
Patient-Reported Outcomes of Endovascular Treatment of Post-Thrombotic Syndrome: Ancillary Study of a French Cohort

 , , , , , , ,
on behalf of the French Society of Cardiovascular Imaging (SFICV)add
Show full author list
, , , , , , ,
on behalf of the French Society of Cardiovascular Imaging (SFICV)add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Data Collection
2.4. Villalta and CIVIQ-20 Scores
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Patients and Procedures
3.2. Changes in the Villalta and CIVIQ-20 Scores
3.3. Factors Associated with Changes in the Villalta and CIVIQ-20 Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahnken, A.H.; Thomson, K.; de Haan, M.; O’Sullivan, G.J. CIRSE Standards of Practice Guidelines on Iliocaval Stenting. Cardiovasc. Interv. Radiol. 2014, 37, 889–897. [Google Scholar] [CrossRef] [Green Version]
- Guillen, K.; Falvo, N.; Nakai, M.; Chevallier, O.; Aho-Glélé, S.; Galland, C.; Demaistre, E.; Pescatori, L.; Samson, M.; Audia, S.; et al. Endovascular Stenting for Chronic Femoro-Iliac Venous Obstructive Disease: Clinical Efficacy and Short-Term Outcomes. Diagn. Interv. Imaging 2020, 101, 15–23. [Google Scholar] [CrossRef] [PubMed]
- David, A.; Thony, F.; Del Giudice, C.; Goyault, G.; Loffroy, R.; Guillen, K.; Le Bras, Y.; Marcelin, C.; Monnin-Bares, V.; Heautot, J.-F.; et al. For the Société Française d’Imagerie Cardiovasculaire Diagnostique et Interventionnelle. Short- and Mid-Term Outcomes of Endovascular Stenting for the Treatment of Post-Thrombotic Syndrome Due to Iliofemoral and Caval Occlusive Disease: A Multi-Centric Study from the French Society of Diagnostic and Interventional Cardiovascular Imaging (SFICV). CardioVasc. Interv. Radiol. 2022, 45, 162–171. [Google Scholar] [CrossRef]
- Baldwin, M.J.; Moore, H.M.; Rudarakanchana, N.; Gohel, M.; Davies, A.H. Post-Thrombotic Syndrome: A Clinical Review. J. Thromb. Haemost. 2013, 11, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Mega, J.L.; Berger, J.S. Duration of Anticoagulation for Venous Thromboembolic Events. Circulation 2014, 130, 2343–2348. [Google Scholar] [CrossRef] [Green Version]
- Roumen-Klappe, E.M.; den Heijer, M.; Janssen, M.C.H.; van der Vleuten, C.; Thien, T.; Wollersheim, H. The Post-Thrombotic Syndrome: Incidence and Prognostic Value of Non-Invasive Venous Examinations in a Six-Year Follow-up Study. Thromb. Haemost. 2005, 94, 825–830. [Google Scholar] [CrossRef]
- Vedantham, S. Valvular Dysfunction and Venous Obstruction in the Post-Thrombotic Syndrome. Thromb. Res. 2009, 123 (Suppl. S4), S62–S65. [Google Scholar] [CrossRef]
- Kahn, S.R. Natural History of Postthrombotic Disease: Transition from Acute to Chronic Disease. J. Vasc. Surg. 2010, 52, 62S–64S. [Google Scholar] [CrossRef]
- O’Donnell, T.F.J.; Passman, M.A.; Marston, W.A.; Ennis, W.J.; Dalsing, M.; Kistner, R.L.; Lurie, F.; Henke, P.K.; Gloviczki, M.L.; Eklöf, B.G.; et al. Management of Venous Leg Ulcers: Clinical Practice Guidelines of the Society for Vascular Surgery® and the American Venous Forum. J. Vasc. Surg. 2014, 60, 3S–59S. [Google Scholar] [CrossRef] [Green Version]
- Khanna, A.K.; Singh, S. Postthrombotic Syndrome: Surgical Possibilities. Thrombosis 2012, 2012, 520604. [Google Scholar] [CrossRef]
- Williams, Z.F.; Dillavou, E.D. A Systematic Review of Venous Stents for Iliac and Venacaval Occlusive Disease. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 8, 145–153. [Google Scholar] [CrossRef]
- Kahn, S.R.; Comerota, A.J.; Cushman, M.; Evans, N.S.; Ginsberg, J.S.; Goldenberg, N.A.; Gupta, D.K.; Prandoni, P.; Vedantham, S.; Walsh, M.E.; et al. The Postthrombotic Syndrome: Evidence-Based Prevention, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Circulation 2014, 130, 1636–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarici, I.S.; Yanar, F.; Agcaoglu, O.; Ucar, A.; Poyanli, A.; Cakir, S.; Aksoy, S.M.; Kurtoglu, M. Our Early Experience with Iliofemoral Vein Stenting in Patients with Post-Thrombotic Syndrome. Phlebology 2014, 29, 298–303. [Google Scholar] [CrossRef]
- Yin, M.; Shi, H.; Ye, K.; Lu, X.; Li, W.; Huang, X.; Lu, M.; Jiang, M. Clinical Assessment of Endovascular Stenting Compared with Compression Therapy Alone in Post-Thrombotic Patients with Iliofemoral Obstruction. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Launois, R.; Mansilha, A.; Lozano, F. Linguistic Validation of the 20 Item-Chronic Venous Disease Quality-of-Life Questionnaire (CIVIQ-20). Phlebology 2014, 29, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Launois, R.; Mansilha, A.; Jantet, G. International Psychometric Validation of the Chronic Venous Disease Quality of Life Questionnaire (CIVIQ-20). Eur. J. Vasc. Endovasc. Surg. 2010, 40, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strijkers, R.H.W.; Wittens, C.H.A.; Kahn, S.R. Villalta Scale: Goals and Limitations. Phlebology 2012, 27 (Suppl. S1), 130–135. [Google Scholar] [CrossRef] [PubMed]
- Menez, C.; Rodiere, M.; Ghelfi, J.; Seinturier, C.; Martinelli, T.; Imbert, B.; Perolat, R.; Bouzat, P.; Blaise, S.; Carpentier, P.; et al. Endovascular Treatment of Post-Thrombotic Venous Ilio-Femoral Occlusions: Prognostic Value of Venous Lesions Caudal to the Common Femoral Vein. Cardiovasc. Interv. Radiol. 2019, 42, 1117–1127. [Google Scholar] [CrossRef]
- Strijkers, R.; Arnoldussen, C.; Wittens, C. Validation of the LET Classification. Phlebology 2015, 30, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Dumantepe, M.; Aydin, S.; Ökten, M.; Karabulut, H. Endophlebectomy of the Common Femoral Vein and Endovascular Iliac Vein Recanalization for Chronic Iliofemoral Venous Occlusion. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 572–582. [Google Scholar] [CrossRef]
- Ruihua, W.; Xin, W.; Guang, L.; Kaichuang, Y.; Jinbao, Q.; Minyi, Y.; Weimin, L.; Xiaobing, L.; Xintian, H.; Min, L.; et al. Technique and Clinical Outcomes of Combined Stent Placement for Postthrombotic Chronic Total Occlusions of the Iliofemoral Veins. J. Vasc. Interv. Radiol. 2017, 28, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Sogomonian, R.; Gonzalez-Lengua, C.A.; Hanumanthu, B.K.; Tesalona, M.A.; Mohajer, P.; Liu, K.; Taghipour, N.; Gowda, R.M.; Misra, D. Early and Mid-Term Outcomes of Femoro-Ilio-Caval Vein Stent Implantation. J. Invasive Cardiol. 2021, 33, E497–E505. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.M.; Oliveira-Pinto, J.; Duarte-Gamas, L.; Coelho, A.; Mansilha, A. Mid-Term Patency of Iliac Venous Stenting for Post-Thrombotic Syndrome. Int. Angiol. 2021, 40, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Ye, K.; Lu, X.; Jiang, M.; Yang, X.; Li, W.; Huang, Y.; Huang, X.; Lu, M. Technical Details and Clinical Outcomes of Transpopliteal Venous Stent Placement for Postthrombotic Chronic Total Occlusion of the Iliofemoral Vein. J. Vasc. Interv. Radiol. 2014, 25, 925–932. [Google Scholar] [CrossRef]
- Qiu, P.; Zha, B.; Xu, A.; Wang, W.; Zhan, Y.; Zhu, X.; Yuan, X. Systematic Review and Meta-Analysis of Iliofemoral Stenting for Post-Thrombotic Syndrome. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Neglén, P.; Hollis, K.C.; Olivier, J.; Raju, S. Stenting of the Venous Outflow in Chronic Venous Disease: Long-Term Stent-Related Outcome, Clinical, and Hemodynamic Result. J. Vasc. Surg. 2007, 46, 979–990. [Google Scholar] [CrossRef] [Green Version]
- Sang, H.; Li, X.; Qian, A.; Meng, Q. Outcome of Endovascular Treatment in Postthrombotic Syndrome. Ann. Vasc. Surg. 2014, 28, 1493–1500. [Google Scholar] [CrossRef]
- Kurklinsky, A.K.; Bjarnason, H.; Friese, J.L.; Wysokinski, W.E.; McBane, R.D.; Misselt, A.; Moller, S.M.; Gloviczki, P. Outcomes of Venoplasty with Stent Placement for Chronic Thrombosis of the Iliac and Femoral Veins: Single-Center Experience. J. Vasc. Interv. Radiol. 2012, 23, 1009–1015. [Google Scholar] [CrossRef] [Green Version]
- de Wolf, M.A.F.; Jalaie, H.; van Laanen, J.H.H.; Kurstjens, R.L.M.; Mensinck, M.J.S.; de Geus, M.J.; Gombert, A.; de Graaf, R.; Wittens, C.H.A. Endophlebectomy of the Common Femoral Vein and Arteriovenous Fistula Creation as Adjuncts to Venous Stenting for Post-Thrombotic Syndrome. Br. J. Surg. 2017, 104, 718–725. [Google Scholar] [CrossRef]
- Piao, L.; Barbati, M.E.; Shekarchian, S.; Jacobs, M.J.; Razavi, M.; Rass, K.; Jalaie, H. Comparison of Endovascular Strategy versus Hybrid Procedure in Treatment of Chronic Venous Obstructions Involving the Confluence of Common Femoral Vein. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 10, 334–341. [Google Scholar] [CrossRef]
- Hartung, O.; Loundou, A.D.; Barthelemy, P.; Arnoux, D.; Boufi, M.; Alimi, Y.S. Endovascular Management of Chronic Disabling Ilio-Caval Obstructive Lesions: Long-Term Results. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gwozdz, A.M.; Doyle, A.J.; Hunt, B.J.; Tincknell, L.G.; Jackson, N.; Saha, P.; Breen, K.A.; Smith, A.; Cohen, A.; Black, S.A. Effect of Thrombophilia on Clinical Outcomes of Chronic Post-Thrombotic Patients after Iliofemoral Stenting with Nitinol Venous Stents. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 9, 888–894. [Google Scholar] [CrossRef] [PubMed]
- De Maeseneer, M.G.; Kakkos, S.K.; Aherne, T.; Baekgaard, N.; Black, S.; Blomgren, L.; Giannoukas, A.; Gohel, M.; De Graaf, R.; Hamel-Desnos, C.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 184–267. [Google Scholar] [CrossRef] [PubMed]
- Szapáry, L.; Tornyos, D.; Kupó, P.; Lukács, R.; El Alaoui El Abdallaoui, O.; Komócsi, A. Combination of Antiplatelet and Anticoagulant Therapy, Component Network Meta-Analysis of Randomized Controlled Trials. Front. Cardiovasc. Med. 2022, 9, 1036609. [Google Scholar] [CrossRef]
- Chan, S.M.; Lee, A.; Roy, B.; Chaar, C.I.O. Diagnostic and Technical Challenges in the Care of a Complex Patient with Post-Thrombotic Syndrome. Vasc. Endovascular. Surg. 2021, 55, 515–518. [Google Scholar] [CrossRef]
- Azirar, S.; Appelen, D.; Prins, M.H.; Neumann, M.H.; de Feiter, A.N.; Kolbach, D.N. Compression Therapy for Treating Post-Thrombotic Syndrome. Cochrane Database Syst. Rev. 2019, 9, CD004177. [Google Scholar] [CrossRef]
- Tang, T.Y.; Lim, M.H.; Damodharan, K.; Yap, C.J.; Lee, S.Q.; Yap, H.Y.; Chong, T.T.; Tan, J.W. Use of the VENOVOTM and Sinus ObliquusTM Venous Stents in the Treatment of Non-Thrombotic or Post-Thrombotic Iliac Vein Lesions-Short-Term Results from a Multi-Centre Asian Cohort. Phlebology 2021, 36, 70–78. [Google Scholar] [CrossRef]
- Baccellieri, D.; Ardita, V.; Apruzzi, L.; Carta, N.; Bilman, V.; Melissano, G.; Chiesa, R. Endovascular Treatment of Iliofemoral Vein Obstruction below the Inguinal Ligament Using a New-Dedicated Stent: Early Experience from a Single Center. Int. Angiol. 2021, 40, 187–195. [Google Scholar] [CrossRef]
- Divakaran, S.; Meissner, M.H.; Kohi, M.P.; Chen, S.; Song, Y.; Hawkins, B.M.; Rosenfield, K.; Parikh, S.A.; Secemsky, E.A. Utilization of and Outcomes Associated with Intravascular Ultrasound during Deep Venous Stent Placement among Medicare Beneficiaries. J. Vasc. Interv. Radiol. 2022, 33, 1476–1484. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years), median [IQR] | 43 [32.3–56.5] |
| Females, n (%) | 324 (60.1) |
| Time from DVT to stenting (months), median [IQR] | 3.1 [1.3–11.9] |
| DVT recurrence, n (%) | |
| One | 96 (17.8) |
| Two | 30 (5.6) |
| Three or more | 25 (4.6) |
| DVT sequelae grade, n (%) | |
| 0 | 198 (36.7) |
| 1 | 124 (23.0) |
| 2 | 171 (31.7) |
| 3 | 46 (8.5) |
| Side of stenting, n (%) | |
| Left | 379 (70.3) |
| Right | 78 (14.5) |
| Both | 82 (15.2) |
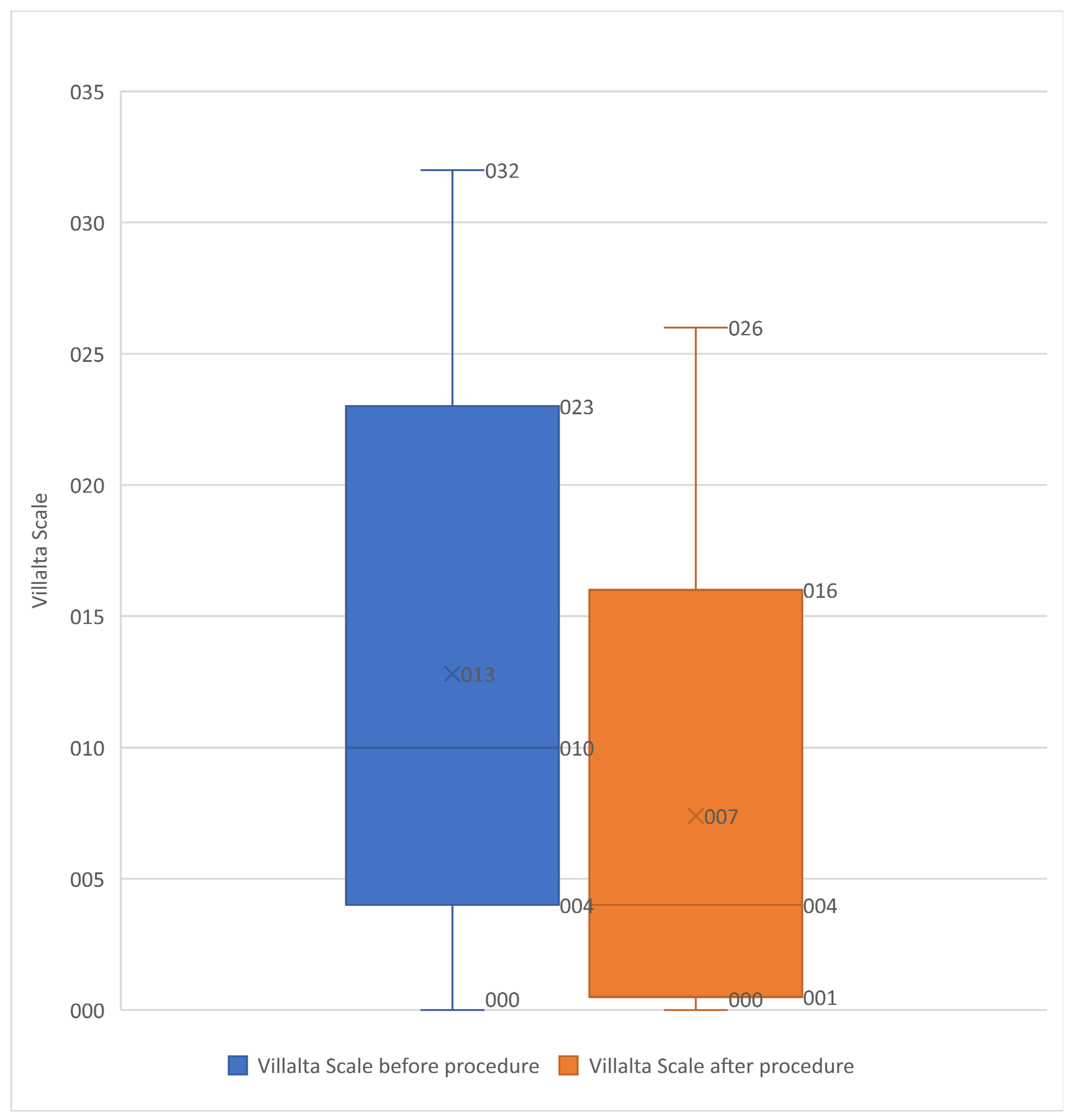
| Baseline Villalta score, median [IQR] | 12 [8–14] |
| Baseline Villalta score category, n (%) | |
| No PTS | 31 (5.8) |
| Mild PTS | 181 (33.6) |
| Moderate PTS | 193 (35.8) |
| Severe PTS | 134 (24.9) |
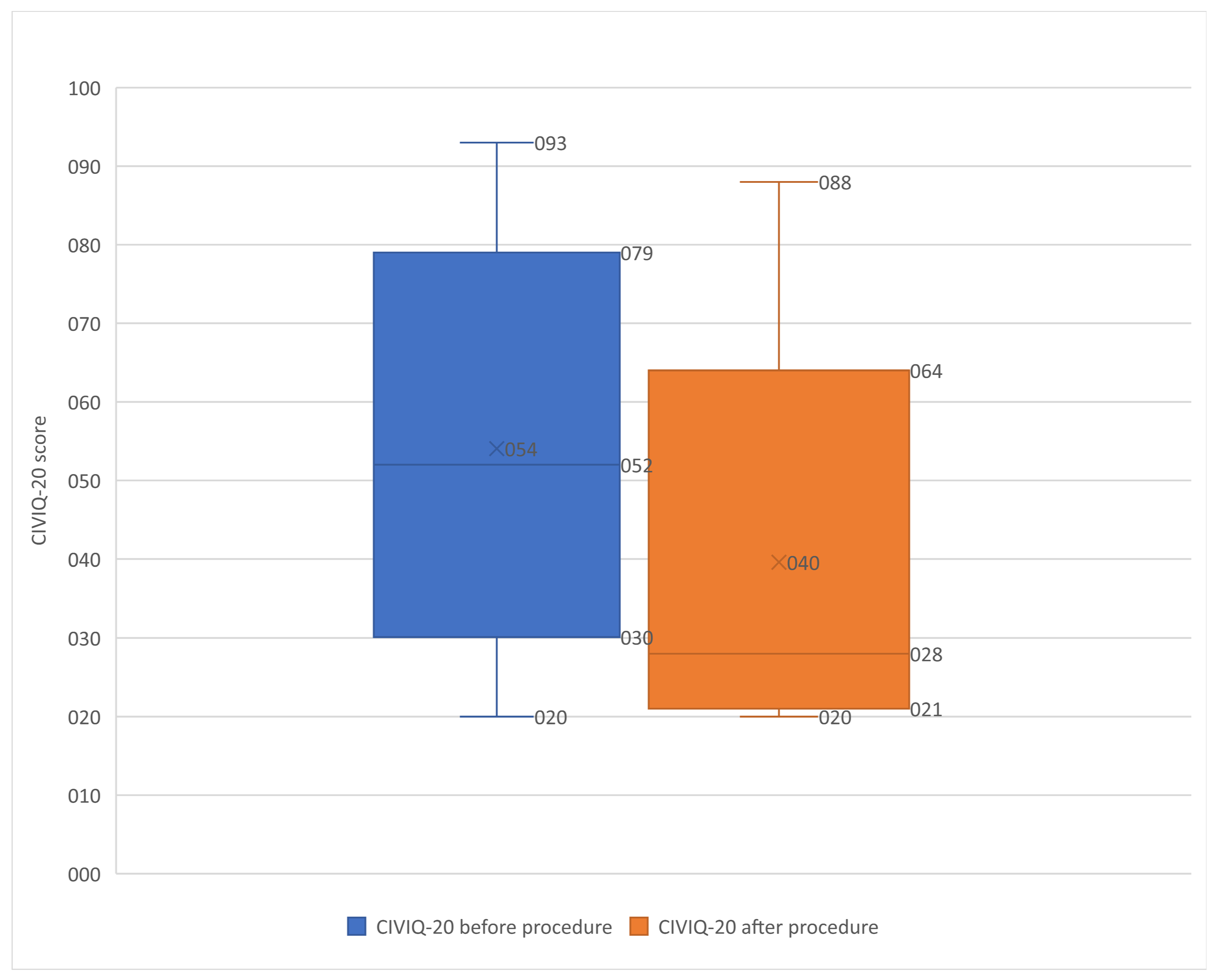
| Baseline CIVIQ-20 score, median [IQR] | 52 [40–65] |
| Stented Segments (LET Classification), n (%) | |
| One | 11 (2.0) |
| Two | 21 (3.9) |
| Three | 96 (17.8) |
| Four | 215 (39.9) |
| Five | 159 (29.5) |
| Six | 36 (6.7) |
| Seven | 1 (0.2) |
| Distal stenting zone | |
| Inferior vena cava | 11 (2.0) |
| Common iliac vein | 100 (18.6) |
| External iliac vein | 366 (67.9) |
| Common femoral vein | 52 (9.7) |
| Immediate technical success, n (%) | 530 (98.3) |
| Post-procedural Villalta score, median [|IQR] | 3 [1,2,3,4,5,6] |
| Post-procedural Villalta score category, n (%) | |
| No PTS | 335 (62.2) |
| Mild PTS | 139 (25.8) |
| Moderate PTS | 40 (7.4) |
| Severe PTS | 25 (4.6) |
| Post-procedural CIVIQ-20 score, median [IQR] | 28 [22–40] |
| p > |t| | 95% Confidence Interval | ||
|---|---|---|---|
| DVT sequelae grade | |||
| 1 | 0.982 | −1.025 | 1.048 |
| 2 | 0.244 | −0.449 | 1.761 |
| 3 | 0.029 | 0.177 | 3.21 |
| DVT recurrence | |||
| One | 0.397 | −0.669 | 1.6851 |
| Two | 0.496 | −1.295 | 2.670 |
| Three | 0.487 | −1.929 | 4.047 |
| Four | 0.078 | −0.307 | 5.794 |
| Five | 0.764 | −3.394 | 2.493 |
| Six or seven | 0.000 | −11.248 | −4.527 |
| Stented segments, n | |||
| One | 0.164 | −6.201 | 1.052 |
| Two | 0.377 | −4.922 | 1.866 |
| Three | 0.356 | −4.802 | 1.728 |
| Four | 0.653 | −4.093 | 2.568 |
| Five | 0.241 | −5.738 | 1.446 |
| Six or seven recurrences | 0.007 | 1.290 | 8.316 |
| Sex | 0.135 | −1.486 | 0.201 |
| Age | 0.18 | −0.047 | 0.009 |
| Median time from DVT to stenting | 0.001 | −0.108 | −0.027 |
| p > |t| | 95% Confidence Interval | ||
|---|---|---|---|
| Thrombosis recurrence, n | |||
| One | 0.001 | −11.107 | −2.874 |
| Two | 0.924 | −7.2136 | 7.947 |
| Three | 0.367 | −15.726 | 5.835 |
| Four | 0.536 | −14.716 | 28.224 |
| Five | 0.649 | −4.887 | 3.050 |
| Six or seven | 0.891 | −9.382 | 10.793 |
| Stented segments, n | |||
| One | 0.042 | 0.743 | 42.574 |
| Two | 0.229 | −7.208 | 30.044 |
| Three | 0.180 | −6.107 | 32.438 |
| Four | 0.332 | −9.837 | 29.053 |
| Five | 0.219 | −7.751 | 33.669 |
| Six | 0.513 | −13.911 | 27.790 |
| Stenting distality a | |||
| Inferior vena cava | 0.173 | −29.269 | 5.279 |
| Common iliac vein | 0.516 | −21.529 | 10.842 |
| External iliac vein | 0.431 | −23.652 | 10.112 |
| Age | 0.189 | −0.183 | 0.037 |
| Bilateral thrombosis | 0.002 | 4.0137 | 17.475 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillen, K.; Thony, F.; Del Giudice, C.; Goyault, G.; David, A.; Douane, F.; Le Bras, Y.; Monnin-Bares, V.; Heautot, J.-F.; Rousseau, H.; et al. Patient-Reported Outcomes of Endovascular Treatment of Post-Thrombotic Syndrome: Ancillary Study of a French Cohort. Diagnostics 2023, 13, 2357. https://doi.org/10.3390/diagnostics13142357
Guillen K, Thony F, Del Giudice C, Goyault G, David A, Douane F, Le Bras Y, Monnin-Bares V, Heautot J-F, Rousseau H, et al. Patient-Reported Outcomes of Endovascular Treatment of Post-Thrombotic Syndrome: Ancillary Study of a French Cohort. Diagnostics. 2023; 13(14):2357. https://doi.org/10.3390/diagnostics13142357
Chicago/Turabian StyleGuillen, Kévin, Frédéric Thony, Costantino Del Giudice, Gilles Goyault, Arthur David, Frédéric Douane, Yann Le Bras, Valérie Monnin-Bares, Jean-François Heautot, Hervé Rousseau, and et al. 2023. "Patient-Reported Outcomes of Endovascular Treatment of Post-Thrombotic Syndrome: Ancillary Study of a French Cohort" Diagnostics 13, no. 14: 2357. https://doi.org/10.3390/diagnostics13142357
APA StyleGuillen, K., Thony, F., Del Giudice, C., Goyault, G., David, A., Douane, F., Le Bras, Y., Monnin-Bares, V., Heautot, J. -F., Rousseau, H., Martinelli, T., Thouveny, F., Barral, P. -A., Le Pennec, V., Chabrot, P., Rogopoulos, A., Aho-Glélé, L. S., Sapoval, M., Rodière, M., ... Loffroy, R., on behalf of the French Society of Cardiovascular Imaging (SFICV). (2023). Patient-Reported Outcomes of Endovascular Treatment of Post-Thrombotic Syndrome: Ancillary Study of a French Cohort. Diagnostics, 13(14), 2357. https://doi.org/10.3390/diagnostics13142357