


Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
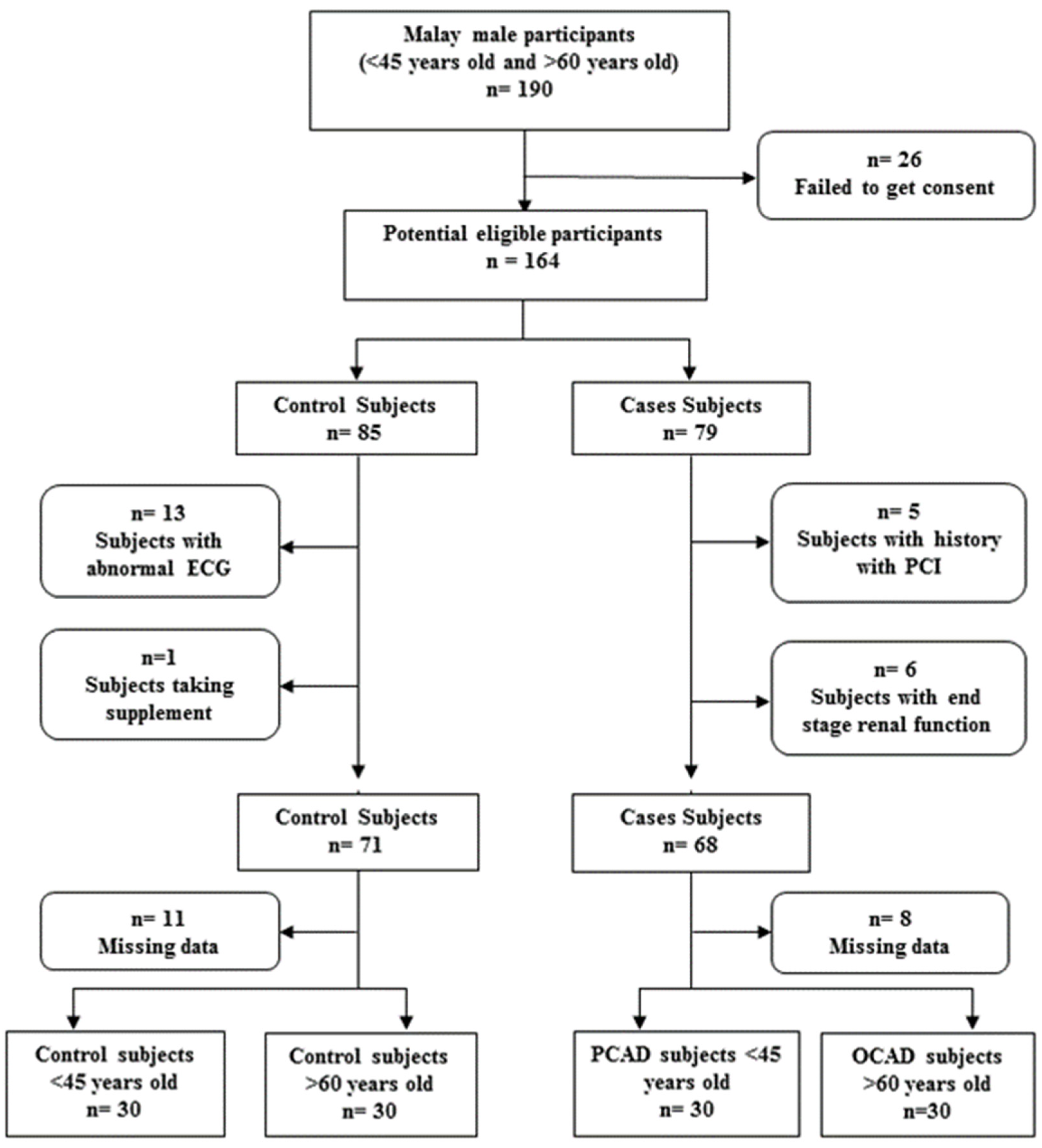
2.1. Study Population
2.2. Demographic and Biochemical Analysis
2.3. Determination of Heart Biomarkers
2.4. Statistical Analysis
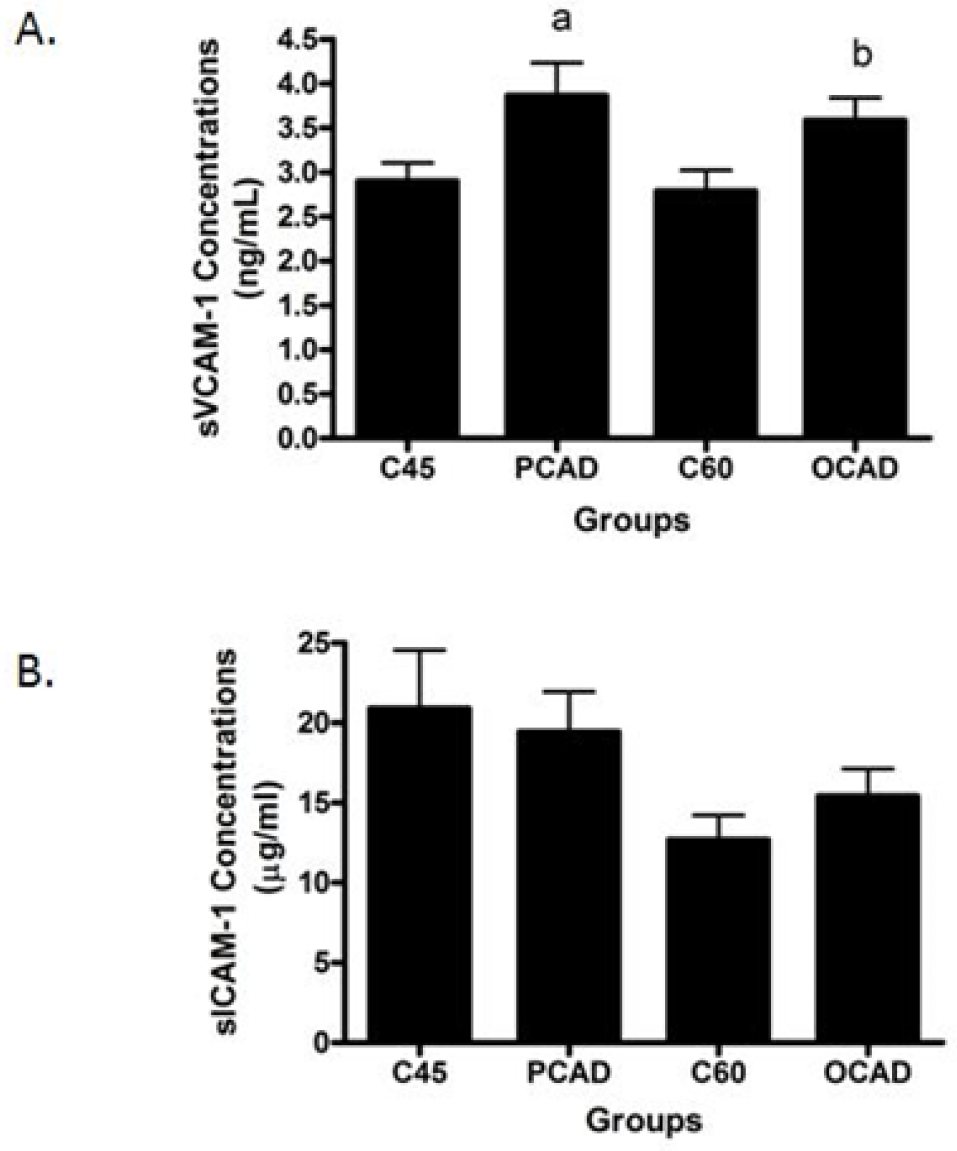
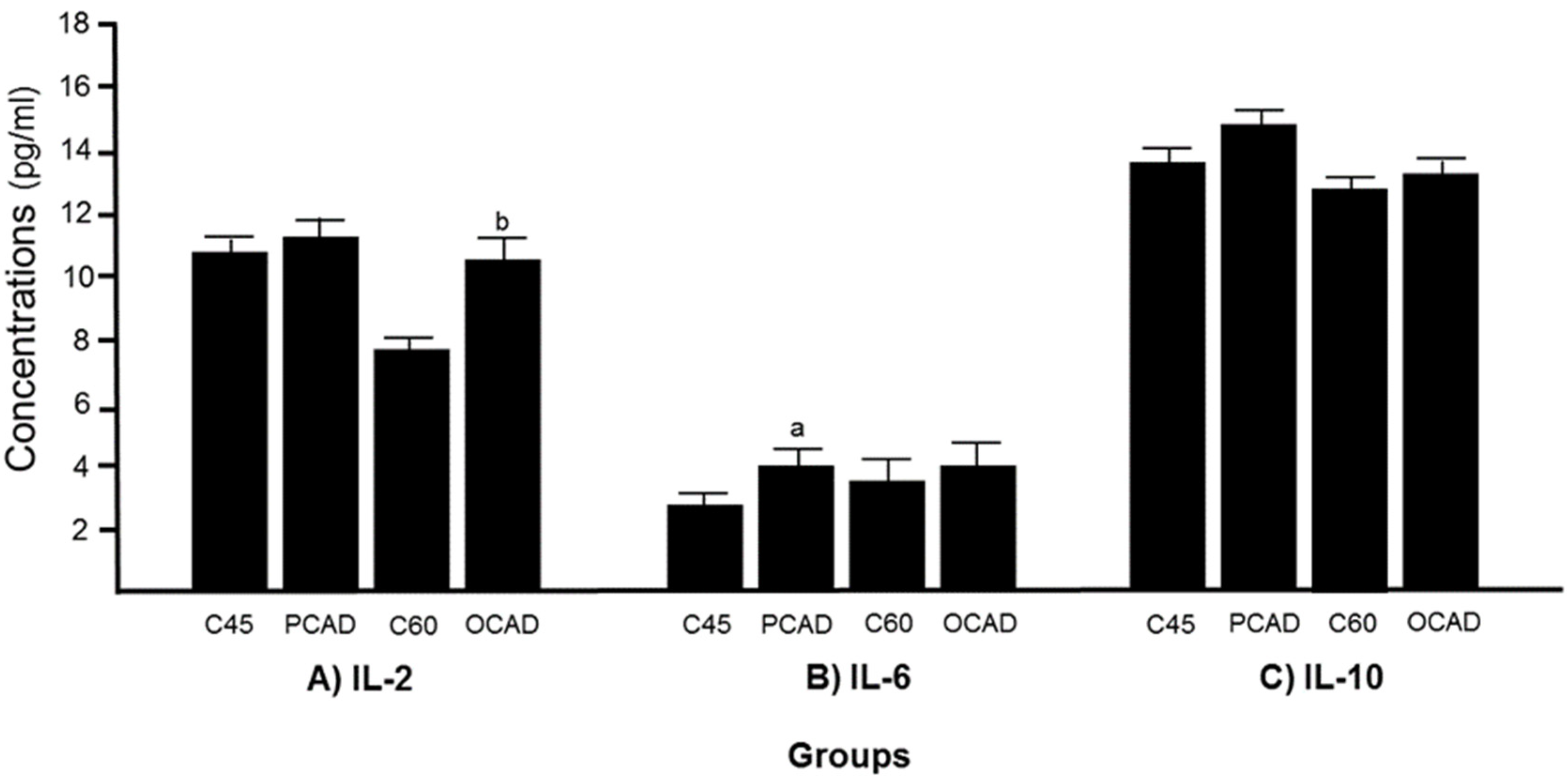
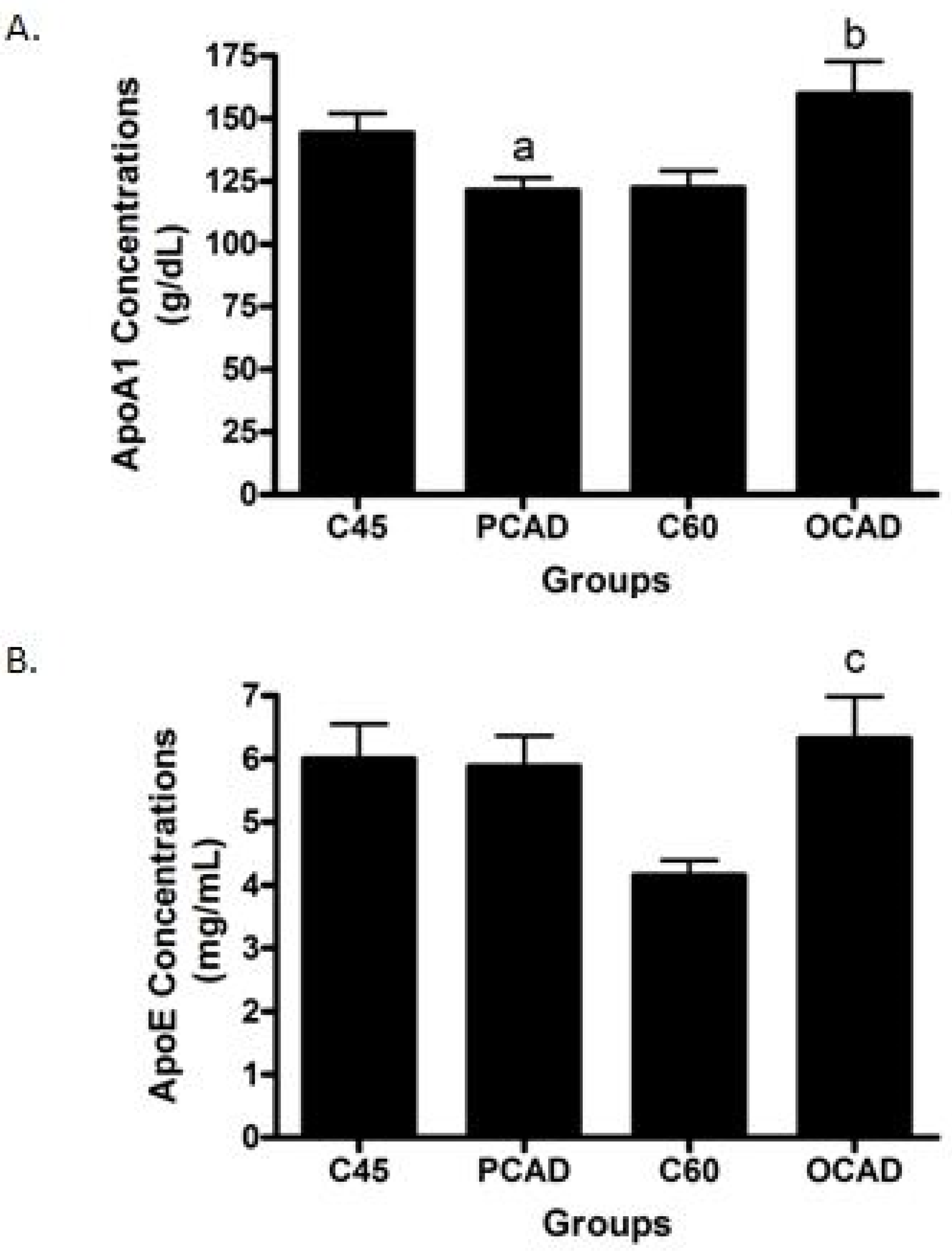
3. Results
4. Discussion
5. Future Direction
6. Limitation of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shukor, M.F.A.; Ismail, N.A.S.; Wan Ngah, W.Z. Challenges in predicting risks of premature coronary artery disease (PCAD). Sains Malays. 2019, 47, 2543–2556. [Google Scholar] [CrossRef]
- Shah, S.A.; Lee, J.; Khalid, M.S.; Najid, F.; Haniff, I.S.; Mohd Ghazi, A.; MohdNor, I.F.; Mohd Ali, R.; Wan Ngah, W.Z. Prevalence and risk factors of premature coronary artery disease: A comparative cross-sectional study between two time frames in Malaysia. J. Public Health Med. 2015, 15, 157–166. [Google Scholar]
- Arzamendi, D.; Benito, B.; Tizon-Marcos, H.; Flores, J.; Tanguay, J.F.; Ly, H.; Doucet, S.; Leduc, L.; Leung, T.K.; Campuzano, O.; et al. Increase in sudden death from coronary artery disease in young adults. Am. Heart J. 2011, 161, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics. Statistics on Causes of Death, Malaysia, 2017; DOSM: Kuala Lumpur, Malaysia, 2017.
- Sazlina, S.G.; Sooryanarayana, R.; Ho, B.K.; Omar, M.A.; Krishnapillai, A.D.; MohdTohit, N.; Inche Zainal Abidin, S.; Ariaratnam, S.; Ahmad, N.A. Cardiovascular disease risk factors among older people: Data from the National Health and Morbidity Survey 2015. PLoS ONE 2020, 15, e0240826. [Google Scholar] [CrossRef]
- Douglas, G.; Channon, K.M. The pathogenesis of atherosclerosis. Medicine 2014, 42, 480–484. [Google Scholar] [CrossRef]
- Troncoso, M.F.; Ortiz-Quintero, J.; Garrido-Moreno, V.; Sanhueza-Olivares, F.; Guerrero-Moncayo, A.; Chiong, M.; Castro, P.F.; García, L.; Gabrielli, L.; Corbalán, R.; et al. VCAM-1 as a predictor biomarker in cardiovascular disease. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166170. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.; Cruz, M.S.; Bortolin, R.H.; Oliveira, K.M.; Araújo, J.; Duarte, V.; Silva, A.; Santos, I.; Dantas, J.; Paiva, M.; et al. Relationship between circulating VCAM-1, ICAM-1, E-selectin and MMP9 and the extent of coronary lesions. Clinics 2018, 73, e203. [Google Scholar] [CrossRef]
- Habas, K.; Shang, L. Alterations in intercellular adhesion molecule 1 (ICAM-1) and vascular cell adhesion molecule 1 (VCAM-1) in human endothelial cells. Tissue Cell 2018, 54, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Zhao, T.X.; Newland, S.A.; Mallat, Z. 2019 ATVB Plenary Lecture: Interleukin-2 Therapy in Cardiovascular Disease: The Potential to Regulate Innate and Adaptive Immunity. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 853–864. [Google Scholar] [CrossRef]
- Posadas-Sánchez, R.; Cardoso-Saldaña, G.; Fragoso, J.M.; Vargas-Alarcón, G. Interferon Regulatory Factor 5 (IRF5) Gene Haplotypes are Associated with Premature Coronary Artery Disease. Association of the IRF5 Polymorphisms with CardiometabolicParameters. The Genetics of Atherosclerotic Disease (GEA) Mexican Study. Biomolecules 2021, 11, 443. [Google Scholar] [CrossRef]
- Ciftdoğan, D.Y.; Coskun, S.; Ulman, C.; Tıkız, H. The association of apolipoprotein E polymorphism and lipid levels in children with a family history of premature coronary artery disease. J. Clin. Lipidol. 2012, 6, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.R.; Lei, Y.Y.; Li, J.; Jiang, N.; Shi, J.P. Association between apolipoprotein E polymorphisms and premature coronary artery disease: A meta-analysis. Clin. Chem. Lab. Med. 2017, 55, 284–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karjalainen, J.P.; Mononen, N.; Hutri-Kähönen, N.; Lehtimäki, M.; Juonala, M.; Ala-Korpela, M.; Kähönen, M.; Raitakari, O.; Lehtimäki, T. The effect of apolipoprotein E polymorphism on serum metabolome—A population-based 10-year follow-up study. Sci. Rep. 2019, 9, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e563–e595. [Google Scholar] [CrossRef]
- Siemelink, M.A.; Zeller, T. Biomarkers of coronary artery disease: The promise of the transcriptome. Curr. Cardiol. Rep. 2014, 16, 513. [Google Scholar] [CrossRef] [Green Version]
- Yayan, J. Emerging families of biomarkers for coronary artery disease: Inflammatory mediators. Vasc. Health Risk Manag. 2013, 9, 435–456. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Garcia, J.; Lerman, A.; Weisz, G.; Maehara, A.; Mintz, G.S.; Fahy, M.; Xu, K.; Lansky, A.J.; Cristea, E.; Farah, T.G.; et al. Age- and gender-related changes in plaque composition in patients with acute coronary syndrome: The PROSPECT study. EuroIntervention 2012, 8, 929–938. [Google Scholar] [CrossRef]
- Dupond, W.D.; Plummer, W.D., Jr. Power and sample size calculations for studies involving linear regression. Control. Clin. Trials 1998, 19, 589–601. [Google Scholar]
- Landmesser, U.; Merten, R.; Spiekermann, S.; Büttner, K.; Drexler, H.; Hornig, B. Vascular extracellular superoxide dismutase activity in patients with coronary artery disease: Relation to endothelium-dependent vasodilation. Circulation 2000, 101, 2264–2270. [Google Scholar] [CrossRef] [Green Version]
- Semaan, H.B.; Gurbel, P.A.; Anderson, J.L.; Muhlestein, J.B.; Carlquist, J.F.; Horne, B.D.; Serebruany, V.L. Soluble VCAM-1 and E-selectin, but not ICAM-1 discriminate endothelial injury in patients with documented coronary artery disease. Cardiology 2000, 93, 7–10. [Google Scholar] [CrossRef]
- Sadeghian, S.; Fallahi, F.; Salarifar, M.; Davoodi, G.; Mahmoodian, M.; Fallah, N.; Darvish, S.; Karimi, A.; Tehran Heart Center. Homocysteine, vitamin B12 and folate levels in premature coronary artery disease. BMC Cardiovasc. Disord. 2006, 6, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammad, A.M.; Jehangeer, H.I.; Shaikhow, S.K. Prevalence and risk factors of premature coronary artery disease in patients undergoing coronary angiography in Kurdistan, Iraq. BMC Cardiovasc. Disord. 2015, 15, 155. [Google Scholar] [CrossRef]
- Salehi, N.; Janjani, P.; Tadbiri, H.; Rozbahani, M.; Jalilian, M. Effect of cigarette smoking on coronary arteries and pattern and severity of coronary artery disease: A review. J. Int. Med. Res. 2021, 49, 3000605211059893. [Google Scholar] [CrossRef] [PubMed]
- Magnoni, M.; Andreini, D.; Pirillo, A.; Uboldi, P.; Latini, R.; Catapano, A.L.; Maggioni, A.P.; Norata, G.D.; CAPIRE Study Group. Predictive value of HDL function in patients with coronary artery disease: Relationship with coronary plaque characteristics and clinical events. Ann. Med. 2022, 54, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Battistoni, A.; Rubattu, S.; Tocci, G. Hypertension in the elderly: Which are the blood pressure threshold values? Eur. Heart J. Suppl. 2019, 21 (Suppl. B), B105–B106. [Google Scholar] [CrossRef]
- Musthafa, Q.A.; Abdul Shukor, M.F.; Ismail, N.A.S.; Mohd Ghazi, A.; Mohd Ali, R.; If, M.N.; Dimon, M.Z.; Wan Ngah, W.Z. Oxidative status and reduced glutathione levels in premature coronary artery disease and coronary artery disease. Free Radic. Res. 2017, 51, 787–798. [Google Scholar] [CrossRef]
- Gurven, M.; Blackwell, A.D.; Rodríguez, D.E.; Stieglitz, J.; Kaplan, H. Does blood pressure inevitably rise with age? Longitudinal evidence among forager-horticulturalists. Hypertension 2012, 60, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Natalie, C.W.; Gerald, F.W.; Robert, H.E. Statin toxicity mechanistic insights and clinical implications. Circ. Res. 2019, 124, 328–350. [Google Scholar]
- Zhang, Y.; Liu, H.; Tang, W.; Qiu, Q.; Peng, J. Resveratrol prevents TNF-α-induced VCAM-1 and ICAM-1 upregulation in endothelial progenitor cells via reduction of NF-κB activation. J. Int. Med. Res. 2020, 48, 300060520945131. [Google Scholar] [CrossRef]
- Postadzhiyan, A.S.; Tzontcheva, A.V.; Kehayov, I.; Finkov, B. Circulating soluble adhesion molecules ICAM-1 and VCAM-1 and their association with clinical outcome, troponin T and C-reactive protein in patients with acute coronary syndromes. Clin. Biochem. 2008, 41, 126–133. [Google Scholar] [CrossRef]
- Ding, R.; Gao, W.; Ostrodci, D.H.; He, Z.; Song, Y.; Ma, L.; Liang, C.; Wu, Z. Effect of interleukin-2 level and genetic variants on coronary artery disease. Inflammation 2013, 36, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Mizia-Stec, K.; Mandecki, T.; Zahorska-Markiewicz, B.; Janowska, J.; Szulc, A.; Jastrzebska-Maj, E.; Szymanski, L.; Majewski, T. Selected cytokines and soluble forms of cytokine receptors in coronary artery disease. Eur. J. Intern. Med. 2002, 13, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Von der Thusen, J.H.; Kuiper, J.; van Berkel, T.J.; Biessen, E.A. Interleukins in atherosclerosis: Molecular pathways and therapeutic potential. Pharmacol. Rev. 2003, 55, 133–166. [Google Scholar] [CrossRef]
- Basiak, M.; Kosowski, M.; Hachula, M.; Okopien, B. Plasma concentrations of cytokines in patients with combined hyperlipidemia and atherosclerotic plaque before treatment initiation-a pilot study. Medicina 2022, 58, 624. [Google Scholar] [CrossRef] [PubMed]
- Hartman, J.; Frishman, W.H. Inflammation and atherosclerosis: A review of the role of interleukin-6 in the development of atherosclerosis and the potential for targeted drug therapy. Cardiol. Rev. 2014, 22, 147–151. [Google Scholar] [CrossRef]
- Han, X.; Boisvert, W.A. Interleukin-10 protects against atherosclerosis by modulating multiple atherogenic macrophage function. Thromb. Haemost. 2015, 113, 505–512. [Google Scholar] [CrossRef]
- Wang, P.; Wu, P.; Siegel, M.I.; Egan, R.W.; Billah, M.M. Interleukin (IL)-10 inhibits nuclear factor kappa B (NF kappa B) activation in human monocytes. IL-10 and IL-4 suppress cytokine synthesis by different mechanisms. J. Biol. Chem. 1995, 270, 9558–9563. [Google Scholar] [CrossRef] [Green Version]
- Posadas-Sánchez, R.; Angeles-Martínez, J.; Pérez-Hernández, N.; Rodríguez-Pérez, J.M.; López-Bautista, F.; Flores-Dominguez, C.; Fragoso, J.M.; Posadas-Romero, C.; Vargas-Alarcón, G. The IL-10-1082 (rs1800896) G allele is associated with a decreased risk of developing premature coronary artery disease and some IL-10 polymorphisms were associated with clinical and metabolic parameters. The GEA study. Cytokine 2018, 106, 12–18. [Google Scholar] [CrossRef]
- Fiehn, C.; Paleolog, E.M.; Feldmann, M. Selective enhancement of endothelial cell VCAM-1 expression by interleukin-10 in the presence of activated leucocytes. Immunology 1997, 91, 565–571. [Google Scholar] [CrossRef]
- Fiorentino, D.F.; Zlotnik, A.; Vieira, P.; Mosmann, T.R.; Howard, M.; Moore, K.W.; O’Garra, A. IL-10 acts on the antigen-presenting cell to inhibit cytokine production by Th1 cells. J. Immunol. 1991, 146, 3444–3451. [Google Scholar] [CrossRef]
- Fukushi, J.; Ono, M.; Morikawa, W.; Iwamoto, Y.; Kuwano, M. The activity of soluble VCAM-1 in angiogenesis stimulated by IL-4 and IL-13. J. Immunol. 2000, 165, 2818–2823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer-Crocker, R.L.; Hughes, C.C.; Pober, J.S. IL-4 and IL-13 activate the JAK2 tyrosine kinase and Stat6 in cultured human vascular endothelial cells through a common pathway that does not involve the gamma c chain. J. Clin. Investig. 1996, 98, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menge, D.M.; Nair, N.K.; Varghese, T.P.; Vijayakumar, P.R.A. High-density lipoprotein: Role in reverse cholesterol transport. IJPSR 2019, 10, 484–488. [Google Scholar]
- Aghajani, M.H.; Neishaboori, A.M.; Ahmadzadeh, K.; Toloui, A.; Yousefifard, M. The association between apolipoprotein A-1 plasma level and premature coronary artery disease: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14578. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.K.; Agarwal, S.; Daga, M.K. Conventional and advanced lipid parameters in premature coronary artery disease patients in India. J. Clin. Diagn. Res. 2015, 9, BC07–BC11. [Google Scholar] [CrossRef]
- Di Donato, J.A.; Huang, Y.; Aulak, K.S.; Even-Or, O.; Gerstenecker, G.; Gogonea, V.; Wu, Y.; Fox, P.L.; Tang, W.H.; Plow, E.F.; et al. Function and distribution of apolipoprotein A1 in the artery wall are markedly distinct from those in plasma. Circulation 2013, 128, 1644–1655. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Di Donato, J.A.; Levison, B.S.; Schmitt, D.; Li, L.; Wu, Y.; Buffa, J.; Kim, T.; Gerstenecker, G.S.; Gu, X.; et al. An abundant dysfunctional apolipoprotein A1 in human atheroma. Nat. Med. 2014, 20, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Nikoulin, I.R.; Curtiss, L.K. An apolipoprotein E synthetic peptide targets to lipoproteins in plasma and mediates both cellular lipoprotein interactions in vitro and acute clearance of cholesterol-rich lipoproteins in vivo. J. Clin. Investig. 1998, 101, 223–234. [Google Scholar] [CrossRef] [Green Version]
- Hasty, A.H.; Linton, M.F.; Swift, L.L.; Fazio, S. Determination of the lower threshold of apolipoprotein E resulting in remnant lipoprotein clearance. J. Lipid Res. 1999, 40, 1529–1538. [Google Scholar] [CrossRef]
- Mensenkamp, A.R.; Jong, M.C.; van Goor, H.; van Luyn, M.J.; Bloks, V.; Havinga, R.; Voshol, P.J.; Hofker, M.H.; van Dijk, K.W.; Havekes, L.M.; et al. Apolipoprotein E participates in the regulation of very low density lipoprotein-triglyceride secretion by the liver. J. Biol. Chem. 1999, 274, 35711–35718. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, P.; Alam, S.F. Role of homocysteine in the development of cardiovascular disease. Nutr. J. 2015, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Ranjith, P.; Devika, P. Clinical Correlation between Plasma Homocysteine Level and Coronary Artery Disease in Indian Patients. World J. Cardiovasc. Dis. 2017, 7, 477–485. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.K.; Kotwal, J.; Kotwal, A.; Dhall, A.; Garg, S. Role of homocysteine & MTHFR C677T gene polymorphism as risk factors for coronary artery disease in young Indians. Indian J. Med. Res. 2012, 135, 506–512. [Google Scholar]
- Eftychiou, C.; Antoniades, L.; Makri, L.; Koumas, L.; Costeas, P.A.; Kyriakou, E.; Nicolaides, E.; Papadogiannis, D. Homocysteine levels and MTHFR polymorphisms in young patients with acute myocardial infarction: A case control study. Hell. J. Cardiol. 2012, 53, 189–194. [Google Scholar]
- Habib, S.S.; Al Masri, A.A. Relationship of high sensitivity C-reactive protein with presence and severity of coronary artery disease. Pak. J. Med. Sci. 2013, 29, 1425–1429. [Google Scholar] [CrossRef] [PubMed]
- Xiaojuan, Z.; Jie, N.; Wei, G.; Lijun, G.; Guisong, W.; Fuchun, Z.; Yongzhen, Z.; Haiyan, L. Clinical and angiographic analysis of premature coronary artery disease in patients with age ≤50 years. Heart 2011, 97, A166. [Google Scholar] [CrossRef]
- Lavie, C.J.; Lee, J.H.; Milani, R.V. Vitamin D and cardiovascular disease will it live up to its hype? J. Am. Coll. Cardiol. 2011, 58, 1547–1556. [Google Scholar] [CrossRef] [Green Version]
- Van de Luijtgaarden, K.M.; Voute, M.T.; Hoeks, S.E.; Bakker, E.J.; Chonchol, M.; Stolker, R.J.; Rouwet, E.V.; Verhagen, H.J. Vitamin D deficiency may be an independent risk factor for arterial disease. J. Am. Coll. Cardiol. 2012, 44, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Amer, M.; Qayyum, R. Relation between serum 25-hydroxyvitamin D and C-reactive protein in asymptomatic adults (from the continuous National Health and Nutrition Examination Survey 2001 to 2006). Am. J. Cardiol. 2012, 109, 226–230. [Google Scholar] [CrossRef]
- Vähätalo, J.; Holmström, L.; Pakanen, L.; Kaikkonen, K.; Perkiömäki, J.; Huikuri, H.; Junttila, J. Coronary Artery Disease as the Cause of Sudden Cardiac Death Among Victims <50 Years of Age. Am. J. Cardiol. 2021, 147, 33–38. [Google Scholar] [CrossRef]
- Panwar, R.B.; Gupta, R.; Gupta, B.K.; Raja, S.; Vaishnav, J.; Khatri, M.; Agrawal, A. Atherothrombotic risk factors & premature coronary heart disease in India: A case-control study. Indian J. Med. Res. 2011, 134, 26–32. [Google Scholar] [PubMed]
- Che, J.; Li, G.; Shao, Y.; Niu, H.; Shi, Y. An analysis of the risk factors for premature coronary artery disease in young and middle-age Chinese patients with hypertension. Exp. Clin. Cardiol. 2013, 18, 89–92. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| C45 | PCAD | p-Value for PCAD vs. C45 | C60 | OCAD | p-Value for OCAD vs. C60 | Normal Value | |
|---|---|---|---|---|---|---|---|
| Demographic Data | |||||||
| Age | 37.96 ± 7.31 | 41.60 ± 5.98 | p = 0.058 * | 66.77 ± 6.05 | 64.87 ± 3.96 | p = 0.156 * | - |
| Height (m) | 1.68 ± 5.48 | 1.65 ± 6.17 | p = 0.148 * | 1.62 ± 4.26 | 1.62 ± 6.09 | p = 0.760 * | - |
| Weight (kg) | 75.67 ± 18.12 | 79.07 ± 12.46 | p = 0.415 * | 73.04 ± 14.35 | 71.46 ± 9.47 | p = 0.631 * | - |
| BMI (kg/m2) | 27.17 ± 5.27 | 28.47 ± 4.03 | p = 0.318 * | 27.85 ± 5.25 | 26.94 ± 2.94 | p = 0.44 * | 19–24 |
| Systolic blood pressure (mmHg) | 125.54 ± 17.40 | 129.14 ± 20.86 | p = 0.493 * | 138.96 ± 15.03 | 146.80 ± 22.02 | p = 0.122 * | 120 |
| Diastolic blood pressure (mmHg) | 74.84 ± 15.30 | 81.45 ± 13.28 | p = 0.092 * | 76.38 ± 11.34 | 77.47 ± 12.67 | p = 0.739 * | 80 |
| Fasting glucose (mmol/L) | 4.90 ± 0.57 | 5.92 ± 1.11 | p < 0.001 a,* | 6.19 ± 2.10 | 7.72 ± 2.93 | p = 0.006 b,** | 3.5–5.5 |
| Liver Profile | |||||||
| Albumin (g/L) | 46.65 ± 2.62 | 45.00 ± 3.95 | p = 0.135 * | 43.48 ± 3.74 | 42.41 ± 4.09 | p = 0.309 ** | 35–52 |
| Total protein (g/L) | 76.12 ± 3.77 | 74.45 ± 5.19 | p = 0.254 * | 73.83 ± 5.43 | 71.55 ± 4.76 | p = 0.095 * | 65–85 |
| Total bilirubin (µmol/L) | 9.94 ± 4.29 | 10.69 ± 9.63 | p = 0.765 * | 10.93 ± 3.06 | 9.00 ± 4.35 | p = 0.056 * | <24 |
| ALT (U/L) | 28.88 ± 8.54 | 38.10 ± 21.42 | p = 0.046 a,* | 25.34 ± 3.74 | 32.17 ± 2.19 | p = 0.301 ** | <41 |
| ALP (U/L) | 72.24 ± 19.29 | 84.68 ± 24.03 | p = 0.078 * | 73.48 ± 14.67 | 79.62 ± 31.53 | p = 0.348 * | <129 |
| Renal Profile | |||||||
| Sodium (mmol/L) | 140.55 ± 1.80 | 138.33 ± 3.23 | p = 0.002 a,* | 141.76 ± 2.67 | 138.00 ± 3.08 | p < 0.001 b,* | 135–152 |
| Potassium (mmol/L) | 4.10 ± 0.43 | 4.38 ± 0.42 | p = 0.013 a,* | 3.91 ± 0.43 | 4.48 ± 0.65 | p < 0.001 b,* | 3.6–5.4 |
| Urea (mmol/L) | 4.36 ± 1.26 | 4.70 ± 1.75 | p = 0.404 * | 4.67 ± 1.02 | 5.88 ± 2.20 | p = 0.011 b,* | <8.3 |
| Creatinine (µmol/L) | 86.55 ± 20.97 | 92.40 ± 20.32 | p = 0.281 * | 98.00 ± 15.39 | 113.18 ± 44.07 | p = 0.094 * | <130 |
| Lipid Profile | |||||||
| Triglyceride (mmol/L) | 1.13 ± 0.48 | 2.57 ± 1.82 | p < 0.001 a,* | 2.10 ± 1.31 | 1.86 ± 0.94 | p = 0.834 ** | <2.3 |
| HDL (mmol/L) | 1.29 ± 0.34 | 0.94 ± 0.27 | p < 0.001 a,* | 1.25 ± 0.29 | 1.10 ± 0.29 | p = 0.066 * | >1 |
| LDL (mmol/L) | 3.11 ± 0.81 | 2.66 ± 1.25 | p = 0.114 * | 3.60 ± 1.16 | 2.44 ± 1.04 | p < 0.001 b,* | <3.9 |
| Total cholesterol (mmol/L) | 4.92 ± 0.96 | 4.89 ± 1.58 | p = 0.919 * | 5.61 ± 0.93 | 4.58 ± 1.86 | p = 0.011 b,* | <5.2 |
| Smoking | |||||||
| Smoking, n (%) | 13 (43) | 20 (67) | 2 (7) | 8( 27) | |||
| Number of arteries affected | |||||||
| 1, n (%) | 15 (50) | 11 (37) | |||||
| 2, n (%) | 4 (13) | 3 (10) | |||||
| 3, n (%) | 11 (37) | 16 (53) | |||||
| Lipid-lowering drug | |||||||
| Lovastatin, n (%) | 7 (23) | 8 (27) | |||||
| Rosuvastatin, n (%) | 2 (7) | 4 (13) | |||||
| Atorvastatin, n (%) | 8 (27) | 5 (17) | |||||
| Simvastatin, n (%) | 10 (33) | 12 (40) | |||||
| CRP | Vitamin D | Homo- cysteine | sVCAM-1 | sICAM-1 | IL-2 | IL-6 | IL-10 | Apo-A1 | Apo-E | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CRP | r | 1 | 0.091 | −0.108 | 0.283 | −0.104 | −0.025 | 0.212 | 0.251 | 0.044 | 0.151 |
| Sig. | 0.664 | 0.625 | 0.214 | 0.655 | 0.908 | 0.333 | 0.227 | 0.837 | 0.493 | ||
| Vitamin D | r | 1 | −0.120 | 0.335 | −0.271 | −0.051 | 0.021 | 0.436 * | 0.241 | 0.120 | |
| Sig. | 0.552 | 0.094 | 0.200 | 0.795 | 0.914 | 0.016 | 0.208 | 0.541 | |||
| Homocysteine | r | 1 | 0.167 | −0.057 | −0.142 | 0.477 * | −0.026 | −0.078 | 0.217 | ||
| Sig. | 0.437 | 0.808 | 0.498 | 0.016 | 0.897 | 0.706 | 0.298 | ||||
| sVCAM-1 | r | 1 | −0.164 | 0.177 | 0.630 ** | 0.734 ** | 0.327 | 0.328 | |||
| Sig. | 0.489 | 0.407 | 0.001 | 0.000 | 0.104 | 0.117 | |||||
| sICAM-1 | r | 1 | 0.316 | 0.137 | 0.065 | −0.385 | −0.208 | ||||
| Sig. | 0.142 | 0.542 | 0.763 | 0.069 | 0.341 | ||||||
| IL-2 | r | 1 | 0.103 | 0.059 | 0.472 * | 0.069 | |||||
| Sig. | 0.617 | 0.765 | 0.013 | 0.737 | |||||||
| IL-6 | r | 1 | 0.436 * | −0.019 | 0.224 | ||||||
| Sig. | 0.020 | 0.927 | 0.270 | ||||||||
| IL-10 | r | 1 | 0.079 | −0.011 | |||||||
| Sig. | 0.685 | 0.957 | |||||||||
| Apo-A1 | r | 1 | 0.583 ** | ||||||||
| Sig. | 0.001 | ||||||||||
| Apo-E | r | 1 | |||||||||
| Sig. |
| CRP | Vitamin D | Homo- cysteine | sVCAM-1 | sICAM-1 | IL-2 | IL-6 | IL-10 | Apo-A1 | Apo-E | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CRP | r | 1 | −0.272 | 0.058 | 0.478 * | 0.032 | −0.147 | −0.094 | 0.289 | 0.120 | 0.058 |
| Sig. | 0.221 | 0.789 | 0.018 | 0.889 | 0.492 | 0.671 | 0.181 | 0.567 | 0.789 | ||
| Vitamin D | r | 1 | 0.249 | −0.232 | −0.220 | 0.086 | −0.266 | −0.328 | −0.010 | 0.122 | |
| Sig. | 0.220 | 0.253 | 0.291 | 0.682 | 0.199 | 0.110 | 0.962 | 0.554 | |||
| Homocysteine | r | 1 | −0.014 | −0.113 | −0.131 | 0.081 | −0.122 | 0.239 | 0.584 ** | ||
| Sig. | 0.943 | 0.583 | 0.515 | 0.687 | 0.544 | 0.212 | 0.001 | ||||
| sVCAM-1 | r | 1 | −0.150 | −0.224 | 0.256 | 0.562 ** | −0.107 | 0.100 | |||
| Sig. | 0.466 | 0.262 | 0.189 | 0.002 | 0.579 | 0.614 | |||||
| sICAM-1 | r | 1 | −0.262 | −0.004 | −0.263 | 0.151 | −0.112 | ||||
| Sig. | 0.206 | 0.985 | 0.194 | 0.451 | 0.586 | ||||||
| IL-2 | r | 1 | 0.134 | −0.078 | 0.127 | −0.047 | |||||
| Sig. | 0.513 | 0.704 | 0.520 | 0.818 | |||||||
| IL-6 | r | 1 | 0.334 | −0.178 | 0.345 | ||||||
| Sig. | 0.096 | 0.366 | 0.078 | ||||||||
| IL-10 | r | 1 | 0.020 | −0.072 | |||||||
| Sig. | 0.921 | 0.720 | |||||||||
| Apo-A1 | r | 1 | 0.078 | ||||||||
| Sig. | 0.686 | ||||||||||
| Apo-E | r | 1 | |||||||||
| Sig. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shukor, M.F.A.; Musthafa, Q.A.; Mohd Yusof, Y.A.; Wan Ngah, W.Z.; Ismail, N.A.S. Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study. Diagnostics 2023, 13, 188. https://doi.org/10.3390/diagnostics13020188
Shukor MFA, Musthafa QA, Mohd Yusof YA, Wan Ngah WZ, Ismail NAS. Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study. Diagnostics. 2023; 13(2):188. https://doi.org/10.3390/diagnostics13020188
Chicago/Turabian StyleShukor, Muhammad Faizan A., Qurratu Aini Musthafa, Yasmin Anum Mohd Yusof, Wan Zurinah Wan Ngah, and Noor Akmal Shareela Ismail. 2023. "Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study" Diagnostics 13, no. 2: 188. https://doi.org/10.3390/diagnostics13020188
APA StyleShukor, M. F. A., Musthafa, Q. A., Mohd Yusof, Y. A., Wan Ngah, W. Z., & Ismail, N. A. S. (2023). Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study. Diagnostics, 13(2), 188. https://doi.org/10.3390/diagnostics13020188