
Two Approaches to Triple Antithrombotic Therapy in Patients with Acute Coronary Syndrome and Non-Valvular Atrial Fibrillation Treated with Percutaneous Coronary Intervention: Which Is More Efficient and Safer?


Abstract
:1. Introduction
2. Methods
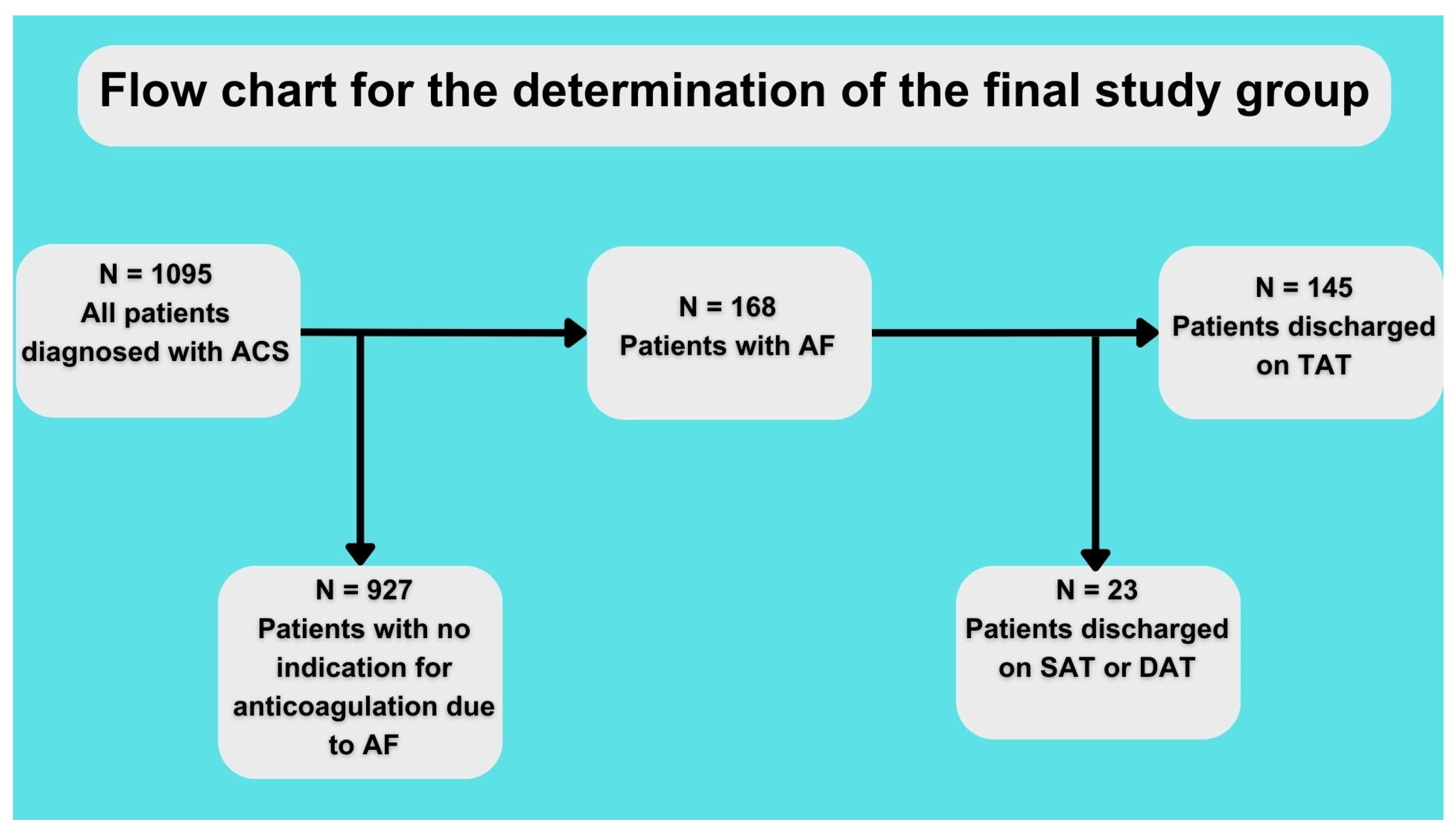
2.1. Subset
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bangalore, S.; Toklu, B.; Patel, N.; Feit, F.; Stone, G.W. Newer-Generation Ultrathin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation 2018, 138, 2216–2226. [Google Scholar] [CrossRef] [PubMed]
- Abadie, B.Q.; Cannon, C.P.; Cavender, M.A. Novel Oral Anticoagulants Following Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2020, 13, e008465. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Antman, E.M.; Gibson, C.M.; Montalescot, G.; Riesmeyer, J.; Weerakkody, G.; Winters, K.J.; Warmke, J.W.; McCabe, C.H.; Braunwald, E. Evaluation of prasugrel compared with clopidogrel in patients with acute coronary syndromes: Design and rationale for the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet InhibitioN with prasugrel Thrombolysis In Myocardial Infarction 38 (TRITON-TIMI 38). Am. Heart J. 2006, 152, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.; Wolf, P.; Benjamin, E.; Levy, D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: Population-based estimates. Am. J. Cardiol. 1998, 82, 2N–9N. [Google Scholar] [CrossRef] [PubMed]
- Kralev, S.; Schneider, K.; Lang, S.; Süselbeck, T.; Borggrefe, M. Incidence and Severity of Coronary Artery Disease in Patients with Atrial Fibrillation Undergoing First-Time Coronary Angiography. PLoS ONE 2011, 6, e24964. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.; Pecen, L.; Lucerna, M.; Huber, K.; Rohla, M.; Renda, G.; Siller-Matula, J.; Schnabel, R.B.; Cemin, R.; Kirchhof, P.; et al. Outcomes of anticoagulated patients with atrial fibrillation treated with or without antiplatelet therapy—A pooled analysis from the PREFER in AF and PREFER in AF PROLONGATON registries. Int. J. Cardiol. 2018, 270, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Eyileten, C.; Postula, M.; Jakubik, D.; Toma, A.; Mirowska-Guzel, D.; Patti, G.; Renda, G.; Siller-Matula, J.M. Non-Vitamin K Oral Anticoagulants (NOAC) versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type. J. Clin. Med. 2020, 9, 1120. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Berg, J.M.T.; et al. Safety and Efficacy of Antithrombotic Strategies in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis of Randomized Controlled Trials. JAMA Cardiol. 2019, 4, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T., Jr.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.H.; Wojdyla, D.; Vora, A.N.; Thomas, L.; Granger, C.B.; Goodman, S.G.; Aronson, R.; Windecker, S.; Mehran, R.; Lopes, R.D. Risk/Benefit Tradeoff of Antithrombotic Therapy in Patients with Atrial Fibrillation Early and Late after an Acute Coronary Syndrome or Percutaneous Coronary Intervention: Insights from AUGUSTUS. Circulation 2020, 141, 1618–1627. [Google Scholar] [CrossRef] [PubMed]
- Kuno, T.; Ueyama, H.; Takagi, H.; Ando, T.; Numasawa, Y.; Briasoulis, A.; Fox, J.; Bangalore, S. Meta-analysis of Antithrombotic Therapy in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention. Am. J. Cardiol. 2020, 125, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Lewalter, T.; Unikas, R.; Marin, F.; Schiele, F.; Laeis, P.; Reimitz, P.-E.; Smolnik, R.; et al. Edoxaban in atrial fibrillation patients with percutaneous coronary intervention by acute or chronic coronary syndrome presentation: A pre-specified analysis of the ENTRUST-AF PCI trial. Eur. Heart J. 2020, 41, 4497–4504. [Google Scholar] [CrossRef] [PubMed]
- Ohman, E.M.; Roe, M.T.; Steg, P.G.; James, S.K.; Povsic, T.J.; White, J.; Rockhold, F.; Plotnikov, A.; Mundl, H.; Strony, J.; et al. Clinically significant bleeding with low-dose rivaroxaban versus aspirin, in addition to P2Y12 inhibition, in acute coronary syndromes (GEMINI-ACS-1): A double-blind, multicentre, randomised trial. Lancet 2017, 389, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.H.; Lopes, R.D.; James, S.; Kilaru, R.; He, Y.; Mohan, P.; Bhatt, D.L.; Goodman, S.; Verheugt, F.W.; Flather, M.; et al. Apixaban with Antiplatelet Therapy after Acute Coronary Syndrome. N. Engl. J. Med. 2011, 365, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Toelg, R.; Wienbergen, H.; Hobbach, H.-P.; Cuneo, A.; Bekeredjian, R.; Ritter, O.; Hailer, B.; Hertting, K.; Hennersdorf, M.; et al. Current status of antithrombotic therapy and in-hospital outcomes in patients with atrial fibrillation undergoing percutaneous coronary intervention in Germany. Herz 2023, 48, 134–140. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | VKA (n = 64) | NOAC (n = 81) | p Value |
|---|---|---|---|
| Age, y | 70.3 ± 10.8 | 71.8 ± 13.5 | 0.18 |
| Women, n (%) | 19 (29.7) | 29 (35.8) | 0.43 |
| Length of hospitalization, d | 9.3 ± 4.8 | 8.6 ± 5.8 | 0.14 |
| BMI, kg/m2 | 28.7 ± 5.2 | 29.6 ± 5.7 | 0.37 |
| Arterial hypertension, n (%) | 51 (79.7) | 67 (82.7) | 0.64 |
| Diabetes, n (%) | 20 (31.2) | 29 (35.8) | 0.56 |
| Hypercholesterolemia, n (%) | 52 (81.2) | 66 (81.5) | 0.97 |
| Smoking, n (%) | 13 (20.6) | 16 (20) | 0.92 |
| Smoking history, n (%) | 30 (48.4) | 27 (34.2) | 0.09 |
| Creatinine clearance | 73.8 ± 35.9 | 86.1 ± 38.9 | 0.07 |
| Prior myocardial infarction, n (%) | 27 (42.2) | 34 (42) | 0.97 |
| Prior percutaneous coronary intervention, n (%) | 20 (31.3) | 32 (40.5) | 0.25 |
| Prior coronary artery bypass grafting, n (%) | 11 (17.2) | 13 (16.3) | 0.88 |
| Chronic obstructive pulmonary disease, n (%) | 4 (6.3) | 4 (5) | 0.73 |
| Ejection fraction, % | 40.6 ± 12.8 | 50.9 ± 19 | 0.0007 |
| Systolic blood pressure, mmHg | 137.6 ± 22.1 | 140.2 ± 25 | 0.5 |
| Heart rate, bpm | 88.7 ± 26.8 | 90.7 ± 30.2 | 0.7 |
| Diagnosis | |||
| STEMI, n (%) | 13 (20.3) | 18 (22.2) | 0.78 |
| NSTEMI, n (%) | 34 (53) | 41 (50.6) | 0.76 |
| UA, n (%) | 17 (26.6) | 22 (27.2) | 0.94 |
| EuroScore 2 | 7.9 ± 6.9 | 8.2 ± 5.9 | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bachorski, W.; Bychowski, J.; Gruchała, M.; Jaguszewski, M. Two Approaches to Triple Antithrombotic Therapy in Patients with Acute Coronary Syndrome and Non-Valvular Atrial Fibrillation Treated with Percutaneous Coronary Intervention: Which Is More Efficient and Safer? Diagnostics 2023, 13, 3055. https://doi.org/10.3390/diagnostics13193055
Bachorski W, Bychowski J, Gruchała M, Jaguszewski M. Two Approaches to Triple Antithrombotic Therapy in Patients with Acute Coronary Syndrome and Non-Valvular Atrial Fibrillation Treated with Percutaneous Coronary Intervention: Which Is More Efficient and Safer? Diagnostics. 2023; 13(19):3055. https://doi.org/10.3390/diagnostics13193055
Chicago/Turabian StyleBachorski, Witold, Jakub Bychowski, Marcin Gruchała, and Miłosz Jaguszewski. 2023. "Two Approaches to Triple Antithrombotic Therapy in Patients with Acute Coronary Syndrome and Non-Valvular Atrial Fibrillation Treated with Percutaneous Coronary Intervention: Which Is More Efficient and Safer?" Diagnostics 13, no. 19: 3055. https://doi.org/10.3390/diagnostics13193055
APA StyleBachorski, W., Bychowski, J., Gruchała, M., & Jaguszewski, M. (2023). Two Approaches to Triple Antithrombotic Therapy in Patients with Acute Coronary Syndrome and Non-Valvular Atrial Fibrillation Treated with Percutaneous Coronary Intervention: Which Is More Efficient and Safer? Diagnostics, 13(19), 3055. https://doi.org/10.3390/diagnostics13193055