar] [CrossRef]
- Boursier, J.; Cassinotto, C.; Hunault, G.; Shili, S.; Lebigot, J.; Lapuyade, B.; Lannes, A.; Hiriart, J.-B.; Cartier, V.; Le Bail, B.; et al. Criteria to Determine Reliability of Noninvasive Assessment of Liver Fibrosis With Virtual Touch Quantification. Clin. Gastroenterol. Hepatol. 2019, 17, 164–171.e5. [Google Scholar] [CrossRef]
- Singh, S.; Venkatesh, S.K.; Wang, Z.; Miller, F.H.; Motosugi, U.; Low, R.N.; Hassanein, T.; Asbach, P.; Godfrey, E.M.; Yin, M.; et al. Diagnostic Performance of Magnetic Resonance Elastography in Staging Liver Fibrosis: A Systematic Review and Meta-Analysis of Individual Participant Data. Clin. Gastroenterol. Hepatol. 2015, 13, 440–451.e6. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, W.M.C.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.P. Serum Markers Detect the Presence of Liver Fibrosis: A Cohort Study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Guha, I.N.; Parkes, J.; Roderick, P.; Chattopadhyay, D.; Cross, R.; Harris, S.; Kaye, P.; Burt, A.D.; Ryder, S.D.; Aithal, G.P.; et al. Noninvasive Markers of Fibrosis in Nonalcoholic Fatty Liver Disease: Validating the European Liver Fibrosis Panel and Exploring Simple Markers. Hepatology 2008, 47, 455–460. [Google Scholar] [CrossRef]
- Calès, P.; Oberti, F.; Michalak, S.; Hubert-Fouchard, I.; Rousselet, M.-C.; Konaté, A.; Gallois, Y.; Ternisien, C.; Chevailler, A.; Lunel, F. A Novel Panel of Blood Markers to Assess the Degree of Liver Fibrosis. Hepatology 2005, 42, 1373–1381. [Google Scholar] [CrossRef]
- Nguyen-Khac, E.; Thiele, M.; Voican, C.; Nahon, P.; Moreno, C.; Boursier, J.; Mueller, S.; de Ledinghen, V.; Stärkel, P.; Gyune Kim, S.; et al. Non-Invasive Diagnosis of Liver Fibrosis in Patients with Alcohol-Related Liver Disease by Transient Elastography: An Individual Patient Data Meta-Analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 614–625. [Google Scholar] [CrossRef]
- Razavi, H.; Robbins, S.; Zeuzem, S.; Negro, F.; Buti, M.; Duberg, A.-S.; Roudot-Thoraval, F.; Craxi, A.; Manns, M.; Marinho, R.T.; et al. Hepatitis C Virus Prevalence and Level of Intervention Required to Achieve the WHO Targets for Elimination in the European Union by 2030: A Modelling Study. Lancet Gastroenterol. Hepatol. 2017, 2, 325–336. [Google Scholar] [CrossRef]
- Srivastava, A.; Gailer, R.; Tanwar, S.; Trembling, P.; Parkes, J.; Rodger, A.; Suri, D.; Thorburn, D.; Sennett, K.; Morgan, S.; et al. Prospective Evaluation of a Primary Care Referral Pathway for Patients with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2019, 71, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Majumdar, A.; Campos, S.; Gurusamy, K.; Pinzani, M.; Tsochatzis, E.A. Defining the Minimum Acceptable Diagnostic Accuracy of Noninvasive Fibrosis Testing in Cirrhosis: A Decision Analytic Modeling Study. Hepatology 2020, 71, 627–642. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- Vieira Barbosa, J.; Lai, M. Nonalcoholic Fatty Liver Disease Screening in Type 2 Diabetes Mellitus Patients in the Primary Care Setting. Hepatol. Commun. 2021, 5, 158–167. [Google Scholar] [CrossRef]
- Ginès, P.; Castera, L.; Lammert, F.; Graupera, I.; Serra-Burriel, M.; Allen, A.M.; Wong, V.W.; Hartmann, P.; Thiele, M.; Caballeria, L.; et al. Population Screening for Liver Fibrosis: Toward Early Diagnosis and Intervention for Chronic Liver Diseases. Hepatology 2022, 75, 219–228. [Google Scholar] [CrossRef]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of Implementing a “FIB-4 First” Strategy on a Pathway for Patients With NAFLD Referred From Primary Care. Hepatol. Commun. 2019, 3, 1322–1333. [Google Scholar] [CrossRef] [Green Version]
- Mansour, D.; Grapes, A.; Herscovitz, M.; Cassidy, P.; Vernazza, J.; Broad, A.; Anstee, Q.M.; McPherson, S. Embedding Assessment of Liver Fibrosis into Routine Diabetic Review in Primary Care. JHEP Rep. 2021, 3, 100293. [Google Scholar] [CrossRef]
- Crossan, C.; Majumdar, A.; Srivastava, A.; Thorburn, D.; Rosenberg, W.; Pinzani, M.; Longworth, L.; Tsochatzis, E.A. Referral Pathways for Patients with NAFLD Based on Non-Invasive Fibrosis Tests: Diagnostic Accuracy and Cost Analysis. Liver International 2019, 39, 2052–2060. [Google Scholar] [CrossRef]
- Congly, S.E.; Shaheen, A.A.; Swain, M.G. Modelling the Cost Effectiveness of Non-Alcoholic Fatty Liver Disease Risk Stratification Strategies in the Community Setting. PLoS ONE 2021, 16, e0251741. [Google Scholar] [CrossRef]
- Patel, P.J.; Banh, X.; Horsfall, L.U.; Hayward, K.L.; Hossain, F.; Johnson, T.; Stuart, K.A.; Brown, N.N.; Saad, N.; Clouston, A.; et al. Underappreciation of Non-Alcoholic Fatty Liver Disease by Primary Care Clinicians: Limited Awareness of Surrogate Markers of Fibrosis. Intern. Med. J. 2018, 48, 144–151. [Google Scholar] [CrossRef]
- Said, A.; Gagovic, V.; Malecki, K.; Givens, M.L.; Nieto, F.J. Primary Care Practitioners Survey of Non-Alcoholic Fatty Liver Disease. Ann. Hepatol. 2013, 12, 758–765. [Google Scholar] [CrossRef]
- Grattagliano, I.; Ubaldi, E.; Napoli, L.; Marulli, C.F.; Nebiacolombo, C.; Cottone, C.; Portincasa, P. Utility of Noninvasive Methods for the Characterization of Nonalcoholic Liver Steatosis in the Family Practice. The “VARES” Italian Multicenter Study. Ann. Hepatol. 2013, 12, 70–77. [Google Scholar] [CrossRef]
- Canivet, C.M.; Smati, S.; Lannes, A.; Brisseau, J.; Judon, L.; Roch, M.L.; Cariou, B.; Bellanger, W.; Guerci, B.; Boursier, J. Awareness of Chronic Liver Diseases, a Comparison between Diabetologists and General Practitioners. Clin. Res. Hepatol. Gastroenterol. 2021, 46, 101848. [Google Scholar] [CrossRef]
- Kallman, J.B.; Arsalla, A.; Park, V.; Dhungel, S.; Bhatia, P.; Haddad, D.; Wheeler, A.; Younossi, Z.M. Screening for Hepatitis B, C and Non-Alcoholic Fatty Liver Disease: A Survey of Community-Based Physicians. Aliment. Pharmacol. Ther. 2009, 29, 1019–1024. [Google Scholar] [CrossRef]
- van Asten, M.; Verhaegh, P.; Koek, G.; Verbeek, J. The Increasing Burden of NAFLD Fibrosis in the General Population: Time to Bridge the Gap between Hepatologists and Primary Care. Hepatology 2017, 65, 1078. [Google Scholar] [CrossRef] [Green Version]
- Boursier, J.; Shreay, S.; Fabron, C.; Torreton, E.; Fraysse, J. Hospitalization Costs and Risk of Mortality in Adults with Nonalcoholic Steatohepatitis: Analysis of a French National Hospital Database. EClinicalMedicine 2020, 25, 100445. [Google Scholar] [CrossRef]
- Bergqvist, C.-J.; Skoien, R.; Horsfall, L.; Clouston, A.D.; Jonsson, J.R.; Powell, E.E. Awareness and Opinions of Non-Alcoholic Fatty Liver Disease by Hospital Specialists. Intern. Med. J. 2013, 43, 247–253. [Google Scholar] [CrossRef]
- Marjot, T.; Sbardella, E.; Moolla, A.; Hazlehurst, J.M.; Tan, G.D.; Ainsworth, M.; Cobbold, J.F.L.; Tomlinson, J.W. Prevalence and Severity of Non-Alcoholic Fatty Liver Disease Are Underestimated in Clinical Practice: Impact of a Dedicated Screening Approach at a Large University Teaching Hospital. Diabet. Med. 2018, 35, 89–98. [Google Scholar] [CrossRef]
- Kim, H.; Yang, J.D.; El-Serag, H.B.; Kanwal, F. Awareness of Chronic Viral Hepatitis in the United States: An Update from the National Health and Nutrition Examination Survey. J. Viral Hepat. 2019, 26, 596–602. [Google Scholar] [CrossRef]
- Alqahtani, S.A.; Paik, J.M.; Biswas, R.; Arshad, T.; Henry, L.; Younossi, Z.M. Poor Awareness of Liver Disease Among Adults With NAFLD in the United States. Hepatol. Commun. 2021, 5, 1833–1847. [Google Scholar] [CrossRef]
- van der Veen, Y.J.; Voeten, H.A.; de Zwart, O.; Richardus, J.H. Awareness, Knowledge and Self-Reported Test Rates Regarding Hepatitis B in Turkish-Dutch: A Survey. BMC Public Health 2010, 10, 512. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, P.; Mourad, A.; Marcellin, F.; Trylesinski, A.; Calleja, J.L.; Protopopescu, C.; Lazarus, J.V. Knowledge of Liver Fibrosis Stage among Adults with NAFLD / NASH Improves Adherence to Lifestyle Changes. Liver Int. 2022, 42, 984–994. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ekstedt, M.; Marchesini, G.; Mullen, J.; Novak, K.; Pericàs, J.M.; Roel, E.; Romero-Gómez, M.; Ratziu, V.; Tacke, F.; et al. A Cross-Sectional Study of the Public Health Response to Non-Alcoholic Fatty Liver Disease in Europe. J. Hepatol. 2020, 72, 14–24. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Location | Patients (Years) | Sample Size with TE Available (n) | VCTE Thresholds | Prevalence of Outcome (%) | Risk Factors Independently Associated with Liver Fibrosis in Multivariate Analysis | |
|---|---|---|---|---|---|---|
| Roulot 2011 [12] | France | ≥45 | 1190 | 8.0 kPa | 7.5 | Metabolic syndrome; BMI ≥30; Age ≥57 years; Diabetes; GGT ≥45 IU/l; ALT ≥40 IU/l |
| Wong 2012 a [19] | Hong Kong | 18–70 | 759 | 9.6 kPa | 2.0 | ALT level; BMI |
| Fabrellas 2013 [13] | Spain | 18–70 | 495 | 6.8 kPa | 5.7 | - |
| You 2015 [17] | Korea | adults | 159 | 7.0 kPa | 6.9 | BMI >24.2; ALT >19 IU/l; carotid intimal media thickness >0.68 mm; ≥1 calcified carotid plaque |
| Koehler 2016 [15] | The Netherlands | ≥45 | 3041 | 8.0 kPa | 5.6 | Type 2 diabetes; liver steatosis; HBsAg and/or anti-HCV positive; age; spleen size; current or former smoking; ALT level |
| Caballeria 2018 [14] | Spain | 18–75 | 3076 | 8.0 kPa | 5.8 | Male sex; AST and/or ALT >ULN; abdominal obesity; glucose level ≥100 mg/dL; low HDL; triglyceride level ≥150 mg/dL; type 2 diabetes |
| Llop 2021 [16] | Spain | 20–79 | 11,440 | 8.0 kPa | 5.6 | Age; male sex; AST level; ALT level; metabolic syndrome |
| Nah 2021 [20] | Korea | 19–85 | 8183 | 2.90 kPa * | 9.5 | Age; male sex; diabetes; HBsAg positivity; abnormal LFT; obesity; metabolic syndrome |
| Advantages | Disadvantages | |
|---|---|---|
| Simple blood tests |
|
|
| Specialized blood tests |
|
|
| Transient elastography |
|
|
| pSWE/2D-SWE |
|
|
| MRE |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canivet, C.M.; Boursier, J. Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022? Diagnostics 2023, 13, 91. https://doi.org/10.3390/diagnostics13010091
Canivet CM, Boursier J. Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022? Diagnostics. 2023; 13(1):91. https://doi.org/10.3390/diagnostics13010091
Chicago/Turabian StyleCanivet, Clémence M., and Jérôme Boursier. 2023. "Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022?" Diagnostics 13, no. 1: 91. https://doi.org/10.3390/diagnostics13010091
APA StyleCanivet, C. M., & Boursier, J. (2023). Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022? Diagnostics, 13(1), 91. https://doi.org/10.3390/diagnostics13010091