
Lightweight Separable Convolution Network for Breast Cancer Histopathological Identification

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Datasets
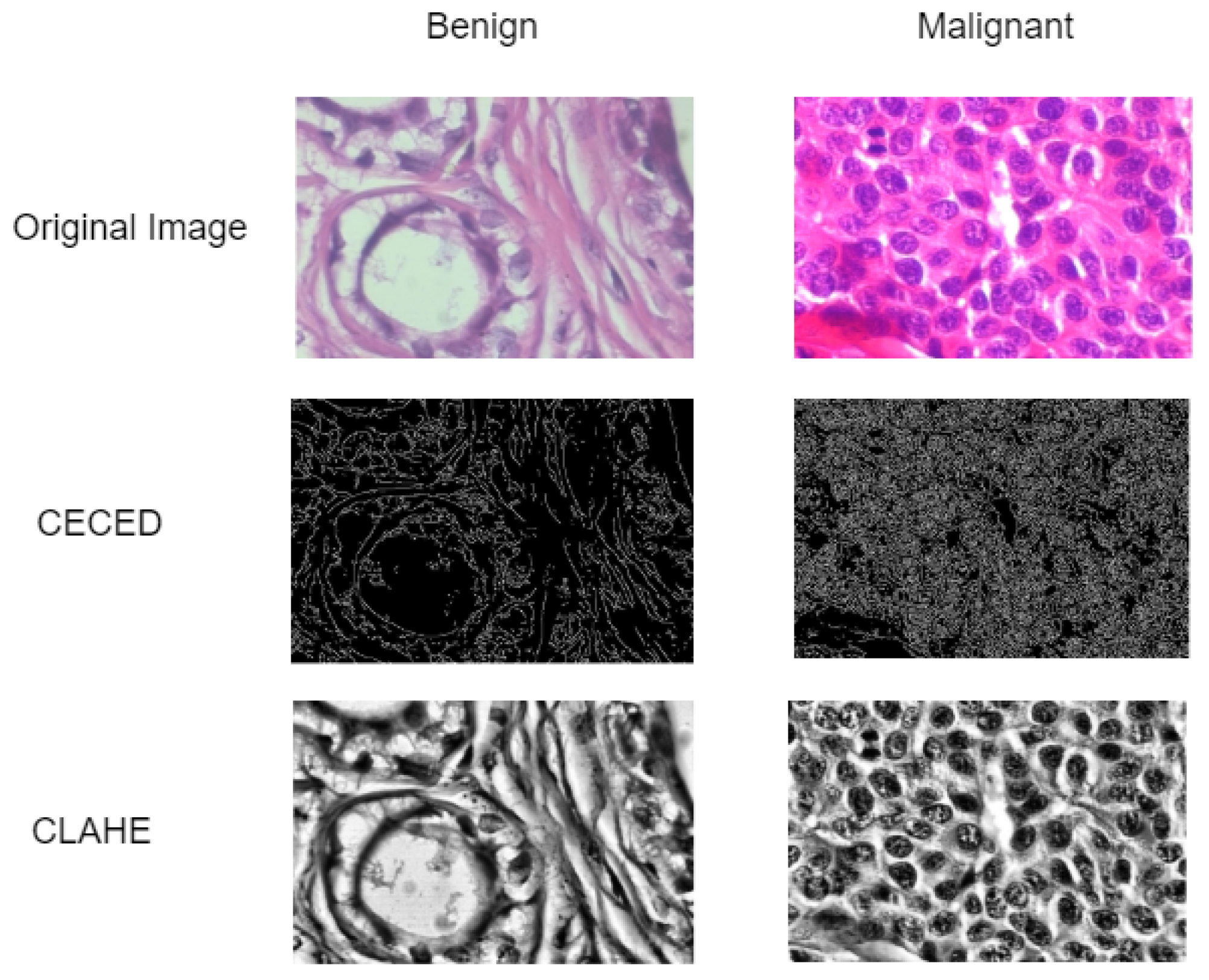
3.2. Data Pre-Processing
Contrast Enhancement (CE) and Edge Detection (ED) Images
3.3. Lightweight Separable Convolution
4. Experimental Results
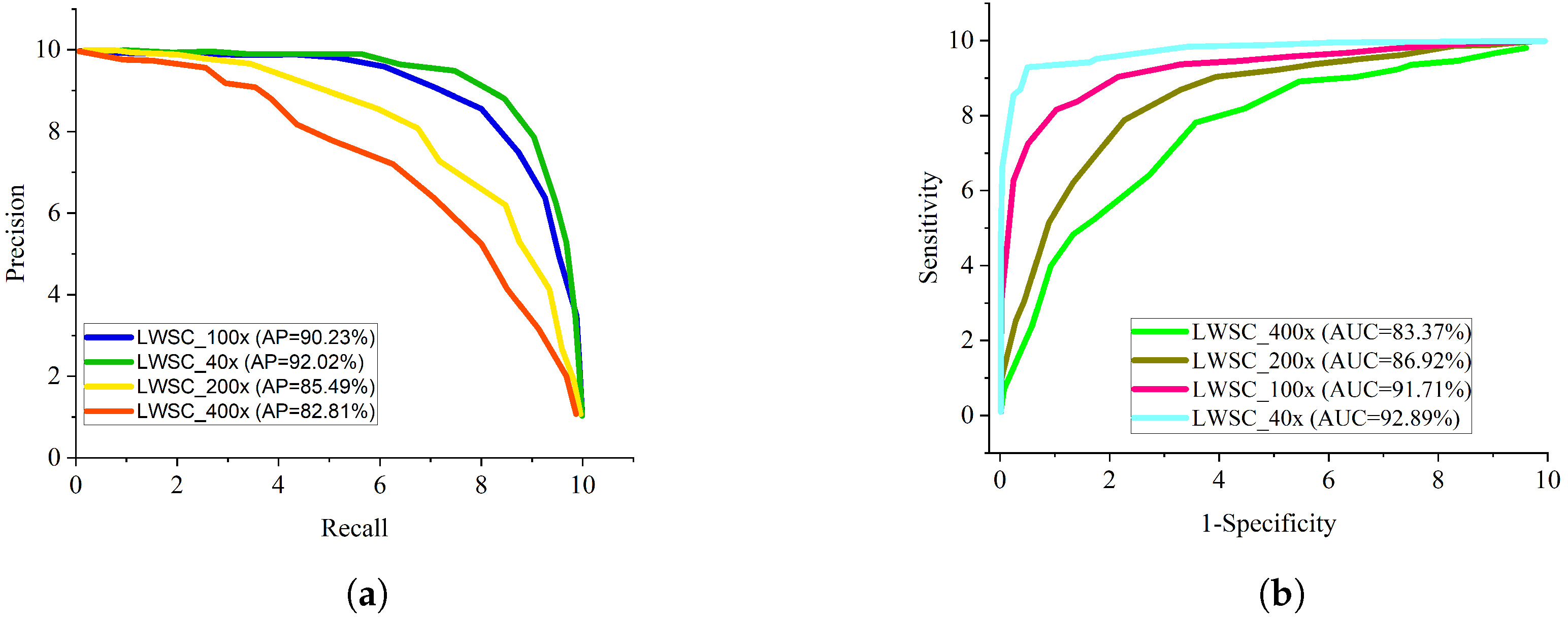
Evaluation of the Lightweight Separable Convolution
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, D.G.R.; Howell, A. Breast cancer risk-assessment models. Breast Cancer Res. 2007, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mehta, J.M.; MacLaughlin, K.L.; Millstine, D.M.; Faubion, S.S.; Wallace, M.R.; Shah, A.A.; Fields, H.E.; Ruddy, B.E.; Bryan, M.J.; Patel, B.; et al. Breast cancer screening: Women’s attitudes and beliefs in light of updated united states preventive services task force and american cancer society guidelines. J. Women’s Health 2019, 28, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, R.M.; Park, Y.; Kreimer, A.R.; Lacey, J.V., Jr.; Pee, D.; Greenlee, R.T.; Buys, S.S.; Hollenbeck, A.; Rosner, B.; Gail, M.H.; et al. Risk prediction for breast, endometrial, and ovarian cancer in white women aged 50 y or older: Derivation and validation from population-based cohort studies. PLoS Med. 2013, 10, e1001492. [Google Scholar] [CrossRef] [PubMed]
- Stark, G.F.; Hart, G.R.; Nartowt, B.J.; Deng, J. Predicting breast cancer risk using personal health data and machine learning models. PLoS ONE 2019, 14, e0226765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sa-nguanraksa, D.; Sasanakietkul, T.; Charoenrat, C.O.; Kulprom, A.; Charoenrat, P.O. Gail model underestimates breast cancer risk in Thai population. Asian Pac. J. Cancer Prev. 2019, 20, 2385–2389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clendenen, T.V.; Ge, W.; Koenig, K.L.; Afanasyeva, Y.; Agnoli, C.; Brinton, L.A.; Darvishian, F.; Dorgan, J.F.; Eliassen, A.H.; Falk, R.T.; et al. Breast cancer risk prediction in women aged 35–50 years: Impact of including sex hormone concentrations in the Gail model. Breast Cancer Res. 2019, 21, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hart, G.R.; Nartowt, B.; Muhammad, W.; Liang, Y.; Huang, G.; Deng, J. Endometrial cancer risk prediction and stratification using personal health data. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E134–E135. [Google Scholar] [CrossRef]
- Belsare, A.D.; Mushrif, M.M.; Pangarkar, M.A.; Meshram, N. Classification of breast cancer histopathology images using texture feature analysis. In Proceedings of the TENCON 2015-2015 IEEE Region 10 Conference, Macao, China, 1–4 November 2015; pp. 1–5. [Google Scholar] [CrossRef]
- Vu, T.H.; Mousavi, H.S.; Monga, V.; Rao, G.; Rao, U.K.A. Histopathological image classification using discriminative feature-oriented dictionary learning. IEEE Trans. Med. Imaging 2016, 35, 738–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anuranjeeta, A.; Shukla, K.K.; Tiwari, A.; Sharma, S. Classification of histopathological images of breast cancerous and non cancerous cells based on morphological features. Biomed. Pharmacol. J. 2017, 10, 353–366. [Google Scholar] [CrossRef]
- Mouelhi, A.; Rmili, H.; Ali, J.B.; Sayadi, M.; Doghri, R.; Mrad, K. Fast unsupervised nuclear segmentation and classification scheme for automatic allred cancer scoring in immunohistochemical breast tissue images. Comput. Methods Programs Biomed. 2018, 165, 37–51. [Google Scholar] [CrossRef]
- Khalilabad, N.D.; Hassanpour, H. Employing image processing techniques for cancer detection using microarray images. Comput. Biol. Med. 2017, 81, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, S.; Helwan, A.; Uzun, D. Breast cancer image classification using artificial neural networks. Procedia Comput. Sci. 2017, 120, 126–131. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, S.; Henderson, L.M. Adaptive decision-making of breast cancer mammography screening: A heuristic based regression model. Omega 2018, 76, 70–84. [Google Scholar] [CrossRef]
- Mohebian, M.R.; Marateb, H.R.; Mansourian, M.; Mañanas, M.A.; Mokarian, F. A hybrid computer-aided-diagnosis system for prediction of breast cancer recurrence (HPBCR) using optimized ensemble learning. Comput. Struct. Biotechnol. J. 2017, 15, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Monday, H.N.; Li, J.; Nneji, G.U.; Hossin, M.A.; Nahar, S.; Jackson, J.; Chikwendu, I.A. WMR-DepthwiseNet: A Wavelet Multi-Resolution Depthwise Separable Convolutional Neural Network for COVID-19 Diagnosis. Diagnostics 2022, 12, 765. [Google Scholar] [CrossRef]
- Wang, P.; Song, Q.; Li, Y.; Lv, S.; Wang, J.; Li, L.; Zhang, H. Cross-task extreme learning machine for breast cancer image classification with deep convolutional features. Biomed. Signal Process. Control 2020, 57, 101789. [Google Scholar] [CrossRef]
- Kumar, A.; Singh, S.K.; Saxena, S.; Lakshmanan, K.; Sangaiah, A.K.; Chauhan, H.; Shrivastava, S.; Singh, R.K. Deep feature learning for histopathological image classification of canine mammary tumors and human breast cancer. Inf. Sci. 2020, 508, 405–421. [Google Scholar] [CrossRef]
- Kaur, P.; Singh, G.; Kaur, P. Intellectual detection and validation of automated mammogram breast cancer images by multi class SVM using deep learning classification. Inform. Med. Unlocked 2019, 16, 100151. [Google Scholar] [CrossRef]
- Ting, F.F.; Tan, Y.J.; Sim, K.S. Convolutional neural network improvement for breast cancer classification. Expert Syst. Appl. 2019, 120, 103–115. [Google Scholar] [CrossRef]
- Li, H.; Zhuang, S.; Li, D.; Zhao, J.; Ma, Y. Benign and malignant classification of mammogram images based on deep learning. Biomed. Signal Process. Control 2019, 51, 347–354. [Google Scholar] [CrossRef]
- Shen, L.; Margolies, L.R.; Rothstein, J.H.; Fluder, E.; McBride, R.; Sieh, W. Deep learning to improve breast cancer detection on screening mammography. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, M.; Chakraborty, C. Her2Net: A deep framework for semantic segmentation and classification of cell membranes and nuclei in breast cancer evaluation. IEEE Trans. Image Process. 2018, 27, 2189–2200. [Google Scholar] [CrossRef]
- Rustam, Z.; Amalia, Y.; Hartini, S.; Saragih, G.S. Linear discriminant analysis and support vector machines for classifying breast cancer. IAES Int. J. Artif. Intell. 2021, 10, 253–256. [Google Scholar] [CrossRef]
- Khan, S.; Islam, N.; Jan, Z.; Din, I.U.; Rodrigues, J.J.P.C. A novel deep learning based framework for the detection and classification of breast cancer using transfer learning. Pattern Recognit. Lett. 2019, 125, 1–6. [Google Scholar] [CrossRef]
- Spanhol, F.A.; Oliveira, L.S.; Petitjean, C.; Heutte, L. A dataset for breast cancer histopathological image classification. IEEE Trans. Biomed. Eng. 2015, 63, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Bayramoglu, N.; Kannala, J.; Heikkila, J. Deep learning for magnification independent breast cancer histopathology image classification. In Proceedings of the 2016 23rd International Conference on Pattern Recognition (ICPR), Cancun, Mexico, 4–8 December 2016; pp. 2440–2445. [Google Scholar]
- Spanhol, F.A.; Oliveira, L.S.; Petitjean, C.; Heutte, L. Breast cancer histopathological image classification using convolutional neural networks. In Proceedings of the 2016 International Joint Conference on Neural Networks OJCN, Vancouver, BC, Canada, 24–29 July 2016; pp. 2560–2567. [Google Scholar]
- Han, Z.; Wei, B.; Zheng, Y.; Yin, Y.; Li, K.; Li, S. Breast cancer multi-classification from histopathological images with structured deep learning model. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Alom, M.K.; Al-Hayani, W.; Algamal, Z.Y. Classification of breast cancer histopathology images based on adaptive sparse support vector machine. Appl. Math. Bioinform. 2017, 7, 49. [Google Scholar]
- Nneji, G.U.; Cai, J.; Deng, J.; Monday, H.N.; James, E.C.; Ukwuoma, C.C. Multi-Channel Based Image Processing Scheme for Pneumonia Identification. Diagnostics 2022, 12, 325. [Google Scholar] [CrossRef]
- Mgbejime, G.T.; Hossin, M.A.; Nneji, G.U.; Monday, H.N.; Ekong, F. Parallelistic Convolution Neural Network Approach for Brain Tumor Diagnosis. Diagnostics 2022, 12, 2484. [Google Scholar] [CrossRef]
- Hao, Y.; Zhang, L.; Qiao, S.; Bai, Y.; Cheng, R.; Xue, H.; Zhang, G. Breast cancer histopathological images classification based on deep semantic features and gray level co-occurrence matrix. PLoS ONE 2022, 17, e0267955. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Magnifying Factor | Benign | Malignant | Total |
|---|---|---|---|
| 40× | 625 | 1370 | 1995 |
| 100× | 644 | 1437 | 2081 |
| 200× | 623 | 1390 | 2013 |
| 400× | 588 | 1232 | 1820 |
| Sum Total | 2480 | 5429 | 7909 |
| Number of Patients | 24 | 58 | 82 |
| Classes | Sub-Classes | Patients Count | 40× | 100× | 200× | 400× | Total |
|---|---|---|---|---|---|---|---|
| Adenosis (A) | 4 | 114 | 113 | 111 | 106 | 444 | |
| Fibroadenoma (F) | 10 | 253 | 260 | 264 | 237 | 1014 | |
| Benign | Tubular Adenoma (TA) | 3 | 109 | 121 | 108 | 115 | 453 |
| Phyllodes Tumor (PT) | 7 | 149 | 150 | 140 | 130 | 569 | |
| Ductal Carcinoma (DC) | 38 | 864 | 903 | 896 | 788 | 3451 | |
| Malignant | Lobular Carcinoma (LC) | 5 | 156 | 170 | 163 | 137 | 626 |
| Mucinous Carcinoma (MC) | 9 | 205 | 222 | 196 | 169 | 792 | |
| Papillary Carcinoma (PC) | 6 | 145 | 142 | 135 | 138 | 560 | |
| Total | 82 | 1995 | 2081 | 2013 | 1820 | 7909 |
| Model | Binary Class | Multi-Class | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACC (%) | SEN (%) | SPE (%) | PRE (%) | AUC (%) | Time (min) | ACC (%) | SEN (%) | SPE (%) | PRE (%) | AUC (%) | Time (min) | |
| LWSC + Original images | 90.11 | 90.07 | 91.76 | 91.78 | 92.45 | 7.3 | 92.13 | 91.78 | 90.66 | 91.92 | 92.41 | 7.5 |
| LWSC + ED-based images | 91.76 | 92.18 | 90.82 | 91.65 | 92.55 | 5.8 | 93.71 | 92.62 | 91.09 | 92.85 | 93.16 | 5.9 |
| LWSC + CE-based images | 93.12 | 93.61 | 94.07 | 93.34 | 94.21 | 5.8 | 97.23 | 97.71 | 97.93 | 98.11 | 98.02 | 5.9 |
| State-of-the-Art Model | ACC (%) | AUC (%) | SPE (%) | SEN (%) | F1-Score (%) |
|---|---|---|---|---|---|
| Kumar et al. [18] | 93.0 | 95.0 | NR | NR | 94 |
| Kaur et al. [19] | 92.0 | 99.0 | 90.0 | 93.0 | 96.0 |
| Ting et al. [20] | 90.50 | 90.10 | 90.71 | 89.4 | NR |
| Rustam et al. [24] | 98.77 | NR | 97.64 | 96.44 | 99.0 |
| Spanhol et al. [26] | 85.0 | 86.1 | NR | NR | NR |
| Bayramoglu et al. [27] | 83.25 | NR | NR | NR | NR |
| Alom et al. [30] | 97.65 | 98.91 | 97.52 | 92.9 | NR |
| Hao et al. [33] | 96.75 | NR | 96.9 | 97.18 | NR |
| LWSC + CE-based images | 97.23 | 96.53 | 97.93 | 97.71 | 97.98 |
| Model | Binary Category | Multi-Class Category | ||||
|---|---|---|---|---|---|---|
| ACC | SEN | SPE | ACC | SEN | SPE | |
| AlexNet | 89.5 | 91.6 | 88.0 | 88.9 | 88.0 | 87.2 |
| VGG-16 | 95.2 | 96.3 | 94.9 | 96.4 | 97.1 | 96.0 |
| ResNet-101 | 93.9 | 94.5 | 94.1 | 94.5 | 95.0 | 93.2 |
| DenseNet-121 | 94.5 | 93.7 | 92.2 | 94.2 | 94.6 | 94.9 |
| Inception V3 | 97.3 | 97.8 | 97.0 | 95.8 | 96.0 | 95.3 |
| Xception | 91.9 | 92.6 | 89.6 | 91.3 | 92.8 | 90.7 |
| LWSC + CE-based images | 93.12 | 93.61 | 94.07 | 97.23 | 97.71 | 97.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nneji, G.U.; Monday, H.N.; Mgbejime, G.T.; Pathapati, V.S.R.; Nahar, S.; Ukwuoma, C.C. Lightweight Separable Convolution Network for Breast Cancer Histopathological Identification. Diagnostics 2023, 13, 299. https://doi.org/10.3390/diagnostics13020299
Nneji GU, Monday HN, Mgbejime GT, Pathapati VSR, Nahar S, Ukwuoma CC. Lightweight Separable Convolution Network for Breast Cancer Histopathological Identification. Diagnostics. 2023; 13(2):299. https://doi.org/10.3390/diagnostics13020299
Chicago/Turabian StyleNneji, Grace Ugochi, Happy Nkanta Monday, Goodness Temofe Mgbejime, Venkat Subramanyam R. Pathapati, Saifun Nahar, and Chiagoziem Chima Ukwuoma. 2023. "Lightweight Separable Convolution Network for Breast Cancer Histopathological Identification" Diagnostics 13, no. 2: 299. https://doi.org/10.3390/diagnostics13020299
APA StyleNneji, G. U., Monday, H. N., Mgbejime, G. T., Pathapati, V. S. R., Nahar, S., & Ukwuoma, C. C. (2023). Lightweight Separable Convolution Network for Breast Cancer Histopathological Identification. Diagnostics, 13(2), 299. https://doi.org/10.3390/diagnostics13020299