

Prevalence of the Bifid Mandibular Condyle and Its Relationship with Pathologies of the Temporomandibular Joint: A Systematic Review and Meta-Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Electronic Search
2.4. Study Selection
2.5. Data Collection Process
2.6. Assessment of the Methodological Quality of the Included Studies
2.7. Statistical Methods
3. Results
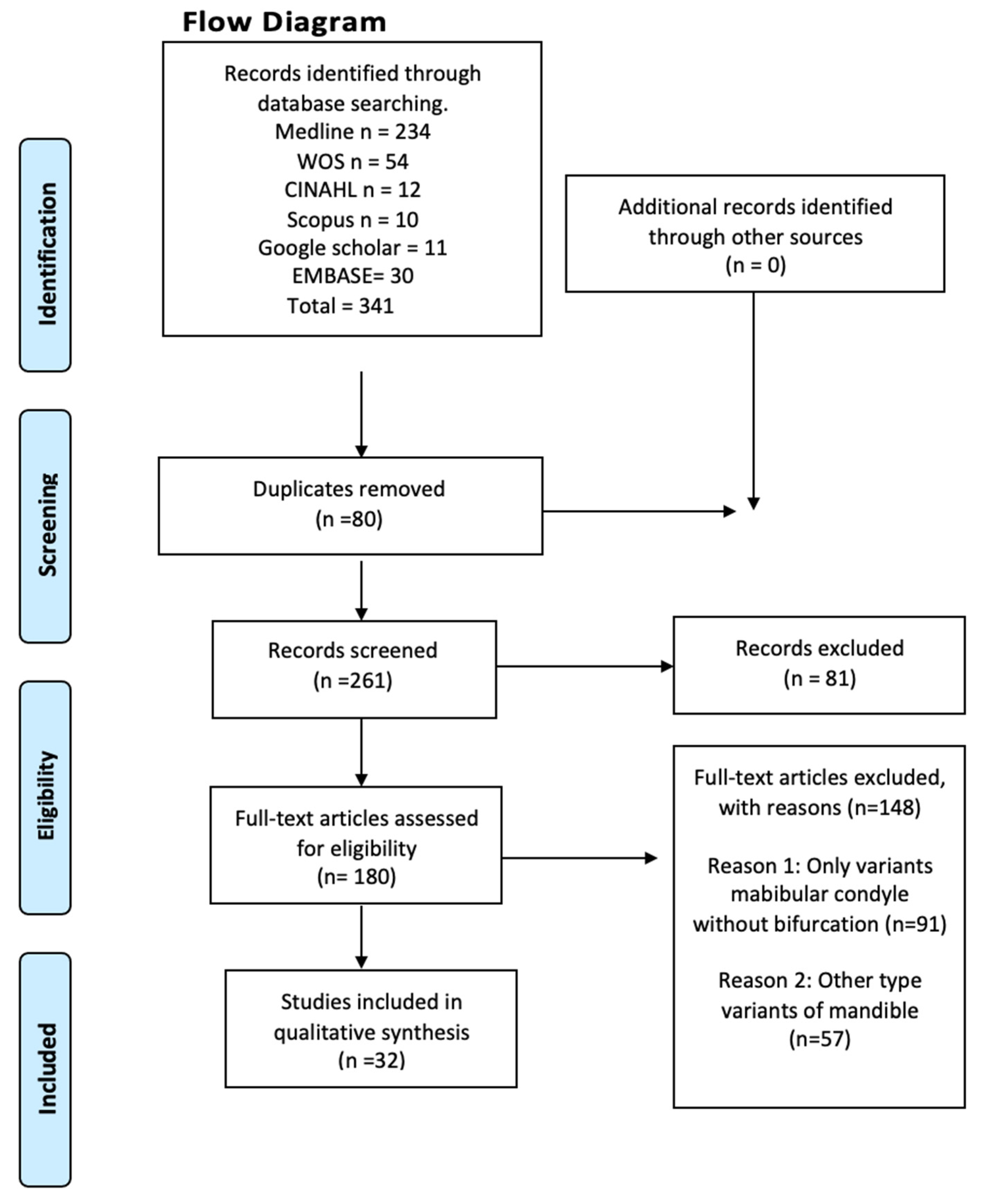
3.1. Included Articles
3.2. Characteristics of the Studies and the Study Population
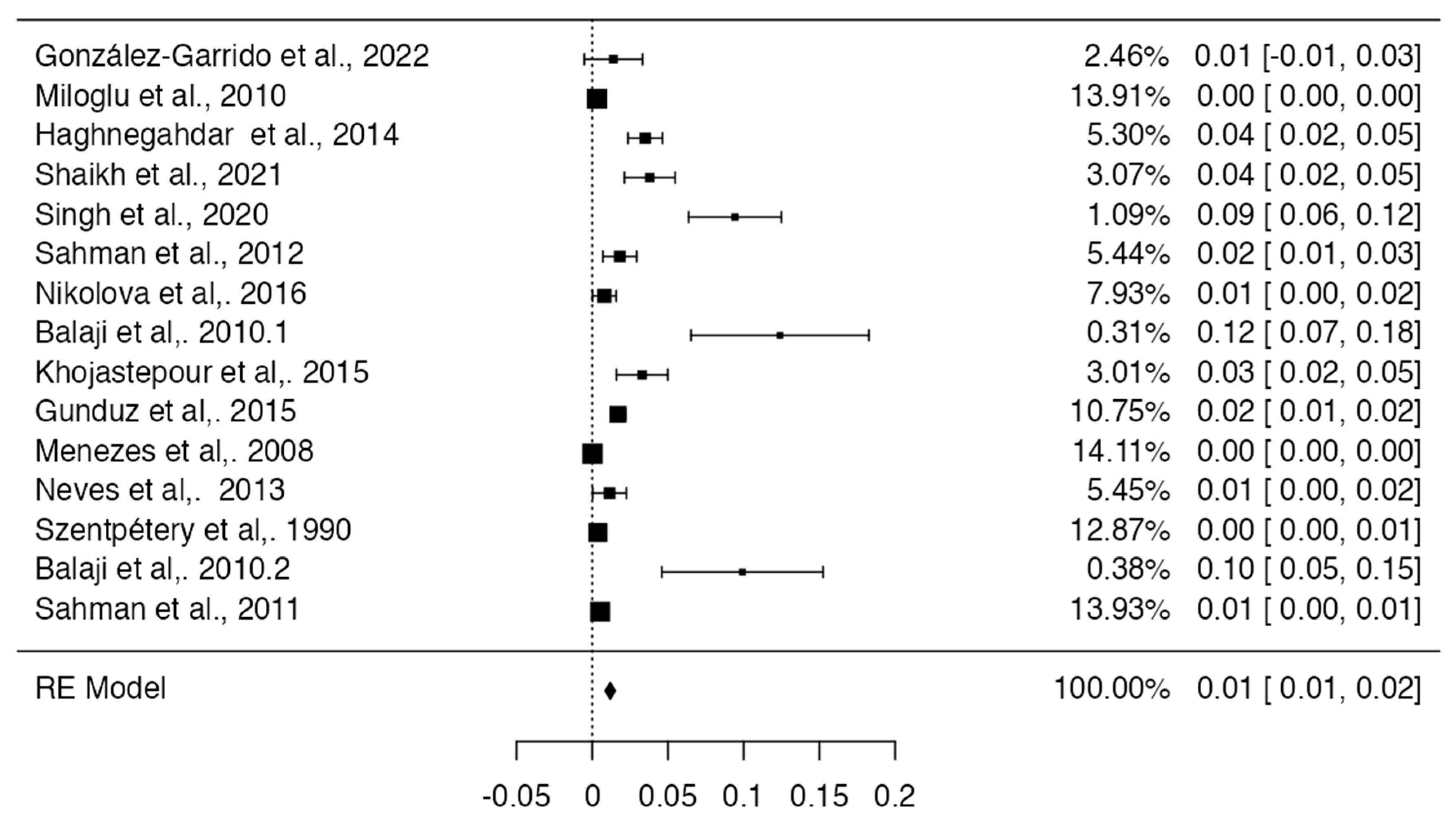
3.3. Prevalence and Risk of Bias
3.4. Clinical Implications
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kendirci, M.; Göksel, S.; Özcan, İ. Multiheaded mandibular condyles. J. Orofac. Orthop. 2023, 84 (Suppl. S3), 165–171. [Google Scholar] [CrossRef]
- Bettoni, J.; Olivetto, M.; Bouaoud, J.; Duisit, J.; Dakpé, S. Bilateral bifid condyles: A rare etiology of temporomandibular joint disorders. Cranio 2021, 39, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Antoniades, K.; Karakasis, D.; Elephtheriades, J. Bifid mandibular condyle resulting from a sagittal fracture of the condylar head. Br. J. Oral. Maxillofac. Surg. 1993, 31, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.F.; Ferguson, M.M. Bifid mandibular condyle. Dentomaxillofac. Radiol. 1997, 26, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Loh, F.C.; Yeo, J.F. Bifid mandibular condyle. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 24–27. [Google Scholar] [CrossRef]
- Antoniades, K.; Hadjipetrou, L.; Antoniades, V.; Paraskevopoulos, K. Bilateral bifid mandibular condyle. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2004, 97, 535–538. [Google Scholar] [CrossRef]
- Hersek, N.; Ozbek, M.; Taşar, F.; Akpinar, E.; Firat, M. Bifid mandibular condyle: A case report. Dent. Traumatol. 2004, 20, 184–186. [Google Scholar] [CrossRef]
- Balciunas, B.A. Bifid mandibular condyle. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1986, 44, 324–325. [Google Scholar] [CrossRef]
- Nagpal, A.; Vaddi, A.; Tadinada, A. Shifting the Spotlight From the Mandibular Condyle to the Coronoid Process: A Report of a Unique Case of Trifid Mandibular Coronoid Process. Cureus 2023, 15, e37593. [Google Scholar] [CrossRef]
- Plevnia, J.R.; Smith, J.A.; Stone, C.G. Bifid mandibular condyle without history of trauma or pain: Report of a case. J. Oral Maxillofac. Surg. 2009, 67, 1555–1561. [Google Scholar] [CrossRef]
- Shriki, J.; Lev, R.; Wong, B.F.; Sundine, M.J.; Hasso, A.N. Bifid mandibular condyle: CT and MR imaging appearance in two patients: Case report and review of the literature. AJNR Am. J. Neuroradiol. 2005, 26, 1865–1868. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Jordan, Z.; Lockwood, C.; Munn, Z.; Aromataris, E. Redeveloping the JBI Model of Evidence Based Healthcare. Int. J. Evid. Based Healthc. 2018, 16, 227–241. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, Version 4.0; Computer Software; R Packages Retrieved from MRAN Snapshot 2021-04-01; R Core Team: Vienna, Austria, 2021. Available online: https://cran.r-project.org(accessed on 18 October 2023).
- Henry, B.M.; Tomaszewski, K.A.; Walocha, J.A. Methods of Evidence-Based Anatomy: A guide to conducting systematic reviews and meta-analysis of anatomical studies. Ann. Anat. 2016, 205, 16–21. [Google Scholar] [CrossRef]
- González-Garrido, L.; Gómez-González, S.; Gonzalo-Orden, J.M.; Wasterlain, S.N. Multi-headed (bifid and trifid) mandibular condyles in archaeological contexts: Two posttraumatic cases. Arch. Oral Biol. 2022, 134, 105326. [Google Scholar] [CrossRef] [PubMed]
- Miloglu, O.; Yalcin, E.; Buyukkurt, M.; Yilmaz, A.; Harorli, A. The frequency of bifid mandibular condyle in a Turkish patient population. Dentomaxillofac. Radiol. 2010, 39, 42–46. [Google Scholar] [CrossRef]
- Neelakandan, R.S.; Bhargava, D. Bifid hyperplastic mandibular condyle. J. Maxillofac. Oral Surg. 2013, 12, 466–471. [Google Scholar] [CrossRef]
- Prol, C.; Álvarez, J.; Mendiola, J. Bilateral bifid mandibular condyle. Acta Otorrinolaringol. Esp. (Engl. Ed.) 2017, 68, 303–304, (In English and Spanish). [Google Scholar] [CrossRef]
- Rajashri, P.; Kumar, S.P. Bifid Mandibular Condyle as the Hidden Cause for Temporomandibular Joint Disorder. Cureus 2021, 13, e17609. [Google Scholar] [CrossRef]
- Tutar, O.; Bas, A.; Gülsen, G.; Bayraktarov, E. Bifid mandibular condyle: CT and MRI appearance. BMJ Case Rep. 2012, 2012, bcr2012006976. [Google Scholar] [CrossRef]
- Haghnegahdar, A.A.; Bronoosh, P.; Khojastepour, L.; Tahmassebi, P. Prevalence of bifid mandibular condyle in a selected population in South of iran. J. Dent. 2014, 15, 156–160. [Google Scholar]
- Shaikh, A.H.; Ahmed, S.; Ahmed, A.R.; Das, G.; Taqi, M.; Nisar, S.; Khan, O. Assessment of radiographic morphology of mandibular condyles: A radiographic study. Folia Morphol. 2022, 81, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Kumar, N.R.; Balan, A.; Nishan, M.; Haris, P.S.; Jinisha, M.; Denny, C.D. Evaluation of Normal Morphology of Mandibular Condyle: A Radiographic Survey. J. Clin. Imaging Sci. 2020, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Sahman, H.; Sisman, Y.; Sekerci, A.E.; Tarim-Ertas, E.; Tokmak, T.; Tuna, I.S. Detection of bifid mandibular condyle using computed tomography. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e930–e934. [Google Scholar] [CrossRef] [PubMed]
- Rehman, T.A.; Gibikote, S.; Ilango, N.; Thaj, J.; Sarawagi, R.; Gupta, A. Bifid mandibular condyle with associated temporomandibular joint ankylosis: A computed tomography study of the patterns and morphological variations. Dentomaxillofac. Radiol. 2009, 38, 239–244. [Google Scholar] [CrossRef]
- Nikolova, S.Y.; Toneva, D.H.; Lazarov, N.E. Incidence of a Bifid Mandibular Condyle in Dry Mandibles. J. Craniofac. Surg. 2017, 28, 2168–2173. [Google Scholar] [CrossRef]
- Faisal, M.; Ali, I.; Pal, U.S.; Bannerjee, K. Bifid mandibular condyle: Report of two cases of varied etiology. Natl. J. Maxillofac. Surg. 2010, 1, 78–80. [Google Scholar] [CrossRef]
- Melo, S.L.; Melo, D.P.; Oenning, A.C.; Haiter-Neto, F.; Almeida, S.M.; Campos, P.S. Magnetic resonance imaging findings of true bifid mandibular condyle with duplicated mandibular fossa. Clin. Anat. 2012, 25, 650–655. [Google Scholar] [CrossRef]
- Lee, J.S.; Xi, T.; Kwon, T.G. Three-dimensional analysis of mandibular condyle position in patients with deviated mandibular prognathism. Int. J. Oral Maxillofac. Surg. 2017, 46, 1052–1058. [Google Scholar] [CrossRef]
- Balaji, S.M. Bifid mandibular condyle: A study of the clinical features, patterns and morphological variations using CT scans. J. Maxillofac. Oral Surg. 2010, 9, 38–41. [Google Scholar] [CrossRef]
- Khojastepour, L.; Kolahi, S.; Panahi, N.; Haghnegahdar, A. Cone Beam Computed Tomographic Assessment of Bifid Mandibular Condyle. J. Dent. 2015, 12, 868–873. [Google Scholar]
- Gyoon, K.; Jeong, Y.H.; Kosel, E.; Agnew, A.M.; McComb, D.W.; Bodnyk, K.; Hart, R.T.; Kim, M.K.; Han, S.Y.; Johnston, W.M. Regional variation of bone tissue properties at the human mandibular condyle. Bone 2015, 77, 98–106. [Google Scholar] [CrossRef]
- Michalski, C.D.; Pollizzi, A.; Dhar, D.; Hayes, L.L.; Chandra, T. Bifid Mandibular Condyle with Associated Temporomandibular Joint Ankylosis: A Rare Skeletal Abnormality. Cureus 2022, 14, e29624. [Google Scholar] [CrossRef] [PubMed]
- Menezes, A.V.; de Moraes Ramos, F.M.; de Vasconcelos-Filho, J.O.; Kurita, L.M.; de Almeida, S.M.; Haiter-Neto, F. The prevalence of bifid mandibular condyle detected in a Brazilian population. Dentomaxillofac. Radiol. 2008, 37, 220–223. [Google Scholar] [CrossRef]
- Neves, F.; Ramirez, L.; Roque, R.; Lopes, G.; Haiter, F.; Queiroz, D. Detection of bifid mandibular condyle by panoramic radiography and cone beam computed tomography. J. Braz. Oral Sci. 2013, 12, 133–139. [Google Scholar]
- Szentpétery, A.; Kocsis, G.; Marcsik, A. The problem of the bifid mandibular condyle. J. Oral Maxillofac. Surg. 1990, 48, 1254–1257. [Google Scholar] [CrossRef]
- Balaji, S.M. Bifid mandibular condyle with tempromandibular joint ankylosis—A pooled data analysis. Dent. Traumatol. 2010, 26, 332–337. [Google Scholar] [CrossRef]
- Sahman, H.; Sekerci, A.E.; Ertas, E.T.; Etoz, M.; Sisman, Y. Prevalence of bifid mandibular condyle in a Turkish population. J. Oral Sci. 2011, 53, 433–437. [Google Scholar] [CrossRef]
- Varun, A.; Suhas, S.; Pai, K.M.; Shetty, C.M.; Auluck, A. Bifid mandibular condyles: Report of four cases. Dent. Update 2006, 33, 368–370. [Google Scholar] [CrossRef]
- Alpaslan, S.; Ozbek, M.; Hersek, N.; Kanli, A.; Avcu, N.; Firat, M. Bilateral bifid mandibular condyle. Dentomaxillofac. Radiol. 2004, 33, 274–277. [Google Scholar] [CrossRef]
- Katti, G.; Najmuddin, M.; Fatima, S.; Unnithan, J. Bifid mandibular condyle. BMJ Case Rep. 2012, 2012, bcr-2012-007051. [Google Scholar] [CrossRef]
- Sreenivasagan, S.; George, A.M.; Rengalakshmi, S. Variation in condylar morphology in different malocclusion among Indians. Bioinformation 2021, 17, 1134–1137. [Google Scholar] [CrossRef]
- Schmitter, M.; Gabbert, O.; Ohlmann, B.; Hassel, A.; Wolff, D.; Rammelsberg, P.; Kress, B. Assessment of the reliability and validity of panoramic imaging for assessment of mandibular condyle morphology using both MRI and clinical examination as the gold standard. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Pérez, S.; Vázquez-Delgado, E.; Rodríguez-Baeza, A.; Gay-Escoda, C. Bifid mandibular condyle: A disorder in its own right? J. Am. Dent. Assoc. 2010, 141, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Anzola, F.L.K.; Moron, A.S.; Jaramillo, C.M.C.; Quijano, G.D.C.; Hernandez, H.N.; González, A.E.; Rodriguez, I.; Moreno, L.S.M.; Amador, P.E.; Orozco, F.M.; et al. Quantitative bone SPECT analysis of mandibular condyles in an asymptomatic population: An approach to normal reference values. Int. J. Oral Maxillofac. Surg. 2021, 50, 733–739. [Google Scholar] [CrossRef]
- Gunduz, K.; Buyuk, C.; Egrioglu, E. Evaluación de la Prevalencia de Cóndilo Mandibular Bífido Detectado en Tomografía Computadorizada Cone-Beam en una Población Turca. Int. J. Morphol. 2015, 1, 43–47. [Google Scholar] [CrossRef]
- Borrás-Ferreres, J.; Sánchez-Torres, A.; Gay-Escoda, C. Bifid mandibular condyles: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e672–e680. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, K.A.; Mai, P.T.; Hogge, M.; Choi, E.Y.; Portnof, J.E. Bifid Mandibular Canal: A Case Review and Retrospective Review of CBCTs. Implant Dent. 2018, 27, 682–686. [Google Scholar] [CrossRef]
- López-López, J.; Ayuso-Montero, R.; Salas, E.J.; Roselló-Llabrés, X. Bifid condyle: Review of the literature of the last 10 years and report of two cases. Cranio 2010, 28, 136–140. [Google Scholar] [CrossRef]
- Ayat, A.; Boudaoud, Z.; Djafer, L. Trifid mandibular condyle: A case report and literature review. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 601–604. [Google Scholar] [CrossRef]
- Vervaeke, K.; Verhelst, P.J.; Orhan, K.; Lund, B.; Benchimol, D.; Van der Cruyssen, F.; De Laat, A.; Jacobs, R.; Politis, C. Correlation of MRI and arthroscopic findings with clinical outcome in temporomandibular joint disorders: A retrospective cohort study. Head Face Med. 2022, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, N.; Zhang, C.; Xu, F.; Chen, T.; Shen, G.; Si, J.; Yu, H. Evaluation of optimal single-photon emission computed tomography reference value and three-dimensional mandibular growth pattern in 54 Chinese unilateral condylar hyperplasia patients. Head Face Med. 2023, 19, 18. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Type Study and N | Prevalence and Characteristics of Subjects | Static Values | Region | Sex of Samples | Laterality | Clinical Considerations |
|---|---|---|---|---|---|---|---|
| González-Garrido et al., 2022 [16] | Adult mandibles and cranial bone (143) | Two (1.4%) mandibles with both condyles exhibit multi-headed condyle | No present static values | Spain | 141 sex unknown; 1 female; 1 male | Unilateral | Both cases of the present study are post-traumatic, no deterioration was identified, severe mandibular use or malfunction, with temporomandibular joint osteoarthritis and eversion of the gonial angle. |
| Miloglu et al., 2010 [17] | Radiographs from patients undergoing dental treatment (10,200) | 32 (0.3%) had bifid mandibular condyle | No present static values | Turkey | 10,168 unknown gender; 17 female; 15 male. | 32 patients, 24 (75.0%) had unilateral, 8 (25.0%) had bilateral | This anomaly does not present any clinical symptoms and dentists are more interested in dental pathologies in the examination of radiographs. |
| Neelakandan and Bhargava., 2011 [18] | Panoramic radiography and computerized tomography evaluation of chin deviation on a 14-year-old male (1) | Unique in study | No present static values | India | One male | Unilateral | First reported case of bifid mandibular condyle with condyle hyperplasia. The etiology of bifid condyle is largely unknown, although various factors have been suggested as possible causes like endocrine. |
| Prol et al., 2016 [19] | 13-year-old female orthopantomography and palpation in masticatory muscles (1) | Unique in study | No present static values | Spain | One female | Bilateral | The authors do not refer to previous trauma. Both upper condylar surfaces with a depression, compatible with bifid condyle of mediolateral type. |
| Rajashri et al., 2021 [20] | Magnetic resonance evaluation of a 38-year-old male patient (1) | Male patient with bifid mandibular condyle | No present static values | India | One male | Unilateral | His magnetic resonance showed signs of mild degenerative changes of the bilateral articular disk with reduced translation on the right side and a bifid left mandibular condyle with a small cyst next to the left temporomandibular joint. |
| Tutar et al., 2012 [21] | Panoramic radiographs of a 24-year-old patient (1) | One patient with bifid mandibular condyle | No present static values | Turkey | One female | Bilateral | Most cases are asymptomatic, but there can be associated symptoms such as clicking, moderate pain, and limitation of mandibular movements. |
| Haghnegahdar AA et al., 2014 [22] | Dental panoramic views of individuals (1000) | Bifidity was detected in 35 cases (3.5%). | No present static values | Iran | 767 female and 233 male individuals. 23 female patients and 12 male patients showed bifidity. | 35 patients; 32 had unilateral (24 on the left and 8 on the right side) and 3 had bilateral bifid mandibular condyle. | Approximately one third of the cases of the study were symptomatic, suffering from clicking, pain, or both. This anomaly may be misinterpreted as the presence of tumors or fractures in the condylar area. |
| A.H.Shaikh et al., 2021 [23] | Panoramic radiographic evaluation of 500 mandibular condyles (250) | Different shapes of condyles have been identified, namely, oval (50%), bird beak (40%), diamond (4.8%) and crooked finger (4.8%) shape. | No present static values | Pakistan | 125 male patients and 125 female patients. | Not mentioned | Other studies reported that the condyle morphology with changes in condyle surface shapes is related to malocclusion and the relation between open bite and erosion of the head of the condyle. |
| Bhupender Singh et al., 2020 [24] | Examination of panoramic radiographs of mandibular condyles (350) | Dentition status was classified using the Eichner index. Eichner class A: 282 persons; Eichner class B: 33 persons; Eichner class C: 35 persons. | The relation between age groups and denture usage history was statistically significant (p = 0.00). | India | 155 male patients (44%) and 195 female patients (56%). | Not mentioned | There is a relation between dentition status and bilaterally similar condylar morphology. |
| Halil Sahman et al., 2012 [25] | Retrospective study of computerized tomography records (550) | This anomaly was found in 10 patients of the 550 (1.82%). A total of 13 bifid mandibular condyles were found in these 10 patients. | No significant gender difference in subjects with Bifid mandibular condyle (p > 0.5) No significant difference between right or left side bifid mandibular condyle (p > 0.5) | Turkey | 328 (59.6%) male patients and 222 (40.4%) female patients. 5 female patients and 5 male patients showed bifidity. | Three patients had bilateral and seven patients had unilateral bifid mandibular condyle (three on the left side and four on the right side). | Six patients were contacted. Two of them had a history of head trauma, reporting clicking on mouth opening and bilateral temporomandibular joint pain. |
| Rehman et al., 2009 [26] | Examination of computerized tomography of patients with temporomandibular joint ankylosis (37) | Of the 37 patients with temporomandibular joint ankylosis, 10 had bifid mandibular condyle. | No present static values | India | Of the 10 patients, 5 were male and 5 were female. | - Two patients had bilateral mediolaterally bifid mandibular condyle with unilateral temporomandibular joint ankylosis. - Two patients had bilateral anteroposteriorly bifid mandibular condyle. One of them had bilateral temporomandibular joint ankylosis and the other unilateral temporomandibular joint ankylosis. - Six patients had unilateral mediolaterally bifid mandibular condyle with ipsilateral temporomandibular joint ankylosis. | Nine patients report a history of trauma and one patient reports a history of infection. Among the nine patients that report a history of trauma, eight sustained falls on the face and one sustained a road traffic accident with penetrating facial injury. One patient refers that when he was 6 years old he had an infection episode, developing facial deformity and restriction of mouth opening. |
| Nikolova et al., 2016 [27] | Macroscopic observation of the condyles of dry intact mandibles from adult males (500) | Four patients present bifid mandibular condyle (0.8%). | No present static values | Bulgaria | All 500 patients were males; 4 showed bifidity. | All of the bifid mandibular condyle cases were unilateral, two on the right side and two on the left side. | Case 1 presents osteoarthritis in the mandibular fossa. Case 2 presents a shallow depression on the left condyle. |
| Faisal et al., 2015 [28] | Computerized tomography examination of two cases (2) | Two patients present bifid mandibular condyle. | No present static values | India | Both patients were female. | Both cases were unilateral bifid mandibular condyles. Case 1 presents left bifid mandibular condyle oriented anteroposteriorly. Case 2 presents right bifid mandibular condyle oriented mediolaterally. | Bifid mandibular condyle appears to be more common on the left side in unilateral cases (2:1). |
| Melo et al., 2012 [29] | Magnetic resonance of a 39-year-old female patient with mouth opening limitation and deviation of the mandible to the left side (1) | One female patient with bifid mandibular condyle and duplicated mandibular fossa, with the articular disc over the anterior head | No present static values | Brazil | Female patient | Unilateral bifid mandibular condyle present on the left side and duplicated mandibular fossa | A diagnosed mouth opening limitation and deflection of the mandible to the left side. This is the only case of bifid mandibular condyle that includes an anteroposterior bifid condyle. |
| Lee JS et al., 2017 [30] | Evaluation of bilateral difference in condyle position of patients with deviated mandibular prognathism using 3D reformatted images from cone beam computerized tomography (51) | 28 patients with asymmetric mandibular prognathism; 23 patients with symmetric mandibular prognathism. | Differences in the position of lateral condyle. More laterally and inferiorly in the contralateral side. (p < 0.05) differences in the position of the sigmoid notch. More laterally, superiorly and posteriorly positioned on the deviated side (p < 0.01) | Republic of Korea | 16 female patients with asymmetric mandibular prognathism and 9 female patients with symmetry; 12 male patients with asymmetric mandibular prognathism and 14 with symmetry. | Bilateral condylar position study | Asymmetric mandibular prognathism |
| Balaji et al., 2010 [31] | Computed tomograms performed on patients with temporomandibular joint ankylosis (121) | Of all 121 cases, 15 were diagnosed with bifid mandibular condyle (12.40%). | Difference between deviation of chin of bilateral bifid mandibular condyle (p = 0.000) | India | Seven male patients with bifid mandibular condyle; eight female patients with bifid mandibular condyle. | Four cases had bilateral bifid mandibular condyle. Eleven cases had unilateral bifid mandibular condyle. | All of the 15 cases reported in the study were oriented mediolaterally and all cases with mandibular joint ankylosis. |
| Khojastepour et al., 2015 [32] | Evaluation of patients’ cone beam computerized tomography scans to evaluate prevalence of bifid mandibular condyle (425) | 309 of 425 patients entered in the study due to acceptable visibility of condyles. 14 cases of bifid mandibular condyle were detected (4.53%). | No present static values | Iran | Of the 309 patients in the study, 170 were female (55%) and 139 were male (45%); 7 female patients and 7 male patients showed bifidity. | 3 had bilateral bifid mandibular condyle; 11 had unilateral bifid mandibular condyle, 5 cases were detected on the right side and 6 were detected on the left side. | The use of cone beam computerized tomography scans to evaluate temporal mandibular joint area has the advantage that it eliminates superimpositions in the images. |
| Gyoon et al., 2015 [33] | Use of nanoindentation in human cadavers to examine variations of the elastic, plastic, and viscoelastic mechanical properties of human mandibular condyle bone tissue. (9) | Cortical and trabecular bone dissected from mandibular condyles of nine human cadavers | Significant difference between high gray values of endosteal cortical bone and periosteal cortical bone and trabecular bone (p < 0.007) | USA | 9 male patients | Not mentioned | This is the first study that measures five parameters of elastic, plastic, and viscoelastic mechanical properties in fresh human mandibular condylar bone using nanoindentation. |
| Kaan Gunduz et al., 2015 [34] | Cone beam computed tomography images of patients to study the frequency of bifid mandibular condyle (2634) | Of the 2634 patients of the study, 45 bifid mandibular condyles were found in 42 (1.7%) patients. | No significant difference of clinical symptoms between patients with normally shaped condyles and bifid mandibular condyle (p > 0.05) | Turkey | Of the 2634 patients, 1455 (45.41%) were male and 1179 (49.54%) were female, and of the 42 patients with bifid mandibular condyle, 22 (52.38%) were male and 20 (47.62%) were female. | Of all 45 bifid mandibular condyles, 39 (92.8%) were unilateral cases and 3 (7.1%) bilateral cases. 24 cases (53.3%) were on the right side and 21 cases (46.6%) were on the left side. | Two patients reported a history of trauma and clicking on mouth opening. |
| Menezes et al., 2008 [35] | Examination of radiographic images in a group of patients to evaluate the morphology and frequency of bifid mandibular condyles (50,080) | Of all 50,080 panoramic radiographs, only 9 (0.018%) cases of bifid mandibular condyle were found. | No present static values | Brazil | Seven female and two male patients with bifid mandibular condyle. | Seven unilateral cases. Four cases on the left side and three on the right side. Two bilateral cases. | There were no cases of history of previous trauma, pain or trismus. |
| Neves et al., 2013 [36] | Comparison between panoramic radiography and cone beam computerized tomography of individuals (350) | Of all 350 individuals, 4 (1.1%) cases of bifid mandibular condyle were detected. | No present static values | Brazil | Three female patients and one male patient with bifid mandibular condyle. | All cases were unilateral. Three of them were detected on the right side and one was detected on the left side. | In all four cases, a history of trauma was reported and the relation of one condylar process to the other was mediolateral. |
| Szentpétery et al., 1990 [37] | Examination of prehistoric skulls with a total number of condyles (1882) | Among the 1882 skulls, 7 cases of bifid mandibular condyle were detected. | No present static values | Hungary | Five female individuals and two male individuals with bifid mandibular condyle. | The seven cases of bifid mandibular condyle were unilateral cases. Two were detected on the left side and five on the right side. | In the seven cases, the grooving was anteroposteriorly directed. |
| Balaji et al., 2010 [38] | Retrospective examination of patients computerized tomography (121) | Of all 121 cases, 12 patients presented bifid mandibular condyle. | No present static values | India | Five male and seven female patients were detected with bifid mandibular condyle. | Three bilateral cases and nine unilateral cases. Eight were detected on the left side and one on the right side. | All cases of the study exhibited mushroom-shaped bifid condyle. History of trauma was reported in 91.7% of cases. |
| Halil Sahman et al., 2011 [39] | Retrospective study of panoramic radiographs (18,798) | Of all 18,798 cases, 98 patients were detected with bifid mandibular condyle. | No statistically significant differences between right and left bifid mandibular condyles, or between female and male patients (p > 0.05). | Turkey | 51 female patients and 47 male patients with bifid mandibular condyle. | 27 bilateral cases and 71 unilateral cases with bifid mandibular condyle. 37 cases were detected on the right side and 34 cases on the left side. | The frequency of bifid mandibular condyle is higher. |
| Agarwal Varun et al., 2006 [40] | Panoramic radiograph of a bifid mandibular condyle. They reported four cases: two patients and two in archived specimens. (48) | The condylar head is duplicated (dividing it into medial and lateral condylar heads) (4/48). | No present static values | India | Two specimens Two female | Two bilateral bifid condyles Two right-sided bifid mandibular condyle | In the first case, a female patient referred to a polyarthralgia before she reported her problem with a limited mouth opening. She referred only to malocclusion. In the other case, the patient has a bifid mandibular condyle, with no pain and normal mouth opening. |
| Alpaslan et al., 2004 [41] | A 40-year-old male with pain at the both temporomandibular joints. In a routine dental examination with a panoramic radiograph revealed bilateral bifid condyles. (1) | Unique in study | No present static values | Turkey | One male | Bilateral | The patient referred to a moderate pain during chewing at the bilateral temporomandibular joint. His maximum opening was 48 mm. |
| Katti et al., 2012 [42] | Panoramic radiography of a 20-year-old male patient with limited mouth opening and cosmetic disfigurement (1) | Unique case in study | No present static values | India. | One male | Right side | The patient presented a limitation of jaw movement and his mouth opening was limited to 27 mm. The examination of the head revealed a mandibular micrognathia. |
| Michalski et al., 2022 [34] | Nine-year-old patient with unilateral ankylosis of the temporomandibular joint (TMJ). In a physical examination a deviation of the mandible was noted. To evaluate they used computed tomography imaging (9) | Unique case in the study | No present static values | USA | One male | Left side | The patient did not refer to a trauma or infection in his clinical history, but the ankylosis of the temporomandibular joint (TMJ) was a defect to development of bifid mandibular condyle, with difficulty opening his mouth. |
| Screenivasagan et al., 2021 [43] | Evaluation of radiographs of condylar heads by an orthopantomogram (987) | 1048 oval, 148 crooked, 382 bird beak, and 396 diamond condylar morphology | No present static values | India | 512 female 475 male | Not mentioned | The anatomical morphology defines the progression of symptoms and the occlusion of the mandible. |
| Schmitter et al., 2006 [44] | Magnetic resonance imaging evaluation (40) | 21 Patients complained about arthrogenic problems and 19 patients did not complain about arthrogenic problems. | No present static values | Germany | 13 male 27 female | Not mentioned | Temporomandibular disorder often involves the action of masticatory muscles. There were symptomatic and asymptomatic patients. |
| Sala Pérez et al., 2012 [45] | Panoramic radiography was the technique of diagnosing bifid mandibular condyle. In this study, cases with anatomical variation of the temporomandibular joint were analyzed. (6) | Microtrauma or trauma, malocclusion, radiotherapy or infections; all of these factors may produce alterations in the condylar joint. | No present static values | USA | Four male Two female | One case with bilateral bifid mandibular condyle. Five cases with unilateral bifid mandibular condyle (right) | Clinical examination revealed a limitation in mouth opening, moderate pain, and joint sounds in the temporomandibular joint (TMJ). |
| Anzola et al., 2021 [46] | This study investigated normal activity values of the mandibular condyles by bone scintigraphy. (25) | Characterized by progressive unilateral growth, resulting in global enlargement of the condyle including the condylar neck and the body and ramus of the jaw | No present static values | Colombia | 16 female 9 male | Not mentioned | Facial asymmetry and occlusal alterations |
| Hiperplasia condilar |
| Diagnostic Method | Number of Articles | Total Number of Subjects |
|---|---|---|
| Macroscopic evaluation (corpse) | 3 | 2525 |
| Magnetic resonance | 3 | 42 |
| CT scan | 6 | 840 |
| Cone beam computerized tomography | 3 | 3110 |
| Orthopantomography | 2 | 988 |
| Panoramic X-ray | 13 | 81,086 |
| Bone scintigraphy | 1 | 25 |
| Nanoindentation | 1 | 9 |
| Author | Total N | Prevalence | Prevalence Meta-Analysis Status |
|---|---|---|---|
| González-Garrido et al., 2022 [16] | 143 | 2 | Included |
| Miloglu et al., 2010 [17] | 10,200 | 32 | Included |
| Haghnegahdar et al., 2014 [22] | 1000 | 35 | Included |
| Shaikh et al., 2021 [23] | 500 | 19 | Included |
| Singh et al., 2020 [24] | 350 | 33 | Included |
| Sahman et al., 2012 [25] | 550 | 10 | Included |
| Nikolova et al., 2016 [27] | 500 | 4 | Included |
| Lee et al., 2017 [30] | 51 | 23 | Not included |
| Rehman et al., 2009 [26] | 37 | 10 | Not included |
| Balaji et al., 2010 [31] | 121 | 15 | Included |
| Khojastepour et al., 2015 [32] | 425 | 14 | Included |
| Gunduz et al., 2015 [47] | 2634 | 45 | Included |
| Menezes et al., 2008 [35] | 50,080 | 9 | Included |
| Neves et al., 2013 [36] | 350 | 4 | Included |
| Szentpétery et al., 1990 [37] | 1882 | 7 | Included |
| Balaji et al., 2010 [38] | 121 | 12 | Included |
| Sahman et al., 2011 [39] | 18,798 | 98 | Included |
| Sreenivasagan S et al., 2021 [43] | 48 | 4 | Not included |
| Schmitter et al., 2006 [44] | 40 | 19 | Not included |
| Anzola et al., 2021 [46] | 25 | 2 | Not included |
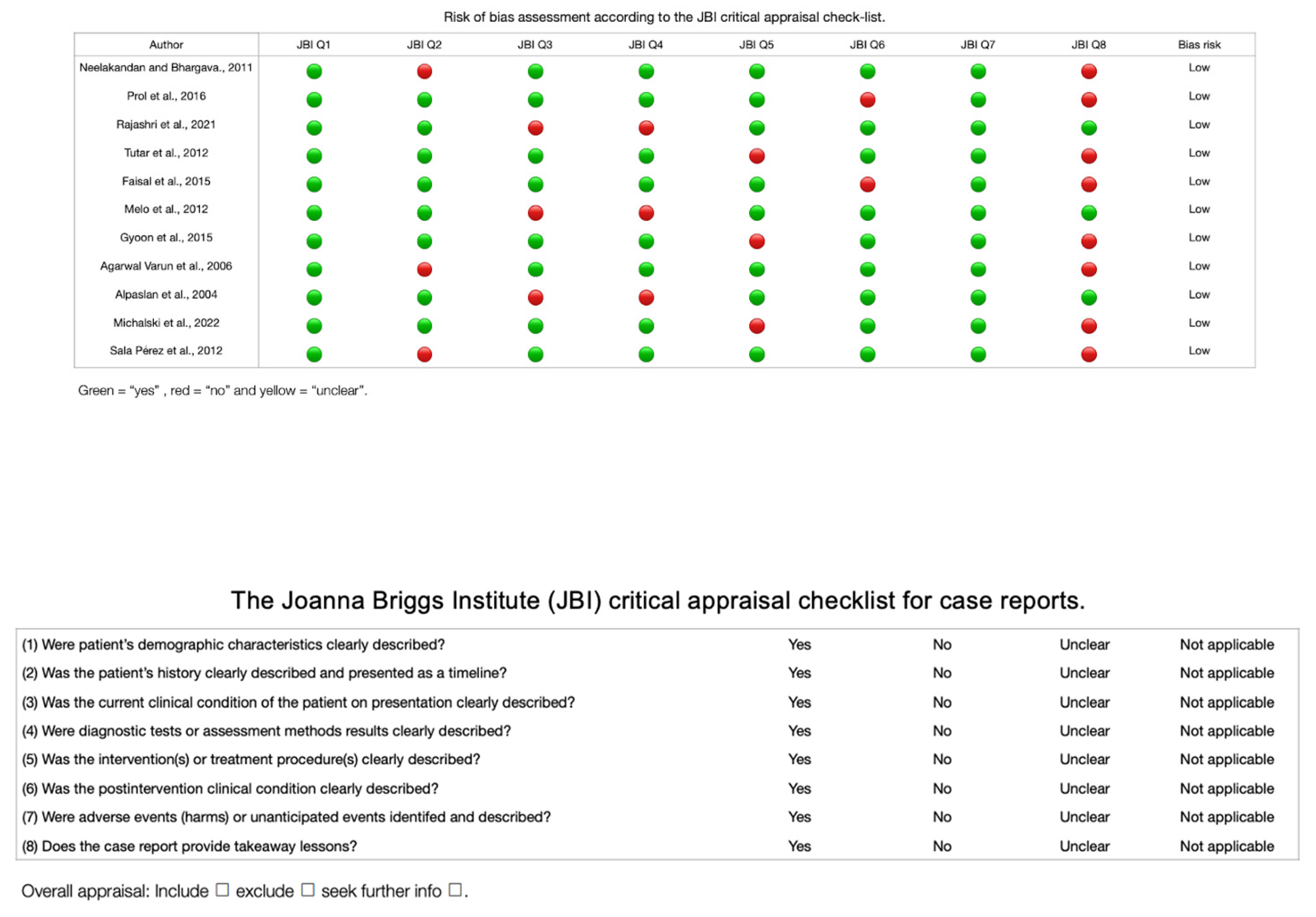
| Author | JBI Q1 | JBI Q2 | JBI Q3 | JBI Q4 | JBI Q5 | JBI Q6 | JBI Q7 | JBI Q8 | Bias Risk |
|---|---|---|---|---|---|---|---|---|---|
| Neelakandan and Bhargava, 2011 [18] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Low |
| Prol et al., 2016 [19] | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Low |
| Rajashri et al., 2021 [20] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Low |
| Tutar et al., 2012 [21] | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Low |
| Faisal et al., 2015 [28] | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Low |
| Melo et al., 2012 [29] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Low |
| Gyoon et al., 2015 [33] | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Low |
| Varun et al., 2006 [40] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Low |
| Alpaslan et al., 2004 [41] | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Low |
| Michalski et al., 2022 [34] | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Low |
| Pérez et al., 2012 [45] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Low |
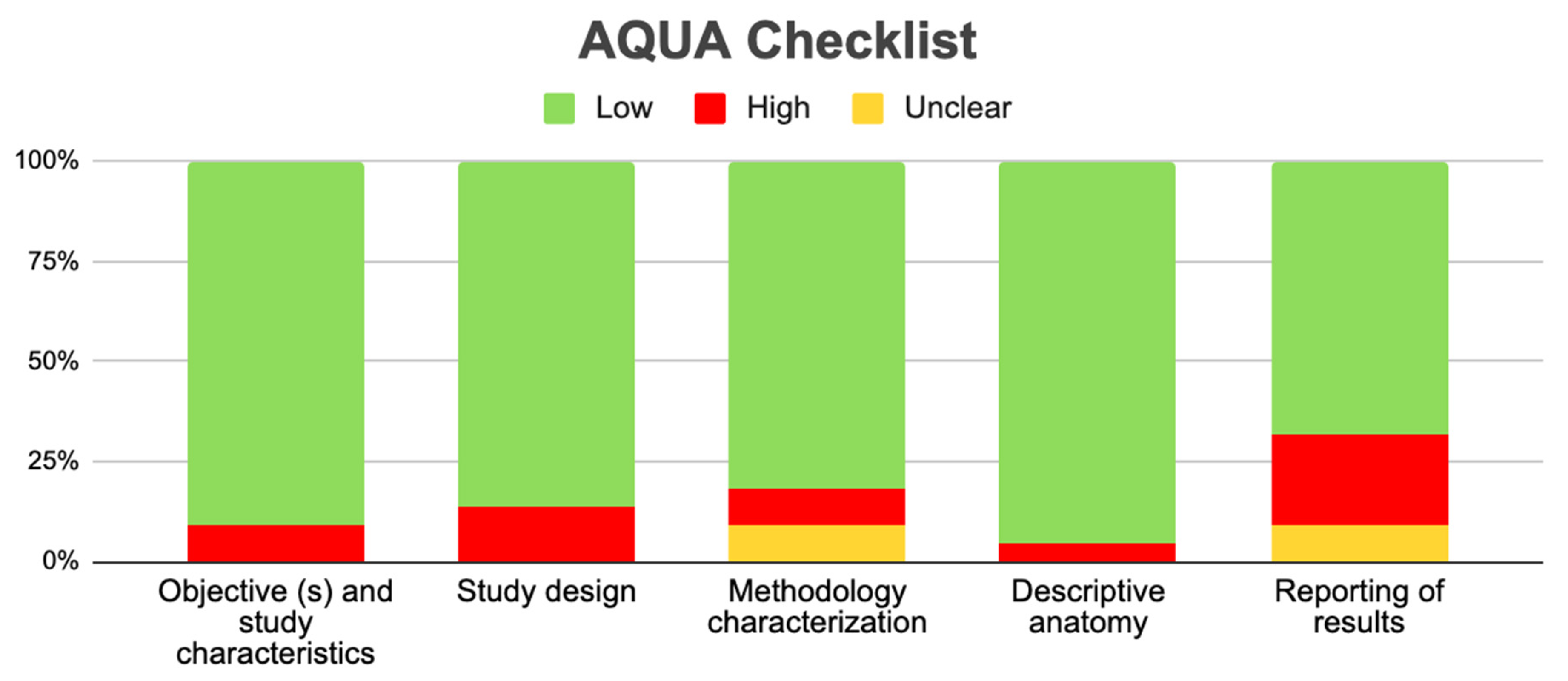
| References | Study Design | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | ||
| González-Garrido et al., 2022 [16] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Miloglu et al., 2010 [17] | Observational study | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Haghnegahdar AA et al., 2014 [22] | Observational study | Y | Y | N | N | Y | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | Y | Y | NA | Y | Y | Y | Y |
| A.H.Shaikh et al., 2021 [23] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | NA | Y | Y | Y | Y |
| Bhupender Singh et al., 2020 [24] | Observational study | Y | N | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA | Y | Y | Y | Y |
| Halil Sahman et al., 2012 [25] | Observational study | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | NA | Y | NA | Y | Y | Y | Y |
| Nikolova et al., 2016 [27] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Lee JS et al. 2017 [30] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | N | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Rehman et al., 2009 [26] | Observational study | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Balaji et al., 2010 [31] | Observational study | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Khojastepour et al., 2015 [32] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | N | Y | N | N | NA | Y | Y | Y | Y |
| Kaan Gunduz et al., 2015 [34] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | NA | Y | NA | Y | Y | Y | Y |
| Menezes et al., 2008 [35] | Observational study | Y | Y | Y | Y | N | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y | N | Y | NA |
| Neves et al., 2013 [36] | Observational study | N | Y | N | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | N | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Szentpétery et al., 1990 [37] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | N | Y | N | N | NA | Y | Y | Y | Y |
| Balaji et al., 2010 [38] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | NA | Y | NA | Y | Y | Y | Y |
| Halil Sahman et al., 2011 [39] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Sreenivasagan S et al., 2021 [43] | Observational study | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Schmitter et al., 2006 [44] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | Y | NA | Y | NA | Y | Y | N | Y |
| Rehman et al., 2009 [26] | Observational study | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Anzola et al., 2021 [46] | Observational study | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | NA | Y | NA | Y | Y | N | Y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenzuela-Fuenzalida, J.J.; Navarro, K.-l.K.; Urbina, P.; Trujillo-Riveros, M.; Nova-Baeza, P.; Orellana-Donoso, M.; Rodriguez-Luengo, M.; Beccerra Farfan, A.; Sanchis-Gimeno, J.A. Prevalence of the Bifid Mandibular Condyle and Its Relationship with Pathologies of the Temporomandibular Joint: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 3282. https://doi.org/10.3390/diagnostics13203282
Valenzuela-Fuenzalida JJ, Navarro K-lK, Urbina P, Trujillo-Riveros M, Nova-Baeza P, Orellana-Donoso M, Rodriguez-Luengo M, Beccerra Farfan A, Sanchis-Gimeno JA. Prevalence of the Bifid Mandibular Condyle and Its Relationship with Pathologies of the Temporomandibular Joint: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(20):3282. https://doi.org/10.3390/diagnostics13203282
Chicago/Turabian StyleValenzuela-Fuenzalida, Juan José, Kora-lle Keller Navarro, Pia Urbina, Martin Trujillo-Riveros, Pablo Nova-Baeza, Mathias Orellana-Donoso, Macarena Rodriguez-Luengo, Alvaro Beccerra Farfan, and Juan A. Sanchis-Gimeno. 2023. "Prevalence of the Bifid Mandibular Condyle and Its Relationship with Pathologies of the Temporomandibular Joint: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 20: 3282. https://doi.org/10.3390/diagnostics13203282
APA StyleValenzuela-Fuenzalida, J. J., Navarro, K. -l. K., Urbina, P., Trujillo-Riveros, M., Nova-Baeza, P., Orellana-Donoso, M., Rodriguez-Luengo, M., Beccerra Farfan, A., & Sanchis-Gimeno, J. A. (2023). Prevalence of the Bifid Mandibular Condyle and Its Relationship with Pathologies of the Temporomandibular Joint: A Systematic Review and Meta-Analysis. Diagnostics, 13(20), 3282. https://doi.org/10.3390/diagnostics13203282