
The Neoplastic Side of the Abdominal Wall: A Comprehensive Pictorial Essay of Benign and Malignant Neoplasms

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Imaging Findings: Benign Neoplasms
2.1. Lipoma
2.2. Desmoid Tumors
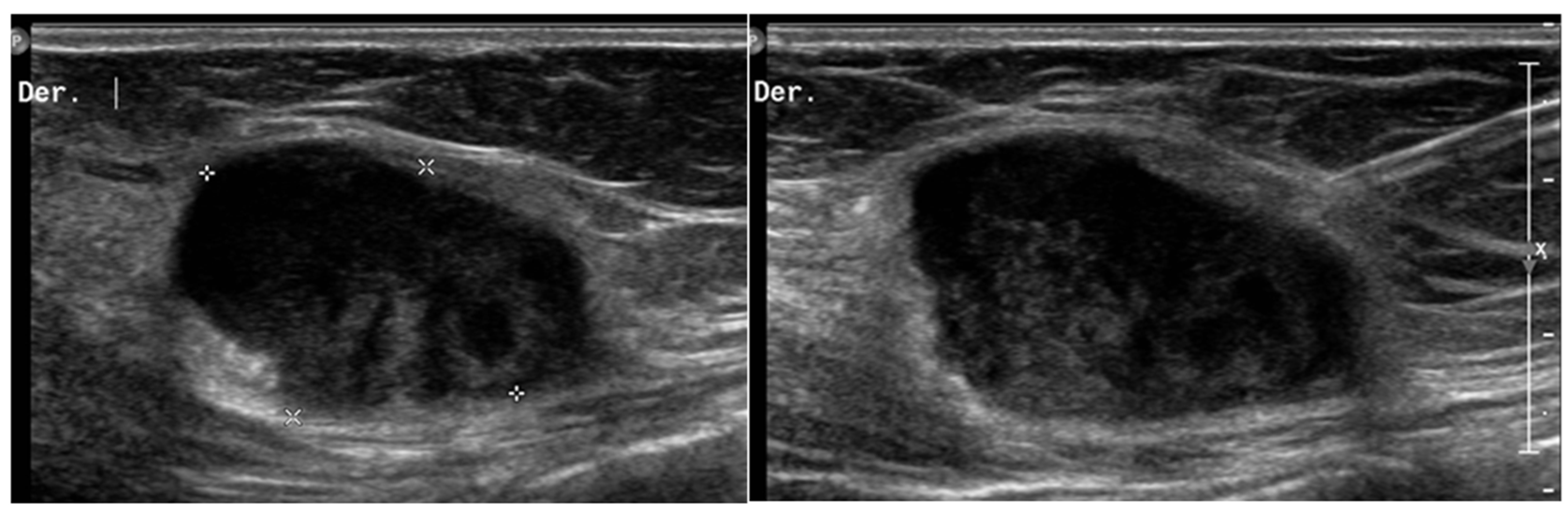
2.3. Hemangioma
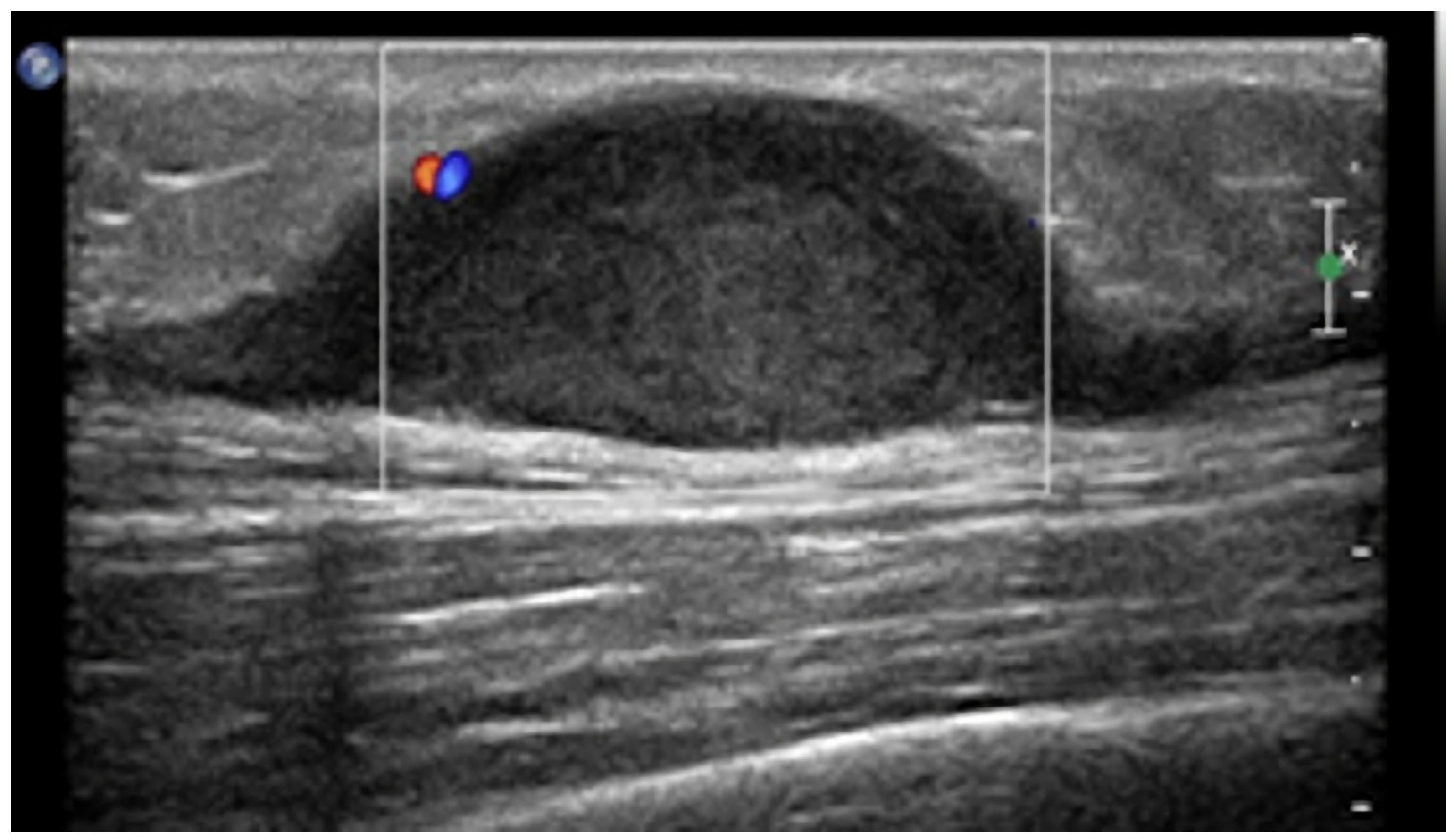
2.4. Nerve Sheath Tumors
3. Imaging Findings: Malignant Primary Neoplasms
3.1. Sarcomas
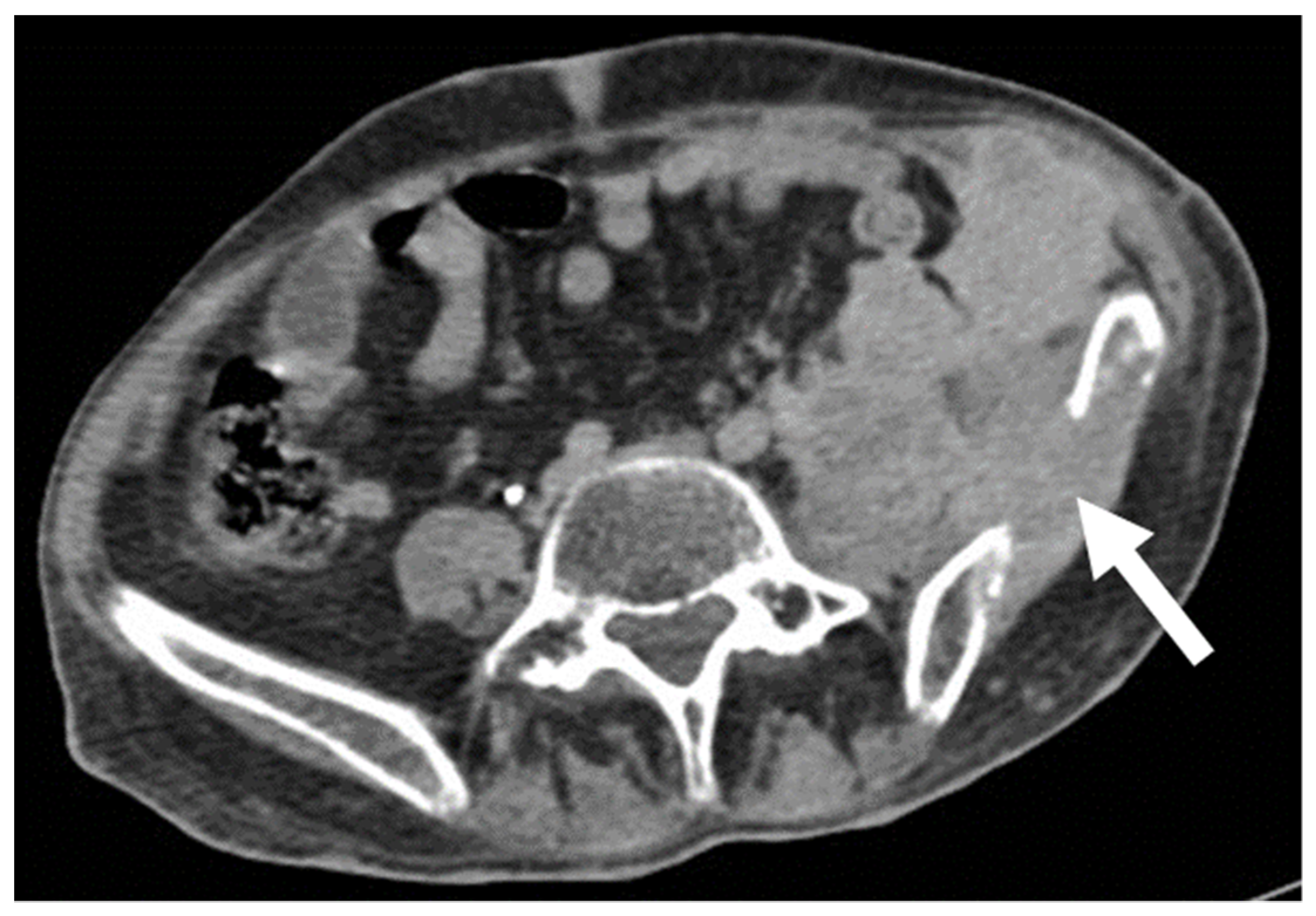
- Leiomyosarcomas: seen on the abdominal wall as either a primary process or as an extension of an intra-abdominal process [23,24]. Leiomyosarcomas demonstrate heterogeneous attenuation and signal intensity, with irregular peripheral enhancement and enhancing solid portions, mixed with hemorrhagic and necrotic areas [24]. Fatty components are absent (Figure 9) [23,24].
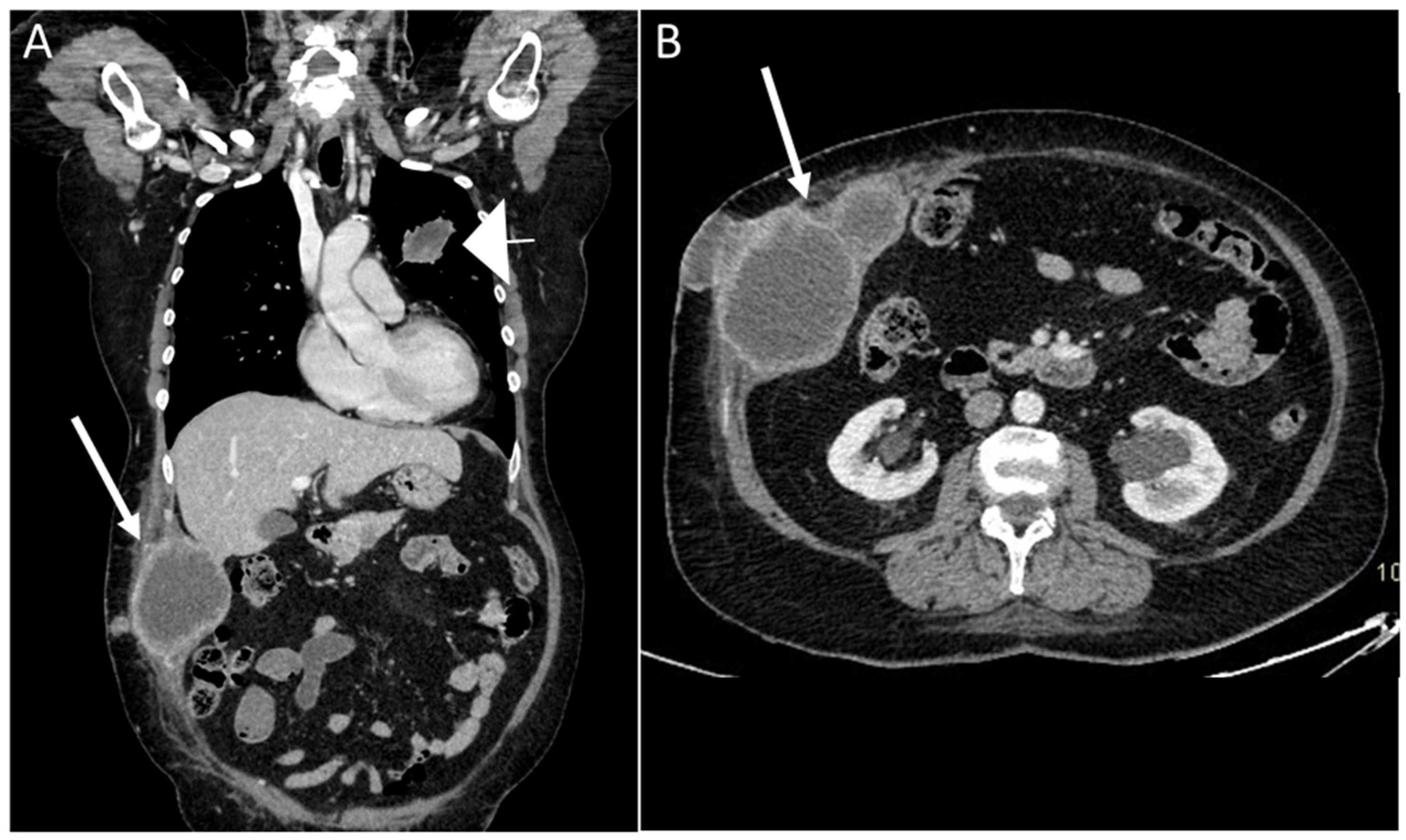
- Gastrointestinal Stromal Tumors (GIST): either primary (extraintestinal GIST, “EGIST”) [25,26] or secondary GIST of the abdominal wall are rare. When extended (>5 cm), GIST may have an aggressive behavior [25]. CT is the imaging modality of choice, showing heterogeneous vivid enhancement, and variable amount of necrosis. Peculiar findings include calcifications and cystic degeneration [27,28,29].
- Desmoplastic Small Round Cell Tumor (DSRCT): rare, highly aggressive sarcoma of adolescents, which primarily involves the serosal surfaces of the abdominal cavity infiltrating the abdominal wall [30,31,32]. Classic findings include bulky multiple, hypoattenuating, soft-tissue masses, with omental, serosal, and rectovesical involvement [31,32] and typical punctate or amorphous calcifications [32]. Modest heterogeneous enhancement is seen on arterial phase, without prolonged enhancement or portal washout [31,32] (Figure 10). On MR, DSRCTs are heterogeneously iso- to-hypointense on T1-w images, with hyperintense foci due to intratumoral hemorrhage [32].
3.2. Subcutaneous Lymphoma
3.3. Metastasis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bashir, U.; Moskovic, E.; Strauss, D.; Hayes, A.; Thway, K.; Pope, R.; Messiou, C. Soft-tissue masses in the abdominal wall. Clin. Radiol. 2014, 69, e422–e431. [Google Scholar] [CrossRef] [PubMed]
- Van Rijswijk, C.S.P.; Geirnaerdt, M.J.A.; Hogendoorn, P.; Taminiau, A.H.M.; Van Coevorden, F.; Zwinderman, A.H.; Pope, T.L.; Bloem, J.L. Soft-Tissue Tumors: Value of Static and Dynamic Gadopentetate Dimeglumine–enhanced MR Imaging in Prediction of Malignancy. Radiology 2004, 233, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Noebauer-Huhmann, I.M.; Weber, M.-A.; Lalam, R.K.; Trattnig, S.; Bohndorf, K.; Vanhoenacker, F.; Tagliafico, A.; Van Rijswijk, C.; Vilanova, J.C.; Afonso, P.D.; et al. Soft Tissue Tumors in Adults: ESSR-Approved Guidelines for Diagnostic Imaging. Semin. Musculoskelet. Radiol. 2015, 19, 475–482, correction in Semin. Musculoskelet. Radiol. 2015, 19, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhoenacker, F.M.; Parizel, P.M.; Gielen, J.L. Imaging of Soft Tissue Tumors, 3rd ed.; Springer: Berlin, Germany, 2017. [Google Scholar]
- Myhre-Jensen, O. A Consecutive 7-Year Series of 1331 Benign Soft Tissue Tumours: Clinicopathologic Data. Comparison with Sarcomas. Acta Orthop. 1981, 52, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Toirkens, J.; De Schepper, A.M.; Vanhoenacker, F.; Van Dyck, P.; Gielen, J.; Creytens, D.; Wouters, K.; Eiber, M.; Wörtler, K.; Parizel, P.M. A comparison between histopathology and findings on magnetic resonance imaging of subcutaneous lipomatous soft-tissue tumors. Insights Imaging 2011, 2, 599–607. [Google Scholar] [CrossRef] [Green Version]
- Ballard, D.H.; Mazaheri, P.; Oppenheimer, D.C.; Lubner, M.G.; Menias, C.O.; Pickhardt, P.J.; Middleton, W.D.; Mellnick, V.M. Imaging of Abdominal Wall Masses, Masslike Lesions, and Diffuse Processes. Radiographics 2020, 40, 684–706. [Google Scholar] [CrossRef]
- Virmani, V.; Sethi, V.; Fasih, N.; Ryan, J.; Kielar, A. The Abdominal Wall Lumps and Bumps: Cross-Sectional Imaging Spectrum. Can. Assoc. Radiol. J. 2014, 65, 9–18. [Google Scholar] [CrossRef]
- Gaskin, C.M.; Helms, C.A. Lipomas, Lipoma Variants, and Well-Differentiated Liposarcomas (Atypical Lipomas): Results of MRI Evaluations of 126 Consecutive Fatty Masses. Am. J. Roentgenol. 2004, 182, 733–739. [Google Scholar] [CrossRef]
- Kucharz, E.J.; Kopeć-Mędrek, M.; Kramza, J.; Chrzanowska, M.; Kotyla, P. Dercum’s disease (Adiposis dolorosa): A review of clinical presentation and management. Rheumatology 2019, 57, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Stein, L.; Elsayes, K.M.; Wagner-Bartak, N. Subcutaneous Abdominal Wall Masses: Radiological Reasoning. Am. J. Roentgenol. 2012, 198, W146–W151. [Google Scholar] [CrossRef]
- Vandevenne, J.E.; De Schepper, A.M.; De Beuckeleer, L.; Van Marck, E.; Aparisi, F.; Bloem, J.L.; Erkorkmaz, Z.; Brijs, S. New concepts in understanding evolution of desmoid tumors: MR imaging of 30 lesions. Eur. Radiol. 1997, 7, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.E.; Park, S.J.; Moon, S.K.; Lee, D.H.; Lim, J.W. Sonography of Abdominal Wall Masses and Masslike Lesions: Correlation with Computed Tomography and Magnetic Resonance Imaging. J. Ultrasound Med. 2016, 35, 189–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desmoid Tumor Working Group. The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients. Eur. J. Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Penel, N.; Le Cesne, A.; Bonvalot, S.; Giraud, A.; Bompas, E.; Rios, M.; Salas, S.; Isambert, N.; Boudou-Rouquette, P.; Honore, C.; et al. Surgical versus non-surgical approach in primary desmoid-type fibromatosis patients: A nationwide prospective cohort from the French Sarcoma Group. Eur. J. Cancer 2017, 83, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.P.; Dubhashi, S.P.; Choudhary, K. Anterior Abdominal Wall Haemangioma with Inguinal Extension. J. Clin. Diagn. Res. 2014, 8, ND15–ND16. [Google Scholar] [CrossRef] [PubMed]
- Saad, D.F.; Shehata, B.M.; Patrick, E.; Gow, K.W. Intramuscular hemangioma of the abdominal wall. J. Pediatr. Surg. 2006, 41, 601–602. [Google Scholar] [CrossRef]
- Morrow, M.S.; Oliveira, A.M. Imaging of Lumps and Bumps in Pediatric Patients: An Algorithm for Appropriate Imaging and Pictorial Review. Semin. Ultrasound CT MRI 2014, 35, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, P.; Vanhoenacker, F.M.; Vogel, J.; Venstermans, C.; Kroon, H.M.; Gielen, J.; Parizel, P.M.; Bloem, J.L.; De Schepper, A.M.A. Prevalence, extension and characteristics of fluid-fluid levels in bone and soft tissue tumors. Eur. Radiol. 2006, 16, 2644–2651. [Google Scholar] [CrossRef]
- Wierzbicki, J.M.; Henderson, J.H.; Scarborough, M.T.; Bush, C.H.; Reith, J.D.; Clugston, J.R. Intramuscular Hemangiomas. Sports Health A Multidiscip. Approach 2012, 5, 448–454. [Google Scholar] [CrossRef]
- Vanhoenacker, F.M.; Van Looveren, K.; Trap, K.; Desimpelaere, J.; Wouters, K.; Van Dyck, P.; Parizel, P.M.; De Schepper, A.M. Grading and characterization of soft tissue tumors on magnetic resonance imaging: The value of an expert second opinion report. Insights Imaging 2012, 3, 131–138. [Google Scholar] [CrossRef]
- Lam, R.; Hunt, B.L.; Arreola-Owen, O. Abdominal Wall Schwannoma. Fed. Prac. 2019, 36, 129–133. [Google Scholar]
- Levy, A.D.; Manning, M.A.; Al-Refaie, W.B.; Miettinen, M.M. Soft-Tissue Sarcomas of the Abdomen and Pelvis: Radiologic-Pathologic Features, Part 1—Common Sarcomas: From the Radiologic Pathology Archives. Radiographics 2017, 37, 462–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eken, H.; Karagul, S.; Topgül, K.; Yoruker, S.; Ozen, N.; Gun, S.; Balci, M.G.; Somuncu, E.; Cimen, O.; Soyturk, M.; et al. Giant Cutaneous Leiomyosarcoma Originating from the Abdominal Wall: A Case Report. Am. J. Case Rep. 2016, 17, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reith, J.D.; Goldblum, J.R.; Lyles, R.H.; Weiss, S.W. Extragastrointestinal (Soft Tissue) Stromal Tumors: An Analysis of 48 Cases with Emphasis on Histologic Predictors of Outcome. Mod. Pathol. 2000, 13, 577–585. [Google Scholar] [CrossRef] [Green Version]
- Alkhatib, L.; Albtoush, O.; Bataineh, N.; Gharaibeh, K.; Matalka, I.; Tokuda, Y. Extragastrointestinal Stromal Tumor (EGIST) in the abdominal wall: Case report and literature review. Int. J. Surg. Case Rep. 2011, 2, 253–255. [Google Scholar] [CrossRef] [Green Version]
- Cannella, R.; Tabone, E.; Porrello, G.; Cappello, G.; Gozzo, C.; Incorvaia, L.; Grignani, G.; Merlini, A.; D’Ambrosio, L.; Badalamenti, G.; et al. Assessment of morphological CT imaging features for the prediction of risk stratification, mutations, and prognosis of gastrointestinal stromal tumors. Eur. Radiol. 2021, 31, 8554–8564. [Google Scholar] [CrossRef]
- Cannella, R.; La Grutta, L.; Midiri, M.; Bartolotta, T.V. New advances in radiomics of gastrointestinal stromal tumors. World J. Gastroenterol. 2020, 26, 4729–4738. [Google Scholar] [CrossRef]
- Vernuccio, F.; Taibbi, A.; Picone, D.; La Grutta, L.; Midiri, M.; Lagalla, R.; Re, G.L.; Bartolotta, T.V. Imaging of Gastrointestinal Stromal Tumors: From Diagnosis to Evaluation of Thera-peutic Response. Anticancer Res. 2016, 36, 2639–2648. [Google Scholar]
- Stiles, Z.E.; Dickson, P.V.; Glazer, E.S.; Murphy, A.J.; Davidoff, A.M.; Behrman, S.W.; Bishop, M.W.; Martin, M.G.; Deneve, J.L. Desmoplastic small round cell tumor: A nationwide study of a rare sarcoma. J. Surg. Oncol. 2018, 117, 1759–1767. [Google Scholar] [CrossRef]
- Bellah, R.; Suzuki-Bordalo, L.; Brecher, E.; Ginsberg, J.P.; Maris, J.; Pawel, B.R. Desmoplastic Small Round Cell Tumor in the Abdomen and Pelvis: Report of CT Findings in 11 Affected Children and Young Adults. Am. J. Roentgenol. 2005, 184, 1910–1914. [Google Scholar] [CrossRef]
- Morani, A.C.; Bathala, T.K.; Surabhi, V.R.; Yedururi, S.; Jensen, C.T.; Huh, W.W.; Prasad, S.; Hayes-Jordan, A. Desmoplastic Small Round Cell Tumor: Imaging Pattern of Disease at Presentation. Am. J. Roentgenol. 2019, 212, W45–W54. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef] [PubMed]
- Vanhoenacker, F.M.; Baten, A.; Vandeputte, V. Imaging findings of a cutaneous B-cell lymphoma. J. Belg. Soc. Radiol. 2010, 92, 285–288. [Google Scholar]
- Ataseven, B.; du Bois, A.; Harter, P.; Prader, S.; Grimm, C.; Kurzeder, C.; Schneider, S.; Heikaus, S.; Kahl, A.; Traut, A.; et al. Impact of Abdominal Wall Metastases on Prognosis in Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2016, 26, 1594–1600. [Google Scholar] [CrossRef] [PubMed]
- Wichtowski, M.; Murawa, D.; Czarnecki, R.; Piechocki, J.; Nowecki, Z.; Witkiewicz, W. Electrochemotherapy in the Treatment of Breast Cancer Metastasis to the Skin and Subcutaneous Tissue—Multicenter Experience. Oncol. Res. Treat. 2018, 42, 47–51. [Google Scholar] [CrossRef]
- Heitz, F.; Ognjenovic, D.; Harter, P.; Kommoss, S.; Ewald-Riegler, N.; Haberstroh, M.; Gomez, R.; Barinoff, J.; Traut, A.; Du Bois, A. Abdominal Wall Metastases in Patients with Ovarian Cancer After Laparoscopic Surgery: Incidence, risk factors, and complications. Int. J. Gynecol. Cancer 2010, 20, 41–46. [Google Scholar] [CrossRef]
- Zhong, G.-B.; Ye, X.-Q.; Liu, J.-L.; Xiao, S.-Z.; Huang, Q.-H.; Wei, W. Male accessory breast cancer on the abdominal wall: A case report and literature review. OncoTargets Ther. 2018, 11, 6625–6631. [Google Scholar] [CrossRef] [Green Version]
- Garrido, M.J.M.; Ponce, C.G.; Martínez, J.L.S.; Sevila, C.M.Y.; Mena, A.C.; Antón, F.M. Cutaneous metastases of lung cancer. Clin. Transl. Oncol. 2006, 8, 330–333. [Google Scholar] [CrossRef]
- Attar, L.; Trabulsi, N.; Maghrabi, A.; Nassif, M. Adenocarcinoma of the Colon Disguised as Abdominal Wall Abscess: Case Report and Review of the Literature. Case Rep. Surg. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Shin, H.C.; Kim, I.Y.; Kim, Y.T.; Kim, C.-J. CT Findings of Colonic Complications Associated with Colon Cancer. Korean J. Radiol. 2010, 11, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Coll, D.M.; Meyer, J.M.; Mader, M.; Smith, R.C. Imaging appearances of Sister Mary Joseph nodule. Br. J. Radiol. 1999, 72, 1230–1233. [Google Scholar] [CrossRef]
- Petch, S.; Sobota, A.; Abu Saadeh, F. Sister Mary Joseph nodule: An unusual site for endometrioid cancer metastasis. BMJ Case Rep. 2019, 12, e229187. [Google Scholar] [CrossRef]
- Ben Kridis, W.; Werda, I.; Khanfir, A. Pancreatic Carcinoma Discovered by Sister Mary Joseph’s Nodules. Clin. Gastroenterol. Hepatol. 2018, 18, A38. [Google Scholar] [CrossRef] [PubMed]
- De Angeli, M.; Carosi, M.; Vizza, E.; Corrado, G. Sister Mary Joseph’s nodule in endometrial cancer: A case report and review of the literature. J. Cancer Res. Ther. 2019, 15, 1408. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.-L.; Zhang, Q.; Masood, W.; Masood, N.; Tang, Y.; Cao, C.-H.; Fu, Q.-H.; Zhang, Y.; Gao, S.-L.; Liang, T.-B. Sister Mary Joseph’s nodule as a first sign of pancreatic cancer. World J. Gastroenterol. 2012, 18, 6686–6689. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Findings—Benign Neoplasms | |||
|---|---|---|---|
| Lesion | Ultrasounds (US) | Computed Tomography (CT) | Magnetic Resonance (MRI) |
| Lipoma |
|
|
|
| Desmoid Tumors |
|
|
|
| Hemangioma |
|
|
|
| Nerve Sheath Tumors |
|
|
|
| Imaging Findings—Malignant Neoplasms | |||
|---|---|---|---|
| Lesion | Ultrasounds (US) | Computed Tomography (CT) | Magnetic Resonance (MRI) |
| Malignant Schwannoma |
|
|
|
| Sarcomas | |||
| Liposarcomas |
|
|
|
| Leiomyosarcomas |
|
|
|
| GIST |
|
|
|
| DSRCT |
|
| |
| Subcutaneous Lymphoma |
|
|
|
| Metastasis | Mirroring imaging characteristics of primary tumor: usually solid masses with target appearance and rim vascularization, with DWI restriction on MRI. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porrello, G.; Cannella, R.; Alvarez-Hornia Pérez, E.; Brancatelli, G.; Vernuccio, F. The Neoplastic Side of the Abdominal Wall: A Comprehensive Pictorial Essay of Benign and Malignant Neoplasms. Diagnostics 2023, 13, 315. https://doi.org/10.3390/diagnostics13020315
Porrello G, Cannella R, Alvarez-Hornia Pérez E, Brancatelli G, Vernuccio F. The Neoplastic Side of the Abdominal Wall: A Comprehensive Pictorial Essay of Benign and Malignant Neoplasms. Diagnostics. 2023; 13(2):315. https://doi.org/10.3390/diagnostics13020315
Chicago/Turabian StylePorrello, Giorgia, Roberto Cannella, Eduardo Alvarez-Hornia Pérez, Giuseppe Brancatelli, and Federica Vernuccio. 2023. "The Neoplastic Side of the Abdominal Wall: A Comprehensive Pictorial Essay of Benign and Malignant Neoplasms" Diagnostics 13, no. 2: 315. https://doi.org/10.3390/diagnostics13020315
APA StylePorrello, G., Cannella, R., Alvarez-Hornia Pérez, E., Brancatelli, G., & Vernuccio, F. (2023). The Neoplastic Side of the Abdominal Wall: A Comprehensive Pictorial Essay of Benign and Malignant Neoplasms. Diagnostics, 13(2), 315. https://doi.org/10.3390/diagnostics13020315