
The Predictive Value of Risk Factors and Prognostic Scores in Hospitalized COVID-19 Patients


 ,
,  , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.1.1. Demographic, Anthropometric Data, Laboratory and Clinically Significant Parameters
2.1.2. Prognostic Scores
2.1.3. COVID-19 Treatment
2.1.4. Statistical Analysis
2.1.5. Ethics
3. Results
3.1. Baseline Characteristics
3.2. Radiographic Findings and Clinical Parameters of the Study Group according to Outcome
3.3. Laboratory Parameters of the Study Group according to Outcome
3.4. Glasgow Coma Score, Pulmonary and Hemodynamic Parameters
3.5. Early Warning Scores (EWS) if the Study Group according to Outcome
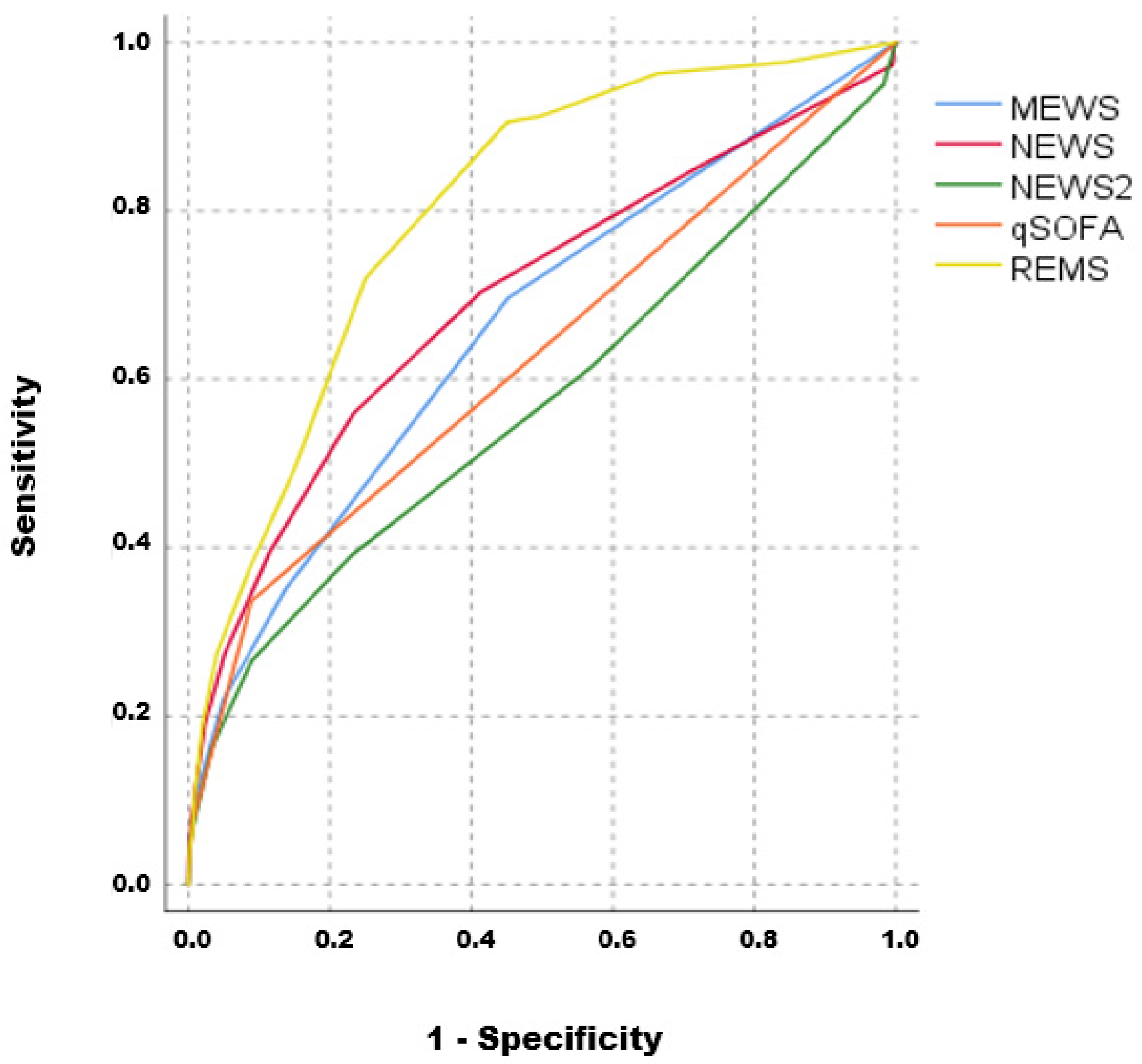
3.6. Diagnostic Performance of Early Warning Scores in the Study Group
3.7. Multivariate Logistic Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knight, S.R.; Harrison, E.M. Risk stratification of patients with COVID-19 in the community. Lancet Digit. Health 2022, 4, e628–e629. [Google Scholar] [CrossRef]
- Hu, H.; Yao, N.; Qiu, Y. Predictive Value of 5 Early Warning Scores for Critical COVID-19 Patients. Disaster Med. Public Health Prep. 2020, 16, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.S.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; Capela, C.; Pedrosa, J.; Gil Castro, A.; Silvestre, R. Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef] [PubMed]
- Al Sulaiman, K.; Aljuhani, O.; Badreldin, H.A.; Korayem, G.B.; Alenazi, A.A.; Alharbi, A.H.; Alghamdi, A.; Alhubaishi, A.; Altebainawi, A.F.; Bosaeed, M.; et al. The clinical outcomes of COVID-19 critically ill patients co-infected with other respiratory viruses: A multicenter, cohort study. BMC Infect Dis. 2023, 23, 75. [Google Scholar]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef]
- Martín-Rodríguez, F.; Martín-Conty, J.L.; Sanz-García, A.; Rodríguez, V.C.; Rabbione, G.O.; Ruíz, I.C.; Ramos, J.R.O.; Portillo, E.C.; Polonio-López, B.; Gambarra, R.E.d.S.; et al. Early Warning Scores in Patients with Suspected COVID-19 Infection in Emergency Departments. J. Pers. Med. 2021, 11, 170. [Google Scholar] [CrossRef]
- Tsai, W.; Chen, C.; Jo, S.-Y.; Hsiao, C.-H.; Chien, D.-K.; Chang, W.-H.; Chen, T.-H. Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan. Medicina 2023, 59, 464. [Google Scholar] [CrossRef]
- Veldhuis, L.; Ridderikhof, M.L.; Schinkel, M.; van den Bergh, J.; Beudel, M.; Dormans, T.; Douma, R.; Oever, N.G.v.D.; de Haan, L.; Koopman, K.; et al. Early warning scores to assess the probability of critical illness in patients with COVID-19. Emerg. Med. J. 2021, 38, 901–905. [Google Scholar] [CrossRef]
- Innocenti, F.; De Paris, A.; Lagomarsini, A.; Pelagatti, L.; Casalini, L.; Gianno, A.; Montuori, M.; Bernardini, P.; Caldi, F.; Tassinari, I.; et al. Stratification of patients admitted for SARS-CoV2 infection: Prognostic scores in the first and second wave of the pandemic. Intern. Emerg. Med. 2022, 17, 2093–2101. [Google Scholar] [CrossRef]
- Lombardi, Y.; Azoyan, L.; Szychowiak, P.; Bellamine, A.; Lemaitre, G.; Bernaux, M.; Daniel, C.; Leblanc, J.; Riller, Q.; Steichen, O.; et al. External validation of prognostic scores for COVID-19: A multicenter cohort study of patients hospitalized in Greater Paris University Hospitals. Intensive Care Med. 2021, 47, 1426–1439. [Google Scholar] [CrossRef]
- Gerry, S.; Bonnici, T.; Birks, J.; Kirtley, S.; Virdee, P.S.; Watkinson, P.J.; Collins, G.S. Early warning scores for detecting deterioration in adult hospital patients: Systematic review and critical appraisal of methodology. BMJ 2020, 369, m1501. [Google Scholar] [CrossRef]
- Fu, L.-H.; Schwartz, J.; Moy, A.; Knaplund, C.; Kang, M.-J.; Schnock, K.O.; Garcia, J.P.; Jia, H.; Dykes, P.C.; Cato, K.; et al. Development and validation of early warning score system: A systematic literature review. J. Biomed. Inform. 2020, 105, 103410. [Google Scholar] [CrossRef] [PubMed]
- Mitsunaga, T.; Hasegawa, I.; Uzura, M.; Okuno, K.; Otani, K.; Ohtaki, Y.; Sekine, A.; Takeda, S. Comparison of the National Early Warning Score (NEWS) and the Modified Early Warning Score (MEWS) for predicting admission and in-hospital mortality in elderly patients in the pre-hospital setting and in the emergency department. PeerJ 2019, 7, e6947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, W.R.; Radhakrishnan, M.; Macko, J.; Hinch, B.T.; Altorok, N.; Assaly, R. Initial MEWS score to predict ICU admission or transfer of hospitalized patients with COVID-19: A retrospective study. J. Infect. 2020, 82, 282–327. [Google Scholar] [CrossRef]
- Thorén, A.; Joelsson-Alm, E.; Spångfors, M.; Rawshani, A.; Kahan, T.; Engdahl, J.; Jonsson, M.; Djärv, T. The predictive power of the National Early Warning Score (NEWS) 2, as compared to NEWS, among patients assessed by a Rapid response team: A prospective multi-centre trial. Resusc. Plus 2022, 9, 100191. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, I.; Smith, G.B.; Prytherch, D.; Meredith, P.; Price, C.; Chauhan, A.; Portsmouth Academic Consortium for Investigating COVID-19 (PACIFIC-19). The performance of the National Early Warning Score and National Early Warning Score 2 in hospitalised patients infected by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Resuscitation 2021, 159, 150–157. [Google Scholar] [CrossRef]
- Smith, G.; Redfern, O.; Pimentel, M.; Gerry, S.; Collins, G.; Malycha, J.; Prytherch, D.; Schmidt, P.; Watkinson, P. The National Early Warning Score 2 (NEWS2). Clin. Med. 2019, 19, 260. [Google Scholar] [CrossRef]
- Williams, B. Evaluation of the utility of NEWS2 during the COVID-19 pandemic. Clin. Med. 2022, 22, 539–543. [Google Scholar]
- Carr, E.; Bendayan, R.; Bean, D.; Stammers, M.; Wang, W.; Zhang, H.; Searle, T.; Kraljevic, Z.; Shek, A.; Phan, H.T.T.; et al. Evaluation and improvement of the National Early Warning Score (NEWS2) for COVID-19: A multi-hospital study. BMC Med. 2021, 19, 1–16. [Google Scholar] [CrossRef]
- Baker, K.F.; Hanrath, A.T.; van der Loeff, I.S.; Kay, L.J.; Back, J.; Duncan, C.J. National Early Warning Score 2 (NEWS2) to identify inpatient COVID-19 deterioration: A retrospective analysis. Clin. Med. 2021, 21, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Bidari, A.; Talachian, E. Rapid Emergency Medicine Score (REMS) As a Predictor of Early Mortality in the Setting of Emergency Department. Iran J. Med. Sci. 2022, 47, 81–82. [Google Scholar]
- Haruna, J.; Tatsumi, H.; Kazuma, S.; Kuroda, H.; Goto, Y.; Aisaka, W.; Terada, H.; Sonoda, T.; Masuda, Y. Comparison of the National Early Warning Scores and Rapid Emergency Medicine Scores with the APACHE II Scores as a Prediction of Mortality in Patients with Medical Emergency Team Activation: A Single-centre Retrospective Cohort Study. J. Crit. Care Med. 2021, 7, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Imhoff, B.F.; Thompson, N.J.; Hastings, M.A.; Nazir, N.; Moncure, M.; Cannon, C.M. Rapid Emergency Medicine Score (REMS) in the trauma population: A retrospective study. BMJ Open 2014, 4, e004738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahdati, S.S.; Jalali, M.; Parsay, S.; Ala, A. Rapid Emergency Medicine Score as a Predictive Value for 30-day Outcome of Nonsurgical Patients Referred to the Emergency Department. Indian J. Crit. Care Med. 2020, 24, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Bourn, S.S.; Crowe, R.P.; Fernandez, A.R.; Matt, S.E.; Brown, A.L.; Hawthorn, A.B.; Myers, J.B. Initial prehospital Rapid Emergency Medicine Score (REMS) to predict outcomes for COVID-19 patients. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12483. [Google Scholar] [CrossRef]
- Ruangsomboon, O.; Phanprasert, N.; Jirathanavichai, S.; Puchongmart, C.; Boonmee, P.; Thirawattanasoot, N.; Dorongthom, T.; Praphruetkit, N.; Monsomboon, A. The utility of the Rapid Emergency Medicine Score (REMS) compared with three other early warning scores in predicting in-hospital mortality among COVID-19 patients in the emergency department: A multicenter validation study. BMC Emerg. Med. 2023, 23, 1–10. [Google Scholar] [CrossRef]
- Alencar, J.; Gómez, L.M.G.; Cortez, A.L.; de Souza, H.P.; Levin, A.S.; Salomão, M.C. Performance of NEWS, qSOFA, and SIRS Scores for Assessing Mortality, Early Bacterial Infection, and Admission to ICU in COVID-19 Patients in the Emergency Department. Front. Med. 2022, 9, 779516. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef]
- Ys, A.; Ravi, K. Comparison of Quick Sequential Organ Failure Assessment (Qsofa) and National Early Warning Score (News) in Covid-19 Patients and its Correlation with the Outcome. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar] [PubMed]
- Zdravkovic, M.; Popadic, V.; Klasnja, S.; Pavlovic, V.; Aleksic, A.; Milenkovic, M.; Crnokrak, B.; Balint, B.; Todorovic-Balint, M.; Mrda, D.; et al. Development and Validation of a Multivariable Predictive Model for Mortality of COVID-19 Patients Demanding High Oxygen Flow at Admission to ICU: AIDA Score. Oxidative Med. Cell. Longev. 2021, 2021, 6654388. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Outcome | p | |
|---|---|---|---|
| Survival (n = 3311) | Exitus Letalis (n = 299) | ||
| Gender, n (%) | |||
| Male | 2075 (62.7) | 169 (56.5) | 0.035 |
| Female | 1234 (37.3) | 130 (43.5) | |
| Age, mean ± sd | 57.9 ± 14.9 | 73.4 ± 11.7 | <0.001 |
| Comorbidities, n (%) | 1888 (57.1) | 230 (76.9) | <0.001 |
| Hypertension | 1564 (47.3) | 177 (59.2) | <0.001 |
| Diabetes mellitus | 559 (16.9) | 95 (31.8) | <0.001 |
| Obesities | 188 (5.7) | 21 (7.0) | 0.334 |
| COPD | 89 (2.7) | 17 (5.7) | 0.003 |
| Asthma | 121 (3.7) | 10 (3.3) | 0.782 |
| Coronary disease | 276 (8.3) | 62 (20.7) | <0.001 |
| Cardiomyopathy | 148 (4.5) | 51 (17.1) | <0.001 |
| Malignancy | 149 (4.5) | 42 (14.0) | <0.001 |
| Variable | Outcome | p | |
|---|---|---|---|
| Survival (n = 3311) | Exitus Letalis (n = 299) | ||
| Radiographic findings, n (%) | |||
| Normal/Unilateral pneumonia | 875 (26.8) | 56 (19.3) | 0.005 |
| Bilateral pneumonia | 2388 (73.2) | 234 (80.7) | |
| CT score, median (25–75th percentile) | 10 (7–14) | 17 (11–22) | <0.001 |
| Admission to ICU, yes, n (%) | 166 (5.0) | 197 (65.9) | <0.001 |
| Need for oxygen support, n (%) | |||
| O2 mask/HFNC | 3235 (97.9) | 264 (88.6) | <0.001 |
| NIV/IMV | 70 (2.1) | 34 (11.4) | |
| Hospital-acquired pneumonia, yes, n (%) | 53 (1.6) | 68 (22.7) | <0.001 |
| Healthcare-associated pneumonia | 34 (70.8) | 21 (31.8) | <0.001 |
| Ventilator-associated pneumonia | 14 (29.2) | 45 (68.2) | |
| Bacterial superinfection, yes, n (%) | 111 (3.4) | 121 (40.5) | <0.001 |
| ARDS, yes, n (%) | 31 (1.1) | 204 (70.3) | <0.001 |
| Corticosteroid therapy, yes, n (%) | 2372 (71.7) | 250 (83.6) | <0.001 |
| Variable | Outcome | p | |
|---|---|---|---|
| Median (25–75th Percentile) | Survival (n = 3311) | Exitus Letalis (n = 299) | |
| Erythrocytes | 4.68 (4.33–5.03) | 4.37 (3.86–4.82) | <0.001 |
| Hemoglobin | 138 (127–148) | 128.5 (111–140) | <0.001 |
| Hematocrit | 0.41 (0.38–0.44) | 0.39 (0.34–0.42) | <0.001 |
| Leukocytes | 5.38 (4.52–7.71) | 7.57 (5.38–11.64) | <0.001 |
| Neutrophils | 3.65 (2.27–5.35) | 5.71 (3.23–9.66) | <0.001 |
| Lymphocytes | 1.22 (0.85–1.86) | 0.83 (0.57–1.28) | <0.001 |
| Neutrophils/Lymphocytes ratio | 3.11 (1.68–5.33) | 6.57 (3.39–13.5) | <0.001 |
| Thrombocytes | 199 (158–255) | 189 (136–266) | 0.021 |
| Il-6 | 23.9 (10.2–52.01) | 81.1 (38.35–173.35) | <0.001 |
| INR | 1.04 (0.97–1.13) | 1.13 (1.02–1.33) | <0.001 |
| aPTT | 24.2 (22.6–26.1) | 25.6 (23.1–29.1) | <0.001 |
| Fibrinogen | 4.0 (3.4–5.0) | 4.2 (3.4–5.3) | 0.041 |
| D-dimer | 440 (253–820) | 1125 (520–3022) | <0.001 |
| PCT | 0.08 (0.05–0.15) | 0.27 (0.15–0.76) | <0.001 |
| CRP | 34.7 (10.4–78.2) | 85.7 (43.1–168.4) | <0.001 |
| Urea | 5.4 (4.3–7.1) | 9.3 (6.3–14.6) | <0.001 |
| Creatinine | 88 (75–105) | 108 (83–147) | <0.001 |
| Glycose | 6.3 (5.6–7.4) | 7.6 (6.3–10.1) | <0.001 |
| AST | 29 (22–42) | 38 (27–57) | <0.001 |
| ALT | 27 (18–43) | 24 (17–42) | 0.091 |
| Bilirubin | 8.4 (6.1–11.8) | 9.6 (6.7–15.3) | <0.001 |
| LDH | 454 (358–601) | 650 (461–875) | <0.001 |
| Ferritin | 440 (243.5–754) | 689 (371–1194) | <0.001 |
| Variable | Outcome | p | |
|---|---|---|---|
| Survival (n = 3311) | Exitus Letalis (n = 299) | ||
| Glasgow Coma Score, n (%) | |||
| =15 | 3231 (97.6) | 234 (79.1) | <0.001 |
| <15 | 79 (2.4) | 62 (20.9) | |
| FiO2 at admission, n (%) | |||
| =21 | 3260 (98.5) | 286 (95.7) | <0.001 |
| >21 | 51 (1.5) | 13 (4.3) | |
| Number of respirations, median (25–75th percentile) | 14 (14–15) | 16 (14–18) | <0.001 |
| SpO2, mean ± sd | 95.2 ± 4.3 | 89.6 ± 9.7 | <0.001 |
| Systolic blood pressure (mm/Hg), mean ± sd | 127.1 ± 16.8 | 125.3 ± 20.6 | 0.089 |
| Diastolic blood pressure (mm/Hg), mean ± sd | 79.4 ± 10.8 | 76.0 ± 12.7 | <0.001 |
| MAP | 95.2 ± 11.6 | 92.4 ± 14.1 | <0.001 |
| Heart rate (/min), mean ± sd | 82.9 ± 13.9 | 87.3 ± 19.4 | <0.001 |
| Variable | Outcome | p | |
|---|---|---|---|
| Survival (n = 3311) | Exitus Letalis (n = 299) | ||
| MEWS | |||
| 0 | 1813 (54.8) | 90 (30.2) | <0.001 |
| >0 | 1497 (45.2) | 208 (69.8) | |
| NEWS, median (25–75th percentile) | 3 (2–4) | 5 (3–7) | <0.001 |
| NEWS2, median (25–75th percentile) | 3 (2–3) | 3 (2–5) | <0.001 |
| REMS | |||
| ≤5 | 2480 (74.9) | 83 (27.9) | <0.001 |
| >5 | 830 (25.1) | 215 (72.1) | |
| qSOFA | |||
| 0 | 3014 (91.1) | 197 (66.1) | <0.001 |
| >0 | 296 (8.9) | 101 (33.9) | |
| Variable | Outcome | |||
|---|---|---|---|---|
| Sensitivity | PPV | Specificity | NPV | |
| MEWS | 69.8 | 12.2 | 54.8 | 95.3 |
| NEWS | 70.6 | 13.4 | 58.6 | 95.7 |
| NEWS2 | 61.9 | 8.9 | 42.8 | 92.6 |
| REMS | 72.1 | 20.6 | 74.9 | 96.8 |
| qSOFA | 33.9 | 25.4 | 91.1 | 93.9 |
| Variable | Multivariate | ||
|---|---|---|---|
| p | OR | 95% CI for OR | |
| Age | <0.001 | 1.056 | 1.032–1.081 |
| CT Score | <0.001 | 1.135 | 1.096–1.174 |
| Urea | <0.001 | 1.082 | 1.038–1.128 |
| Bacterial superinfection | <0.001 | 13.554 | 8.741–21.017 |
| REMS | 0.002 | 1.183 | 1.063–1.316 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brajkovic, M.; Vukcevic, M.; Nikolic, S.; Dukic, M.; Brankovic, M.; Sekulic, A.; Popadic, V.; Stjepanovic, M.; Radojevic, A.; Markovic-Denic, L.; et al. The Predictive Value of Risk Factors and Prognostic Scores in Hospitalized COVID-19 Patients. Diagnostics 2023, 13, 2653. https://doi.org/10.3390/diagnostics13162653
Brajkovic M, Vukcevic M, Nikolic S, Dukic M, Brankovic M, Sekulic A, Popadic V, Stjepanovic M, Radojevic A, Markovic-Denic L, et al. The Predictive Value of Risk Factors and Prognostic Scores in Hospitalized COVID-19 Patients. Diagnostics. 2023; 13(16):2653. https://doi.org/10.3390/diagnostics13162653
Chicago/Turabian StyleBrajkovic, Milica, Miodrag Vukcevic, Sofija Nikolic, Marija Dukic, Marija Brankovic, Ana Sekulic, Viseslav Popadic, Mihailo Stjepanovic, Aleksandra Radojevic, Ljiljana Markovic-Denic, and et al. 2023. "The Predictive Value of Risk Factors and Prognostic Scores in Hospitalized COVID-19 Patients" Diagnostics 13, no. 16: 2653. https://doi.org/10.3390/diagnostics13162653
APA StyleBrajkovic, M., Vukcevic, M., Nikolic, S., Dukic, M., Brankovic, M., Sekulic, A., Popadic, V., Stjepanovic, M., Radojevic, A., Markovic-Denic, L., Rajovic, N., Milic, N., Tanasilovic, S., Todorovic, Z., & Zdravkovic, M. (2023). The Predictive Value of Risk Factors and Prognostic Scores in Hospitalized COVID-19 Patients. Diagnostics, 13(16), 2653. https://doi.org/10.3390/diagnostics13162653