
Intraoperative MRI Assessment of the Tissue Damage during Laser Ablation of Hypothalamic Hamartoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Aim
3. Material and Methods
3.1. Study Population and Imaging Analysis
3.2. Statistical Methods
4. Results
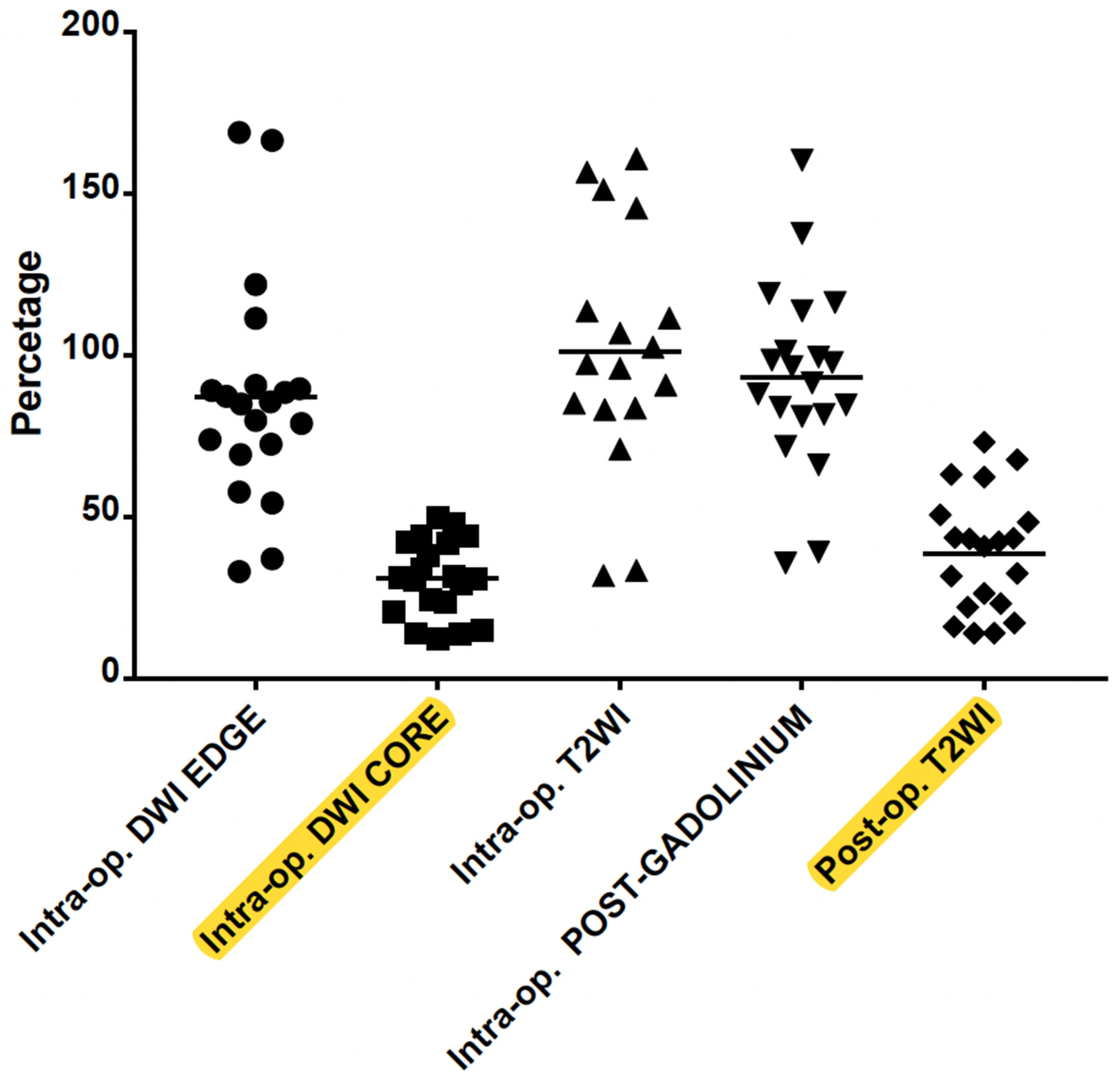
Summary of the Results: The Area of DWI Hypointense Core, Immediately after the Ablation, Better Correlates with the Final Encephalomalacic Damage on the Follow-Up Scan
5. Discussion
5.1. LITT Technique and Thermal Heat Maps
5.2. Literature Analysis
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wei, Z.; Vodovotz, L.; Luy, D.D.; Deng, H.; Niranjan, A.; Lunsford, L.D. Stereotactic radiosurgery as the initial management option for small-volume hypothalamic hamartomas with intractable epilepsy: A 35-year institutional experience and systematic review. J. Neurosurg. Pediatr. 2023, 31, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Consales, A.; Cognolato, E.; Pacetti, M.; Mancardi, M.M.; Tortora, D.; Di Perna, G.; Piatelli, G.; Nobili, L. Magnetic Resonance-Guided Laser Interstitial Thermal Therapy (MR-gLiTT) in Pediatric Epilepsy Surgery: State of the Art and Presentation of Giannina Gaslini Children’s Hospital (Genoa, Italy) Series. Front. Neurol. 2021, 12, 739034. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.H.D.; Lo, W.B.; Mundil, N.R.; Walsh, A.R. Transtemporal approach to hypothalamic hamartomas in children: Report of 3 cases. J. Neurosurg. Pediatr. 2020, 25, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Lehner, K.R.; D’Amico, R.S.; Rahme, R.; Schneider, J.R.; Privler, G.G.; Faltings, L.J.; Du, V.X.; Boockvar, J.A.; Rekate, H.L.; Langer, D.J. Microsurgical management of complex hypothalamic hamartomas in the era of minimally invasive therapy: A case series and narrative review. World Neurosurg. 2022, 160, e388–e397. [Google Scholar] [CrossRef]
- Rolston, J.D.; Chang, E.F. Stereotactic laser ablation for hypothalamic hamartoma. Neurosurg. Clin. N. Am. 2016, 27, 59–67. [Google Scholar] [CrossRef]
- Grewal, S.S.; Tatum, W.O. Laser thermal ablation in epilepsy. Expert Rev. Neurother. 2019, 19, 1211–1218. [Google Scholar] [CrossRef]
- Fangusaro, J.; Witt, O.; Hernáiz Driever, P.; Bag, A.K.; de Blank, P.; Kadom, N.; Kilburn, L.; Lober, R.M.; Robison, N.J.; Fisher, M.J.; et al. Response assessment in paediatric low-grade glioma: Recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) working group. Lancet Oncol. 2020, 21, e305–e316. [Google Scholar] [CrossRef]
- Kilday, J.-P.; Branson, H.; Rockel, C.; Laughlin, S.; Mabbott, D.; Bouffet, E.; Bartels, U. Tumor volumetric measurements in surgically inaccessible pediatric low-grade glioma. J. Pediatr. Hematol. Oncol. 2015, 37, e31–e36. [Google Scholar] [CrossRef]
- Shah, G.D.; Kesari, S.; Xu, R.; Batchelor, T.T.; O’Neill, A.M.; Hochberg, F.H.; Levy, B.; Bradshaw, J.; Wen, P.Y. Comparison of linear and volumetric criteria in assessing tumor response in adult high-grade gliomas. Neuro Oncol. 2006, 8, 38–46. [Google Scholar] [CrossRef] [Green Version]
- D’Arco, F.; O’Hare, P.; Dashti, F.; Lassaletta, A.; Loka, T.; Tabori, U.; Talenti, G.; Thust, S.; Messalli, G.; Hales, P.; et al. Volumetric assessment of tumor size changes in pediatric low-grade gliomas: Feasibility and comparison with linear measurements. Neuroradiology 2018, 60, 427–436. [Google Scholar] [CrossRef]
- Wu, C.; Schwalb, J.M.; Rosenow, J.M.; McKhann, G.M.; Neimat, J.S.; American Society for Stereotactic and Functional Neurosurgeons. The American Society for Stereotactic and Functional Neurosurgery Position Statement on Laser Interstitial Thermal Therapy for the Treatment of Drug-Resistant Epilepsy. Neurosurgery 2022, 90, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Tovar-Spinoza, Z.; Carter, D.; Ferrone, D.; Eksioglu, Y.; Huckins, S. The use of MRI-guided laser-induced thermal ablation for epilepsy. Childs Nerv. Syst. 2013, 29, 2089–2094. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Sharma, M.; Juthani, R.; Meola, A.; Barnett, G.H. Magnetic resonance thermometry and laser interstitial thermal therapy for brain tumors. Neurosurg. Clin. N. Am. 2017, 28, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Kalia, S.K.; Hong, S.H. A Primer on Magnetic Resonance-Guided Laser Interstitial Thermal Therapy for Medically Refractory Epilepsy. J. Korean Neurosurg. Soc. 2019, 62, 353–360. [Google Scholar] [CrossRef]
- Salem, U.; Kumar, V.A.; Madewell, J.E.; Schomer, D.F.; de Almeida Bastos, D.C.; Zinn, P.O.; Weinberg, J.S.; Rao, G.; Prabhu, S.S.; Colen, R.R. Neurosurgical applications of MRI guided laser interstitial thermal therapy (LITT). Cancer Imaging 2019, 19, 65. [Google Scholar] [CrossRef] [Green Version]
- Rieke, V.; Butts Pauly, K. MR thermometry. J. Magn. Reson. Imaging 2008, 27, 376–390. [Google Scholar] [CrossRef]
- Zhu, M.; Sun, Z.; Ng, C.K. Image-guided thermal ablation with MR-based thermometry. Quant. Imaging Med. Surg. 2017, 7, 356–368. [Google Scholar] [CrossRef] [Green Version]
- Patel, N.V.; Mian, M.; Stafford, R.J.; Nahed, B.V.; Willie, J.T.; Gross, R.E.; Danish, S.F. Laser Interstitial Thermal Therapy Technology, Physics of Magnetic Resonance Imaging Thermometry, and Technical Considerations for Proper Catheter Placement during Magnetic Resonance Imaging-Guided Laser Interstitial Thermal Therapy. Neurosurgery 2016, 79 (Suppl. S1), S8–S16. [Google Scholar] [CrossRef] [Green Version]
- Gadgil, N.; Lam, S.; Pan, I.-W.; LoPresti, M.; Wagner, K.; Ali, I.; Wilfong, A.; Curry, D.J. Staged Magnetic Resonance-Guided Laser Interstitial Thermal Therapy for Hypothalamic Hamartoma: Analysis of Ablation Volumes and Morphological Considerations. Neurosurgery 2020, 86, 808–816. [Google Scholar] [CrossRef]
- Parisi, A.J.; Sundararajan, S.H.; Garg, R.; Hargreaves, E.L.; Patel, N.V.; Danish, S.F. Assessment of Optimal Imaging Protocol Sequences after Laser-Induced Thermal Therapy for Intracranial Tumors. Neurosurgery 2018, 83, 471–479. [Google Scholar] [CrossRef]
- Patel, N.V.; Jethwa, P.R.; Barrese, J.C.; Hargreaves, E.L.; Danish, S.F. Volumetric trends associated with MRI-guided laser-induced thermal therapy (LITT) for intracranial tumors. Lasers Surg. Med. 2013, 45, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Munier, S.M.; Desai, A.N.; Patel, N.V.; Danish, S.F. Effects of intraoperative magnetic resonance thermal imaging signal artifact during laser interstitial thermal therapy on thermal damage estimate and postoperative magnetic resonance imaging ablative area concordance. Oper. Neurosurg. 2020, 18, 524–530. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
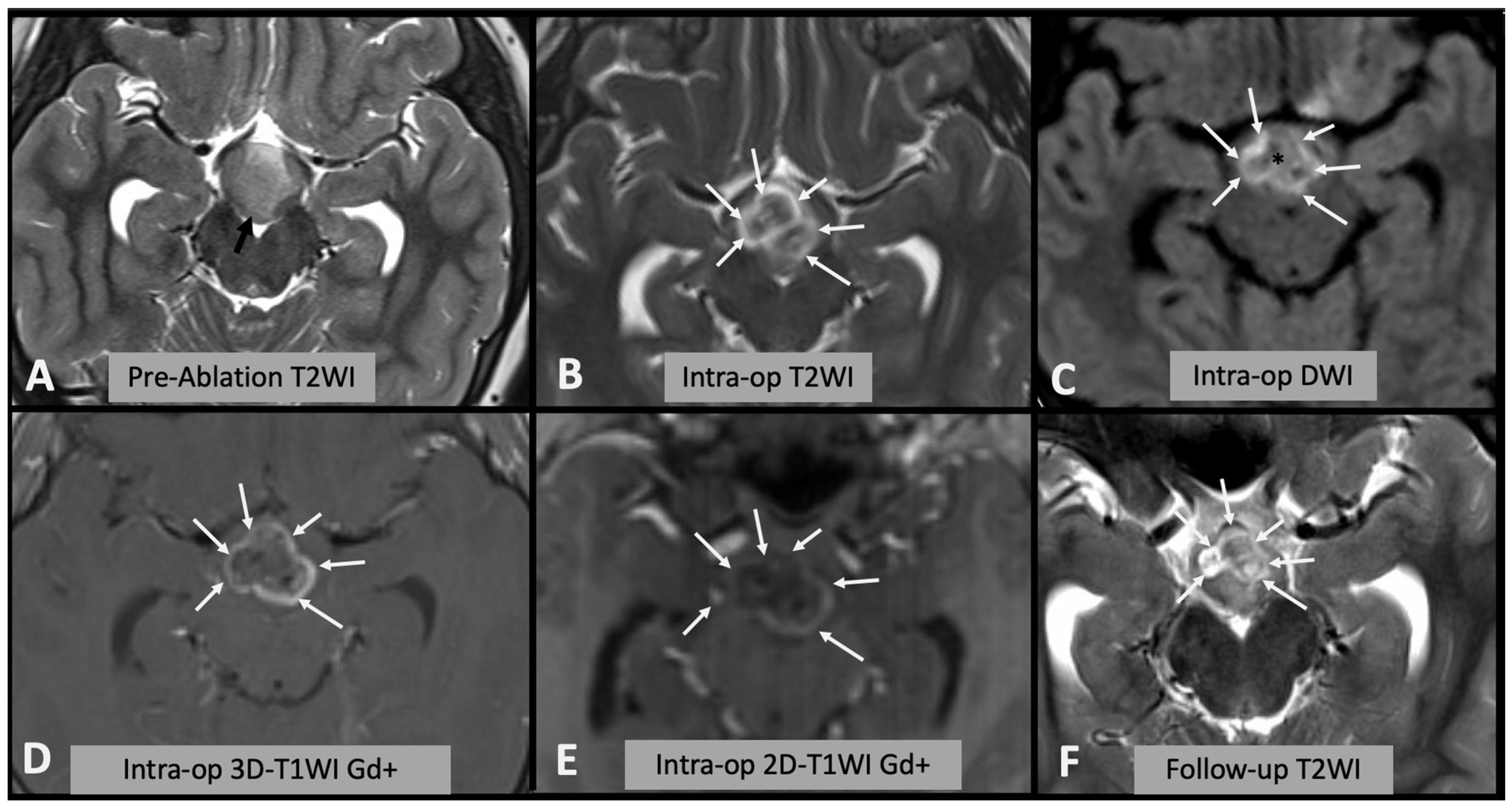
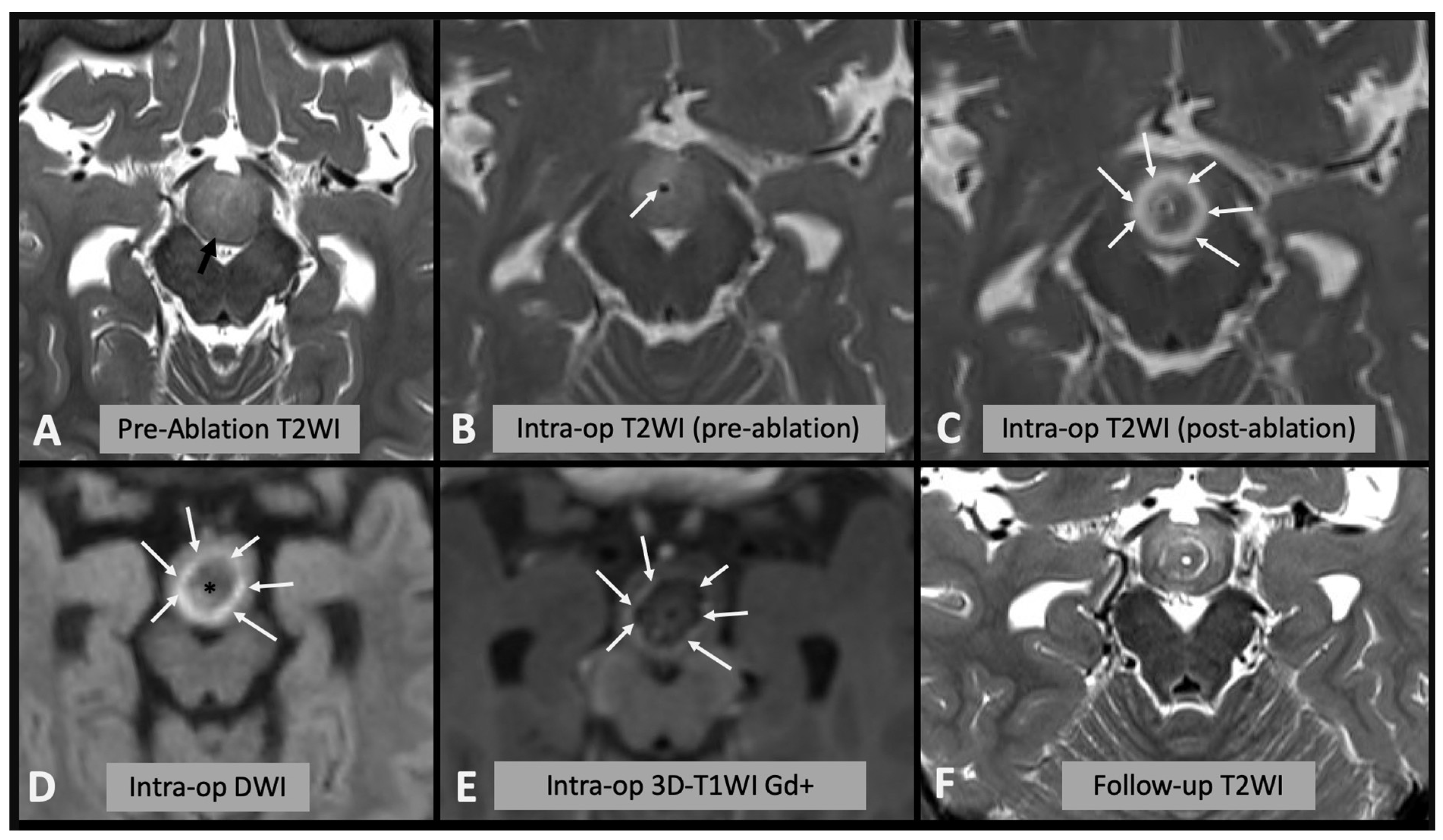
| Pre-operative evaluation and follow-up (essential sequences): |
|
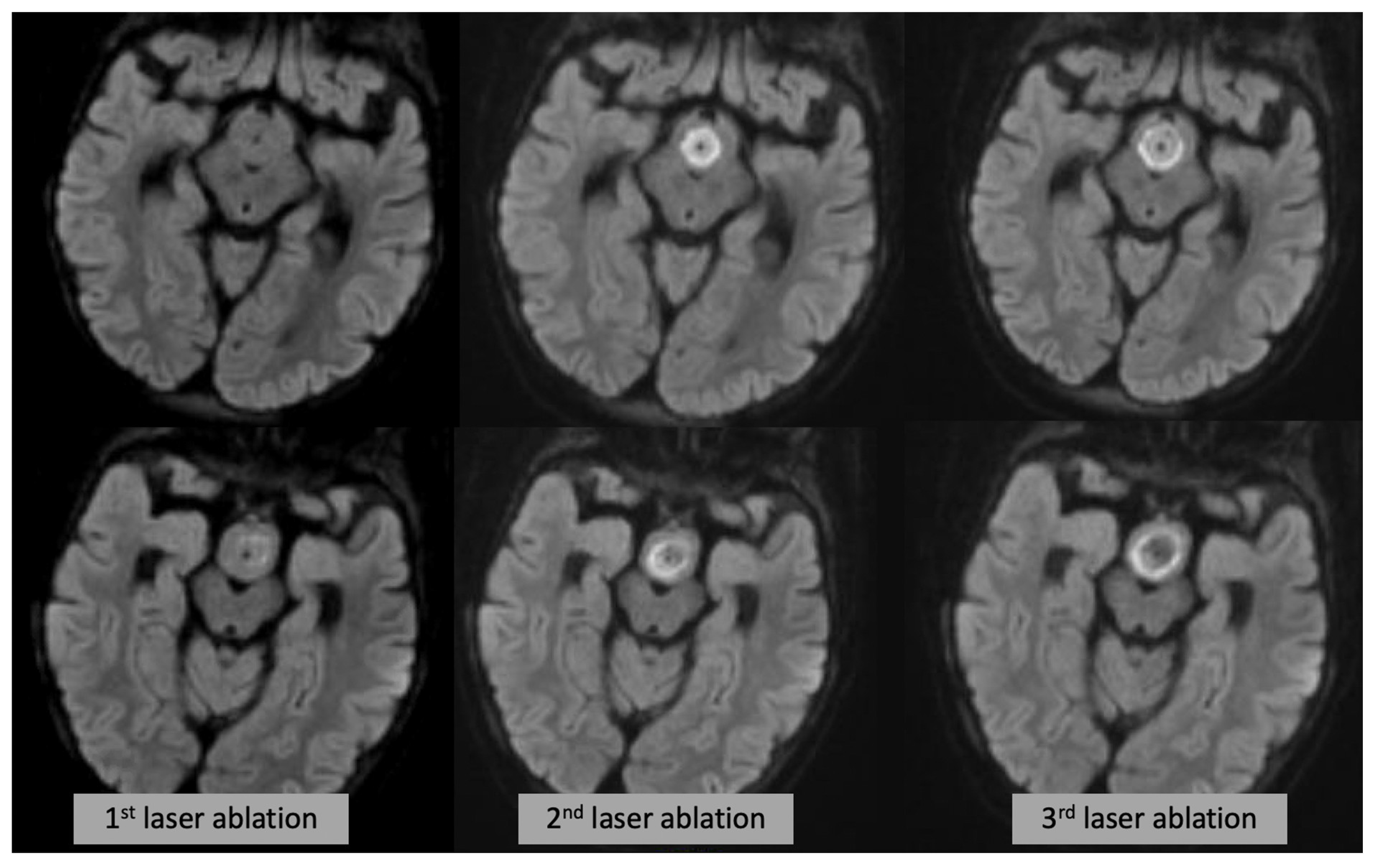
| Intraoperative evaluation |
|
| Immediate Post-operative evaluation |
|
| Follow-up evaluation |
|
| Timing | Sequence Contrast, ROI | Mean Product Diameter (mm2) | Standard Deviation (mm2) |
|---|---|---|---|
| Pre-operative | T2WI HH | 241.4 | 168.5 |
| Intra-operative | DWI (includes edge) | 174.8 | 88.5 |
| Intra-operative | DWI core | 71.8 | 52.8 |
| Intra-operative | T2WI | 211.4 | 109.3 |
| Intra-operative | T1WI post-Gadolinium | 195.9 | 103.3 |
| Post-operative | T2WI encephalomalacia | 59.0 | 39.7 |
| Post-operative | T2WI residual HH | 175.8 | 133.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, S.; Tortora, D.; Picariello, S.; Sudhakar, S.; De Vita, E.; Mankad, K.; Varadkar, S.; Consales, A.; Nobili, L.; Cooper, J.; et al. Intraoperative MRI Assessment of the Tissue Damage during Laser Ablation of Hypothalamic Hamartoma. Diagnostics 2023, 13, 2331. https://doi.org/10.3390/diagnostics13142331
Lombardi S, Tortora D, Picariello S, Sudhakar S, De Vita E, Mankad K, Varadkar S, Consales A, Nobili L, Cooper J, et al. Intraoperative MRI Assessment of the Tissue Damage during Laser Ablation of Hypothalamic Hamartoma. Diagnostics. 2023; 13(14):2331. https://doi.org/10.3390/diagnostics13142331
Chicago/Turabian StyleLombardi, Sophie, Domenico Tortora, Stefania Picariello, Sniya Sudhakar, Enrico De Vita, Kshitij Mankad, Sophia Varadkar, Alessandro Consales, Lino Nobili, Jessica Cooper, and et al. 2023. "Intraoperative MRI Assessment of the Tissue Damage during Laser Ablation of Hypothalamic Hamartoma" Diagnostics 13, no. 14: 2331. https://doi.org/10.3390/diagnostics13142331
APA StyleLombardi, S., Tortora, D., Picariello, S., Sudhakar, S., De Vita, E., Mankad, K., Varadkar, S., Consales, A., Nobili, L., Cooper, J., Tisdall, M. M., & D’Arco, F. (2023). Intraoperative MRI Assessment of the Tissue Damage during Laser Ablation of Hypothalamic Hamartoma. Diagnostics, 13(14), 2331. https://doi.org/10.3390/diagnostics13142331