

Inflammatory Status Assessment by Machine Learning Techniques to Predict Outcomes in Patients with Symptomatic Aortic Stenosis Treated by Transcatheter Aortic Valve Replacement
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Machine Learning
2.2. Statistical Analysis
3. Results
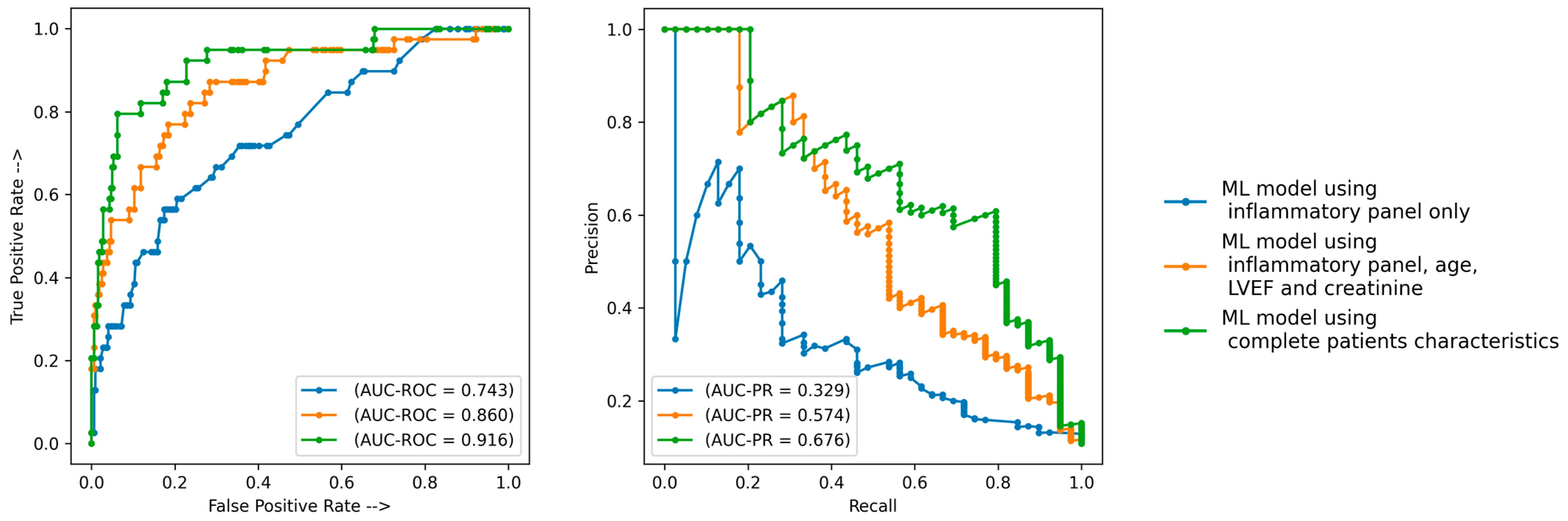
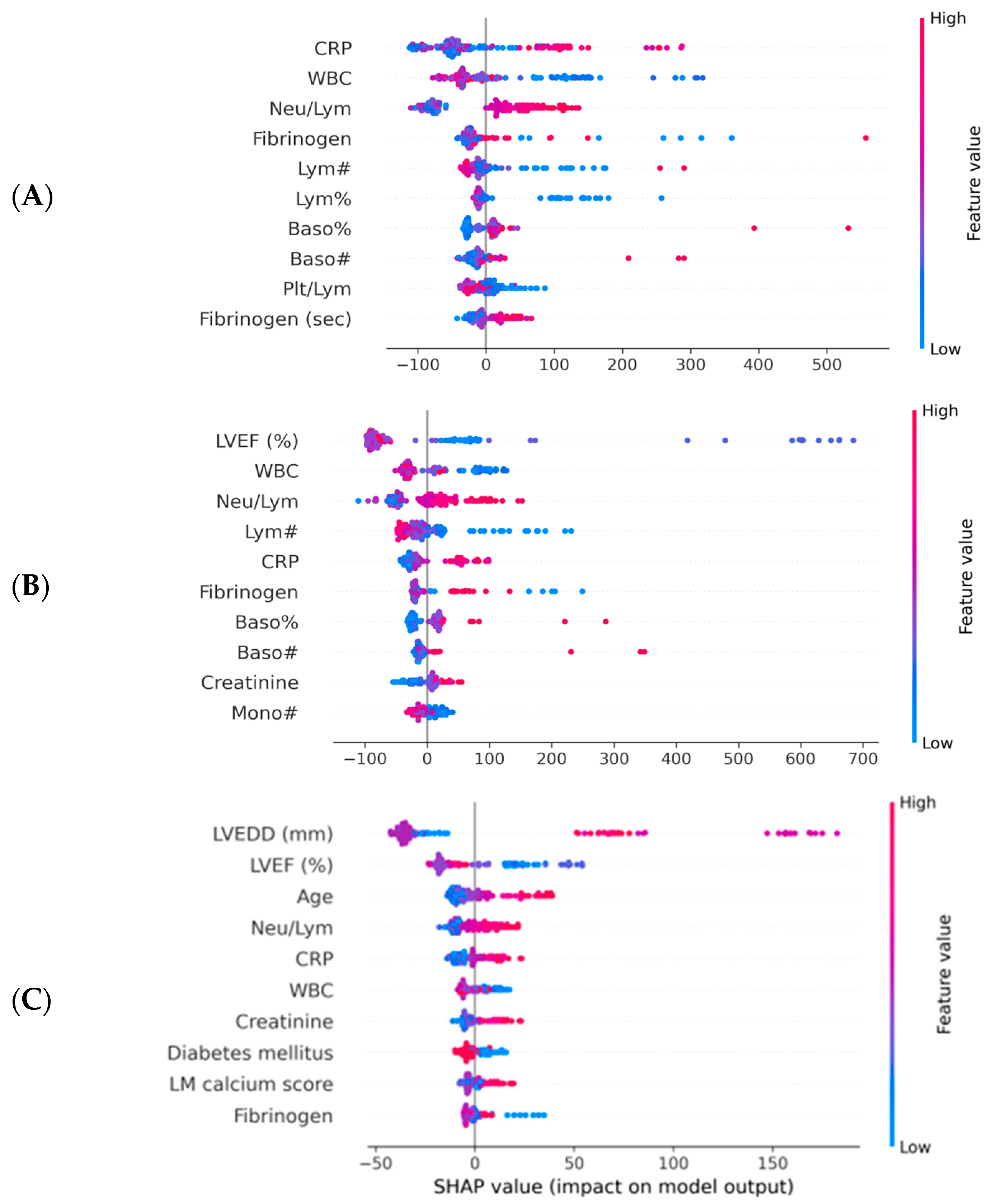
Machine Learning Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet Lond Engl. 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Ross, J.; Braunwald, E. Aortic stenosis. Circulation 1968, 38, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M. Valvular aortic stenosis: Disease severity and timing of intervention. J. Am. Coll. Cardiol. 2006, 47, 2141–2151. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Bärwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.-L.; Vermeer, F.; Boersma, E.; et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef]
- Webb, J.G.; Wood, D.A. Current Status of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2012, 60, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Gurvitch, R.; Wood, D.A.; Tay, E.L.; Leipsic, J.; Ye, J.; Lichtenstein, S.V.; Thompson, C.R.; Carere, R.G.; Wijesinghe, N.; Nietlispach, F.; et al. Transcatheter Aortic Valve Implantation. Circulation 2010, 122, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Ussia, G.P.; Barbanti, M.; Petronio, A.S.; Tarantini, G.; Ettori, F.; Colombo, A.; Violini, R.; Ramondo, A.; Santoro, G.; Klugmann, S.; et al. Transcatheter aortic valve implantation: 3-year outcomes of self-expanding CoreValve prosthesis. Eur. Heart J. 2012, 33, 969–976. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Tribouilloy, C.; Rusinaru, D.; Maréchaux, S.; Castel, A.-L.; Debry, N.; Maizel, J.; Mentaverri, R.; Kamel, S.; Slama, M.; Lévy, F. Low-Gradient, Low-Flow Severe Aortic Stenosis With Preserved Left Ventricular Ejection Fraction. J. Am. Coll. Cardiol. 2015, 65, 55–66. [Google Scholar] [CrossRef]
- Breiman, L. Classification and Regression Trees; Routledge: New York, NY, USA, 1984; ISBN 978-1-315-13947-0. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J. Big-ECG: Cardiographic Predictive Cyber-Physical System for Stroke Management. IEEE Access 2021, 9, 123146–123164. [Google Scholar] [CrossRef]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Ghahramani, Z. Probabilistic machine learning and artificial intelligence. Nature 2015, 521, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Savage, N. Breaking into the black box of artificial intelligence. Nature 2022. [Google Scholar] [CrossRef] [PubMed]
- Călburean, P.-A.; Grebenișan, P.; Nistor, I.-A.; Pal, K.; Vacariu, V.; Drincal, R.-K.; Țepes, O.; Bârlea, I.; Șuș, I.; Somkereki, C.; et al. Prediction of 3-year all-cause and cardiovascular cause mortality in a prospective percutaneous coronary intervention registry: Machine learning model outperforms conventional clinical risk scores. Atherosclerosis 2022, 350, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, S.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. arXiv 2017, arXiv:1705.07874. [Google Scholar]
- Saito, T.; Rehmsmeier, M. The Precision-Recall Plot Is More Informative than the ROC Plot When Evaluating Binary Classifiers on Imbalanced Datasets. PLoS ONE 2015, 10, e0118432. [Google Scholar] [CrossRef]
- Călburean, P.-A.; Osorio, T.G.; Sorgente, A.; Almorad, A.; Pannone, L.; Monaco, C.; Miraglia, V.; Al Housari, M.; Mojica, J.; Bala, G. High vagal tone predicts pulmonary vein reconnection after cryoballoon ablation for paroxysmal atrial fibrillation. Pacing Clin. Electrophysiol. 2021, 44, 2075–2083. [Google Scholar] [CrossRef]
- Călburean, P.-A.; Pannone, L.; Sorgente, A.; Gauthey, A.; Monaco, C.; Strazdas, A.; Almorad, A.; Bisignani, A.; Bala, G.; Ramak, R.; et al. Heart rate variability and microvolt T wave alternans changes during ajmaline test may predict prognosis in Brugada syndrome. Clin. Auton. Res. 2023, 33, 51–62. [Google Scholar] [CrossRef]
- Sinning, J.-M.; Wollert, K.C.; Sedaghat, A.; Widera, C.; Radermacher, M.-C.; Descoups, C.; Hammerstingl, C.; Weber, M.; Stundl, A.; Ghanem, A.; et al. Risk scores and biomarkers for the prediction of 1-year outcome after transcatheter aortic valve replacement. Am. Heart J. 2015, 170, 821–829. [Google Scholar] [CrossRef]
- Sexton, T.R.; Wallace, E.L.; Chen, A.; Charnigo, R.J.; Reda, H.K.; Ziada, K.M.; Gurley, J.C.; Smyth, S.S. Thromboinflammatory response and predictors of outcomes in patients undergoing transcatheter aortic valve replacement. J. Thromb. Thrombolysis 2016, 41, 384–393. [Google Scholar] [CrossRef]
- Uhle, F.; Castrup, C.; Necaev, A.-M.; Grieshaber, P.; Lichtenstern, C.; Weigand, M.A.; Böning, A. Inflammation and Its Consequences After Surgical Versus Transcatheter Aortic Valve Replacement. Artif. Organs 2018, 42, E1–E12. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, P.; Mehran, R.; Collet, J.-P.; Claessen, B.E.; ten Berg, J.; Dangas, G.D. Antithrombotic Therapy After Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2019, 12, e007411. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Deeb, G.M.; Reardon, M.J.; Chetcuti, S.; Patel, H.J.; Grossman, P.M.; Yakubov, S.J.; Kleiman, N.S.; Coselli, J.S.; Gleason, T.G.; Lee, J.S.; et al. 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2565–2574. [Google Scholar] [CrossRef]
- Sannino, A.; Gargiulo, G.; Schiattarella, G.G.; Brevetti, L.; Perrino, C.; Stabile, E.; Losi, M.A.; Toscano, E.; Giugliano, G.; Scudiero, F.; et al. Increased mortality after transcatheter aortic valve implantation (TAVI) in patients with severe aortic stenosis and low ejection fraction: A meta-analysis of 6898 patients. Int. J. Cardiol. 2014, 176, 32–39. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Entire Population (n = 338) | Alive at 3 Years (n = 282) | Deceased at 3 Years (n = 56) | p |
|---|---|---|---|---|
| Age (years) | 76 (71–80) | 76 (71–80) | 78 ± 6 | 0.01 |
| BMI (kg/m2) | 29.01 ± 4.48 | 29.28 ± 4.52 | 26.02 ± 2.65 | 0.08 |
| Male sex | 204 (60.3%) | 171 (60.6%) | 33 (58.9%) | 0.88 |
| LVEF (%) | 50 (40–60) | 50 (40–60) | 40 (35–55) | 0.001 |
| DCM | 33 (9.76%) | 22 (7.8%) | 11 (19.64%) | 0.01 |
| CAD | 202 (59.76%) | 165 (58.51%) | 37 (66.07%) | 0.37 |
| Previous MI | 21 (6.21%) | 16 (5.67%) | 5 (8.93%) | 0.36 |
| Previous PCI | 183 (54.1%) | 151 (53.5%) | 32 (57.1%) | 0.66 |
| Previous CABG | 12 (3.55%) | 10 (3.55%) | 2 (3.57%) | 0.99 |
| Hypertension | 270 (79.88%) | 229 (81.21%) | 41 (73.21%) | 0.20 |
| Diabetes mellitus | 104 (30.77%) | 79 (28.01%) | 25 (44.64%) | 0.01 |
| Atrial fibrillation | 99 (29.29%) | 79 (28.01%) | 20 (35.71%) | 0.26 |
| Stroke | 19 (5.62%) | 15 (5.32%) | 4 (7.14%) | 0.26 |
| COPD | 22 (6.51%) | 19 (6.74%) | 3 (5.36%) | 0.99 |
| Parameter | Entire Population (n = 338) | Alive at 3 Years (n = 282) | Deceased at 3 Years (n = 56) | p |
|---|---|---|---|---|
| LVEDD (mm) | 50 (45–55.75) | 50 (45–55) | 54.05 ± 7.41 | 0.03 |
| RVEDD (mm) | 28 (24.75–32) | 28 (24–31.25) | 28.98 ± 6.22 | 0.45 |
| PWT (mm) | 13 (11–14) | 13 (11–13.25) | 12 (11.75–14) | 0.23 |
| IVST (mm) | 14 (12–16) | 14 (12–16) | 14 (12–15) | 0.65 |
| Aortic annulus (mm) | 21 (19–22) | 21 (19–22) | 21 (20–22) | 0.49 |
| Ascending aorta (mm) | 33 (27–36) | 33 (21–36) | 33 (30.75–36.25) | 0.98 |
| LVOT diameter (mm) | 20 (18–21) | 20 (18–21) | 20.65 ± 1.93 | 0.07 |
| LA diameter (mm) | 43 (37.75–47) | 43 (36.75–47) | 45 (39–49.25) | 0.06 |
| RA diameter (mm) | 20 (15–30.75) | 20 (15–29) | 27.6 ± 16.31 | 0.23 |
| Maximum gradient (mmHg) | 71 (52.5–81) | 72 (54.5–81.5) | 66 (43.25–75.25) | 0.42 |
| PHT (ms) | 300 (50–461) | 270 (51.5–459) | 335 (48.25–472.5) | 0.44 |
| Parameter | Entire Population (n = 338) | Alive at 3 Years (n = 282) | Deceased at 3 Years (n = 56) | p |
|---|---|---|---|---|
| Annulus area (mm2) | 510 (448.5–577.5) | 509 (439–573) | 573.67 ± 88.64 | 0.63 |
| Annulus perimeter (mm) | 82.36 ± 9.14 | 82 ± 9.27 | 86.37 ± 6.83 | 0.15 |
| LVOT perimeter (mm) | 81.2 (73.8–88.9) | 80.6 (73.8–88.5) | 85.23 ± 5.61 | 0.95 |
| LVOT area (mm) | 493 (414.5–591.25) | 486.5 (405.75–585.75) | 551.5 ± 69.39 | 0.29 |
| Sinotubular diameter (mm) | 28.79 ± 3.5 | 28.1 (26.9–30.7) | 29.92 ± 4.57 | 0.78 |
| LCA height (mm) | 13.6 (12.4–16) | 13.6 (12.7–16) | 13.45 ± 2.89 | 0.81 |
| RCA height (mm) | 15.5 (13.25–18.4) | 15.5 (13.4–18.2) | 16.95 ± 4.55 | 0.44 |
| LM calcium score | 0 (0–111) | 55 (0–72) | 161 ± 61 | 0.02 |
| LAD calcium score | 246 (93–655) | 239 (106–654) | 403 ± 324 | 0.80 |
| CX calcium score | 13 (0–254) | 10 (0–271) | 136 ± 116 | 0.19 |
| RCA calcium score | 157 (24–444) | 155 (21–441) | 123 ± 44 | 0.17 |
| Total coronary calcium score | 689 (212–1336) | 644 (213–1281) | 983 ± 748 | 0.13 |
| Parameter | Entire Population (n = 338) | Alive at 3 Years (n = 282) | Deceased at 3 Years (n = 56) | p |
|---|---|---|---|---|
| WBC count (×103/µL) | 6.86 (5.94–8.36) | 6.91 (6.06–8.35) | 6.33 (5.44–8.46) | 0.22 |
| Neu (×103/µL) | 4.91 (4.08–5.96) | 4.91 (4.11–5.95) | 4.87 (3.9–6.53) | 0.89 |
| Lym (×103/µL) | 1.43 (1.14–1.87) | 1.45 (1.15–1.89) | 1.24 (0.81–1.59) | 0.006 |
| Neu (%) | 66.3 (61.17–71.03) | 66.28 (61–70.8) | 68.03 (63.56–72.84) | 0.98 |
| Lym (%) | 20 (16.3–24.01) | 20.14 (16.42–24.17) | 17.84 (12.75–22.03) | 0.03 |
| Neu/Lym ratio | 3.43 (2.61–4.51) | 3.41 (2.57–4.46) | 3.99 (2.99–5.88) | 0.04 |
| Plt/Lym ratio | 115.1 (91.4–150.1) | 113.9 (90.8–147.6) | 140.3 ± 66.4 | 0.12 |
| CRP (mg/dL) | 0.59 (0.16–1.39) | 0.55 (0.15–1.33) | 1.18 (0.52–2.39) | 0.006 |
| Fibrinogen (mg/dL) | 371.9 (322.5–432.7) | 371.9 (322.5–427.9) | 392.6 ± 104.5 | 0.20 |
| ESR (s) | 27.7 (15–45) | 28.3 (15–45) | 28.0 ± 23.1 | 0.97 |
| Parameter | Entire Population (n = 338) | Alive at 3 Years (n = 282) | Deceased at 3 Years (n = 56) | p |
|---|---|---|---|---|
| Creatinine (mg/dL) | 1.05 (0.88–1.31) | 1.04 (0.88–1.29) | 1.27 (0.98–1.53) | 0.001 |
| Total serum proteins (mg/dL) | 6.6 (6.16–6.95) | 6.57 ± 0.6 | 6.22 (5.98–6.91) | 0.06 |
| Serum albumin (mg/dL) | 3.89 ± 0.44 | 3.93 ± 0.4 | 3.55 ± 0.54 | 0.001 |
| Total serum CK (U/L) | 80.67 (55.38–124.06) | 81.5 (57.5–122.5) | 78.4 (49.33–140) | 0.73 |
| Serum CK-MB (U/L) | 19.42 (15.31–24.38) | 19.42 (16–24) | 19.25 (12.38–30.38) | 0.81 |
| Total bilirubin (mg/dL) | 0.68 (0.51–0.88) | 0.67 (0.51–0.87) | 0.81 (0.56–1.23) | 0.06 |
| Cholesterol (mg/dL) | 147 (125–180.75) | 149.8 (127–181.12) | 145.77 ± 41.66 | 0.10 |
| LDL-cholesterol (mg/dL) | 88.75 (72–115.25) | 89.75 (72–115.62) | 89.21 ± 30.57 | 0.35 |
| HDL-cholesterol (mg/dL) | 36.5 (30.83–44) | 36.65 (31–44) | 37.19 ± 12.14 | 0.43 |
| Triglyceride (mg/dL) | 98 (74.5–130.5) | 99 (74.5–131) | 92 (77.35–121.25) | 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stan, A.; Călburean, P.-A.; Drinkal, R.-K.; Harpa, M.; Elkahlout, A.; Nicolae, V.C.; Tomșa, F.; Hadadi, L.; Brînzaniuc, K.; Suciu, H.; et al. Inflammatory Status Assessment by Machine Learning Techniques to Predict Outcomes in Patients with Symptomatic Aortic Stenosis Treated by Transcatheter Aortic Valve Replacement. Diagnostics 2023, 13, 2907. https://doi.org/10.3390/diagnostics13182907
Stan A, Călburean P-A, Drinkal R-K, Harpa M, Elkahlout A, Nicolae VC, Tomșa F, Hadadi L, Brînzaniuc K, Suciu H, et al. Inflammatory Status Assessment by Machine Learning Techniques to Predict Outcomes in Patients with Symptomatic Aortic Stenosis Treated by Transcatheter Aortic Valve Replacement. Diagnostics. 2023; 13(18):2907. https://doi.org/10.3390/diagnostics13182907
Chicago/Turabian StyleStan, Alexandru, Paul-Adrian Călburean, Reka-Katalin Drinkal, Marius Harpa, Ayman Elkahlout, Viorel Constantin Nicolae, Flavius Tomșa, Laszlo Hadadi, Klara Brînzaniuc, Horațiu Suciu, and et al. 2023. "Inflammatory Status Assessment by Machine Learning Techniques to Predict Outcomes in Patients with Symptomatic Aortic Stenosis Treated by Transcatheter Aortic Valve Replacement" Diagnostics 13, no. 18: 2907. https://doi.org/10.3390/diagnostics13182907
APA StyleStan, A., Călburean, P. -A., Drinkal, R. -K., Harpa, M., Elkahlout, A., Nicolae, V. C., Tomșa, F., Hadadi, L., Brînzaniuc, K., Suciu, H., & Mărușteri, M. (2023). Inflammatory Status Assessment by Machine Learning Techniques to Predict Outcomes in Patients with Symptomatic Aortic Stenosis Treated by Transcatheter Aortic Valve Replacement. Diagnostics, 13(18), 2907. https://doi.org/10.3390/diagnostics13182907