
Changes in Clinical Manifestations Due to AFLD Retyping Based on the New MAFLD Criteria: An Observational Study Based on the National Inpatient Sample Database
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
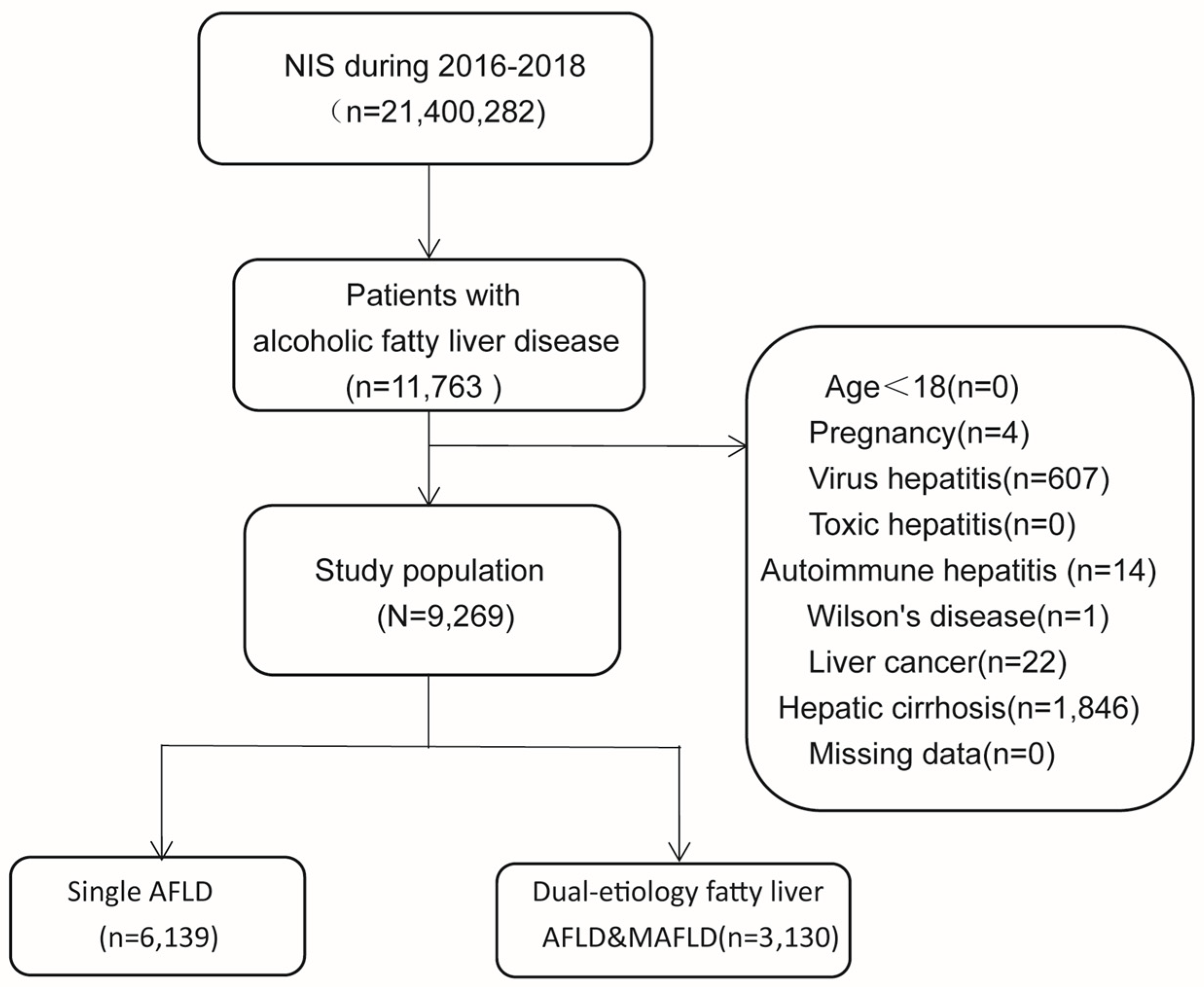
2.1. Study Population and Study Design
2.2. Data Collection
2.3. Definition of AFLD&MAFLD and Single AFLD
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients in the Two AFLD Groups
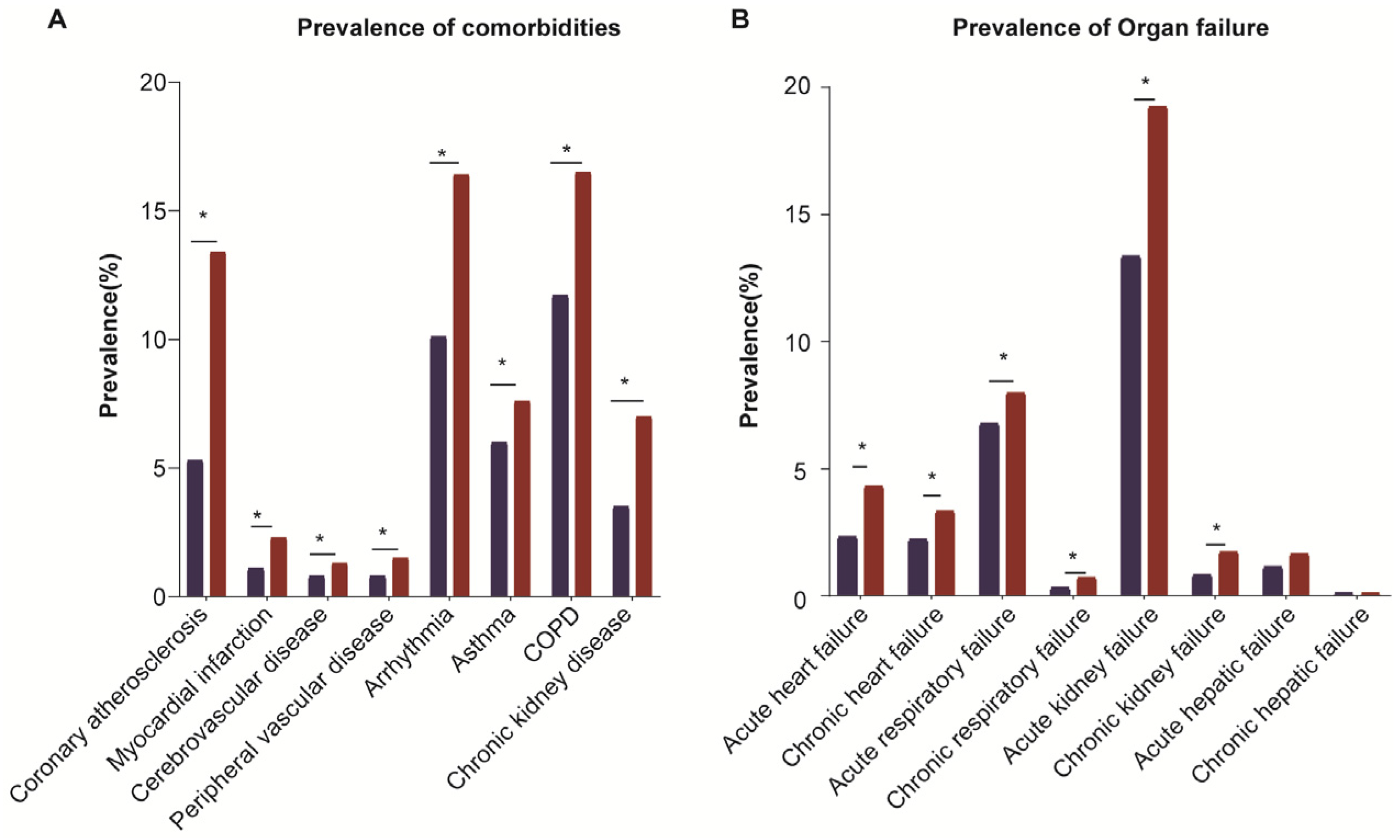
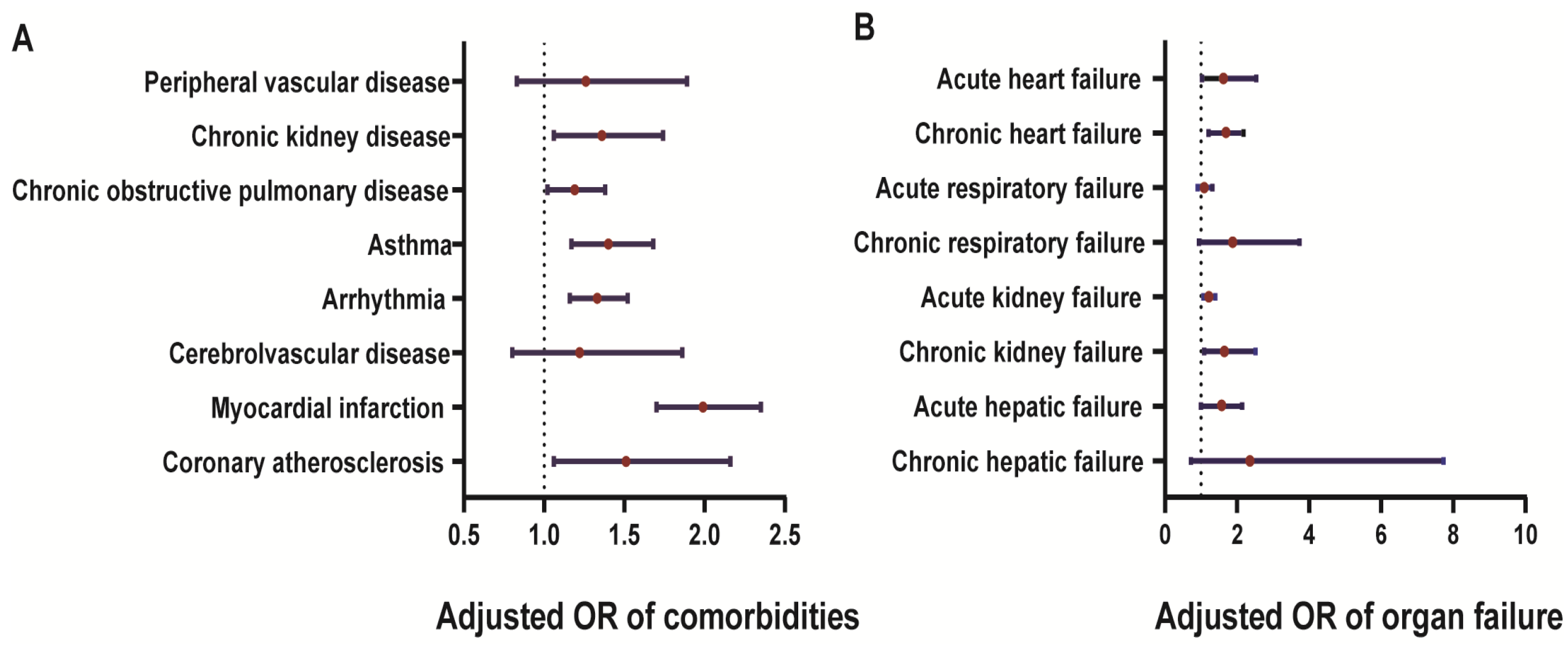
3.2. High Risk of Comorbidities and Organ Failure in the AFLD&MAFLD Group
3.3. Characteristics of Length of Stay, Hospital Total Charges, Nonelective Admission, and All-Cause Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.S.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Méndez-Sánchez, N.; Bugianesi, E.; Gish, R.G.; Lammert, F.; Tilg, H.; Nguyen, M.H.; Sarin, S.K.; Fabrellas, N.; Zelber-Sagi, S.; Fan, J.-G.; et al. Global multi-stakeholder endorsement of the MAFLD definition. Lancet Gastroenterol. Hepatol. 2022, 7, 388–390. [Google Scholar] [CrossRef] [PubMed]
- Poniachik, J.; Roblero, J.P.; Urzúa, A.; Cattaneo, M. A new definition for non-alcoholic fatty liver disease. J. Hepatol. 2021, 74, 982–983. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; Bataller, R. Alcoholic liver disease: Pathogenesis and new therapeutic targets. Gastroenterology 2011, 141, 1572–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Shea, R.S.; Dasarathy, S.; McCullough, A.J. Practice Guideline Committee of the American Association for the Study of Liver D, Practice Parameters Committee of the American College of G. Alcoholic liver disease. Hepatology 2010, 51, 307–328. [Google Scholar] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Merz, C.N.B.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, T.; Dang, K.; Ladhani, S.; Singal, A.K.; Wong, R.J. Prevalence of Alcoholic Fatty Liver Disease Among Adults in the United States, 2001–2016. JAMA 2019, 321, 1723–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Cho, Y.K.; Cho, J.; Jung, H.-S.; Yun, K.E.; Ahn, J.; Sohn, C.I.; Shin, H.; Ryu, S. Alcoholic and Nonalcoholic Fatty Liver Disease and Liver-Related Mortality: A Cohort Study. Am. J. Gastroenterol. 2019, 114, 620–629. [Google Scholar] [CrossRef]
- Kim, D.; Konyn, P.; Sandhu, K.K.; Dennis, B.B.; Cheung, A.C.; Ahmed, A. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J. Hepatol. 2021, 75, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Rodas, M.C.; Valenzuela, R.; Videla, L.A. Relevant Aspects of Nutritional and Dietary Interventions in Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, V.H.; Le, M.H.; Cheung, R.C.; Nguyen, M.H. Differential Clinical Characteristics and Mortality Outcomes in Persons with NAFLD and/or MAFLD. Clin. Gastroenterol. Hepatol. 2021, 19, 2172–2181.e2176. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiatiove. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Singal, A.K.; Bataller, R.; Ahn, J.; Kamath, P.S.; Shah, V.H. ACG Clinical Guideline: Alcoholic Liver Disease. Am. J. Gastroenterol. 2018, 113, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.A.; Park, H. Comorbidity network analysis related to obesity in middle-aged and older adults: Findings from Korean population-based survey data. Epidemiol. Health 2021, 43, e2021018. [Google Scholar] [CrossRef]
- Åberg, F.; Puukka, P.; Salomaa, V.; Männistö, S.; Lundqvist, A.; Valsta, L.; Perola, M.; Jula, A.; Färkkilä, M. Combined Effects of Alcohol and Metabolic Disorders in Patients with Chronic Liver Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 995–997. [Google Scholar] [CrossRef]
- Aberg, F.; Helenius-Hietala, J.; Puukka, P.; Farkkila, M.; Jula, A. Interaction between alcohol consumption and metabolic syndrome in predicting severe liver disease in the general population. Hepatology 2018, 67, 141–2149. [Google Scholar] [CrossRef] [Green Version]
- Agborsangaya, C.B.; Ngwakongnwi, E.; Lahtinen, M.; Cooke, T.; Johnson, J.A. Multimorbidity prevalence in the general population: The role of obesity in chronic disease clustering. BMC Public Health 2013, 13, 1161. [Google Scholar] [CrossRef] [Green Version]
- Madlock-Brown, C.R.; Reynolds, R.B.; Bailey, J.E. Increases in multimorbidity with weight class in the United States. Clin. Obes. 2021, 11, e12436. [Google Scholar] [CrossRef]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef] [PubMed]
- Sorop, O.; Heinonen, I.; Van Kranenburg, M.; Van De Wouw, J.; De Beer, V.J.; Nguyen, I.T.; Octavia, Y.; Van Duin, R.W.; Stam, K.; van Geuns, R.J.; et al. Multiple common comorbidities produce left ventricular diastolic dysfunction associated with coronary microvascular dysfunction, oxidative stress, and myocardial stiffening. Cardiovasc. Res. 2018, 114, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Gakidou, E.; Mallinger, L.; Abbott-Klafter, J.; Guerrero, R.; Villalpando, S.; Ridaura, R.L.; Aekplakorn, W.; Naghavi, M.; Lim, S.; Lozano, R.; et al. Management of diabetes and associated cardiovascular risk factors in seven countries: A comparison of data from national health examination surveys. Bull. World Health Organ. 2011, 89, 172–183. [Google Scholar] [CrossRef]
- Zhang, H.; Park, Y.; Wu, J.; Chen, X.P.; Lee, S.; Yang, J.; Dellsperger, K.C.; Zhang, C. Role of TNF-alpha in vascular dysfunction. Clin. Sci. 2009, 16, 219–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, I.; Suzuki, A.; Vallée, M.; Matano, Y.; Masunaga, T.; Zenda, T.; Shinozaki, K.; Okada, T. Serum insulin levels and the prevalence of adenomatous and hyperplastic polyps in the proximal colon. Clin. Gastroenterol. Hepatol. 2006, 4, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Giouleme, O.; Diamantidis, M.; Katsaros, M.G. Is diabetes a causal agent for colorectal cancer? Pathophysiological and molecular mechanisms. World J. Gastroenterol. 2011, 17, 444–448. [Google Scholar] [CrossRef]
- Soubry, A.; Il’yasova, D.; Sedjo, R.; Wang, F.; Byers, T.; Rosen, C.; Yashin, A.; Ukraintseva, S.; Haffner, S.; D’Agostino, R., Jr. Increase in circulating levels of IGF-1 and IGF-1/IGFBP-3 molar ratio over a decade is associated with colorectal adenomatous polyps. Int. J. Cancer 2012, 131, 512–517. [Google Scholar] [CrossRef] [Green Version]
- Xie, C.; Wen, P.; Su, J.; Li, Q.; Ren, Y.; Liu, Y.; Shen, R.; Ren, J. Elevated serum triglyceride and low-density lipoprotein cholesterol promotes the formation of colorectal polyps. BMC Gastroenterol. 2019, 19, 195. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Liu, H.; Niu, Z.; Zhong, W.; Xue, M.; Wang, J.; Yang, F.; Zhou, Y.; Zhou, Y.; Xu, T. Temporal Proteomic Analysis of Pancreatic beta-Cells in Response to Lipotoxicity and Glucolipotoxicity. Mol. Cell Proteom. 2018, 17, 2119–2131. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi, A.G.; Hollister-Lock, J.; Sullivan, B.A.; Tsuchida, R.; Bonner-Weir, S.; Weir, G.C. Beta cell identity changes with mild hyperglycemia: Implications for function, growth, and vulnerability. Mol. Metab. 2020, 35, 100959. [Google Scholar] [CrossRef] [PubMed]
- Samuel, V.T.; Shulman, G.I. The pathogenesis of insulin resistance: Integrating signaling pathways and substrate flux. J. Clin. Investig. 2016, 126, 12–22. [Google Scholar] [CrossRef] [Green Version]
- James, D.E.; Stöckli, J.; Birnbaum, M.J. The aetiology and molecular landscape of insulin resistance. Nat. Rev. Mol. Cell Biol. 2021, 22, 751–771. [Google Scholar] [CrossRef] [PubMed]
- Ismail, N.; Becker, B.; Strzelczyk, P.; Ritz, E. Renal disease and hypertension in non-insulin-dependent diabetes mellitus. Kidney Int. 1999, 55, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Tan, W.; Pan, X.; Tian, E.; Wu, Z.; Yang, J. Metabolic Syndrome-Related Kidney Injury: A Review and Update. Front. Endocrinol. 2022, 13, 904001. [Google Scholar] [CrossRef]
- Yeh, M.M.; Brunt, E.M. Pathological features of fatty liver disease. Gastroenterology 2014, 147, 754–764. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 9269) | Single AFLD Group (n = 6139) | AFLD&MAFLD Group (n = 3130) | p Value * |
|---|---|---|---|---|
| Age (years) (mean ± SD) | 49.40 ± 13.0 | 47.69 ±12.92 | 52.74 ± 12.42 | <0.001 |
| Male (%) | 6476 (69.9) | 4154 (67.7) | 2322 (74.2) | <0.001 |
| Race | <0.001 | |||
| White (%) | 6389 (70.0) | 4317 (70.1) | 2072 (68.4) | |
| African American (%) | 1066 (11.9) | 703 (11.8) | 363 (12) | |
| Hispanic (%) | 1170 (13) | 750 (12.6) | 420 (13.9) | |
| Asian/Pacific Islander (%) | 110 (1.2) | 64 (1.1) | 46 (1.5) | |
| Native American (%) | 124 (1.4) | 77 (1.3) | 47 (1.6) | |
| Other races (%) | 262 (2.9) | 180 (3.0) | 82 (2.7) | |
| Tobacco abuse (%) | 488 (5.3) | 336 (5.5) | 152 (4.9) | 0.208 |
| Overweight (%) | 263 (2.8) | 0 (0.0) | 263 (8.4) | <0.001 |
| Obesity (%) | 1239(13.4) | 0 (0.0) | 1239 (39.6) | <0.001 |
| Hypertension (%) | 4305 (46.5) | 2240 (36.5) | 2065 (66.0) | <0.001 |
| Comorbidity | ||||
| Prediabetes (%) | 1544 (16.7) | 60 (1.0) | 1484 (47.4) | <0.001 |
| DM | ||||
| T1DM (%) | 71 (0.8) | 31 (0.5) | 40 (1.3) | <0.001 |
| T2DM (%) | 1328 (14.3) | 0 (0.0) | 1328 (42.4) | <0.001 |
| Dyslipidemia | ||||
| Hyperlipidemia (%) | 1714 (18.5) | 321 (5.2) | 1393 (44.5) | <0.001 |
| Hypercholesterolemia (%) | 2085 (22.5) | 533 (8.7) | 1552 (49.6) | <0.001 |
| Hypertriglyceridemia (%) | 256 (2.8) | 121 (2.0) | 135 (4.3) | <0.001 |
| Coronary atherosclerosis (%) | 759 (8.2) | 340 (5.3) | 419 (13.4) | <0.001 |
| Myocardial infarction (%) | 138 (1.5) | 67 (1.1) | 71 (2.3) | <0.001 |
| Cerebrovascular disease (%) | 93 (1.0) | 52 (0.8) | 41 (1.3) | 0.034 |
| Peripheral vascular disease (%) | 110 (1.1) | 52 (0.8) | 48 (1.5) | 0.002 |
| Arrhythmia (%) | 1133 (12.2) | 620 (10.1) | 513 (16.4) | <0.001 |
| Asthma (%) | 608 (6.6) | 370 (6.0) | 238 (7.6) | 0.030 |
| COPD (%) | 1234 (13.3) | 718 (11.7) | 516 (16.5) | <0.001 |
| Chronic kidney disease (%) | 434 (4.7) | 214 (3.5) | 220 (7.0) | <0.001 |
| Organ failure | ||||
| Acute heart failure (%) | 280 (3.0) | 144 (2.3) | 136 (4.3) | <0.001 |
| Chronic heart failure (%) | 237 (2.6) | 135 (2.2) | 103 (3.3) | 0.002 |
| Acute respiratory failure (%) | 664 (7.16) | 415 (6.76) | 249 (7.96) | 0.035 |
| Chronic respiratory failure (%) | 40 (0.4) | 19 (0.3) | 21 (0.7) | 0.012 |
| Acute kidney failure (%) | 1421 (15.33) | 819 (13.34) | 602 (19.23) | <0.001 |
| Chronic kidney failure (%) | 104 (1.1) | 52 (0.8) | 52 (1.7) | <0.001 |
| Acute hepatic failure (%) | 120 (1.29) | 69 (1.12) | 51 (1.63) | 0.42 |
| Chronic hepatic failure (%) | 11 (0.1) | 5 (0.1) | 6 (0.1) | 0.145 |
| Ventilator support during operation (%) | 451 (4.87) | 289 (4.71) | 162 (5.18) | 0.322 |
| Length of stay (days) (mean ± SD) | 5.38 ± 6.24 | 5.27 ± 6.05 | 5.59 ± 6.60 | 0.026 |
| Total Charge (1000 dollars) (mean ± SD) | 52.19 ± 76.93 | 49.84 ± 75.65 | 56.82 ± 79.21 | <0.001 |
| Death (%) | 106 (1.11) | 64 (1.04) | 42 (1.34) | 0.201 |
| Variables | Univariable Model | Multivariable Model | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| LOS ≥ 9 days | ||||
| AFLD | 1 (Reference) | 1 (Reference) | ||
| AFLD&MAFLD | 1.26 (1.12–1.42) | <0.001 | 1.16(1.02–1.31) | 0.020 |
| TC ≥ 50,000 dollars | ||||
| AFLD | 1 (Reference) | 1 (Reference) | ||
| AFLD&MAFLD | 1.28(1.17–1.41) | <0.001 | 1.12(1.02–1.23) | 0.024 |
| Non-elective admission | ||||
| AFLD | 1 (Reference) | 1 (Reference) | ||
| AFLD&MAFLD | 1.54(1.27–1.87) | <0.001 | 1.28(1.04–1.57) | 0.019 |
| All-cause mortality | ||||
| AFLD | 1 (Reference) | 1 (Reference) | ||
| AFLD&MAFLD | 1.29(0.87–1.91) | 0.202 | 1.003(0.664–1.515) | 0.989 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, X.; Xuan, R.; Dong, Y.; Wu, X.; Cheng, Y.; Yuan, Z.; Dong, H.; Han, J.; Zhong, F.; Zhao, J.; et al. Changes in Clinical Manifestations Due to AFLD Retyping Based on the New MAFLD Criteria: An Observational Study Based on the National Inpatient Sample Database. Diagnostics 2023, 13, 488. https://doi.org/10.3390/diagnostics13030488
Feng X, Xuan R, Dong Y, Wu X, Cheng Y, Yuan Z, Dong H, Han J, Zhong F, Zhao J, et al. Changes in Clinical Manifestations Due to AFLD Retyping Based on the New MAFLD Criteria: An Observational Study Based on the National Inpatient Sample Database. Diagnostics. 2023; 13(3):488. https://doi.org/10.3390/diagnostics13030488
Chicago/Turabian StyleFeng, Xiaoshan, Ruirui Xuan, Yingchun Dong, Xiaoqin Wu, Yiping Cheng, Zinuo Yuan, Hang Dong, Junming Han, Fang Zhong, Jiajun Zhao, and et al. 2023. "Changes in Clinical Manifestations Due to AFLD Retyping Based on the New MAFLD Criteria: An Observational Study Based on the National Inpatient Sample Database" Diagnostics 13, no. 3: 488. https://doi.org/10.3390/diagnostics13030488
APA StyleFeng, X., Xuan, R., Dong, Y., Wu, X., Cheng, Y., Yuan, Z., Dong, H., Han, J., Zhong, F., Zhao, J., & Fan, X. (2023). Changes in Clinical Manifestations Due to AFLD Retyping Based on the New MAFLD Criteria: An Observational Study Based on the National Inpatient Sample Database. Diagnostics, 13(3), 488. https://doi.org/10.3390/diagnostics13030488