
Bacteremia (Sepsis), Hepatorenal Syndrome, and Serum Creatinine Levels Rather than Types or Microbial Patterns Predicted the Short-Term Survival of Cirrhotic Patients Complicated with Spontaneous Bacterial Peritonitis

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
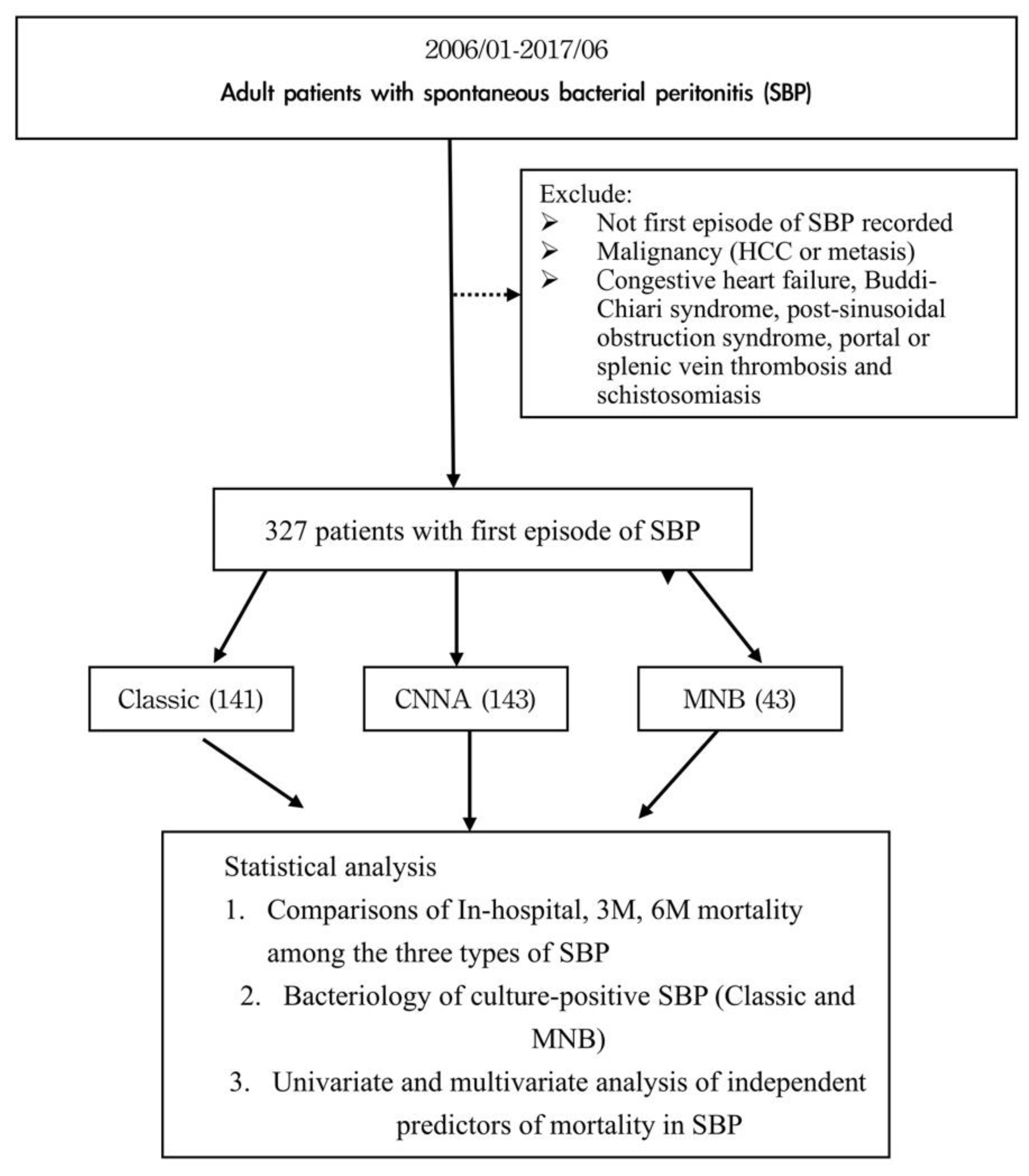
2.1. Patient Selection and Follow-Ups
2.2. Diagnosis, Definition, and Management of Liver Cirrhosis and Spontaneous Bacterial Peritonitis
2.3. The Outcomes of SBP
2.4. The Diagnosis of Hepatorenal Syndrome and Hepatic Encephalopathy
2.5. The Diagnosis of Bacteremia (Sepsis)
2.6. Calculations of Predicting Scores
2.7. Methods/Assays Used For Serum Biochemistry and Hemogram
2.8. Statistical Analysis
3. Results
3.1. Flowchart
3.2. Baseline Demographic Characteristics of 327 Patients
3.3. Baseline Characteristics and Prognosis Comparison of the Three Types of SBP
3.4. The Bacteriology of SBP
3.5. Multivariable Logistic Regression Analysis to Predict Mortality
3.5.1. In-Hospital Mortality
3.5.2. 3-Month Mortality
3.5.3. 6-Month Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albillos, A.; Lario, M.; Alvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.H.; Jeng, W.J.; Ho, Y.P.; Teng, W.; Chen, W.T.; Chen, Y.C.; Lin, S.M.; Chiu, C.T.; Sheen, I.S.; Lin, C.Y. Increased regulatory T cells in patients with liver cirrhosis correlated with hyperbilirubinemia and predict bacterial complications. J. Gastroenterol. Hepatol. 2015, 30, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Wiest, R.; Garcia-Tsao, G. Bacterial translocation (BT) in cirrhosis. Hepatology 2005, 41, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Navasa, M.; Gómez, J.; Colmenero, J.; Vila, J.; Arroyo, V.; Rodés, J. Bacterial infections in cirrhosis: Epidemiological changes with invasive procedures and norfloxacin prophylaxis. Hepatology 2002, 35, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Lata, J.; Stiburek, O.; Kopacova, M. Spontaneous bacterial peritonitis: A severe complication of liver cirrhosis. World J. Gastroenterol. 2009, 15, 5505–5510. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Tseng, H.J.; Amodio, P.; Chen, Y.L.; Wang, S.F.; Chang, S.H.; Hsieh, S.Y.; Lin, C.Y. Hepatic Encephalopathy and Spontaneous Bacterial Peritonitis Improve Cirrhosis Outcome Prediction: A Modified Seven-Stage Model as a Clinical Alternative to MELD. J. Pers. Med. 2020, 10, 186. [Google Scholar] [CrossRef]
- Runyon, B.A.; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology 2013, 57, 1651–1653. [Google Scholar] [CrossRef]
- Oladimeji, A.A.; Temi, A.P.; Adekunle, A.E.; Taiwo, R.H.; Ayokunle, D.S. Prevalence of spontaneous bacterial peritonitis in liver cirrhosis with ascites. Pan Afr. Med. J. 2013, 15, 128. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [Green Version]
- Al-Ghamdi, H.; Al-Harbi, N.; Mokhtar, H.; Daffallah, M.; Memon, Y.; Aljumah, A.A.; Sanai, F.M. Changes in the patterns and microbiology of spontaneous bacterial peritonitis: Analysis of 200 cirrhotic patients. Acta Gastroenterol. Belg. 2019, 82, 261–266. [Google Scholar]
- Almeida, P.R.L.; Leao, G.S.; Goncalves, C.D.G.; Picon, R.V.; Tovo, C.V. Impact of Microbiological Changes on Spontaneous Bacterial Peritonitis in Three Different Periods over 17 Years. Arq. Gastroenterol. 2018, 55, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Oey, R.C.; de Man, R.A.; Erler, N.S.; Verbon, A.; van Buuren, H.R. Microbiology and antibiotic susceptibility patterns in spontaneous bacterial peritonitis: A study of two Dutch cohorts at a 10-year interval. United Eur. Gastroenterol. J. 2018, 6, 614–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, D.Y.; Sheen, I.S.; Chiu, C.T.; Lin, S.M.; Kuo, Y.C.; Liaw, Y.F. Ultrasonographic changes of early liver cirrhosis in chronic hepatitis B: A longitudinal study. J. Clin. Ultrasound 1993, 21, 303–308. [Google Scholar] [CrossRef]
- Runyon, B.A.; Montano, A.A.; Akriviadis, E.A.; Antillon, M.R.; Irving, M.A.; McHutchison, J.G. The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Ann. Intern. Med. 1992, 117, 215–220. [Google Scholar] [CrossRef]
- de Franchis, R.; Baveno, V.I.F. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liaw, Y.F.; Leung, N.; Guan, R.; Lau, G.K.; Merican, I.; McCaughan, G.; Gane, E.; Kao, J.H.; Omata, M.; Chronic Hepatitis B Guideline Working Party of the Asian-Pacific Association for the Study of the Liver. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2005 update. Liver Int. 2005, 25, 472–489. [Google Scholar] [CrossRef] [Green Version]
- Rimola, A.; García-Tsao, G.; Navasa, M.; Piddock, L.J.; Planas, R.; Bernard, B.; Inadomi, J.M. Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: A consensus document. J. Hepatol. 2000, 32, 142–153. [Google Scholar] [CrossRef]
- Akriviadis, E.A.; Runyon, B.A. Utility of an algorithm in differentiating spontaneous from secondary bacterial peritonitis. Gastroenterology 1990, 98, 127–133. [Google Scholar] [CrossRef]
- Runyon, B.A.; Committee, A.P.G. Management of adult patients with ascites due to cirrhosis: An update. Hepatology 2009, 49, 2087–2107. [Google Scholar] [CrossRef]
- Biggins, S.W.; Angeli, P.; Garcia-Tsao, G.; Gines, P.; Ling, S.C.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef]
- Angeli, P.; Gines, P.; Wong, F.; Bernardi, M.; Boyer, T.D.; Gerbes, A.; Moreau, R.; Jalan, R.; Sarin, S.K.; Piano, S.; et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. J. Hepatol. 2015, 62, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Campagna, F.; Montagnese, S.; Ridola, L.; Senzolo, M.; Schiff, S.; De Rui, M.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Merkel, C.; et al. The animal naming test: An easy tool for the assessment of hepatic encephalopathy. Hepatology 2017, 66, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Association for the Study of Liver Diseases; European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Luca, A.; Angermayr, B.; Bertolini, G.; Koenig, F.; Vizzini, G.; Ploner, M.; Peck-Radosavljevic, M.; Gridelli, B.; Bosch, J. An integrated MELD model including serum sodium and age improves the prediction of early mortality in patients with cirrhosis. Liver Transpl. 2007, 13, 1174–1180. [Google Scholar] [CrossRef]
- Garcia-Tsao, G. Current management of the complications of cirrhosis and portal hypertension: Variceal hemorrhage, ascites, and spontaneous bacterial peritonitis. Gastroenterology 2001, 120, 726–748. [Google Scholar] [CrossRef]
- Hung, T.H.; Tsai, C.C.; Hsieh, Y.H.; Tsai, C.C. The long-term mortality of spontaneous bacterial peritonitis in cirrhotic patients: A 3-year nationwide cohort study. Turk. J. Gastroenterol. 2015, 26, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Garcia-Tsao, G. Renal dysfunction is the most important independent predictor of mortality in cirrhotic patients with spontaneous bacterial peritonitis. Clin. Gastroenterol. Hepatol. 2011, 9, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Huo, T.I.; Lin, H.C.; Wu, J.C.; Hou, M.C.; Lee, F.Y.; Lee, P.C.; Chang, F.Y.; Lee, S.D. Limitation of the model for end-stage liver disease for outcome prediction in patients with cirrhosis-related complications. Clin. Transplant. 2006, 20, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Huo, T.I.; Lin, H.C.; Huo, S.C.; Lee, P.C.; Wu, J.C.; Lee, F.Y.; Hou, M.C.; Lee, S.D. Comparison of four model for end-stage liver disease-based prognostic systems for cirrhosis. Liver Transpl. 2008, 14, 837–844. [Google Scholar] [CrossRef]
- Chen, P.C.; Chen, B.H.; Huang, C.H.; Jeng, W.J.; Hsieh, Y.C.; Teng, W.; Chen, Y.C.; Ho, Y.P.; Sheen, I.S.; Lin, C.Y. Integrated model for end-stage liver disease maybe superior to some other model for end-stage liver disease-based systems in addition to Child-Turcotte-Pugh and albumin-bilirubin scores in patients with hepatitis B virus-related liver cirrhosis and spontaneous bacterial peritonitis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Follo, A.; Llovet, J.M.; Navasa, M.; Planas, R.; Forns, X.; Francitorra, A.; Rimola, A.; Gassull, M.A.; Arroyo, V.; Rodes, J. Renal impairment after spontaneous bacterial peritonitis in cirrhosis: Incidence, clinical course, predictive factors and prognosis. Hepatology 1994, 20, 1495–1501. [Google Scholar] [CrossRef]
- Salerno, F.; Navickis, R.J.; Wilkes, M.M. Albumin infusion improves outcomes of patients with spontaneous bacterial peritonitis: A meta-analysis of randomized trials. Clin. Gastroenterol. Hepatol. 2013, 11, 123–130.e121. [Google Scholar] [CrossRef] [PubMed]
- Sort, P.; Navasa, M.; Arroyo, V.; Aldeguer, X.; Planas, R.; Ruiz-del-Arbol, L.; Castells, L.; Vargas, V.; Soriano, G.; Guevara, M.; et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N. Engl. J. Med. 1999, 341, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Lin, C.Y.; Sheen, I.S.; Chen, W.T.; Lin, T.N.; Ho, Y.P.; Chiu, C.T. Recurrence of spontaneous bacterial peritonitis in cirrhotic patients non-prophylactically treated with norfloxacin: Serum albumin as an easy but reliable predictive factor. Liver Int. 2011, 31, 184–191. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit. Care Med. 2008, 36, 296–327. [Google Scholar] [CrossRef] [Green Version]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437, 1437.e1–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Na, S.H.; Kim, E.J.; Nam, E.Y.; Song, K.H.; Choe, P.G.; Park, W.B.; Bang, J.H.; Kim, E.S.; Park, S.W.; Kim, H.B.; et al. Comparison of clinical characteristics and outcomes of spontaneous bacterial peritonitis and culture negative neutrocytic ascites. Scand. J. Gastroenterol. 2017, 52, 199–203. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Parameters | Values |
|---|---|
| Clinical parameters | |
| Age, mean ± SD | 57.1 ± 13.6 |
| Male No. (%) | 236 (72%) |
| Etiology No. (%) | |
| Alcohol HBV HCV Others | 94 (28.7) 118 (36.0) 74 (22.6) 74 (22.6) |
| Classic (Positive PMN and culture) | 141 (43.2) |
| CNNA | 143 (43.7) |
| MNB | 43 (13.1) |
| Blood culture positive | 42(12.8%) |
| Laboratory parametersMedian (IQR) | |
| iMELD score | 44.44 (37.58–52.94) |
| MELD score | 21.11 (15.39–28.36) |
| CTP score | 9(8–11) |
| INR | 1.64 (1.39–2.20) |
| WBC (103/μL) | 7.9 (5.20–12.80) |
| Hemoglobin (g/dL) | 9.6 (8.4–11.0) |
| PLT (103/μL) | 74.0 (48.0–122.0) |
| Creatinine (mg/dL) | 1.2 (0.86–2.41) |
| Bilirubin Total (mg/dL) | 4.1 (1.9–9.8) |
| AST (U/L) | 70 (46–129) |
| ALT (U/L) | 36 (23–60) |
| Sodium (mEq/L) | 135 (131–139) |
| Albumin (g/dL) | 2.4 (2.2–2.8) |
| Anti-viral agents, n, (%) | |
| Entecavir | 64(19.5) |
| Lamivudine | 4 (1.2) |
| Telbivudine | 2 (0.6) |
| Tenofovir disoproxil fumarate | 15 (4.5) |
| SBP Types(n) | Classic (141) | CNNA (143) | MNB (43) | p-Value |
|---|---|---|---|---|
| Clinical parameters | ||||
| Age, mean ± SD | 57.6 ± 14.1 | 57.3 ± 13.5 | 55.1 ± 12.8 | 0.578 |
| Male No. (%) | 104(73.8) | 101(70.6) | 31(72.1) | 0.841 |
| Etiology No. (%) | 0.157 | |||
| Alcohol HBV HCV Others | 43(30.5) 58(40.2) 36(25.5) 4(2.8) | 39(27.3) 65(45.5) 33(23.0) 6(4.2) | 10(23.3) 23(53.5) 9(20.9) 1(2.3) | |
| Blood culture positive, n (%) | 39(27.7) | 0 | 3(7) | <0.001 |
| Laboratory parametersMedian (IQR) | ||||
| iMELD score | 44.8(30.7–55.0) | 44.6(37.4–53.2) | 40.2(33.9–47.5) | 0.015 |
| MELD score | 20.5(15.8–28.6) | 21.9(12.6–30.5) | 21.2(12.6–30.5) | 0.055 |
| CTP score | 9(8–10) | 10(8–11) | 9(8–11) | 0.196 |
| INR | 1.7(1.4–2.1) | 1.6(1.4–2.3) | 1.6(1.3–2.2) | 0.869 |
| WBC (103/μL) | 8.4(5.8–11.6) | 7.8(5.5–13.3) | 6.6(4.0–12.6) | 0.348 |
| Hemoglobin (g/dL) | 9.6(8.4–11.2) | 9.8(8.5–11.1) | 9.2(8.1–10.2) | 0.248 |
| PLT (103/μL) | 72(46–105) | 76(50–139) | 72(46–120) | 0.259 |
| Creatinine (mg/dL) | 1.5(1.0–2.7) | 1.0(0.7–1.8) | 1.0(0.7–2.0) | <0.001 |
| Bilirubin Total (mg/dL) | 4.0(2.1–8.8) | 4.2(2.0–11.0) | 3.0(1.4–7.8) | 0.457 |
| Sodium (mEq/L) | 135(130–138) | 134(131–139) | 137(135–141) | <0.001 |
| Albumin (g/dL) | 2.3(2.0–2.6) | 2.6(2.3–3.0) | 2.4(2.1–2.8) | <0.001 |
| Ascites analysis, (Median (IQR)) | |
|---|---|
| WBC (103/μL) | 1585 (439–4996) |
| PMN (cells/mm3) | 1394 (344–4203) |
| Total protein (g/dL) | 1.3 (1.3–1.7) |
| Albumin (g/dL) | 0.5 (0.3–0.7) |
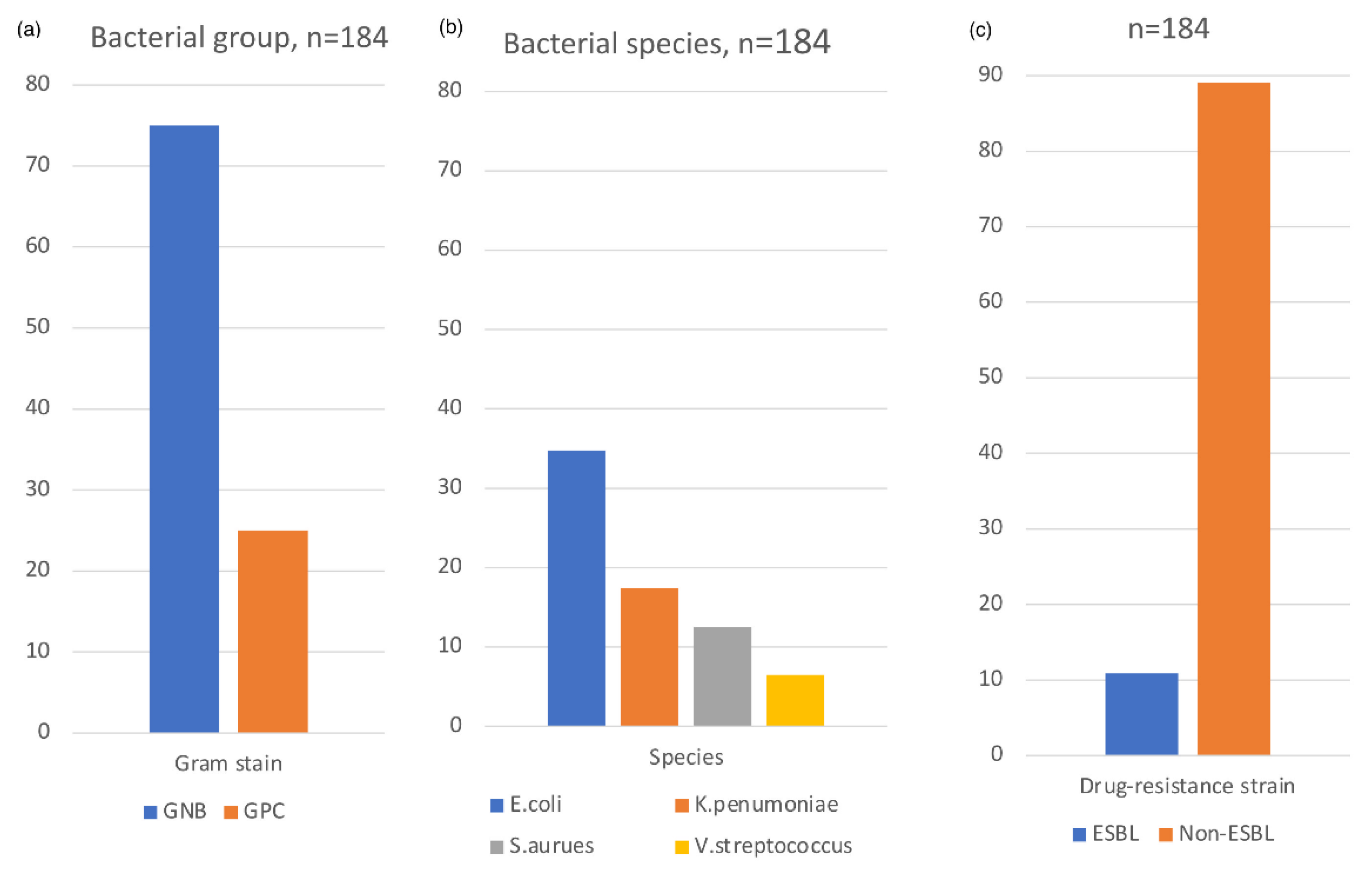
| Bacterial group, n, (%), total n = 184 | |
| Gram-negative bacteria (GNB) | 138 (75.0) |
| Ceftriaxone sensitive GNB | 110 (79.7) |
| Ceftriaxone resistant GNB | 28 (20.3) |
| Gram-positive coccus (GPC) | 46 (25.0) |
| Bacterial species, n, (%), total n = 184 | |
| Escherichia coli | 64 (34.8) |
| Escherichia coli, ESBL strain | 14/64 (21.8) |
| Klebsiella pneumoniae | 32 (17.4) |
| Klebsiella pneumoniae, ESBL strain | 1/32 (3.1) |
| Staphylococcus aureus | 23 (12.5) |
| ORSA | 5/23 (21.7) |
| Viridans streptococcus | 12 (6.5) |
| SBP Types(n) | Classic (141) | MNB (43) | p-Value |
|---|---|---|---|
| GNB vs. GPC | 0.005 | ||
| GNB, No. (%) | 110(78) | 29(67.4) | |
| GPC, No. (%) | 34 (22) | 14(32.6) | |
| Ceftriaxone sensitive vs. resistant GNB | |||
| Ceftriaxone sensitive GNB | 91(82.7) | 19(65.5) | 0.008 |
| Ceftriaxone resistant GNB | 19(17.3) | 9(34.5) | 0.233 |
| ESBL strain, No. (%) | 15(13.6) | 0(0) | <0.001 |
| Univariable Logistic Reg | Multivariable Logistic Reg | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| SBP types | ||||
| CNNA | Reference | |||
| MNB | 0.938 (0.459–1.914) | 0.859 | ||
| Classic | 1.373 (0.853–2.211) | 0.191 | ||
| Bacteremia | 2.286 (1.185–4.408) | 0.014 | 3.192 (1.419–7.176) | 0.005 |
| Gram stain | ||||
| 0 | Reference | |||
| GNB | 1.283 (0.796–2.066) | 0.306 | ||
| GPC | 1.391 (0.690–2.805) | 0.356 | ||
| ESBL strain | 2.366 (0.654–8.553) | 0.189 | ||
| CRO-resistant | ||||
| 0 | Reference | Reference | ||
| Ascites | 5.155 (1.623–16.373) | 0.005 | 6.493 (1.791–23.538) | 0.004 |
| Blood cult. | 1.145 (0.188–6.961) | 0.883 | 1.487 (0.232–9.515 | 0.676 |
| Ascites + Blood | 4.295 (0.82–22.514) | 0.085 | 0.803 (0.113–5.720) | 0.826 |
| Age | 1.018 (1.001–1.035) | 0.038 | 1.013 (0.992–1.034) | 0.242 |
| Sex | 0.875 (0.535–1.432) | 0.596 | ||
| Etiology | ||||
| Alcohol | Reference | |||
| HBV | 1.117 (0.659–1.891) | 0.682 | 1.196 (0.638–2.244) | 0.576 |
| HCV | 0.429 (0.221–0.833) | 0.012 | 0.582 (0.265–1.277) | 0.177 |
| Others | 0.762 (0.208–2.787) | 0.681 | 0.746 (0.175–3.337) | 0.720 |
| HE | ||||
| 0 | Reference | Reference | ||
| 1 | 1.538 (0.706–3.349) | 0.278 | 1.161 (0.436–3.094) | 0.765 |
| 2 | 2.766 (1.302–5.876) | 0.008 | 1.862 (0.764–4.538) | 0.171 |
| 3–4 | 3.786 (1.253–11.437) | 0.018 | 1.843 (0.537–6.330) | 0.331 |
| HRS | 9.744 (3.633–26.132) | <0.001 | 7.274 (2.497–21.192) | <0.001 |
| Cr | 1.397 (1.218–1.601) | <0.001 | 1.198 (1.035–1.388) | 0.015 |
| Albumin | 0.836 (0.536–1.305) | 0.431 | ||
| WBC | 1.031 (1.004–1.058) | 0.023 | 1.026 (1–1.052) | 0.049 |
| CTP score | 1.257 (1.091–1.448) | 0.002 | 1.118 (0.899–1.391) | 0.316 |
| MELD score | 1.05 (1.026–1.075) | <0.001 | 0.985 (0.926–1.047) | 0.622 |
| MELD-Na | 1.048 (1.025–1.071) | <0.001 | 1.04 (0.98–1.094) | 0.126 |
| iMELD score | 1.05 (1.028–1.073) | <0.001 | 1.009 (0.948–1.073) | 0.783 |
| Univariable Logistic Reg | Multivariable Logistic Reg | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| SBP types | ||||
| CNNA | Reference | |||
| MNB | 0.938 (0.459–1.914) | 0.859 | ||
| Classic | 1.328 (0.833–2.117) | 0.234 | ||
| Bacteremia | 2.343 (1.170–4.691) | 0.016 | 2.244 (1.077–4.673) | 0.031 |
| Gram stain | ||||
| 0 | Reference | |||
| GNB | 1.328 (0.834–2.115) | 0.232 | ||
| GPC | 1.422 (0.709–2.849) | 0.321 | ||
| ESBL strain | 2.261 (0.574–8.900) | 0.243 | ||
| CRO-resistant | ||||
| 0 | Reference | |||
| Ascites | 3.102 (0.978–9.837) | 0.055 | ||
| Blood cult. | 1.551 (0.255–9.416) | 0.883 | ||
| Ascites + Blood | 6.204 (0.738–52.16) | 0.093 | ||
| Age | 1.010 (0.994–1.026) | 0.24 | ||
| Sex | 1.113 (0.686–1.805) | 0.665 | ||
| Etiology | ||||
| Alcohol | Reference | |||
| HBV | 0.775 (0.456–1.315) | 0.344 | ||
| HCV | 0.452 (0.244–0.838) | 0.012 | ||
| Others | 0.571 (0.162–2.010) | 0.383 | ||
| HE | ||||
| 0 | Reference | |||
| 1 | 1.325 (0.611–2.874) | 0.476 | ||
| 2 | 2.369 (1.077–5.214) | 0.032 | ||
| 3–4 | 2.154 (0.715–6.487) | 0.173 | ||
| HRS | 7.420 (2.534–21.732) | <0.001 | 6.034 (1.977–18.416) | 0.002 |
| Cr | 1.283 (1.122–1.468) | <0.001 | 1.188 (1.024–1.378) | 0.023 |
| Albumin | 0.643 (0.414–1.000) | 0.431 | 0.711 (0.436–1.157) | 0.170 |
| WBC | 1.017 (0.994–1.041) | 0.158 | ||
| CTP Score | 1.169 (1.020–1.340) | 0.025 | 1.128 (0.929–1.370) | 0.225 |
| MELD score | 1.033 (1.010–1.056) | 0.005 | 0.968 (0.918–1.020) | 0.221 |
| MELD-Na | 1.029 (1.009–1.051) | 0.006 | 0.995 (0.953–1.039) | 0.811 |
| iMELD score | 1.035 (1.014–1.057) | 0.001 | 1.040 (0.991–1.092) | 0.107 |
| Univariable Logistic Reg | Multivariable Logistic Reg | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| SBP types | ||||
| CNNA | Reference | |||
| MNB | 1.118 (0.554–2.259) | 0.755 | ||
| Classic | 1.036 (0.644–1.668) | 0.883 | ||
| Bacteremia | 1.963 (0.948–4.061) | 0.069 | 1.797 (0.829–3.894) | 0.138 |
| Gram stain | ||||
| 0 | Reference | |||
| GNB | 0.982 (0.612–1.576) | 0.939 | ||
| GPC | 1.436 (0.689–2.993) | 0.334 | ||
| ESBL strain | 1.519 (0.386–5.985) | 0.550 | ||
| CRO-resistant | ||||
| 0 | Reference | |||
| Ascites | 2.039 (0.643–6.472) | 0.227 | ||
| Blood cult. | 1.020 (0.168–6.194) | 0.983 | ||
| Ascites + Blood | 4.079 (0.485–34.306) | 0.196 | ||
| Age | 1.015 (0.999–1.032) | 0.07 | 1.009 (0.989–1.030) | 0.388 |
| Sex | 1.239 (0.758–2.025) | 0.393 | ||
| Etiology | ||||
| Alcohol | Reference | |||
| HBV | 0.856 (0.497–1.474) | 0.576 | ||
| HCV | 0.633 (0.341–1.175) | 0.147 | ||
| Others | 1.446 (0.358–5.835) | 0.604 | ||
| HE | ||||
| 0 | Reference | |||
| 1 | 1.329 (0.593–2.978) | 0.490 | ||
| 2 | 1.538 (0.698–3.390) | 0.285 | ||
| 3–4 | 2.797 (0.769–10.169) | 0.118 | ||
| HRS | 4.866 (1.661–14.260) | 0.004 | 3.857 (1.248–11.919) | 0.019 |
| Cr | 1.343 (1.146–1.574) | <0.001 | 1.218 (1.030–1.441) | 0.021 |
| Albumin | 0.685 (0.438–1.070) | 0.097 | 0.731 (0.443–1.204) | 0.218 |
| WBC | 1.035 (1.002–1.069) | 0.035 | 1.029 (0.996–1.062) | 0.083 |
| CTP Score | 1.142 (0.993–1.313) | 0.062 | 1.126 (0.924–1.373) | 0.240 |
| MELD score | 1.030 (1.006–1.055) | 0.013 | 0.972 (0.918–1.028) | 0.316 |
| MELD-Na | 1.024 (1.003–1.045) | 0.024 | 0.982 (0.967–1.028) | 0.437 |
| iMELD score | 1.036 (1.014–1.058) | 0.001 | 1.048 (0.991–1.107) | 0.098 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-H.; Wang, S.-F.; Lee, C.-H.; Wu, Y.-M.; Chang, C.; Chen, B.-H.; Huang, Y.-T.; Ho, Y.-P. Bacteremia (Sepsis), Hepatorenal Syndrome, and Serum Creatinine Levels Rather than Types or Microbial Patterns Predicted the Short-Term Survival of Cirrhotic Patients Complicated with Spontaneous Bacterial Peritonitis. Diagnostics 2023, 13, 94. https://doi.org/10.3390/diagnostics13010094
Huang C-H, Wang S-F, Lee C-H, Wu Y-M, Chang C, Chen B-H, Huang Y-T, Ho Y-P. Bacteremia (Sepsis), Hepatorenal Syndrome, and Serum Creatinine Levels Rather than Types or Microbial Patterns Predicted the Short-Term Survival of Cirrhotic Patients Complicated with Spontaneous Bacterial Peritonitis. Diagnostics. 2023; 13(1):94. https://doi.org/10.3390/diagnostics13010094
Chicago/Turabian StyleHuang, Chien-Hao, Sheng-Fu Wang, Chen-Hung Lee, Yen-Mu Wu, Ching Chang, Bo-Huan Chen, Yu-Tung Huang, and Yu-Pin Ho. 2023. "Bacteremia (Sepsis), Hepatorenal Syndrome, and Serum Creatinine Levels Rather than Types or Microbial Patterns Predicted the Short-Term Survival of Cirrhotic Patients Complicated with Spontaneous Bacterial Peritonitis" Diagnostics 13, no. 1: 94. https://doi.org/10.3390/diagnostics13010094
APA StyleHuang, C. -H., Wang, S. -F., Lee, C. -H., Wu, Y. -M., Chang, C., Chen, B. -H., Huang, Y. -T., & Ho, Y. -P. (2023). Bacteremia (Sepsis), Hepatorenal Syndrome, and Serum Creatinine Levels Rather than Types or Microbial Patterns Predicted the Short-Term Survival of Cirrhotic Patients Complicated with Spontaneous Bacterial Peritonitis. Diagnostics, 13(1), 94. https://doi.org/10.3390/diagnostics13010094